

Abstract
Objective We sought to investigate whether women present adequate knowledge of the main pelvic floor disorders (PFDs) (urinary incontinence – UI, fecal incontinence – FI, and pelvic organ prolapse – POP).
Data sources A systematic review was performed in the MEDLINE, PEDro, CENTRAL, and Cochrane databases for publications from inception to April 2018.
Selection of studies A total of 3,125 studies were reviewed. Meta-analysis was not possible due to the heterogeneity of primary outcomes and the diversity of instruments for measuring knowledge. The quality of the articles included in the analysis was evaluated with the Newcastle-Ottawa Scale (NOS) adapted for cross-sectional studies.
Data collection Two authors performed data extraction into a standardized spreadsheet.
Data synthesis Nineteen studies were included, comprising 11,512 women. About the methodological quality (NOS), most of the studies (n = 11) presented a total score of 6 out of 10. Validated questionnaires and designed pilot-tested forms were the most frequently used ways of assessing knowledge. Some studies were stratified by race, age, or group minorities. The most used questionnaire was the prolapse and incontinence knowledge questionnaire (PIKQ) (n = 5). Knowledge and/or awareness regarding PFD was low to moderate among the studies. Urinary incontinence was the most prevalent PFD investigated, and the most important risk factors associated with the lack of knowledge of the pelvic floor were: African-American ethnicity (n = 3), low educational level (n = 4), low access to information (n = 5) and socioeconomic status (n = 3).
Conclusion Most women have a gap in the knowledge of pelvic floor muscle dysfunctions, do not understand their treatment options, and are not able to identify risk factors for these disorders.
Keywords: knowledge, pelvic floor, urinary incontinence, systematic review
Abstract
Resumo
Objetivos Nós investigamos se as mulheres possuem adequado nível de conhecimento sobre as principais disfunções do assoalho pélvico (incontinência urinária – IU, incontinência fecal – IF, e prolapso de órgãos pélvicos – POP).
Fontes de dados Uma revisão sistemática foi realizada nas bases de dados MEDLINE, PEDro, CENTRAL e Cochrane com publicações até abril de 2018.
Seleção dos estudos Foram triados 3.125 estudos. A metanálise não foi possível devido a heterogeneidade dos desfechos analisados e a diversidade de instrumentos para aferir o conhecimento. A qualidade dos artigos incluídos na análise foi avaliada pela escala de Newcastle-Ottawa (NOS) adaptada para estudos transversais.
Extração de dados Dois autores fizeram a extração em uma planilha previamente testada.
Síntese de dados Dezenove estudos foram incluídos, totalizando 11.512 mulheres. A NOS apresentou um score de 6 (total = 10) na maioria dos estudos (n = 11). Para a avaliação do conhecimento do assoalho pélvico, questionários validados e testados de forma piloto foram empregados. Alguns estudos foram estratificados segundo raça, idade, ou minorias. Encontrou-se baixo a moderado nível de conhecimento e/ou percepção sobre as disfunções do assoalho pélvico. O mais usado foi o prolapse and incontinence knowledge questionnaire (PIKQ) (n = 5). A IU foi a disfunção pélvica mais investigada, e os fatores de risco mais importantes associados com a falta de conhecimento foram: etnicidade afro-americana (n = 3), nível baixo educacional (n = 5), baixo acesso a informação (n = 5), e status socioeconômico (n = 3).
Conclusão A maioria das mulheres leigas tem uma lacuna de conhecimento sobre as disfunções do assoalho pélvico, baixo conhecimento sobre opções de tratamento e sobre os fatores de risco para essas disfunções.
Palavras-chave: conhecimento, assoalho pélvico, incontinência urinária, revisão sistemática
Introduction
Pelvic floor muscle (PFM) dysfunctions have a negative impact in the quality of life of many women. These dysfunctions mainly include pelvic organ prolapse (POP), urinary incontinence (UI), and fecal incontinence (FI).1 Female stress urinary incontinence and pelvic organ prolapse (POP) are prevalent conditions and are rarely associated with severe comorbidities, despite the costs and restriction caused to women's lives.2 The prevalence of POP varies from 2 (symptomatic women) to 50% o(women with clinically insignificant POP).3 Meanwhile, the prevalence of UI reaches indices varying between 10 and 58% in women living at community settings and 50 to 84% in women residing at long-permanence institutions.4 Annual health costs related to UI care in the USA exceed 16 billion dollars. Despite the prevalence and the cost for treating PFM dysfunctions, many women do not receive adequate attention. Less than 50% of incontinent women seek for medical treatment.2 Pelvic floor muscle treatment (PFMT), bladder training, and other conservative approaches are considered the first line of treatment for women who suffer PFM dysfunctions. However, many of these women do not have information or knowledge regarding conservative treatment for PFM disorders.5 There are studies that have addressed the knowledge of patients regarding these dysfunctions, but with no compiled data on this matter. This increases the chances of successful therapy, changes in life habits, and reductions on disease's symptoma.2 Thus, our study aimed to perform a systematic review of women's knowledge about the pelvic floor structures (muscles, ligaments, organs), its functions, dysfunctions, and possible conservative treatments for each disorder by measurement through surveys, questionnaires, or any available instrument within the literature.
Methods
Eligibility Criteria and Study Selection
The eligibility criteria were scientific articles and juts cross-sectional studies (cross-sectional scientifics articles) in English language that investigated women's knowledge regarding the pelvic floor (PF) functions and/or dysfunctions and possible conservative treatments for them. Studies that aimed to focus on health professionals or that were not specifically aiming to understand women's knowledge of the pelvic floor, studies involving pregnant and postpartum patients, those with qualitative designs, or quantitative studies that did not separate data according to gender were excluded from the analysis.
Information Sources and Search
The last literature search was performed on April 2018 and included studies from inception. The consulted databases were: Medline/PubMed, PEDro, Cochrane Central Register of Controlled Trials and Cochrane Database of Systematic Reviews. The overall search strategy used was (knowledge OR comprehension OR education OR education level) (urinary incontinence OR pelvic organ prolapse OR genital prolapse OR stress urinary incontinence OR urgency urinary incontinence OR mixed urinary incontinence OR cystocele OR rectocele OR apical prolapse OR uterine prolapse OR overactive bladder OR detrusor overactivity) NOT (m?n OR animal*). A detailed example of search strategy (Pubmed) is illustrated in Appendix 1.
Screening and Data Extraction
Data search was performed by authors (J. F. F. and T. D. S.), and if a study was not a common decision to include or exclude, a third author (L. G. O. B.) was included to come to a consensus. A standardized data extraction form was used to collect the following data: authors, year of publication, journal, country of origin, sample, age (years), objectives, outcome measure, and results/conclusions. Data extraction was performed by two independent raters (J. F. F. and T. D. S.).
Outcomes
The primary outcome was knowledge regarding the pelvic floor muscles, ligaments or organs, and related disorders, measured by a questionnaire that could be previously prepared (e.g. incontinence quiz, prolapse and incontinence knowledge questionnaire) or prepared by the authors (previously or not pilot-tested). Knowledge could also be assessed with or without attitude and/or practice (Knowledge, attitude, and practice - KAP) format. Answers for knowledge could be categorical or as continuous variable (e.g. score results).
Risk of Bias Assessment and Quantitative Analysis
Assessment of methodological quality was performed by the Newcastle-Ottawa Scale adapted for cross-sectional studies. This scale was originally developed to assess the quality of observational studies and contains eight items that assesses three domains: selection, comparability and outcome. The score was divided into: good quality (3–5 stars in selection, 1–2 stars in comparability, 2–3 outcome), fair quality (2 stars in selection, 1–2 in comparability and 2–3 in outcome) and poor quality (0–1 star in selection, 0 star in comparability and 0–1 star in outcome).6 7
As data were extracted and described, heterogeneity between the outcomes did not reach possibility for pooling data and performing subgroup analysis or metanalysis. Results were displayed in tables in a synthesized format.
Results
Characteristics of the Selected Studies and Newcastle-Ottawa Scale Quality Assessment
Figure 1 shows all the pathways for this systematic review. Database searches identified a total of 3,125 studies with no duplicates, and after excluding title and abstract, 68 studies remained for screening. The reasons for exclusion are explained in the flowchart. Despite having found 19 articles for data extraction, some aspects of these studies were highly heterogeneous, such as sampling, methods of investigating the subjects' knowledge, and knowledge as primary outcome.
Fig. 1.
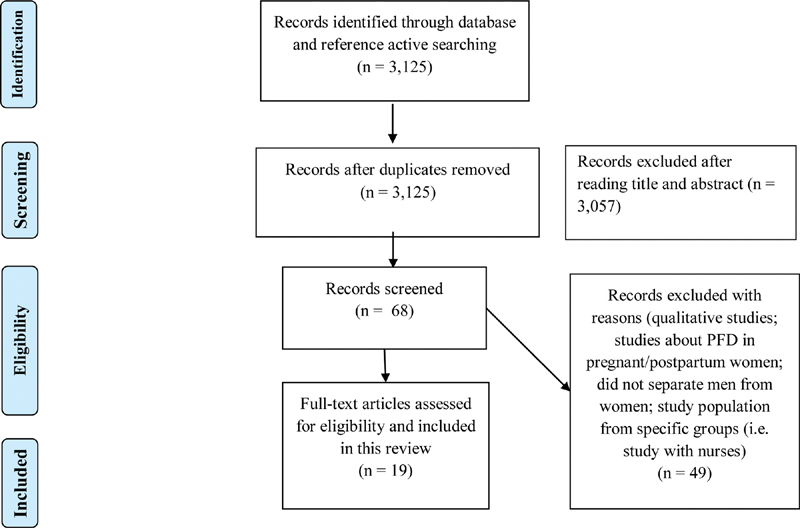
PRISMA flow diagram for the selected studies. Abbreviations: PRISMA, preferred reporting items for systematic reviews and meta-analyses; PFD, pelvic floor disorders.
Almost all studies were cross-sectional,8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 except for one pilot study26 that included a systematic review. Most of the studies were from United States (n = 8) and regarding the time period of the studies, 7 studies did not inform the time period of data collection,11 13 16 19 20 25 26 and the others informed different durations (from 3 weeks to 21 months).8 9 10 12 14 15 17 18 21 22 23 24 From these retrieved studies, a total of 11,512 women were included, with a mean age varying from 17 to 77 years (Table 1). Some studies focused only on UI,10 15 19 22 25 26 while other studies investigated other pelvic floor disorders (PFDs), pelvic floor function (PFF) or pelvic floor symptom (PFS),8 9 11 12 14 such as POP.18 Regarding the NOS quality assessment, most of the studies scored 6 (n = 11) on a scale varying from 0–10. The maximum score obtained by the studies in the present review was 7 (n = 4), 3 studies were classified with score 5 (fair quality), and only 1 article with a score of 3 (Table 2).
Table 1. General characteristics of the selected studies.
| References | Study Design/Period | Country | Sample (n) | Mean age ± SD (range) | Objectives |
|---|---|---|---|---|---|
| Freitas et al (2018)8 | CS/From January 2016 to October 2017 | Brazil | 133 | 53.3 (13.8) | To assess the level of knowledge about PFMs and the relationships between PFM knowledge and the ability to contract the PFMs, PFM strength, and prevalence of UI. |
| Arbuckle et al (2018)9 | CS/From August 2015 to June 2016 | United States of America | 216 | 17 ± 2.1 (14–17; 18–21) | To determine the prevalence and awareness of pelvic floor disorder (PFD) symptoms among adolescent females. Patient awareness of these disorders and awareness of pregnancy as a risk factor for PFD were also investigated |
| Cardoso et al (2018)10 | CS/March–June 2016 | Brazil | 118 | 21.6 ± 2.7 | To evaluate the prevalence of UI in female athletes practicing high-impact sports and its association with knowledge, attitude, and practice (KAP). |
| Neels et al (2016)11 | CS/NI | Belgium | 212 | 21.6 (18–27) | To evaluate the knowledge of PFF in young nulliparous women. |
| Parden et al (2016)12 | CS/2014–2015 | United States of America | 1092 | 23.5 ± 3.1 (19–30) | To characterize lower urinary tract and PFS prevalence, awareness of these symptoms in women in general and in their family members |
| Dunivan et al (2015)13 | CS/NI | Mexico | 144 | 77.7 ± 9.1 (55–90) | To evaluate knowledge about UI and POP among elder southwestern American-Indian women and to assess knowledge by comparing questionnaire scores of these American-Indian women to historic controls. |
| Mandimika et al. (2015)14 | CS/Febr2010–Aug2011 | United States of America | 416 | 52.5 ± 18.0; 38.3 ± 15.2; 50.2 ± 17.5 (19–98) | To compare PFD knowledge among women of different racial/ethnic groups, focusing on aspects of knowledge that are more likely to influence patient behavior, including PFD risk factors and treatment options. |
| Day et al (2014)26 | PS/NI | Ireland | 36 | NI – included 50+ | To describe community-dwelling Irish women's knowledge of UI. |
| Perera et al (2014)15 | CS/3 weeks | Sri Lanka | 400 | 41.94 (21–88) | To determine the prevalence, degree of severity, identify associated factors and study the perceptions and health seeking behavior of women with SUI attending a health care facility. |
| Shrestha et al (2014)16 | CS/NI | Nepal | 4,693 | 30.0 ± 7.4 | To assess UP knowledge among married women of reproductive age and to determine the association between UP knowledge and socioeconomic characteristics. |
| Mandimika et al. (2014)17 | CS/ Feb 2010–Aug 2011 | United States of America | 431 | 49.2 ± 17.9 (19–98) | To investigate baseline knowledge and demographic factors associated with a lack of knowledge about UI and POP. |
| Good et al (2013)18 | CS/ May2011–Aug 2012 | United States of America | 213 | 58.9 ± 14.1 | To describe patient knowledge about POP diagnosis and treatment, and patient attitudes regarding the uterus in women seeking care for POP symptoms. |
| Morhason-Bello et al (2012)19 | CS/NI | Nigeria | 1,955 | 34.8 (15–65) | To describe the perceived causes of UI and factors associated with awareness of causes of UI among women in the community. |
| Kang (2009)20 | CS/NI | Korea | 182 | 51.2 | To explore knowledge and attitudes about UI among Korean-American women with incontinence and provide initial information. |
| Shah et al (2008)21 | CS/ March–December 2006 | United States of America | 126 | 35.7 | To assess the knowledge of UI and POP of white women versus non-white women. |
| Wong et al (2006)22 | CS/3 months | China | 540 | (17–77) | To assess the prevalence, knowledge, and behavior of the search for treatment of UI by Chinese women. |
| Kubik et al (2004)24 | CS/May2002–Febr2003 | United States of America | 212 | (35–80) | To investigate if UI knowledge is different between white and minority groups, and if there is an association between SES and UI knowledge, and if SES explains differences in UI knowledge between white and minority race/ethnic groups. |
| Kim et al (2004)23 | CS/ Dec2002–Jan2003 | Korea | 276 | (55–97) | To examine the prevalence of UI and UI-related knowledge among community-dwelling Korean women aged 55 and over. |
| Kubik et al (2004)24 | CS/May2002–Febr2003 | United States of America | 212 | (35–80) | To investigate if UI knowledge is different between white and minority groups, if there is an association between SES and UI knowledge, and if SES explains differences in UI knowledge between white and minority race/ethnic groups. |
Abbreviations: BT, bladder training; CS, cross-sectional; FI, fecal incontinence; NI, not informed; PF, pelvic floor; PFDs, pelvic floor disorders; PFEs, pelvic floor exercises; PFF, pelvic floor function; PFMT, pelvic floor muscle training; PFM, pelvic floor muscle; PFS, pelvic floor symptoms; PS, pilot study; POP, pelvic organ prolapse; SES, socioeconomic status; SUI, stress urinary incontinence; UI, urinary incontinence; UP, uterine prolapsed; KAP, knowledge, attitude, and practice.
Table 2. Methodological quality (as per Newcastle-Ottawa scale), independent variable(s), instruments, and main results of selected studies.
| References | Quality | Independent Variables | Questionnaires | Results |
|---|---|---|---|---|
| Freitas et al (2018)8 | Selection: ✸✸✸ Comparability: ✸ Outcome: ✸✸ |
Knowledge/ PFM | Designed questionnaire but no information if pilot-tested; ICIQ-UI-SF | Most of the women presented no PFM knowledge, with a mean total score of 0.48 (±0.97). The ICIQ-UISF mean score was 7.1 (±6.8). There were weak correlations between PFM knowledge and age (r −0.2044/ p = 0.01), and PFM knowledge and parity (r −0.19568/p = 0.02). Pelvic floor muscle knowledge was higher among women with higher education levels (p = 0.0012) and those who had previously performed PFM training (p < 0.001). |
| Arbuckle et al (2018)9 | Selection: ✸ Comparability: ✸ Outcome: ✸ |
Awareness; PFD | ISI-P; FISI; ISI-2; POPDI-6; Designed questionnaire but no information if pilot-tested | The majority of respondents had at least heard about UI and FI (62.9%). The prevalence of any UI was 31.5 %. Approximately 29% of adolescents reported an interest in learning more about pelvic floor disorders. Early education regarding PFS may lead to prevention or empowerment to seek treatment as adolescents age. |
| Cardoso et al (2018)10 | Selection: ✸✸✸✸ Comparability: ✸ Outcome: ✸✸ |
IU; KAP | KAP; ICIQ-SF; QOL; Designed and pilot-tested questionnaire | The prevalence of UI in 118 athletes was 70% (82). Regarding the KAP survey, 31% of the athletes (37) demonstrated adequate knowledge, 53% (63) adequate attitude, and zero adequate practice. Athletes with adequate knowledge were 57% less likely to develop UI. |
| Neels et al (2016)11 | Selection: ✸✸✸ Comparability: ✸ Outcome: ✸ |
Knowledge of PFF | Designed and pilot-tested questionnaire | Using a VAS scale (0–10), the women rated their knowledge about the pelvic floor as a mean of 2.4 (SD 2.01). A total of 93% of the women were insufficiently informed and requested more information; 25% had concerns about developing UI, and 14% about FI. Many of the women were unaware what pelvic floor training meant. |
| Parden et al (2016)12 | Selection: ✸✸✸ Comparability: ✸ Outcome: ✸✸ |
PFS (UI, POP, FI, PFS's knowledge) | Designed questionnaire but no information if pilot-tested | There was no difference between groups in awareness of family members with UI, FI, or POP symptoms (p ≥ 0.24). Young women were more likely to have received education regarding UI; (aOR 2.6, 95% CI 1.8–3.6), FI (aOR, 3.3; 95% CI, 2.2–4.8), POP (aOR, 2.9; 95% CI, 2.1–4.2), and have greater understanding regarding the causes of UI (aOR, 2.9; 95% CI, 1.7–4.8), FI (aOR, 1.6; 95% CI, 1.1–2.3), and POP (aOR, 1.9; 95% CI, 1.3–2.9). |
| Dunivan et al (2015)13 | Selection: ✸✸✸ Comparability: ✸ Outcome: ✸ |
UI, POP's Knowledge | PIKQ; BICS-Q | The mean (SD) for PIKQ of UI score was 6.6 (3.0) (similar to historic gynecology controls 6.8 [3.3], p = 0.49), and the mean (SD) for PIKQ on POP score was 5.4 (2.9) (better than historic gynecology controls 3.6 [3.2], p < 0.01). |
| Mandimika et al (2015)14 | Selection: ✸✸✸ Comparability: ✸ Outcome: ✸✸✸ |
PFD's Knowledge stratified by race | PIKQ | African-American women presented higher odds for lack of knowledge in UI and POP etiology (aOR 3.05 95%CI [1.70–5.47] and aOR 2.15 95%CI [1.18–3.91], respectively) but no difference with regard to UI and POP diagnosis. |
| Day et al (2014)26 | Selection: ✸✸ Comparability: ✸ Outcome: ✸✸ |
UI's Knowledge | UIK | Participants had poor knowledge of UI, especially in relation to risk, prevention, treatment, and management factors. Less than 20% of the participants indicated they had been given information on bladder and bowel health issues |
| Perera et al (2014)15 | Selection: ✸✸✸ Comparability: ✸ Outcome: ✸✸ |
SUI; Perceptions and Health seeking behavior | Designed and pilot-tested questionnaire | Stress urinary incontinence was perceived as an illness by 210 (52.5%) subjects. Stress urinary incontinence was significantly associated with pregnancy, parity, vaginal delivery, complicated labor, diabetes mellitus, chronic cough, constipation, and fecal incontinence (p < 0.05). |
| Shrestha et al (2014)16 | Selection: ✸✸✸ Comparability: ✸ Outcome: ✸✸ |
UP's Knowledge | Designed and no information if pilot-tested | Fifty-three percent had never heard about UP. Among women who had heard about UP, 37.5% had satisfactory knowledge. Any knowledge about UP was associated with both urban and rural settings, age group, and education level. However, satisfactory knowledge about UP was associated with administrative region, ecological zones, caste/ethnic group, and age group of women |
| Mandimika et al (2014)17 | Selection: ✸✸✸ Comparability: ✸ Outcome: ✸✸ |
UI; POP | PIKQ | There is a global lack of knowledge about UI and POP among community-dwelling women, with more pronounced knowledge gaps among nonwhite women. |
| Good et al (2013)18 | Selection: ✸✸ Comparability: ✸ Outcome: ✸✸✸ |
POP's Knowledge | Designed and no information if pilot-tested | Prolapse-related knowledge is low in women seeking care for prolapse symptoms. |
| Morhason-Bello et al (2012)19 | Selection: ✸✸✸ Comparability: ✸ Outcome: ✸✸ |
UI | Designed and no information if pilot-tested | There was a lower odd of awareness of the UI etiology among women less than 30 years, with lower level of education, from rural areas, with five or more children and without history of urine leakage. |
| Kang (2009)20 | Selection: ✸✸✸ Comparability: ✸ Outcome: ✸✸ |
IU; Knowledge | Incontinence quiz | Results suggest that Korean-American women are less knowledgeable and have more negative attitudes toward UI than the general population. |
| Shah et al (2008)21 | Selection: ✸✸✸ Comparability: ✸ Outcome: ✸✸ |
UI; POP | PIKQ | Punctuation mean for white women was higher than non-white at UI scale (p =.019), but not at POP scale (p =.354). Regardless of race, both groups had a higher knowledge for UI than for POP. |
| Wong et al (2006)22 | Selection: ✸✸✸✸ Comparability: ✸ Outcome: ✸✸ |
UI | UDI-6/ IIQ-7 | A total of 78.3% of the interviewed women did not know that UI is a disease, and 60.6% of them thought urine loss is a normal part of the aging process. |
| Kim et al (2004)23 | Selection: ✸✸✸✸ Comparability: ✸ Outcome: ✸ |
UI's Knowledge | Questions derived from BFLUTSQ and Incontinence Quiz | More than 50% of respondents incorrectly agreed that “UI is the result of normal aging”. Only 20.9% knew that there were exercises that control urine leakage after strain. Older women who had sought treatment had higher mean score for UI-related knowledge. |
| Kubik et al (2004)24 | Selection: ✸✸✸✸ Comparability: ✸ Outcome: ✸✸ |
UI's Knowledge; SES | Incontinence Quiz | White women scored better than minority women on the incontinence quiz. Socioeconomic status explains racial differences in total UI knowledge. |
| Keller (1999)25 | Selection: ✸✸✸✸ Comparability: ✸ Outcome: ✸ |
UI's Knowledge | Incontinence Quiz | Over half of the 117 respondents incorrectly indicated that incontinence is a normal result of advanced age, almost one third of the respondents incorrectly believed that most people become incontinent by the time they reach the age of 85. |
Abbreviations: BICS-Q, barriers to incontinence care seeking questionnaire; BT, bladder training; CI, confidence interval; FI, fecal incontinence; IIQ-7, incontinence impact questionnaire short form; ICIQ-UI-SF, international consultation on incontinence questionnaire on urinary incontinence-short form; PF, pelvic floor; PFDs, pelvic floor disorders; PFC, pelvic floor complications; PFEs, pelvic floor exercises; PFF, pelvic floor function; PFS, pelvic floor symptom; PFMT, pelvic floor muscle training; PS, pilot study; PIKQ, prolapse and incontinence knowledge questionnaire; POP, pelvic organ prolapse; SD, standard deviation; SUI, stress urinary incontinence; SES, socioeconomic status; UI, urinary incontinence; UIK, urinary incontinence knowledge scale; UDI-6, urogenital distress inventory short form; UP, uterine prolapse; VAS, visual analogue scale; KAP, knowledge, attitude and practice.
There were risk factors that were mostly related to the lack of knowledge of pelvic floor (PF) such as educational level, access to information, socioeconomic status, age and race (Table 3).
Table 3. Most frequently cited risk factors for lack of knowledge of pelvic floor dysfunction.
| Variables | References |
|---|---|
| African-American ethnicity | Mandimika et al (2014, 2015),14 17 and Shah et al (2008)21 |
| Low educational level | Mandimika et al (2014),17 Good et al (2013),18 and Morhason-Bello et al (2012)19 |
| Low access to information | Neels et al (2016),11 Parden et al (2016),12 and Dunivan et al (2015)13 |
| Low socioeconomic status | Shrestha et al (2014),16 Morhason-Bello et al (2012),19 and Kubik et al (2004)24 |
Questionnaires
All selected studies have utilized validated8 9 10 13 14 17 21 22 23 24 25 26 questionnaires, developed or not by the authors.8 9 10 11 12 15 16 18 19 23 Some developed questionnaires were validated by the authors.10 11 15 Nells et al11 have validated the questionnaire with experts and non-trained volunteers, and both groups presented low interobserver variability. Perera et al15 validated their questionnaire by a pretest that analyzed the questionnaire content, and Cardoso et al10 have utilized the assessment of seven experts in the gynecology/ womens' health area by a Delphi panel to analyze the concept and relevance of the elaborated questions. The most cited questionnaires were: prolapse incontinence knowledge questionnaire (PIKQ) (n = 5), incontinence quiz (n = 4), urinary incontinence knowledge (UIK), urogenital distress inventory short form (UDI-6) and incontinence impact questionnaire short form (IIQ-7) (n = 1); Bristol female lower urinary tract symptom (BFLUTS) and UI-related questionnaire (n = 1).
Knowledge about Pelvic Floor Anatomy and Function
Four studies were included,8 9 11 12 one11 assessed the knowledge of nulliparous women regarding the pelvic floor functions. It was found that women presented some knowledge regarding some functions of the pelvic floor, such as pelvic floor structure and function, since 93% of women knew about the existence of muscles in this region, and 92% managed to locate this region. However, few of them had knowledge about the role of pelvic floor anatomy on sexual function (6.2–64.3%). Furthermore, most of them did not know how many openings exist in the female pelvic floor. It was concluded that most of the patients (81%) had never received information regarding the pelvic floor.
Arbuckle et al9 analyzed the prevalence and the knowledge of PFD in adolescents (14–21 years). They have observed that the prevalence of UI was 31.5%, and urge incontinence was present in 15.7% of the women included in the study. Regarding knowledge, only 19.5% and 5.1% of the participants had heard about POP and FI, respectively. Furthermore, discussion about PFD at schools was also low (1.9–6.5%) within this group, and 29.4% of the adolescents would want to know more about the topic. Parden et al12 have shown that even with low rates of symptoms in both groups, the adolescent women (19–24 years) and young women (25–30 years) groups had similar interest in learning more about PFD (33.9% vs 31.4%, p = 0.45). After stratifying the groups by age and educational level, it was found that, when compared to adolescents, female young adults were more prone to receive education regarding UI, FI, and POP. The same association was found for the group of women with higher education, who had significantly higher rates of willingness to receiving information (UI = 31.5% vs 8.4%, p ≤ 0.0001; FI = 24% vs 5.4%, p ≤ 0.0001; POP = 27.6% vs 8.2%, p ≤ 0.0001) while teenagers were not aware of most of pelvic dysfunctions.
Freitas et al8 have analyzed the knowledge of Brazilian women about PFM and its relationship with the capacity to contract the PFM. Most of women (55%) presented a low level of knowledge, and 79.7% did not know the PFM functions. Moreover, a low correlation between PFM knowledge and age was found (p = 0.01), and there was a statistically significant difference between the years of education and previous practice of PFMT.
Knowledge about UI
Eight studies10 15 19 20 22 23 25 26 aimed to investigate women's knowledge about UI, and all of them have shown that women had a low knowledge about UI. Most of the studies have also shown that treatment for UI and associated risk factors for UI were not fully understood by the patients, regardless of age and country of origin. Women perceived some risk factors for UI. Day et al26 and Keller25 have found that women described aging as an important factor for UI. Regarding treatment, women did not look for treatment, and the following reasons were pointed out: lack of knowledge, embarrassment, and UI seen as a minor health issue. These findings were similar to another study performed by Cardoso et al,10 in which knowledge, attitude, and practice regarding UI was investigated in high impact athletes. Despite 70% of them have complained about UI during exercise, 96% did not consider this as a problem worthy of seeking help, and none had ever told her coach about the UI.
Knowledge about POP
One study has only focused on POP.18 Good et al18 have found that American women presented a lack of knowledge regarding POP, with 44% of them scoring the questionnaire about this subject. Another study16 has focused only on uterine prolapse (UP). Shrestha et al16 have observed knowledge about UP on married women at reproductive age. Half of them have never heard about UP, and within the group that presented some knowledge about UP, only 37.5% presented a satisfactory level. Women that were living in an urban area presented more chance to have knowledge about UP, as well as higher educational level.
Knowledge about UI and POP
Two studies13 17 have analyzed UI and POP within their objectives, one of which has compared its results with those of control groups. Dunivan et al13 used a control group formed by women with PFDs, because they assumed they would have better knowledge if informed during consultations, and compared with healthy women and elderly American-Indian women. The former group presented a higher knowledge score when compared to the other groups. Mandimika et al17 found that approximately one third (32.2%) of the participants reported having a history of UI; however, only 4.6% of all women reported being treated for this condition; Also, 6% of the women reported having a problem with POP, but only 4.0% of them reported having been treated by POP. Moreover, 71.2% of the subjects lacked UI proficiency (< 80% was correct), whereas 48.1% lacked proficiency in POP knowledge (< 50% was correct). Regarding the association of risk factors with UI or POP, educational level was the only factor associated with knowledge about UI.
Knowledge about UI and POP According to Race
Some studies have related the l of treatment seeking for pelvic floor dysfunctions to minority groups. Three studies14 21 24 assessed the knowledge separating the subjects by racial groups. Mandimika et al14 found that African-American women were more prone to not having adequate knowledge about UI and the etiology and treatment of POP. Furthermore, women did not know that PFMs could be useful for treating UI. Shah et al21 identified a higher knowledge level for white women when compared with Asian, Hispanic, and African-American women. Kubik et al24 perceived that white women presented a higher score on the incontinence quiz questionnaire compared with other racial groups (6.16 ± 2.86 vs 5.46 ± 2.66, p = 0.71) (Hispanic, African-American). Furthermore, higher socioeconomic status (SES) was associated with higher incontinence quiz total score.
Discussion
This systematic review showed that women's knowledge of PFDs was very limited, and that it could be influenced by socioeconomic variables, such as racial groups. All included studies were quantitative, but this evidence was also found on qualitative studies. Anger et al27 performed a focus group of women with overactive bladder to better understand the experiences and level of understanding related to the problem. As a result, it was found that women had no understanding of the cause of overactive bladder, chronicity, and the rationale for various diagnostic tests.
Women's beliefs may also give them a chance to reflect about the cause of their disease. Melville et al28 have found that 50% of women suggested an inherent problem with the pelvic floor or bladder as a cause for their symptoms. Obviously, knowledge is connected to the educational and socioeconomic level; thus, cultural aspects are not only the main factor influencing beliefs.
Race is a variable with a possible effect modification. Another point for discussion is that the percentage of surgeries performed for PFDs may be different among racial groups, and this may influence the prevalence of PFDs. If we know that PFDs may differ among racial groups, it will be possible to promote aims focusing on education for this population.14 Further cohort studies are necessary to understand this variable as we know that cross-sectional studies cannot establish the route of causality between one variable and the outcome.
Only half or less of women with UI discusses their condition with a health professional.29 Even when health professionals are consulted, there are surprisingly low rates of treatment of women with symptoms of UI.30 In studies that investigate the reasons why women do not seek treatment for UI, several other themes were identified: shame, belief that incontinence is part of the normal aging process, sensation that they can handle the problem on their own, and low expectations of benefits with treatment.31 32 33 34 This information is related with the findings of this review, since the studies that focus on the lack of knowledge have identified the lack of search for treatment due to lack of knowledge, embarrassment, and because some women have considered UI as a small problem and a “normal” part of the aging process.
Jácome et al35 observed a high prevalence (30.2–35.8%) of UI in athletes; however, more than half (61.4%) of the athletes had never talked to anyone about their leakage, and 9 (20.4%) reported having discussed the problem with a friend. And when urine loss occurred, the athletes felt concerned, annoyed, frustrated, and fearful that a new activity might trigger another leakage but with no current impact on their daily lives.
It is important to highlight that patients with chronic diseases, such as overactive bladder and UI, seek different information from patients with acute illnesses, regarding diagnosis and treatments available. Furthermore, a study of patients with heart failure found that patients with good disease control have achieved better functional status, suffer less anxiety, and present fewer reports of depression and better quality of life than patients with low perceived control of disease.36
Liao et al37 administered an educational 4-hour program with pelvic muscle training to a cohort of 55 women with UI in Taiwan. The researchers applied a knowledge questionnaire containing 20 statements of yes/no questions as well as an index of severity of UI and self-perceived severity of UI to patients before and 8 weeks after the educational intervention. The participants showed significant improvement of knowledge scores and reported a significant decrease in the severity of UI.
In a study conducted over a decade ago, Branch et al38 found substantial gaps in knowledge about UI among community-dwelling individuals aged 65 years and concluded that levels of knowledge about UI should be increased to ensure that proper treatment and management are achieved. The lack of knowledge about the pelvic floor in women demonstrates the necessity of creating educational programs for health professionals on this topic.
Stadnicka et al39 aimed to perform a prophylactic program for Stress Urinary Incontinence (SUI). Through literature review and results of their own investigations, it is concluded that a program for prevention of SUI should include mainly: [1] preparation of health professionals to spread health education among women in the prevention of SUI; [2] the preparation of appropriate educational materials in the form of brochures, leaflets, posters of information on symptoms, causes and prevention of UI indicates that health care available to all women when the disease is suspected or institutions already present, [3] the spread problems related to SUI in the means of mass communication that provide information to a wide audience in order to raise awareness about the significance of this social problem and also in order to break the stereotype associated with this disease, [4] clarifying about the importance of performing exercises for the PFM during pregnancy, and menopause to maintain its own function, and [5] focus on the possibilities of changes in factors that predispose SUI in order to reduce or eliminate these factors.
According to Herbruck,40 the costs of UI are financially and socially significant to those who are living with its effects. The determination of possible modifiable factors that cause changes in the UI and in the PF is complicated. A reasonable starting point could be counseling patients about the importance of education and awareness of the PF to improve their quality of life. In addition, health professionals in general should get closely involved to the theme in order to provide quality information that improves with reverse in preventive and rehabilitative care female UI. These data confirm the findings of Kang,20 that suggest that the absence of a sharing decision-making process may contribute for an inadequate interpretation of patient symptoms.
The limitations of this review are, mainly, the heterogeneity of measuring knowledge, the non-stratification of baseline sociodemographic variables, such as education level, and the response bias that is implicit to any study that assesses knowledge; maybe these percentages are worse than the findings from each study. It should be highlighted that the research on the PF knowledge had a specific validated questionnaire, and that the interviews between professional and patients were more objective; thus, future studies could reproduce them.
The knowledge about PFM is important for women to know their own bodies, easing comprehension about their orientations and proposed treatment by health professionals. Communication and information are essential for the treatment of patients with PFDs. Correct information is important to obtain consent from patients about proposed therapy during treatment, the increase of participation, reduction of anxiety, increase of knowledge about the disease, and the satisfaction of the patients with the obtained results, which might increase the chances of therapeutic success. This knowledge about the PF showed to be increased through several programs, such as PFMT, behavioral modification, and educational workshops by physicians, physiotherapists and/or nurses.
According to this review, there is a lack of data on the knowledge of adult women regarding to the physiological role of the PF and the ability to contract the PFM. It is important that women receive information on the PFM function and dysfunction. It is also essential to establish models of preventive and rehabilitation activities to be included in women's care in all health care levels.
Conclusion
Knowledge of the PFM is necessary for the understanding of women over their own bodies, facilitating the understanding of the guidelines and treatments offered by health professionals. Communication and information are essential in the treatment of patients with PFDs. The correct information is important in obtaining the patient's consent on the proposed therapy in treatment, increasing their participation, reducing anxiety, providing knowledge about the disease and assessing the patients' satisfaction with the results.
Footnotes
Conflicts of Interest The authors declare that there are no conflicts of interest.
Appendix 1 Search strategy on PubMed.
((“knowledge”[MeSH Terms] OR “knowledge”[All Fields]) OR (“comprehension”[MeSH Terms] OR “comprehension”[All Fields]) OR (“education”[Subheading] OR “education”[All Fields] OR “educational status”[MeSH Terms] OR (“educational”[All Fields] AND “status”[All Fields]) OR “educational status”[All Fields] OR “education”[All Fields] OR “education”[MeSH Terms]) OR “education level”[All Fields]) AND (“urinary incontinence”[All Fields] OR “pelvic organ prolapse”[All Fields] OR “genital prolapse”[All Fields] OR “stress urinary incontinence”[All Fields] OR (urgence[All Fields] AND (“urinary incontinence”[MeSH Terms] OR (“urinary”[All Fields] AND “incontinence”[All Fields]) OR “urinary incontinence”[All Fields])) OR “mixed urinary incontinence”[All Fields] OR (“cystocoele”[All Fields] OR “cystocele”[MeSH Terms] OR “cystocele”[All Fields]) OR (“rectocoele”[All Fields] OR “rectocele”[MeSH Terms] OR “rectocele”[All Fields]) OR “apical prolapse”[All Fields] OR “uterine prolapse”[All Fields] OR “overactive bladder”[All Fields] OR “detrusor overactivity”[All Fields]) NOT (m?n[All Fields] OR (animal[All Fields] OR animal'[All Fields] OR animal'naia[All Fields] OR animal'no[All Fields] OR animal's[All Fields] OR animal1[All Fields] OR animal2[All Fields] OR animal80[All Fields] OR animala[All Fields] OR animalae[All Fields] OR animaland[All Fields] OR animalarial[All Fields] OR animalario[All Fields] OR animalarium[All Fields] OR animalas[All Fields] OR animalbase[All Fields] OR animalbehavior[All Fields] OR animalbehaviorclinic[All Fields] OR animalbehavior[All Fields] OR animalbiology[All Fields] OR animalcare[All Fields] OR animalcentric[All Fields] OR animalcentro[All Fields] OR animalci[All Fields] OR animalclinicofregina[All Fields] OR animalcognition[All Fields] OR animalcompassionfoundation[All Fields] OR animalconcepts[All Fields] OR animalconsultants[All Fields] OR animalcula[All Fields] OR animalcular[All Fields] OR animalcule[All Fields] OR animalcules[All Fields] OR animalcules'[All Fields] OR animalculi[All Fields] OR animalculi'[All Fields] OR animalculis[All Fields] OR animalculos[All Fields] OR animald[All Fields] OR animaldairy[All Fields] OR animalde[All Fields] OR animaldentalcenter[All Fields] OR animaldentalservices[All Fields] OR animaldepartamento[All Fields] OR animalderived[All Fields] OR animaldocfox[All Fields] OR animale[All Fields] OR animale'[All Fields] OR animalearn[All Fields] OR animaleau[All Fields] OR animaledu[All Fields] OR animalefaculte[All Fields] OR animalele[All Fields] OR animalelimogesfrance[All Fields] OR animalelor[All Fields] OR animalem[All Fields] OR animalemergency[All Fields] OR animalen[All Fields] OR animalendocrine[All Fields] OR animaleolor[All Fields] OR animaler[All Fields] OR animalerc[All Fields] OR animalerie[All Fields] OR animaleries[All Fields] OR animales[All Fields] OR animales'[All Fields] OR animalessin[All Fields] OR animaletoulouse[All Fields] OR animaletti[All Fields] OR animaleuniversite[All Fields] OR animalexp[All Fields] OR animaleyecare[All Fields] OR animaleyedoctor[All Fields] OR animalfacultad[All Fields] OR animalfeed[All Fields] OR animalfeeds[All Fields] OR animalfree[All Fields] OR animalgenome[All Fields] OR animalgesic[All Fields] OR animalgrupo[All Fields] OR animalh[All Fields] OR animalhealth[All Fields] OR animalhealthaustralia[All Fields] OR animalhealthireland[All Fields] OR animali[All Fields] OR animalia[All Fields] OR animalian[All Fields] OR animalibus[All Fields] OR animalibus'[All Fields] OR animalic[All Fields] OR animalien[All Fields] OR animalier[All Fields] OR animaliere[All Fields] OR animalieres[All Fields] OR animalies[All Fields] OR animaliieiu[All Fields] OR animalin[All Fields] OR animalinia[All Fields] OR animalinla[All Fields] OR animalinsides[All Fields] OR animalinstituto[All Fields] OR animalis[All Fields] OR animalisante[All Fields] OR animalisation[All Fields] OR animalische[All Fields] OR animalischem[All Fields] OR animalischen[All Fields] OR animalischer[All Fields] OR animalises[All Fields] OR animalisierte[All Fields] OR animalism[All Fields] OR animalisssp[All Fields] OR animalistic[All Fields] OR animalistol[All Fields] OR animalists[All Fields] OR animalite[All Fields] OR animality[All Fields] OR animalium[All Fields] OR animalium'[All Fields] OR animaliumque[All Fields] OR animalivore[All Fields] OR animalivores[All Fields] OR animalivorous[All Fields] OR animalization[All Fields] OR animalizatsii[All Fields] OR animalize[All Fields] OR animalized[All Fields] OR animalizes[All Fields] OR animalizing[All Fields] OR animalizing'[All Fields] OR animalizzante[All Fields] OR animalkulismus[All Fields] OR animall[All Fields] OR animallectindb[All Fields] OR animallectindb'[All Fields] OR animallee[All Fields] OR animallevel[All Fields] OR animallifesolutions[All Fields] OR animalloimia[All Fields] OR animalls[All Fields] OR animally[All Fields] OR animalmedical[All Fields] OR animalmedicine[All Fields] OR animalmodel[All Fields] OR animalmodels[All Fields] OR animalmost[All Fields] OR animalne[All Fields] OR animalneho[All Fields] OR animalness[All Fields] OR animalni[All Fields] OR animalnich[All Fields] OR animalnih[All Fields] OR animalniho[All Fields] OR animalnim[All Fields] OR animalnl[All Fields] OR animalnu[All Fields] OR animalny[All Fields] OR animalnych[All Fields] OR animaloid[All Fields] OR animalomics[All Fields] OR animaloris[All Fields] OR animalous[All Fields] OR animalpathogene[All Fields] OR animalpathogenic[All Fields] OR animalphysio[All Fields] OR animalproductivity[All Fields] OR animalqtldb[All Fields] OR animalrelated[All Fields] OR animalreproduction[All Fields] OR animals[All Fields] OR animals'[All Fields] OR animals'behavior[All Fields] OR animals'behavioral[All Fields] OR animals'equally[All Fields] OR animals'fibrinolytic[All Fields] OR animals'hepatic[All Fields] OR animals'hips[All Fields] OR animals'life[All Fields] OR animals'motor[All Fields] OR animals's[All Fields] OR animals'serum[All Fields] OR animals'skin[All Fields] OR animals'suboriferous[All Fields] OR animals2[All Fields] OR animals2,3[All Fields] OR animals37[All Fields] OR animalsa1[All Fields] OR animalsand[All Fields] OR animalsaustralia[All Fields] OR animalscan[All Fields] OR animalschangchun[All Fields] OR animalscience[All Fields] OR animalsciences[All Fields] OR animalscommunities[All Fields] OR animalsdepartment[All Fields] OR animalses[All Fields] OR animalsethical[All Fields] OR animalsha[All Fields] OR animalsin[All Fields] OR animalsinstitute[All Fields] OR animalsk[All Fields] OR animalskawasaki[All Fields] OR animalskawasakijapan[All Fields] OR animalske[All Fields] OR animalskinallergy[All Fields] OR animalsmin[All Fields] OR animalspecialtycenter[All Fields] OR animalspecies[All Fields] OR animalsperformance[All Fields] OR animalsr[All Fields] OR animalsroyal[All Fields] OR animalss[All Fields] OR animalsschool[All Fields] OR animalssix[All Fields] OR animalssun[All Fields] OR animalsthe[All Fields] OR animalsthis[All Fields] OR animalstreated[All Fields] OR animalsu[All Fields] OR animalsunder[All Fields] OR animalsversus[All Fields] OR animalswere[All Fields] OR animalswild[All Fields] OR animaltfdb[All Fields] OR animalthe[All Fields] OR animaltissues[All Fields] OR animaltracker[All Fields] OR animalu[All Fields] OR animalul[All Fields] OR animalultrasound[All Fields] OR animalului[All Fields] OR animaluniversidade[All Fields] OR animalvegetative[All Fields] OR animalviren[All Fields] OR animalward[All Fields] OR animalwards[All Fields] OR animalwelfare[All Fields] OR animalwere[All Fields] OR animalwith[All Fields] OR animalx[All Fields] OR animalx100[All Fields] OR animalxside[All Fields] OR animaly[All Fields] OR animalytics[All Fields] OR animalzellen[All Fields]))
References
- 1.Haylen B T, de Ridder D, Freeman R Met al. An International Urogynecological Association (IUGA)/International Continence Society (ICS) joint report on the terminology for female pelvic floor dysfunction Neurourol Urodyn 201029014–20.. Doi: 10.1002/nau.20798 [DOI] [PubMed] [Google Scholar]
- 2.Shah A D, Massagli M P, Kohli N, Rajan S S, Braaten K P, Hoyte L.A reliable, valid instrument to assess patient knowledge about urinary incontinence and pelvic organ prolapse Int Urogynecol J Pelvic Floor Dysfunct 200819091283–1289.. Doi: 10.1007/s00192-008-0631-x [DOI] [PubMed] [Google Scholar]
- 3.Samuelsson E C, Victor F T, Tibblin G, Svärdsudd K F.Signs of genital prolapse in a Swedish population of women 20 to 59 years of age and possible related factors Am J Obstet Gynecol 1999180(2 Pt 1):299–305.. Doi: 10.1016/S0002-9378(99)70203-6 [DOI] [PubMed] [Google Scholar]
- 4.Fultz N H, Herzog A R. Epidemiology of urinary symptoms in the geriatric population. Urol Clin North Am. 1996;23(01):1–10. doi: 10.1016/s0094-0143(05)70288-3. [DOI] [PubMed] [Google Scholar]
- 5.Geoffrion R, Robert M, Ross Set al. Evaluating patient learning after an educational program for women with incontinence and pelvic organ prolapse Int Urogynecol J Pelvic Floor Dysfunct 200920101243–1252.. Doi: 10.1007/s00192-009-0919-5 [DOI] [PubMed] [Google Scholar]
- 6.Herzog R, Álvarez-Pasquin M J, Díaz C, Del Barrio J L, Estrada J M, Gil Á.Are healthcare workers' intentions to vaccinate related to their knowledge, beliefs and attitudes? A systematic review BMC Public Health 201313154. Doi: 10.1186/1471-2458-13-154 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Stang A.Critical evaluation of the Newcastle-Ottawa scale for the assessment of the quality of nonrandomized studies in meta-analyses Eur J Epidemiol 20102509603–605.. Doi: 10.1007/s10654-010-9491-z [DOI] [PubMed] [Google Scholar]
- 8.de Freitas L M, Bø K, Fernandes A CNL, Uechi N, Duarte T B, Ferreira C HJ.Pelvic floor muscle knowledge and relationship with muscle strength in Brazilian women: a cross-sectional studyInt Urogynecol J Pelvic Floor Dysfunct2018;••• Doi: 10.1007/s00192-018-3824-y [DOI] [PubMed]
- 9.Arbuckle J L, Parden A M, Hoover K, Griffin R L, Richter H E.Prevalence and awareness of pelvic floor disorders in adolescent females seeking gynecologic careJ Pediatr Adolesc Gynecol2018;••• Doi: 10.1016/j.jpag.2018.11.010 [DOI] [PubMed]
- 10.Cardoso A MB, Lima C ROP, Ferreira C WS.Prevalence of urinary incontinence in high-impact sports athletes and their association with knowledge, attitude and practice about this dysfunction Eur J Sport Sci 201818101405–1412.. Doi: 10.1080/17461391.2018.1496146 [DOI] [PubMed] [Google Scholar]
- 11.Neels H, Wyndaele J J, Tjalma W A, De Wachter S, Wyndaele M, Vermandel A.Knowledge of the pelvic floor in nulliparous women J Phys Ther Sci 201628051524–1533.. Doi: 10.1589/jpts.28.1524 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Parden A M, Griffin R L, Hoover Ket al. Prevalence, awareness, and understanding of pelvic floor disorders in adolescent and young women Female Pelvic Med Reconstr Surg 20162205346–354.. Doi: 10.1097/SPV.0000000000000287 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Dunivan G C, Komesu Y M, Cichowski S B, Lowery C, Anger J T, Rogers R G.Elder American Indian women's knowledge of pelvic floor disorders and barriers to seeking care Female Pelvic Med Reconstr Surg 2015210134–38.. Doi: 10.1097/SPV.0000000000000103 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Mandimika C L, Murk W, Mcpencow A Met al. Racial disparities in knowledge of pelvic floor disorders among community-dwelling women Female Pelvic Med Reconstr Surg 20152105287–292.. Doi: 10.1097/SPV.0000000000000182 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Perera J, Kirthinanda D S, Wijeratne S, Wickramarachchi T K.Descriptive cross sectional study on prevalence, perceptions, predisposing factors and health seeking behaviour of women with stress urinary incontinence BMC Womens Health 20141478. Doi: 10.1186/1472-6874-14-78 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Shrestha B, Devkota B, Khadka B Bet al. Knowledge on uterine prolapse among married women of reproductive age in Nepal Int J Womens Health 20146771–779.. Doi: 10.2147/IJWH.S65508 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Mandimika C L, Murk W, Mühlhäuser McPencow Aet al. Knowledge of pelvic floor disorders in a population of community-dwelling women Am J Obstet Gynecol 2014210021650–1.65E11.. Doi: 10.1016/j.ajog.2013.10.011 [DOI] [PubMed] [Google Scholar]
- 18.Good M M, Korbly N, Kassis N Cet al. Prolapse-related knowledge and attitudes toward the uterus in women with pelvic organ prolapse symptoms Am J Obstet Gynecol 2013209054810–4.81E8.. Doi: 10.1016/j.ajog.2013.06.001 [DOI] [PubMed] [Google Scholar]
- 19.Morhason-Bello I O, Ojengbede O A, Adedokun B O, Okonkwo N S, Kolade C.Theories of urinary incontinence causation: aetiological descriptions by sub-Saharan African women Eur J Obstet Gynecol Reprod Biol 201216201109–112.. Doi: 10.1016/j.ejogrb.2012.01.023 [DOI] [PubMed] [Google Scholar]
- 20.Kang Y.Knowledge and attitudes about urinary incontinence among community-dwelling Korean American women J Wound Ostomy Continence Nurs 20093602194–199.. Doi: 10.1097/01.WON.0000347662.33088.c9 [DOI] [PubMed] [Google Scholar]
- 21.Shah A D, Shott S, Kohli N, Wu J M, Catlin S, Hoyte L.Do racial differences in knowledge about urogynecologic issues exist? Int Urogynecol J Pelvic Floor Dysfunct 200819101371–1378.. Doi: 10.1007/s00192-008-0639-2 [DOI] [PubMed] [Google Scholar]
- 22.Wong T, Lau B Y, Mak H L, Pang M W, Cheon C, Yip S K.Changing prevalence and knowledge of urinary incontinence among Hong Kong Chinese women Int Urogynecol J Pelvic Floor Dysfunct 20061706593–597.. Doi: 10.1007/s00192-006-0072-3 [DOI] [PubMed] [Google Scholar]
- 23.Kim J S, Lee E H, Park H C.Urinary incontinence: prevalence and knowledge among community-dwelling Korean women aged 55 and over Taehan Kanho Hakhoe Chi 20043404609–616.. Doi: 10.4040/jkan.2004.34.4.609 [DOI] [PubMed] [Google Scholar]
- 24.Kubik K, Blackwell L, Heit M.Does socioeconomic status explain racial differences in urinary incontinence knowledge? Am J Obstet Gynecol 200419101188–193.. Doi: 10.1016/j.ajog.2004.03.084 [DOI] [PubMed] [Google Scholar]
- 25.Keller S L. Urinary incontinence: occurrence, knowledge, and attitudes among women aged 55 and older in a rural Midwestern setting. J Wound Ostomy Continence Nurs. 1999;26(01):30–38. doi: 10.1016/s1071-5754(99)90008-6. [DOI] [PubMed] [Google Scholar]
- 26.Day M R, Patricia L W, Loughran S, O'Sullivan E.Community-dwelling women's knowledge of urinary incontinence Br J Community Nurs 20141911534–538.. Doi: 10.12968/bjcn.2014.19.11.534 [DOI] [PubMed] [Google Scholar]
- 27.Anger J T, Nissim H A, Le T Xet al. Women's experience with severe overactive bladder symptoms and treatment: insight revealed from patient focus groups Neurourol Urodyn 201130071295–1299.. Doi: 10.1002/nau.21004 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Melville J L, Wagner L E, Fan M Y, Katon W J, Newton K M.Women's perceptions about the etiology of urinary incontinence J Womens Health (Larchmt) 200817071093–1098.. Doi: 10.1089/jwh.2007.0606 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Hägglund D, Walker-Engström M L, Larsson G, Leppert J.Reasons why women with long-term urinary incontinence do not seek professional help: a cross-sectional population-based cohort study Int Urogynecol J Pelvic Floor Dysfunct 20031405296–304., discussion 304 [DOI] [PubMed] [Google Scholar]
- 30.Melville J L, Newton K, Fan M Y, Katon W.Health care discussions and treatment for urinary incontinence in U.S. women Am J Obstet Gynecol 200619403729–737.. Doi: 10.1016/j.ajog.2005.09.011 [DOI] [PubMed] [Google Scholar]
- 31.Hägglund D, Walker-Engström M L, Larsson G, Leppert J.Quality of life and seeking help in women with urinary incontinence Acta Obstet Gynecol Scand 200180111051–1055.. Doi: 10.1034/j.1600-0412.2001.801117.x [PubMed] [Google Scholar]
- 32.Holst K, Wilson P D. The prevalence of female urinary incontinence and reasons for not seeking treatment. N Z Med J. 1988;101(857):756–758. [PubMed] [Google Scholar]
- 33.Saleh N, Bener A, Khenyab N, Al-Mansori Z, Al Muraikhi A.Prevalence, awareness and determinants of health care-seeking behaviour for urinary incontinence in Qatari women: a neglected problem? Maturitas 2005500158–65.. Doi: 10.1016/j.maturitas.2004.04.003 [DOI] [PubMed] [Google Scholar]
- 34.Dugan E, Roberts C P, Cohen S Jet al. Why older community-dwelling adults do not discuss urinary incontinence with their primary care physicians J Am Geriatr Soc 20014904462–465.. Doi: 10.1046/j.1532-5415.2001.49094.x [DOI] [PubMed] [Google Scholar]
- 35.Jácome C, Oliveira D, Marques A, Sá-Couto P.Prevalence and impact of urinary incontinence among female athletes Int J Gynaecol Obstet 20111140160–63.. Doi: 10.1016/j.ijgo.2011.02.004 [DOI] [PubMed] [Google Scholar]
- 36.Parker R M, Baker D W, Williams M V, Nurss J R.The test of functional health literacy in adults: a new instrument for measuring patients' literacy skills J Gen Intern Med 19951010537–541.. Doi: 10.1007/bf02640361 [DOI] [PubMed] [Google Scholar]
- 37.Liao Y M, Dougherty M C, Liou Y S, Tseng I J.Pelvic floor muscle training effect on urinary incontinence knowledge, attitudes, and severity: an experimental study Int J Nurs Stud 2006430129–37.. Doi: 10.1016/j.ijnurstu.2005.01.004 [DOI] [PubMed] [Google Scholar]
- 38.Branch L G, Walker L A, Wetle T T, DuBeau C E, Resnick N M.Urinary incontinence knowledge among community-dwelling people 65 years of age and older J Am Geriatr Soc 199442121257–1262.. Doi: 10.1111/j.1532-5415.1994.tb06507.x [DOI] [PubMed] [Google Scholar]
- 39.Stadnicka G, Iwanowicz-Palus G J, Bień A M.[A prophylactic program for strain urinary incontinence] Wiad Lek 200255(Pt 2, Suppl 1):890–894. [PubMed] [Google Scholar]
- 40.Herbruck L F.Stress urinary incontinence: prevention, management, and provider education Urol Nurs 20082803200–206., quiz 207 [PubMed] [Google Scholar]