

Small cell lung cancer (SCLC) accounts for ~14% of all lung cancer cases and incidence is associated with a previous history of cigarette smoking. It is a fast-growing and aggressive neuroendocrine tumor that has high metastatic potential, strong propensity for the development of drug resistance, and a low survival rate. Treatment options for SCLC patients are poor and standard of care has changed little over the past 20 years with first-line therapy for limited disease mostly consisting of chemotherapy (carboplatin or cisplatin plus etoposide) and radiation (1,2). The addition of immune checkpoint inhibitors (ICIs) in extensive stage has brought some benefit but only a minimal increase in median overall survival (mOS). Recent results from the IMpower133 study, combining carboplatin plus etoposide (C/E) with the ICI atezolizumab targeting PD-L1 (programmed cell death-ligand 1 or CD274) versus C/E with placebo, showed that first-line combination treatment of extensive-stage SCLC (ES-SCLC) improved mOS by only 2 months (10.2 versus 12.2 months plus ICI). The results were independent of the blood mutational tumor burden or the PD-L1 status of the tumor cells (3). Similarly, recent results from the CASPIAN study showed that etoposide plus platin-based therapy with the ICI durvalumab targeting PD-1 (programmed cell death protein 1 or CD279) or placebo in ES-SCLC, improved mOS also by only ~2 months (10.5 versus 12.9 months plus ICI). Interestingly, the addition of the CTLA4 (cytotoxic T-lymphocyte-associated protein 4 or CD152) targeting tremelimumab was not beneficial in this setting (4). While both studies showed significant benefits for ICI combination treatment, the KEYNOTE-604 trial in ES-SCLC, studying etoposide with platinum-based chemotherapy with the PD-targeting ICI pembrolizumab did not reach a significant endpoint (9.7 versus 10.8 months plus ICI) (5) (Table 1). It should be noted though that all three trials led to prolonged progression-free survival and there was a trend towards improved overall survival in a small subset of patients. Predictive biomarkers that could identify this small group of patients have yet to be identified. Even though only few SCLC patients may benefit from ICIs and obtain a long-term durable response, the results are encouraging as they may give lead to additional combination approaches that could improve current therapy.
Table 1. Clinical trials of ICIs in SCLC.
| Trial | ICI/target | mOS-combo (months) | mOS-chemo (months) | ClinicalTrials.gov ID |
|---|---|---|---|---|
| IMpower133 | Atezolizumab/PD-L1 | 12.2 | 10.2 | NCT02763579 |
| CASPIAN | Durvalumab/PD-1 | 12.9 | 10.5 | NCT03043872 |
| Keynote 604 | Pembrolizumab/PD-1 | 10.8 | 9.7 | NCT03066778 |
Targeting PD-L1 with atezolizumab in the IMpower133 trial and PD-1 with durvalumab in the CASPIAN trial have led to a significant increase in mOS in combination with chemo versus chemo alone. The PD-1 inhibitor pembrolizumab failed to reach significant improvement in the Keynote 604 trial. ICI, immune checkpoint inhibitor; SCLC, small cell lung cancer; mOS, median overall survival; chemo, chemotherapy; PD-L1, programmed cell death-ligand 1; PD-1, programmed cell death protein 1.
The high mutation rate and diversity of transforming mechanisms in SCLC has made it difficult to define new targeted approaches. Distinct molecular subtypes in SCLC have been identified, based on expression of transcription factors and immune infiltrate, suggesting a model wherein SCLC can be divided into five treatment groups with different therapeutic approaches (6). Whether these results find their way into clinical practice remains to be determined, but they indicate that transcriptional programs are specifically associated with altered immune programs and that these distinct mechanisms are vulnerable to targeted approaches in SCLC subtypes. It has long been argued that effective targeted therapy may have, at some level, an effect on immune suppressive functions of cancer cells and that combination of both would be warranted (7), yet extensive use of combination therapy has not come to fruition.
Few clinical trials in ES-SCLC combining targeted approaches with ICIs are currently conducted (see clinicaltrials.gov) and these trials do not specifically select for the above-mentioned molecular subgroups. In general, there are two approaches for small molecule drugs as targeted therapy combinations with ICIs in cancers. The first approach attempts to identify novel therapeutic targets in signaling or metabolic pathways that primarily inhibit cell growth but can also directly enhance the immune response in combinations with ICIs. For example, targeting of protein phosphatase 2A (PP2A) with LB100 in combination with platinum-based chemotherapy was identified as a potential vulnerability in SCLC, in part through increasing the uptake of carboplatin (8). PP2A was also identified as an enhancer of anti-tumor immunity in other models, in part through acting on tumor cells but also through activation of mTORC1 signaling and reduction of the regulatory T cell pool and increased expression of Th1 versus Th2 cytokines (9). LB-100, is currently being tested in a clinical trial combining carboplatin, etoposide and atezolizumab for the treatment of ES-SCLC (ClinicalTrials.gov ID: NCT04560972). The second approach is geared towards chromatin remodeling and altered gene expression programs, leading to changes in transcriptional activities, thereby also inhibiting immune suppressive function of cancer cells. This may directly affect transcription factors but can also occur through altered chromatin accessibility by modulating the function of epigenetic modifiers. These molecules have gained considerable interest as they are known to be major contributors to transformation and may also be involved in nongenetic mechanisms of drug resistance. One of the key regulators of the neuroendocrine phenotype of SCLC was identified as lysine-specific demethylase 1A (LSD1 or KDM1A) (10). LSD1 is thought to act through inhibition of NOTCH, a cell surface receptor normally engaged through cell-cell interaction and involved in cell growth, viability and differentiation pathways (11,12).
Hiatt et al. (13) have now provided additional details about the LSD1-dependent epigenetic program and inhibition of LSD1 in pre-clinical models of SCLC that may have potential significant impact on how we approach future treatment of patients with this disease. Using syngeneic cells from a genetically defined murine SCLC model with Rb1/Trp53-deletion and artificial expression of antigens (to compensate for low tumor burden within this model), PD-1 targeting significantly enhanced the anti-tumor effects of the small molecule LSD1 inhibitor bomedemstat in immunocompetent mice. Anti-PD1 treatment by itself was ineffective, but combination with bomedemstat led to a significant increase in immune cell tumor infiltration, functional activation of CD8+ T cells and a reduction in neutrophils, whereas other blood cells showed little change. Bomedemstat is currently being tested in phase I/II clinical trials combined with atezolizumab (anti-PD-L1) maintenance immunotherapy in newly diagnosed ES-SCLC patients (ClinicalTrials.gov ID: NCT05191797). It is not known how well this drug is tolerated in patients but LSD1 inhibition can alter myeloid progenitor pools and neutropenia is a possible adverse event (14), thus it is not surprising that LSD1 inhibitors are currently also tested for their efficacy in myeloid malignancies. Interestingly, the reversible LSD1 inhibitor pulrodemstat (CC-90011) has already been tested in a phase 1 clinical trial and in particular patients with neuroendocrine neoplasms showed clinical responses with dose dependent thrombocytopenia as the most common treatment-related adverse event (15). This drug will now also be evaluated in combination with nivolumab (anti-PD-1) in SCLC patients (ClinicalTrials.gov ID: NCT04350463).
LSD1 is an opportune target as it not only acts on SCLC cells, but it also affects the anti-tumor immune response. It functions as a lysine-specific demethylase that has a broad substrate specificity towards many cellular proteins, but its role in SCLC epigenetics and the efficacy of bomedemstat appear to be largely based on the demethylation of mono-/di-methylated histone H3 on lysine 4 or 9, thereby changing chromatin accessibility and altering gene expression (see also Figure 1). Specific biomarkers for ICIs in SCLC have not come to fruition and the hope is that LSD1 targeted approaches will provide molecular clues for the regulation of tumor growth and the SCLC immune response that can then be integrated with algorithms to also capture the fractalness of the disease with the intent to improve patient stratification (16). Studies with the LSD1 inhibitor iadademstat (ORY-1001) demonstrated activation of NOTCH1 and suppression of ASCL1, a key regulator of the neuroendocrine phenotype in SCLC, likely initiated through release of LSD1 from the NOTCH1 locus (11). Iadademstat is considered in a clinical trial for relapsed/refractory SCLC patients in combination with paclitaxel (ClinicalTrials.gov ID: NCT05420636). The functional regulation of neuroendocrine features in SCLC through NOTCH may be intrinsically linked to the efficacy of PD-1/PD-L1 blockade (17), and a related link may exist between efficient NOTCH activation and suppression of ASCL1 in ASCL1-positive SCLC cells (11). Hiatt et al. (13) have now shown that bomedemstat can not only activate NOTCH and suppress neuroendocrine transcripts, but it can also induce the expression of antigen presentation through upregulation of MHC-I and stimulate the recruitment of T cells and dendritic cells through chemokines (including CXC3L1, CXCL12, CXCL14 or IL33) to allow for a proper immune response during PD-1 blockade. It is important to note that MHC-I upregulation was found to be independent of NOTCH signaling or IFN-γ pathway activation. In a parallel study, Nguyen et al. (18) also found that epigenetic silencing of MHC-I though LSD1 in SCLC models enhanced the activity of ICIs, likely in part through the activation of MHC-I restricted T cells.
Figure 1.
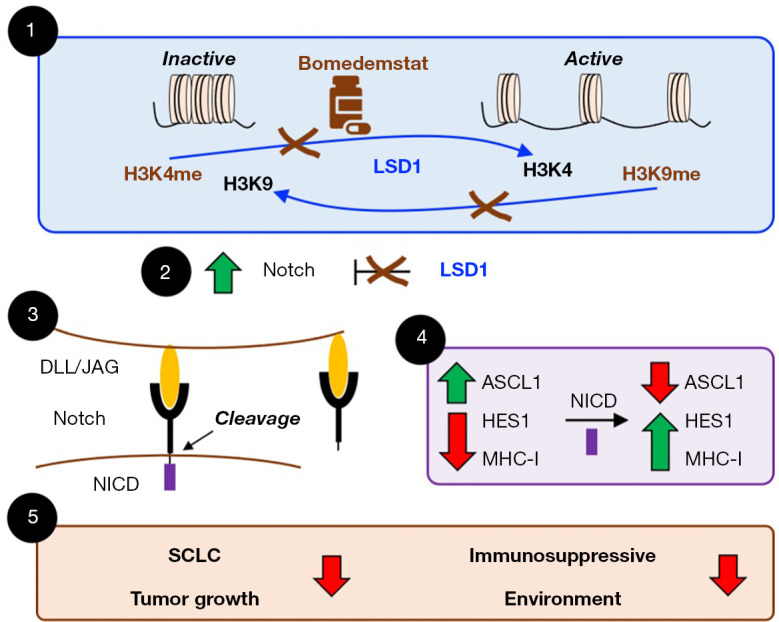
LSD1 and its inhibitor bomedemstat in SCLC. ① LSD1 is a demethylase for mono- and di-methylated histone H3K4 and H3K9 as well as other methylated proteins. Histone methylation marks can either repress (inactive chromatin) or allow (active chromatin) gene expression. The small molecule drug bomedemstat inhibits LSD1 and leads to accumulation of methylated H3K4me and H3K9me, thereby altering chromatin structure and subsequently gene expression. ② LSD1 also blocks the expression of NOTCH and its inhibition by bomedemstat leads to upregulation of the receptor protein. ③ Functionally expressed NOTCH proteins are activated by cell-cell interactions through their ligands, DLL or JAG, resulting in protease mediated cleavage and release of their extracellular domain and the NICD. ④ NICD translocate to the nucleus where it interacts with the CSL transcription factor to alter gene expression. NICD allows for the decreased expression of ASCL1, a key regulator of the SCLC neuroendocrine phenotype, and the increased expression of MHC-I, the NOTCH effector HES1 and other molecules. ⑤ Ultimately, bomedemstat affects SCLC tumor growth and reduces the immunosuppressive environment of SCLC, including improved antigen presentation through upregulation of MHC-I. SCLC, small cell lung cancer; NICD, NOTCH intracellular domain.
With the discovery of LSD1 as a therapeutic target in SCLC and the potential for improved efficacy of ICI combinations with bomedemstat and other LSD1 inhibitors, we may have finally arrived at impactful therapeutic combinations for this devastating disease. It will now be interesting to see whether this class of drugs can indeed provide a positive risk-benefit profile, whether there are clinical differences between reversible and covalent LSD1 inhibitors, whether a meaningful biomarker strategy can be developed, and how this group of inhibitors acts on other malignancies with neuroendocrine features. NOTCH may be an important target for LSD1 in SCLC, but the broad effect of its demethylase activity on a variety of proteins and its epigenetic function may make it more likely that there are other factors that contribute to the whole picture which may provide additional future opportunities for drug development.
Supplementary
The article’s supplementary files as
Acknowledgments
Funding: This work was supported in part by Robert and Kathleen Henderson via the Robert and Kathleen Henderson Lung Cancer Research Accelerator Fund at the City of Hope and by William and Anna Tenenblatt via The William & Anna Tenenblatt Foundation.
Ethical Statement: The authors are accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Footnotes
Provenance and Peer Review: This article was commissioned by the editorial office, Translational Lung Cancer Research. The article did not undergo external peer review.
Conflicts of Interest: Both authors have completed the ICMJE uniform disclosure form (available at https://tlcr.amegroups.com/article/view/10.21037/tlcr-23-40/coif). The authors have no conflicts of interest to declare.
References
- 1.Byers LA, Rudin CM. Small cell lung cancer: where do we go from here? Cancer 2015;121:664-72. 10.1002/cncr.29098 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Gong J, Salgia R. Managing Patients With Relapsed Small-Cell Lung Cancer. J Oncol Pract 2018;14:359-66. 10.1200/JOP.18.00204 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Liu SV, Reck M, Mansfield AS, et al. Updated Overall Survival and PD-L1 Subgroup Analysis of Patients With Extensive-Stage Small-Cell Lung Cancer Treated With Atezolizumab, Carboplatin, and Etoposide (IMpower133). J Clin Oncol 2021;39:619-30. 10.1200/JCO.20.01055 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Goldman JW, Dvorkin M, Chen Y, et al. Durvalumab, with or without tremelimumab, plus platinum-etoposide versus platinum-etoposide alone in first-line treatment of extensive-stage small-cell lung cancer (CASPIAN): updated results from a randomised, controlled, open-label, phase 3 trial. Lancet Oncol 2021;22:51-65. 10.1016/S1470-2045(20)30539-8 [DOI] [PubMed] [Google Scholar]
- 5.Rudin CM, Awad MM, Navarro A, et al. Pembrolizumab or Placebo Plus Etoposide and Platinum as First-Line Therapy for Extensive-Stage Small-Cell Lung Cancer: Randomized, Double-Blind, Phase III KEYNOTE-604 Study. J Clin Oncol 2020;38:2369-79. 10.1200/JCO.20.00793 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Gay CM, Stewart CA, Park EM, et al. Patterns of transcription factor programs and immune pathway activation define four major subtypes of SCLC with distinct therapeutic vulnerabilities. Cancer Cell 2021;39:346-360.e7. 10.1016/j.ccell.2020.12.014 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Vanneman M, Dranoff G. Combining immunotherapy and targeted therapies in cancer treatment. Nat Rev Cancer 2012;12:237-51. 10.1038/nrc3237 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Mirzapoiazova T, Xiao G, Mambetsariev B, et al. Protein Phosphatase 2A as a Therapeutic Target in Small Cell Lung Cancer. Mol Cancer Ther 2021;20:1820-35. 10.1158/1535-7163.MCT-21-0013 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Ho WS, Wang H, Maggio D, et al. Pharmacologic inhibition of protein phosphatase-2A achieves durable immune-mediated antitumor activity when combined with PD-1 blockade. Nat Commun 2018;9:2126. 10.1038/s41467-018-04425-z [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Jotatsu T, Yagishita S, Tajima K, et al. LSD1/KDM1 isoform LSD1+8a contributes to neural differentiation in small cell lung cancer. Biochem Biophys Rep 2016;9:86-94. 10.1016/j.bbrep.2016.11.015 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Augert A, Eastwood E, Ibrahim AH, et al. Targeting NOTCH activation in small cell lung cancer through LSD1 inhibition. Sci Signal 2019;12:eaau2922. 10.1126/scisignal.aau2922 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Zhou B, Lin W, Long Y, et al. Notch signaling pathway: architecture, disease, and therapeutics. Signal Transduct Target Ther 2022;7:95. 10.1038/s41392-022-00934-y [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Hiatt JB, Sandborg H, Garrison SM, et al. Inhibition of LSD1 with Bomedemstat Sensitizes Small Cell Lung Cancer to Immune Checkpoint Blockade and T-Cell Killing. Clin Cancer Res 2022;28:4551-64. 10.1158/1078-0432.CCR-22-1128 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Sprüssel A, Schulte JH, Weber S, et al. Lysine-specific demethylase 1 restricts hematopoietic progenitor proliferation and is essential for terminal differentiation. Leukemia 2012;26:2039-51. 10.1038/leu.2012.157 [DOI] [PubMed] [Google Scholar]
- 15.Hollebecque A, Salvagni S, Plummer R, et al. Clinical activity of CC-90011, an oral, potent, and reversible LSD1 inhibitor, in advanced malignancies. Cancer 2022;128:3185-95. 10.1002/cncr.34366 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Salgia R, Mambetsariev I, Hewelt B, et al. Modeling small cell lung cancer (SCLC) biology through deterministic and stochastic mathematical models. Oncotarget 2018;9:26226-42. 10.18632/oncotarget.25360 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Roper N, Velez MJ, Chiappori A, et al. Notch signaling and efficacy of PD-1/PD-L1 blockade in relapsed small cell lung cancer. Nat Commun 2021;12:3880. 10.1038/s41467-021-24164-y [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Nguyen EM, Taniguchi H, Chan JM, et al. Targeting Lysine-Specific Demethylase 1 Rescues Major Histocompatibility Complex Class I Antigen Presentation and Overcomes Programmed Death-Ligand 1 Blockade Resistance in SCLC. J Thorac Oncol 2022;17:1014-31. 10.1016/j.jtho.2022.05.014 [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
The article’s supplementary files as