

Abstract
Studies of life expectancy (LE) in small areas of cities are relatively common in high-income countries but rare in Latin American countries. Small-area estimation methods can help to describe and quantify inequities in LE between neighborhoods and their predictors. Our objective was to analyze the distribution and spatial patterning of LE across small areas of Ciudad Autónoma de Buenos Aires (CABA), Argentina, and its association with socioeconomic characteristics. As part of the SALURBAL project, we used georeferenced death certificates in 2015–2017 for CABA, Argentina. We used a spatial Bayesian Poisson model using the TOPALS method to estimate age- and sex-specific mortality rates. We used life tables to estimate LE at birth. We obtained data on neighborhood socioeconomic characteristics from the 2010 census and analyzed their associations. LE at birth was higher for women (median of across neighborhoods = 81.1 years) compared to men (76.7 years). We found a gap in LE of 9.3 (women) and 14.9 years (men) between areas with the highest and the lowest LE. Better socioeconomic characteristics were associated with higher LE. For example, mean differences in LE at birth in areas with highest versus lowest values of composite SES index were 2.79 years (95% CI: 2.30 to 3.28) in women and 5.61 years (95% CI: 4.98 to 6.24) in men. We found large spatial inequities in LE across neighborhoods of a large city in Latin America, highlighting the importance of place-based policies to address this gap.
Keywords: Life expectancy, Small area estimation, Urban health, Latin America
Introduction
More than 80% of the population of Latin America (LA) resides in urban areas, and this urban growth has been especially intense in the last half-century, creating both challenges and opportunities to enact public policies based on scientific findings [1, 2]. LA is also a highly unequal region, with strong residential segregation within countries and cities [3]. The interrelated process of urbanization and segregation directly impact spatial inequities in health outcomes, including mortality and life expectancy. Studies focusing on the heterogeneity of mortality and life expectancy (LE) within urban areas are more common in high-income countries but remain limited to low- and middle-income countries (LMIC) [4–7]. Moreover, much of what is known about health inequities in LA countries is based on city-level indicators [4, 8], not in small areas such as neighborhoods. Challenges for small area estimation (SAE) include the definition and operationalization of what a small area is [9], statistical noise around death counts with small populations [4, 10], and the availability of data, especially given confidentiality concerns [11]. Previous studies found wide inequities in the distribution of LE for sub-city units in LA countries [12, 13]. Although some studies have explored small area variations in LMIC using SAE methods [14, 15], there has been little examination of heterogeneity in LE within the rapidly growing cities of LMIC [16]. For this work, we use the definition of census fraction from the National Statistics Office of Argentina, a unit of analysis that we selected because of the death count required to estimate a reliable small-area estimate and its spatial delimitation used for census data collection.
Ciudad Autónoma de Buenos Aires (CABA) is the administrative and political center of Argentina, located in the Buenos Aires metropolitan area, which houses 31.9% of the national population [17]. Significant inequities in social and environmental conditions exist across the city, even though it has a relatively low illiteracy rate, high access to resources, and a lower proportion of the health-uninsured population [18]. Studies on social inequity in CABA have focused on “social maps” describing geographic variation in health and socioeconomic indicators across the city [19, 20] or have characterized multiple dimensions of the sociospatial structure of the city [21]. To our knowledge, no studies have examined variations in LE within CABA using high spatial resolution data to address neighborhood health effects.
To improve on the presence and magnitude of small-area effects on LE, we used state-of-the-art methods to (a) describe the distribution and variability of LE at birth for the period 2015–2017, (b) characterize the spatial patterning of LE across small areas, and (c) analyze its association with socioeconomic characteristics.
Methods
Study Setting and Data Sources
This is an ecological study using vital registration data from the 351 fracciones censales of CABA in 2015–2017. Fracciones censales, henceforth “small areas,” are geostatistical census units based on an average of 5000 households defined by Argentina’s National Institute of Statistics and Census (INDEC). We used georeferenced data from death registry records for CABA obtained from the Dirección General de Estadística y Censos (DGEC) for the triennium 2015 to 2017. We obtained population data from the 2010 census and population projections created by DGEC [22] for the 2010 and 2015–2017 periods, given that population distribution from the 2010 census are different from the 2010 projected population distributions (see Appendix 1 for further explanation). We obtained data for socioeconomic data for small areas from the 2010 census [17].
Mortality and Population
Death records were georeferenced to the small area level by the SALud URBana en America Latina-Urban Health in Latin America (SALURBAL) project, using street address shapefiles created by the Unidad de Sistemas de Información Geográfica of the CABA government. Among the total deaths recorded (n = 89,410) for the study period, we excluded deaths not georeferenced to the small areas (1,2%), resulting in 88,330 analyzed deaths. Finally, we aggregated death counts by small area, single-year age, and sex for the pooled period of 2015–2017.
To estimate age-specific mortality rates, we needed population denominators by small area, single-year age, and sex for 2015–2017. Because these were not available at that level for that time period, we estimated them using two sources: (a) population counts by small area, single age, and sex from the 2010 census and (b) population projection counts by comuna (the next higher administrative level with a median population of 192,677) by 5-year age group and sex, for 2010 and 2015–2017. First, we calculated the census proportion of people for each single-year age/sex/small area within each comuna using data from the 2010 census. Second, we graduated the 2010 population projections data by comuna using a penalized composite link model (PCLM) [23]. PCLM allows for the graduation (redistribution of a group, in this case, 5-year age groups into single years) of population counts assuming that the age distribution is smooth with limited assumptions [23]. Also, we employed a maximum open-ended age group of 103 years for women and 100 years for men, based on a comparison with the single-year populations available from the 2010 census. We then applied the small-area 2010 census proportions to the population projections to obtain corrected population counts by single-year age/sex/small area for 2010. Lastly, we calculated the proportion of people for each age/sex/small area within each comuna based on the 2010 corrected population estimates and applied those proportions to the 2015–2017 population by sex and single age. For more details on population estimation, refer to Appendix 1.
Socioeconomic Characteristics
Area-level socioeconomic characteristics from the 2010 census were obtained from the SALURBAL project [24]. We selected the following measures for socioeconomic status (SES): percentage of households with water access inside dwellings, percentage of households with overcrowding (more than 3 people per room), percentage of 15–17-year-old population attending school, percentage of the population aged 25 years or above who completed at least high school education, and the unemployment rate. These variables were selected because (a) they have been shown to be associated with LE and mortality in LA cities in previous studies [8, 19] and (b) they are commonly available from census data at the small-area level. Each of these variables was used not as markers per se (patterning of education, overcrowding, water access, etc.) but as markers of the general small area effect (socioeconomic patterning generally). To reduce measurement error in the estimation of socioeconomic status, we also computed a composite index (Z-score) of the aforementioned SES variables. Although there is little agreement on which SES indicator summarizes different aspects of overall health risk better, composite indicators enhance the explanatory power of inequities. A similar index was tested empirically in other studies [25]. To create the composite index, we standardized all variables with a mean of 0 and a standard deviation of 1, and the unemployment and overcrowding variables were reversed (so that higher values signified higher socioeconomic status for all variables). The average of these standardized scores is defined as the composite Z-score representing the socioeconomic characteristics of small areas. A higher score value signifies better living conditions.
Statistical Analysis
To compute LE, we obtained estimates of single-year age- and sex-specific mortality rates using a Bayesian adaptation of the Tool for Projecting Age-Specific Rates using Linear Splines (TOPALS) method, described in Appendix 2. The city-level mortality schedule served as the standard mortality schedule required in the TOPALS method. To address the unstable log mortality rates of the standard mortality schedule, we performed a LOESS regression, and the smoothed rates were used as the standard schedule for mortality. Based on a Bayesian model, we ran the Markov Chain Monte Carlo algorithm for 100,000. The first 80,000 samples were discarded as burn-ins, and the remaining samples were thinned by a factor of 10. We retained 2000 sets of age- and sex-specific mortality rates from the posterior distributions, which were inputted into standard single-age life tables.
We then calculated LE at birth and at ages 20, 40, and 60 years using the DemoTools package in R. The life tables were calculated for each iteration of posterior age-specific mortality estimates, resulting in a total of 2000 life tables with their corresponding life expectancies for each small area. The median of the 2000 samples was reported as the point estimate for LE, while the 2.5th and 97.5th percentiles of the posterior samples were reported as lower and upper credible intervals.
To describe inequities in LE in the city, we calculated the 10th (P10) and 90th percentiles (P90) of the point estimate of LE across small areas by sex and computed the P90–P10 gap. To describe the spatial patterning of LE, we created choropleth maps of the LE using ArcGisPro. To study the association between LE and socioeconomic characteristics, we fit linear regressions of LE on each predictor variable converted into deciles and scored on a continuous scale between 0 and 1. Specifically, for each socioeconomic variable, we assigned the value of 0 if it corresponds to the first decile of its distribution across all small areas. The second decile obtained the value of 1/9, the third decile obtained the value of 2/9, and so on. To acknowledge the uncertainty around the estimates of LE, these models were repeated 2000 times with each set of posterior estimates. Coefficients were pooled using Rubin’s formula [26]. These analyses were done for LE at birth (main results) and LE at ages 20, 40, and 60 years (see Appendix 3 for results). The resulting regression coefficient represents the mean difference in LE in areas with the highest socioeconomic variable (i.e., those in the tenth decile) versus the areas with the lowest value of the socioeconomic variable (those in the first decile) and is presented as the slope index of inequality (SII). Finally, while we accounted for spatial autocorrelation to improve our estimates of LE, we did not account for spatial correlation to describe the predictors of inequities in LE. This was motivated by research from the spatial statistics literature, which recommends against including spatial random effects when the focus is on estimating associations [27] and by the computational burden of fitting our second-stage models 2000 times (once for each set of samples) to account for the uncertainty in the life expectancy estimates.
Analyses were conducted using R® version 4.1.1 software and SAS® 9.4. The data used for this study were aggregated to respect confidentiality and the data agreement policy of the SALURBAL project. None of the sources used had data to identify the individuals involved. The study was approved by the Drexel University institutional review board.
Results
Between 2015 and 2017, there were 88,330 deaths in the 351 small areas of CABA. Table 1 describes the socioeconomic characteristics of small areas. Median LE at birth across all small areas was higher for women (81.9 years) compared to men (76.7 years). These patterns held for LE at 20, 40, and 60 years. We found wide variability in LE between small areas, ranging from 76.6 to 85.9 years for women and from 68.1 to 83.0 years for men, demonstrating a gap of 9.3 and 14.9 years between areas with the highest and the lowest LE (Fig. 1). The 90th percentile of LE at birth was 83.2 years for women and 79.3 for men, while the 10th percentile was 80.3 for women and 74.0 years for men, for a P90–P10 difference of 2.9 years and 5.3 years among women and men, respectively.
Table 1.
Number of deaths, life expectancy among women and men, and selected sociodemographic characteristics by small area (n = 351). Ciudad Autónoma de Buenos Aires, 2015-2017
| Characteristics | Median (10th–90th percentile) | |
|---|---|---|
| Women | Men | |
| Number of deaths | 140 (96, 191) | 110 (74, 156) |
| Estimated populationa | 13,628 (10,030, 18,082) | 11,715 (8,530, 16,203) |
| Life expectancy at birtha | 81.9 (80.3, 83.2) | 76.7 (74.0, 79.3) |
| Life expectancy at age 20a | 62.6 (60.9, 63.9) | 57.5 (54.7, 60.0) |
| Life expectancy at age 40a | 43.0 (41.5, 44.3) | 38.2 (35.9, 40.6) |
| Life expectancy at age 60a | 24.6 (23.4, 25.6) | 20.5 (18.8, 22.3) |
| Population aged 15 or youngera (%) | 17.7 (13.1, 23.0) | 21.7 (17.0, 27.0) |
| Population aged 65 or oldera (%) | 19.8 (15.7, 24.0) | 13.2 (10.4, 17.1) |
| Households with water inside dwellingsb (%) | 99.1 (93.5,99.9) | |
| Households with overcrowdingb (%) | 0.7 (0.25, 2.9) | |
| School attendance among 15–17 years oldb (%) | 99.2 (86.3, 96.3) | |
| At least high school educationb (%) | 72.7 (52.7, 86.7) | |
| Unemploymentb (%) | 4.1 (3.1, 5.5) | |
Overcrowding: proportion of households with more than 3 people per room. Unemployment: proportion among the population 15 years or above in the labor force
aData from 2015 to 2017
bData from the 2010 census
Fig. 1.
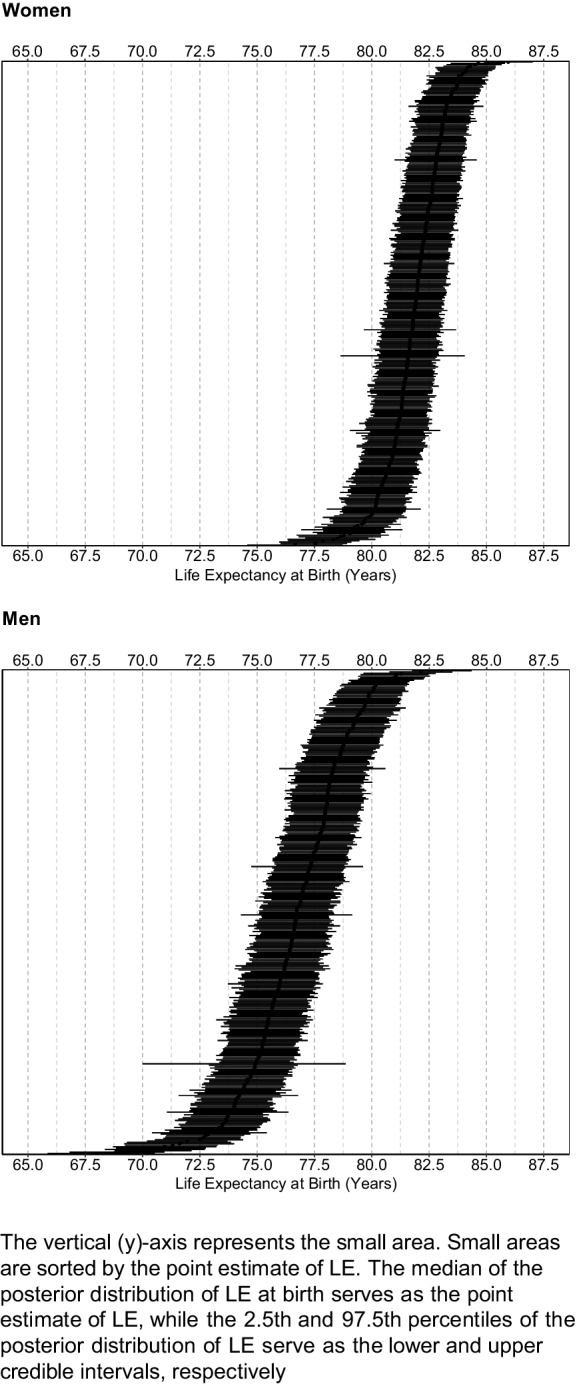
Life expectancy at birth (95% credible intervals) among women and men, by small area in Ciudad Autónoma de Buenos Aires, 2015–2017
We found a general North–South spatial gradient for LE at birth (Fig. 2). LE was higher in the North and North-east parts of the city, as compared to the South and South-western areas (lower LE). In addition, there is a strip in the central region of the city with higher levels of LE, surrounded by other areas of low LE.
Fig. 2.

Maps of life expectancy at birth among women and men in small areas of Ciudad Autónoma de Buenos Aires, 2015–2017
Figure 3 displays the scatterplots of LE at birth versus small-area socioeconomic characteristics. Education, school attendance, and accessibility to water are positively associated with LE, while unemployment and overcrowding are negatively associated. Table 2 shows the SII in LE at birth associated with each socioeconomic characteristic, by sex. All variables were associated with LE at birth, and the magnitude of association was stronger among men. For example, men living in areas with the highest decile of education (% with at least high school education) had 5.63 years (95% CI: 5.00, 6.25) higher LE at birth than those living in the areas with the lowest levels of education. This association was relatively weaker among women (SII = 2.99 years, 95% CI: 2.51, 3.46). We found a similar pattern with all other socioeconomic variables. For example, men and women living in areas with the highest levels of unemployment had 4.72 and 2.52 years lower LE than those living in areas with the lowest levels of unemployment. The socioeconomic index (composite Z-score) was also strongly associated with LE: small areas at the tenth decile of the Z-score had 5.61 and 2.79 years of higher LE than the areas at the first decile of the Z-score, in men and women, respectively. Analysis with LE at ages 20, 40, and 60 years showed similar results (see Appendix 3).
Fig. 3.

Scatterplots for the association between life expectancy and socioeconomic characteristics by sex for CABA 2015–2017
Table 2.
Slope index of inequality (SII) in life expectancy at birth (years) associated with small-area characteristics in Ciudad Autónoma de Buenos Aires, 2015-2017
| Variable | SII in LE at birth in years (95% confidence intervals) | |
|---|---|---|
| Women | Men | |
| At least high school education (%) | 2.99 (2.51, 3.46) | 5.63 (5.00, 6.25) |
| Households with overcrowding (%) | −2.19 (−2.71, −1.68) | −4.77 (−5.47, −4.08) |
| School attendance among 15–17 years old (%) | 2.15 (1.64, 2.65) | 4.48 (3.77, 5.18) |
| Unemployment (%) | −2.52 (−3.01, −2.04) | −4.72 (−5.40, −4.03) |
| Households with water inside dwellings (%) | 1.93 (1.41, 2.45) | 4.38 (3.66, 5.09) |
| Composite Z-score | 2.79 (2.30, 3.28) | 5.61 (4.98, 6.24) |
The models were run in a univariate fashion, one variable at a time. Small-area characteristics were transformed into deciles. The SII represents the mean difference in life expectancy in areas with the highest predictor variable (i.e., those in the tenth decile, having value = 1) versus the areas with the lowest value of the predictor variable (those in the first decile, having value = 0). Socioeconomic data for small areas came from the 2010 census. Overcrowding: proportion of households with more than three people per room
Discussion
We found evidence of spatial heterogeneity and intraurban variability in LE at birth and at ages 20, 40, and 60 years in CABA. Overall, LE at birth was 5.2 years higher for women (81.9 vs. 76.7 years in men). We found a P90th–P10th gap of 2.9 and 5.3 years within the city for women and men, respectively. We also evidenced a north-south spatial patterning, with higher LE in the north, and a transitional strip at the core of the city. Furthermore, we found strong associations of socioeconomic status in small areas with LE at birth. Women who lived in small areas with the best socioeconomic indicators can expect to live 2–3 years longer than those living in the most disadvantaged areas, while men who lived in small areas with the better socioeconomic indicators lived 5–6 years longer than those living in the most disadvantaged areas.
Studies focusing on the analysis of spatial variability can provide meaningful information on place-related health effects. Bilal et al. [13] described intraurban variations in LE in six LA cities, including the Buenos Aires metropolitan area (with CABA within), and documented 5.8 and 4.4 years of difference in women’s and men’s LE at birth between the top 90th and bottom 10th percentiles of the metropolitan area of CABA. Sacco et al. [12] reported a significant heterogeneity in LE across departments in the province of Buenos Aires (CABA was not included), showing a 7.6-year gap between departments with the highest and lowest LE at birth. Our findings show that it is possible to reveal and visualize important spatial heterogeneity at a smaller scale within the city. These epidemiological estimates and visualizations can be used to monitor health-based events and to motivate research into the drivers of this spatial heterogeneity.
Although the mechanism underlying the impact of gender inequities in urban agglomerations remains elusive [28], findings from other studies have identified an existing gender gap in life expectancy, and a few have described it for low-income countries [29]. In our study, we found a median age difference of 5.2 years between women and men. Also, the strength of associations between LE and the selected predictors was stronger for men than for women. Previous findings could shed a light on this difference, which could be explained by the concentration of violent deaths among young men [8] and the scale of cities, where larger cities are likely to have a higher proportionate mortality by violence than smaller cities [8, 16, 30]. This gender difference is a health outcome likely to be critical in understanding how cities are shaped by gender inequities that have both biological and nonbiological origins, rooted in gender norms and inequities [29].
The north-south gradient in LE that we observed is similar to that reported by other studies focused on all-cause and cause-specific mortality in Buenos Aires [19]. Our results showed a mosaic pattern in the central part of the city, with a strip of higher LE, like that observed in the northern part of the city. This spatial variability in LE is not random and can be explained by the spatial distribution of people with different socioeconomic characteristics between subcity units (Appendix 4). Sensitivity analyses with LE at ages 20, 40, and 60 showed similar patterns, suggesting that these socioeconomic characteristics are important predictors of mortality outcomes throughout the life span. Unsurprisingly, the spatial patterns of LE exhibit a similar gradient as the spatial pattern observed in the maps of small-area socioeconomic characteristics.
Understanding the historical and economic processes that led to this spatial patterning can help explain inequities in LE. Our findings are consistent with studies inspired by critical geography that proposed habitant-based classificatory typologies for neighborhoods of CABA where the colonial city, the central city, and higher SES residential areas overlap with the northern region—as for this study [21, 31]. In contrast, the southern region of the city was the last area to be incorporated into CABA’s jurisdiction, producing informal settlements and areas of low SES as a result of unplanned interventions [21, 32, 33]. The central strip also corresponds to an area formerly linked to railway employees that has been recently gentrified as part of a renewed city-branding strategy (24).
We also found that small area-level socioeconomic characteristics were strongly predictive of LE. Specifically, advantaged small areas had higher LE, with these associations being stronger among men. These associations could be the result of differences in context (e.g., lower pollution and lower violence in higher SES areas) or in composition (e.g., higher SES individuals in these areas). Differences in composition across areas resulting from residential segregation may explain part of our findings [33]. Our ecological study design cannot differentiate between the effects of segregation patterns and contextual factors.
Quantitative comparisons across studies in the size of inequities are rendered complex by the different areas and metrics used. For example, we used a much smaller spatial unit (Fracciones censales) than Bilal et al. (comuna/partidos) [13]. The geographical definition of the city can also differ and influence estimates of heterogeneity. We focused on the core city (CABA), while Bilal et al. used a much broader definition based on a larger urban agglomeration that included adjacent areas that are part of the broader metropolitan area [13]. On the one hand, the use of smaller areas may allow us to see more heterogeneity, but the inclusion of larger geographic areas allows comparisons with peripheral areas which, in the LA context, are often more disadvantaged than the core (although these patterns may be rapidly changing with the construction of private neighborhoods in the outskirts of large cities).
This study has several strengths. First, we used data on all deaths registered in CABA during a 3-year period, resulting in more than 88,000 deaths, all georeferenced to a small-area level (average area size = 0.58 km2). Second, the Bayesian application of the TOPALS method allowed us to obtain precise and reliable LE estimates. Third, data availability for this study is specifically for the administrative boundaries of CABA. Our findings could inform future research integrating peripheral areas of CABA to describe and study the urban socioeconomic structure [31]. An examination of the larger metropolitan area within which CABA is located would capture a much greater socioeconomic heterogeneity that could potentially exhibit a stronger association between LE and socioeconomic characteristics, as we reported previously for larger geographical areas [13]. Our study also has limitations. First, given that the census data are updated every decade and the 2020 census has not been carried out yet, we relied on the 2010 census for SES variables. The time difference between census (2010) and georeferenced deaths (2015–2017) could bias these results. We also relied on the 2010 population along with population projections for 2015–2017 to obtain population denominators. The total city population has only changed by 2% over the 7-year period, according to previous projections, which would allow us to assume that the impact is likely to be small [22]. Second, deaths that could not be georeferenced were less than 1.5% each year for all age groups and 6% for infants (under 1 year). This lack of georeferenced data could be related to areas of low socioeconomic characteristics, whose residents are less likely to report vital events than residents in areas with high socioeconomic status [34]. Consequently, LE estimates could be overestimated in lower socioeconomic areas, resulting in a conservative estimation of the associations between area socioeconomic status and LE.
In summary, we found wide within-city spatial and socioeconomic heterogeneities in LE across small areas of one of the wealthiest cities of Argentina, a middle-high-income LA country. These heterogeneities are driven by modifiable factors that configure inequities that could potentially be addressed through oriented place-based policies, for example, community gender-based interventions.
Acknowledgements
The Salud Urbana en América Latina (SALURBAL)—Urban Health in Latin America project is funded by the Wellcome Trust [205177/Z/16/Z]. UB was partially supported by the Office of the Director of the National Institutes of Health under award number DP5OD26429. The authors acknowledge the contribution of all SALURBAL project team members. For more information on SALURBAL and to see a full list of current researchers, see https://drexel.edu/lac/salurbal/team/. Also, we want to acknowledge Luis María Donati, General Director of Dirección de Estadística y Censos in CABA, and Nora Zuloaga, former subdirector of the Dirección de Estadística y Censos for facilitating the access to data, its orientations, and feedbacks, and Carlos Guevel, General Director of Dirección de Estadísticas e Información en Salud, for its advisory in georeferencing criteria. SALURBAL acknowledges the contributions of many different agencies in generating, processing, facilitating access to data, or assisting with other aspects of the project. Please visit (lacurbanhealth.org) for a complete list of data sources and institutions.
Role of the Funding Source
The funder had no role in the design, collection analysis, writing, or decision to submit the paper for publication.
Appendix 1
Estimating the Corrected Population for 2010
Although the 2010 census provides population counts by single-year age (0,1,…,110), sex, and small area, the population distribution from the 2010 census is different from the 2010 projected population distribution. In particular, the 2010 projected population makes a correction for the census that omitted an estimated 5.13% of the population of Buenos Aires, most of which impacted the younger age groups. This omission was determined by using prior censuses, vital statistics, and migration registration (from the Direccion General de Estadistica y Censos, Gobierno de la Ciudad de Buenos Aires). However, the 2010 projected population is available at the comuna level, with the highest age group being 80 years. We obtained corrected 2010 population estimates by single age (0,1,..85), sex, and small area as follows:
Aggregated the census 2010 population into single-year ages (0,1,… 85+) by sex and small area. Population aged ≥ 85 years are included in the highest age category, 85+. All other ages remain as a single year.
Graduated the projected 2010 population for each comuna by sex into single ages using the penalized composite link model (PCLM)1. This redistributes the population into single-year age groups. Population aged ≥ 85 years are included in the highest age category, 85+, to match the census population.
Using the census 2010 data, we calculated the proportion of the comuna population that lives within a given small area for each age–sex combination.
Applied those proportions to the projected 2010 population to obtain the corrected age and sex counts for each small area for 2010.
Let nasi; j represent the 2010 census population for age (a), sex (s), and small areas (i). Let the small area (i) be nested within the comuna (j). Assume there are Ni small areas nested in the jth comuna. Then, the proportion of people living in each small area of a given comuna (i.e., the proportion of the comuna population within the small area for each sex–age combination) is,
Now, let Pasj be the projected 2010 population for a, s, and j.
The corrected 2010 population estimate by age, sex, and L2.5 will be: Easi; j = Pasj × rasi; j.
Estimating the Population for 2015–2017—Was Used as the Denominator
We estimate the population counts by single-year age, sex, and a small area for 2015–2017—the years that correspond to the mortality data—with the following steps.
We graduate the 2015–2017 comuna-level projected population by sex into single ages.
We calculate the proportion of people in each small area out of comuna-level population by age and sex based on the 2010 corrected population estimates
We apply those proportions to the 2015–2017 population by sex and single age
For example, if P2015 asj is the 2015 comuna-level projected population at jth comuna, for a and s, and if Easi; j is the estimated 2010 population for the small area calculated above, the estimated population for the year 2015 by age, sex, and a small area will be:
Appendix 2
Modeling Mortality Rates
In this paper, we employ the Bayesian adaptation of the tool for projecting age patterns using the linear spline method (TOPALS), which incorporates spatial smoothing in small areas [4].
For a {a = 0, 1, 2, …, 85+} and i {i = 1, 2, …, 351} with corresponding population (nia), we assume that the number of deaths comes from a Poisson distribution with an underlying rate (λia).
We further assume that the vector of log mortality rates in i is,
where λi is the vector with elements λia representing age-specific mortality rates in small areas, λ∗ is the vector of the standard mortality schedule (i.e., the smoothed city-level rates), B is a matrix of constants of size 86 × 7 in which each column is a linear B-spline basis function (βk) is a vector of parameters with elements βik representing offsets to the standard schedule. We used the 2015–2017 mortality schedule for the whole city of CABA as the standard schedule. We obtained a smoothed version of this schedule by fitting a LOESS regression of log(mortality) on age.
We define knots at ages t0,…,t6 = (0, 1, 10, 20, 40, 70, 85). For ages a in {0, 1, 2, ..., 85} and columns k in {0,...,6}, the basis functions in B are:
We further decompose the βik into the intercepts at each knot β0k, the spatial random effects (zik)and unstructured random effects (ϕik) that vary by knot age and area.
We assign the unstructured, non-spatial random effect (ϕik) an exchangeable zero-mean normal prior to the knot-specific variance (). The variance parameter in turn receives the uninformative inverse gamma hyper-prior with the shape and rate parameters of 0.05 and 0.005, respectively.
That is,
For the intercept (β0k), we assign a vague normal prior with a mean of 0 and variance of 1000. That is,
For the spatial random effect (zik), we assign the intrinsic conditional autoregressive (ICAR) prior distribution for each knot, k. We define areas i and j as neighbors if they share one or more common vertex between boundaries, commonly referred to as Queen’s contiguity.
For any given knot and for each area, the conditional expected value of zik given the remaining values are the mean of its neighboring areas and the variance of zik is inversely proportional to the number of neighbors in that area, mi.
If we drop the subscript for knot here, we can denote the CAR distribution as:
where
Here, W = [wi, j] is 351 ×351 adjacency matrix with elements wi, j = 1 if areas i and j are neighbors and 0 otherwise. We complete the prior specification by assigning an uninformative inverse gamma prior (0.001, 0.001) for the variance of CAR random effects.
The models were run using WinBUGS by calling the software with the R2WinBUGS package in R for 50,000 iterations for each of the two chains. For each chain, the first 40,000 samples were discarded as burn-ins, and the remaining samples were thinned by a factor of 10 to reduce the autocorrelation of the samples. We fit the models for males and females separately.
Appendix 3
See Table 3.
Table 3.
Slope index of inequality (95% CI) in life expectancy (years) at ages 20, 40, and 60 associated with small area characteristics in CABA
| Variable | At 20 | At 40 | At 60 | |||
|---|---|---|---|---|---|---|
| Women | Men | Women | Men | Women | Men | |
| At least high school education (%) | 2.94 (2.48, 3.40) | 5.46 (4.86, 6.06) | 2.72 (2.27, 3.16) | 4.76 (4.21, 5.32) | 1.99 (1.59, 2.39) | 3.40 (2.93, 3.87) |
| Households with overcrowding (%) | −2.14 (−2.64, −1.64) | −4.60 (−5.27, −3.93) | −1.97 (−2.45, −1.49) | −3.92 (−4.54, −3.31) | −1.42 (−1.84, −1.00) | −2.73 (−3.24, −2.21) |
| School attendance among 15–17 years old (%) | 2.10 (1.60, 2.59) | 4.33 (3.64, 5.01) | 1.92 (1.44, 2.39) | 3.68 (3.05, 4.31) | 1.37 (0.96, 1.78) | 2.54 (2.02, 3.06) |
| Unemployment (%) | −2.48 (−2.95, −2.01) | −4.58 (−5.24, −3.91) | −2.29 (−2.75, −1.83) | −3.95 (−4.56, −3.35) | −1.68 (−2.08, −1.28) | −2.76 (−3.27, −2.25) |
| Households with water inside dwellings (%) | 1.88 (1.37, 2.39) | 4.22 (3.52, 4.91) | 1.74 (1.25, 2.23) | 3.63 (2.99, 4.26) | 1.26 (0.84, 1.69) | 2.57 (2.04, 3.09) |
| Composite Z-score | 2.73 (2.26, 3.21) | 5.43 (4.82, 6.03) | 2.52 (2.06, 2.97) | 4.69 (4.13, 5.25) | 1.83 (1.42, 2.24) | 3.29 (2.81, 3.78) |
The models were run in a univariate fashion, one variable at a time. Small-area characteristics were transformed into deciles. The SII represents the mean difference in life expectancy in areas with the highest predictor variable (i.e., those in the tenth decile, having value = 1) versus the areas with the lowest value of the predictor variable (those in the first decile, having value = 0. Socioeconomic data for small areas came from the 2010 census; overcrowding: proportion of households with more than three people per room
Appendix 4
See Fig. 4.
Fig. 4.

Choropleth maps of selected socioeconomic characteristics in small areas of CABA. Map cutoffs are based on quintiles; on the purple scale maps, a higher percentage indicates better socioeconomic characteristics of the small areas; on the orange scale maps, a higher percentage indicates a worse socioeconomic characteristic of the small areas; data on socioeconomic characteristics are from the 2010 Argentina census
Footnotes
The maximum open-ended age group in population graduation was set at 103 for females and 100 for males.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
References
- 1.United Nations, DESA/Population Division. Final report. World urbanization prospects 2018. New York: United Nations; 2019. Available from: https://population.un.org/wup/Publications/Files/WUP2018-Report.pdf. Accessed 2 Mar 2023.
- 2.Oliver K, Cairney P. The dos and don’ts of influencing policy: a systematic review of advice to academics. Palgrave Commun Palgrave. 2019;5:1–11. [Google Scholar]
- 3.dos SMI, dos SGF, Freitas A, de SFJF, Castro C, ASS P, et al. Urban income segregation and homicides: an analysis using Brazilian cities selected by the Salurbal project. SSM - Popul Health. 2021;14:100819. doi: 10.1016/j.ssmph.2021.100819. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Gonzaga MR, Schmertmann CP. Estimating age- and sex-specific mortality rates for small areas with TOPALS regression: an application to Brazil in 2010. Rev Bras Estud Popul Scielo. 2016;33:629–652. doi: 10.20947/S0102-30982016c0009. [DOI] [Google Scholar]
- 5.Hoffmann R, Borsboom G, Saez M, Dell’Olmo M, Burström B, Corman D, et al. Social differences in avoidable mortality between small areas of 15 European cities: an ecological study. Int J Health Geogr. Int J Health Geogr. 2014; [cited 2023 Jan 6];13. Available from: https://pubmed.ncbi.nlm.nih.gov/24618273/. Accessed 2 Mar 2023. [DOI] [PMC free article] [PubMed]
- 6.Bennett JE, Li G, Foreman K, Best N, Kontis V, Pearson C, et al. The future of life expectancy and life expectancy inequalities in England and Wales: Bayesian spatiotemporal forecasting. Lancet Lond Engl. 2015;386:163–170. doi: 10.1016/S0140-6736(15)60296-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Nolasco A, Moncho J, Quesada JA, Melchor I, Pereyra-Zamora P, Tamayo-Fonseca N, et al. Trends in socioeconomic inequalities in preventable mortality in urban areas of 33 Spanish cities, 1996-2007 (MEDEA project) Int J Equity Health. 2015;14:33. doi: 10.1186/s12939-015-0164-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Bilal U, Hessel P, Perez-Ferrer C, Michael YL, Alfaro T, Tenorio-Mucha J, et al. Life expectancy and mortality in 363 cities of Latin America. Nat Med. 2021;27:463–470. doi: 10.1038/s41591-020-01214-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Diez Roux AV, Mair C. Neighborhoods and health: neighborhoods and health. Ann N Y Acad Sci. 2010;1186:125–145. doi: 10.1111/j.1749-6632.2009.05333.x. [DOI] [PubMed] [Google Scholar]
- 10.Quick H, Terloyeva D, Wu Y, Moore K, Diez Roux AV. Trends in tract-level prevalence of obesity in Philadelphia by race-ethnicity, space, and time. Epidemiol Camb Mass. 2020;31:15–21. doi: 10.1097/EDE.0000000000001118. [DOI] [PubMed] [Google Scholar]
- 11.Economic Commission for Latin America and the Caribbean E. Generic Law on Official Statistics for Latin America: United Nations; 2020. Available from: https://repositorio.cepal.org/bitstream/handle/11362/45254/1/S2000045_en.pdf. Accessed 2 Mar 2023.
- 12.Sacco N, Williams I, Queiroz BL. Estimaciones de esperanza de vida al nacer en áreas menores de la región pampeana: estimates of life expectancy at birth in minor areas of the Pampean region. Rev Bras Estud Popul. 2021;38:1–41. doi: 10.20947/S0102-3098a0160. [DOI] [Google Scholar]
- 13.Bilal U, Alazraqui M, Caiaffa WT, Lopez-Olmedo N, Martinez-Folgar K, Miranda JJ, et al. Inequalities in life expectancy in six large Latin American cities from the SALURBAL study: an ecological analysis. Lancet Planet Health Elsevier. 2019;3:e503–e510. doi: 10.1016/S2542-5196(19)30235-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Schmertmann CP, Gonzaga MR. Bayesian estimation of age-specific mortality and life expectancy for small areas with defective vital records. Demography. 2018;55:1363–1388. doi: 10.1007/s13524-018-0695-2. [DOI] [PubMed] [Google Scholar]
- 15.Chandra H, Aditya K, Sud UC. Localised estimates and spatial mapping of poverty incidence in the state of Bihar in India—an application of small area estimation techniques. Plos One Public Libr Sci. 2018;13:1–14. doi: 10.1371/journal.pone.0198502. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.López SR, Tumas N, Bilal U, Moore KA, Acharya B, Quick H, et al. Intraurban socioeconomic inequalities in life expectancy: a population-based cross-sectional analysis in the city of Córdoba, Argentina (2015–2018) BMJ Open Br Med J Publ Group. 2022;12:e061277. doi: 10.1136/bmjopen-2022-061277. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.INDEC: Instituto Nacional de Estadística y Censos de la República Argentina. Censo 2010. Available from: https://www.indec.gob.ar/indec/web/Nivel4-Tema-2-41-135. Accessed 23 Jul 2022.
- 18.Banco de Datos Estadística y Censos. 2022. Available from: https://www.estadisticaciudad.gob.ar/eyc/?page_id=536, Accessed 15 Mar 2023.
- 19.Alazraqui M, Roux AVD, Fleischer N, Spinelli H. Self-rated health and social inequalities, Buenos Aires, Argentina, 2005. Cad Saúde Pública. Escola Nacional de Saúde Pública. Fundação Oswaldo Cruz. 2009;25:1990–2000. [DOI] [PubMed]
- 20.Martínez ML, Guevel CG. Desigualdades sociales en la mortalidad por cáncer de cuello de útero en la Ciudad Autónoma de Buenos Aires, 1999-2003 y 2004-2006. Salud Colect. 2013;9:169–182. doi: 10.18294/sc.2013.30. [DOI] [PubMed] [Google Scholar]
- 21.Marcos M. Estructura socioespacial de la aglomeración Gran Buenos Aires. Geo UERJ. 2015;0:22–54. doi: 10.12957/geouerj.2015.11583. [DOI] [Google Scholar]
- 22.Dirección General de Estadística y Censos Dge. Evaluación de la proyección de la población de la Ciudad de Buenos Aires. Años 2010 a 2040. In: Informe de resultados 733; 2014. Report No.: 733. Available from: https://www.estadisticaciudad.gob.ar/eyc/wp-content/uploads/2015/04/ir_2014_733.pdf. Accessed 1 April 2023.
- 23.Rizzi S, Halekoh U, Thinggaard M, Engholm G, Christensen N, Johannesen TB, et al. How to estimate mortality trends from grouped vital statistics. Int J Epidemiol. 2019;48:571–582. doi: 10.1093/ije/dyy183. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Quistberg DA, Diez Roux AV, Bilal U, Moore K, Ortigoza A, Rodriguez DA, et al. Building a data platform for cross-country urban health studies: the SALURBAL study. J Urban Health Bull N Y Acad Med. 2019;96:311–337. doi: 10.1007/s11524-018-00326-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Ortigoza AF, Tapia Granados JA, Miranda JJ, Alazraqui M, Higuera D, Villamonte G, et al. Characterising variability and predictors of infant mortality in urban settings: findings from 286 Latin American cities. J Epidemiol Community Health. 2021;75:264. doi: 10.1136/jech-2020-215137. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Rubin D. Multiple imputation for nonresponse in surveys. New York: John Wiley and Sons; 1987. [Google Scholar]
- 27.Hodges JS, Reich BJ. Adding spatially-correlated errors can mess up the fixed effect you love. Am Stat Taylor Francis. 2010;64:325–334. [Google Scholar]
- 28.Glei DA, Horiuchi S. The narrowing sex differential in life expectancy in high-income populations: effects of differences in the age pattern of mortality. Popul Stud Popul Invest Comm, Taylor Francis, Ltd. 2007;61:141–159. doi: 10.1080/00324720701331433. [DOI] [PubMed] [Google Scholar]
- 29.Chant S. Cities through a “gender lens”: a golden “urban age” for women in the global South? Environ Urban SAGE Publications Ltd. 2013;25:9–29. [Google Scholar]
- 30.Bilal U, de Castro CP, Alfaro T, Barrientos-Gutierrez T, Barreto ML, Leveau CM, et al. Scaling of mortality in 742 metropolitan areas of the Americas. Sci Adv Am Assoc Adv Sci. 2021;7:eabl6325. doi: 10.1126/sciadv.abl6325. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Buzai GD, Marcos M. The social map of Greater Buenos Aires as empirical evidence of urban models. J Lat Am Geogr Univ Texas Press. 2012;11:67–78. doi: 10.1353/lag.2012.0012. [DOI] [Google Scholar]
- 32.Marcos M, Mera GS, Virgilio MMD. Contextos urbanos de la Ciudad de Buenos Aires: una propuesta de clasificación de la ciudad según tipos de hábitat: Papeles Poblac 2015. [cited 2023 Apr 8];21. Available from: https://rppoblacion.uaemex.mx/article/view/8319. Accessed 2 Mar 2023.
- 33.Virgilio MD, Gil A, Perea C, Vitale P, Ostuni F. La ciudad al sur de la ciudad: historia sociourbana de los barrios Villa Lugano y Villa Riach. Cuad Vivienda Urban. 2010; [cited 2023 Apr 8];3. Available from: https://revistas.javeriana.edu.co/index.php/cvyu/article/view/5549. Accessed 2 April 2023.
- 34.Dirección General de Estadística y Censo. La mortalidad en la Ciudad de Buenos Aires. In: Sus diferencias por grupo de edad, sexo y comuna. Informe de resultados N 479. Ciudad Autónoma de Buenos Aires; 2011. Report No.: 479. Available from: https://www.estadisticaciudad.gob.ar/eyc/wp-content/uploads/2015/04/ir_2011_479.pdf. Accessed 2 Mar 2023.