

Abstract
Background:
The Italian Society of Echocardiography and Cardiovascular Imaging (SIECVI) conducted a national survey to understand better how different echocardiographic modalities are used and accessed in Italy.
Methods:
We analyzed echocardiography laboratory activities over a month (November 2022). Data were retrieved via an electronic survey based on a structured questionnaire, uploaded on the SIECVI website.
Results:
Data were obtained from 228 echocardiographic laboratories: 112 centers (49%) in the northern, 43 centers (19%) in the central, and 73 (32%) in the southern regions. During the month of observation, we collected 101,050 transthoracic echocardiography (TTE) examinations performed in all centers. As concern other modalities there were performed 5497 transesophageal echocardiography (TEE) examinations in 161/228 centers (71%); 4057 stress echocardiography (SE) examinations in 179/228 centers (79%); and examinations with ultrasound contrast agents (UCAs) in 151/228 centers (66%). We did not find significant regional variations between the different modalities. The usage of picture archiving and communication system (PACS) was significantly higher in the northern (84%) versus central (49%) and southern (45%) centers (P < 0.001). Lung ultrasound (LUS) was performed in 154 centers (66%), without difference between cardiology and noncardiology centers. The evaluation of left ventricular (LV) ejection fraction was evaluated mainly using the qualitative method in 223 centers (94%), occasionally with the Simpson method in 193 centers (85%), and with selective use of the three-dimensional (3D) method in only 23 centers (10%). 3D TTE was present in 137 centers (70%), and 3D TEE in all centers where TEE was done (71%). The assessment of LV diastolic function was done routinely in 80% of the centers. Right ventricular function was evaluated using tricuspid annular plane systolic excursion in all centers, using tricuspid valve annular systolic velocity by tissue Doppler imaging in 53% of the centers, and using fractional area change in 33% of the centers. When we divided into cardiology (179, 78%) and noncardiology (49, 22%) centers, we found significant differences in the SE (93% vs. 26%, P < 0.001), TEE (85% vs. 18%), UCA (67% vs. 43%, P < 0001), and STE (87% vs. 20%, P < 0.001). The incidence of LUS evaluation was similar between the cardiology and noncardiology centers (69% vs. 61%, P = NS).
Conclusions:
This nationwide survey demonstrated that digital infrastructures and advanced echocardiography modalities, such as 3D and STE, are widely available in Italy with a notable diffuse uptake of LUS in the core TTE examination, a suboptimal diffusion of PACS recording, and conservative use of UCA, 3D, and strain. There are significant differences between northern and central-southern regions and echocardiographic laboratories that pertain to the cardiac unit. This inhomogeneous distribution of technology represents one of the main issues that must be solved to standardize the practice of echocardiography.
Keywords: Diastolic function, echocardiography activities, left and right ventricular function, lung ultrasound
INTRODUCTION
Standardization of image acquisition and analysis, as well as defining clear reference values for each parameter, is of crucial importance in achieving uniformity in the interpretation and communication of the results of a transthoracic echocardiography (TTE), transesophageal echocardiography (TEE), and stress echocardiography (SE) examinations.[1,2]
One of the main commitments of the Italian Society of Echocardiography and Cardiovascular Imaging (SIECVI) is to improve the standardization of cardiovascular imaging practice and to support knowledge sharing. However, depending on the internal organization, workload, financial resources, expertise, and patient population, each echo laboratory may report the findings differently, use different methods of reporting and archiving images, and vary in their ability to integrate novel measurements alongside traditional assessments.
This survey aimed to analyze the activities of echocardiographic laboratories in Italy and to analyze the difference in the activities and exams across the italian macroregions (North, Center, and South), and between in cardiology and noncardiology departments.
METHODS
We analyzed the activity of echocardiography laboratories in 1 month. November 2022 was chosen as an ideal reference month (30 days; away from holidays).
A list of accredited echocardiographic laboratories was obtained from SIECVI. Each member of SIECVI was contacted by mail. Data were retrieved via an electronic survey based on a structured questionnaire uploaded on the SIECVI website (www.siec.it.)
For allocation of the response, the questionnaire required general information, such as the name of the hospital, the investigator, and the interviewed person’s name:
General information: Date, hospital’s name, department, name of the interviewed physician, city, and region of Italy
The type of organization of the laboratories
The echo machines available in the laboratories
The methods of archiving echocardiographic images
The methods of reporting echocardiographic examinations
Principal modality of booking echocardiographic examinations
The number of TTE, TEE, and SE performed
The number of echocardiographic examinations with ultrasound contrast agent (UCA)
Use of the lung ultrasound (LUS)
Use of the speckle tracking-derived myocardial deformation imaging (STE)
Modality of analysis of ejection fraction (EF), the universal standard to assess left ventricular (LV) global systolic function
Modality of analysis of diastolic function
Modality of analysis of right ventricular function.
Statistical analysis
Categorical data are expressed in terms of the number of subjects and percentage, while continuous data are expressed as mean ± standard deviation or median (minimum–maximum) depending on the variables’ distribution. For continuous variables, intergroup differences were tested with a one-way analysis of variance and inter-group comparison by Bonferroni or Kruskal–Wallis, followed by the Mann–Whitney test as appropriate. The Chi-square test or Fisher’s exact test was used to compare the distribution of categorical variables among groups.
All statistical calculations were performed using SPSS for Windows, release 20.0 (Chicago, Illinois, USA).
RESULTS
Activities and geographic distribution
Data were obtained from 228 echocardiographic laboratories: 112 centers (49%) were in northern regions of Italy (Emilia-Romagna 28, Lombardy 27, Piedmont 25, Veneto 19, Friuli-Venezia Giulia 6, Liguria 4, Trentino-Alto Adige 2, and Valle D’Aosta 1), 43 centers (19%) were in the central regions (Latium 16, Tuscany 16, Marche 6, Abruzzo 3, and Umbria 2), and 73 (32%) in southern regions (Campania 25, Apulia 15, Sicily 13, Calabria 8, Sardinia 6, Basilicata 4, and Molise 2). During the month of observation, we annotated a total of 101050 TTE examinations performed in all centers. As concern other modalities there were performed 5497 transesophageal echocardiography (TEE) examinations in 161/228 centers (71%); 4057 stress echocardiography (SE) examinations in 179/228 centers (79%); and examinations with ultrasound contrast agents (UCAs) in 151/228 centers (66%) [Figure 1].
Figure 1.
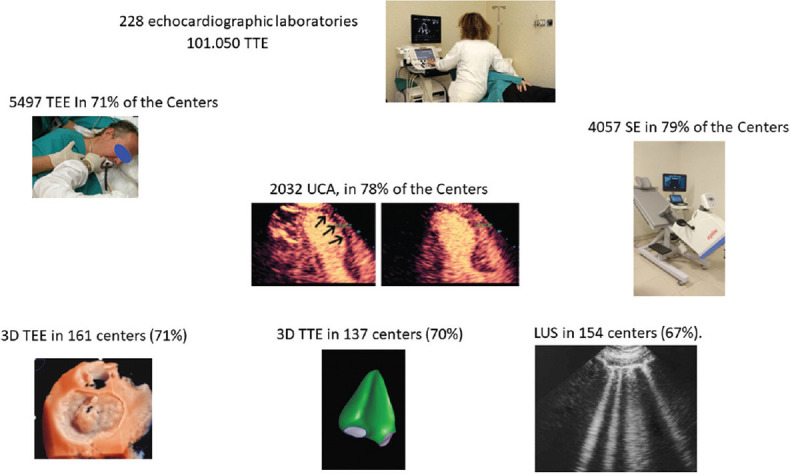
Echocardiographic laboratories activities during study period (November 2022): number of examinations and % of centers that performed: TTE = Transthoracic echocardiography, TEE = Transesophageal echocardiography, SE = Stress echocardiography, UCA = Ultrasound contrast agent, 3D TTE = Three-dimensional transthoracic echocardiography, LUS = Lung ultrasound
The echocardiographic laboratories had a median number of ultrasound units of 4 (range: 1–24), including a median value of 1 (range: 0–12) for portable machines and 1 (range: 0–11) equipped with three-dimensional (3D) probes. We did not find a significant difference in the northern, central, and southern regions concerning ultrasound units [Table 1]. However, we found substantial differences in the methods of archiving echocardiographic images and reporting echocardiographic examinations among northern, central, and southern regions [Table 1]. The use of picture archiving and communication system (PACS) was significantly different between the northern versus central and southern centers [P < 0.001, Table 1]: in addition, 2 (2%) in northern, 8 (19%) in the central, and 11 centers (15%) in the southern regions did not have an archiving mode of images and reporting echocardiographic examinations.
Table 1.
Activity of all centers and the northern, central, and southern centers
| All centers (n=228) | Northern centers (n=112) | Central centers (n=43) | Southern centers (n=73) | P | |
|---|---|---|---|---|---|
| Archiving imaging, n (%) | |||||
| PACS | 148 (65) | 94 (84) | 21 (49)* | 33 (45)* | <0.001 |
| Hard disk/CD | 59 (26) | 16 (14) | 14 (33) | 29 (40) | |
| Nothing | 21 (9) | 2 (2) | 8 (19) | 11 (15) | |
| Ultrasound units (n, median IQR) | 1019, 4 (1-24) | 522, 4 (1-24) | 188, 4 (1-16) | 309, 4 (1-24) | 0.662 |
| Portable ultrasound units (n, median IQR) | 375, 1 (0-12) | 200, 2 (0-12) | 74, 1 (0-9) | 101, 1 (0-9) | 0.191 |
| Echocardiographic examinations (n, median IQR) | 101,050, 300 (15-3130) | 57,758, 400 (20-3130) | 17,608, 250 (20-1600) | 25,684*, 250 (15-3000) | 0.041 |
| LUS performed, n (%) | 154 (66) | 68 (61) | 31 (72) | 55 (76) | 0.090 |
| LUS not performed, n (%) | 74 (34) | 44 (39) | 12 (28) | 18 (24) | |
| STE performed, n (%) | 166 (73) | 87 (78) | 24 (56)* | 55 (75) | 0.019 |
| STE not performed, n (%) | 62 (37) | 25 (22) | 16 (44) | 18 (25) | |
| 3D TTE performed, n (%) | 137 (60) | 70 (63) | 23 (53) | 47 (64) | 0.090 |
| 3D TTE not performed, n (%) | 91 (34) | 42 (37) | 20 (47) | 26 (46) | |
| TEE examinations (n, median IQR) | 5497, 15 (0-126) | 3053, 15 (0-126) | 1072, 12 (0-100) | 1372, 14 (0-80) | 0.125 |
| TEE performed, n (%) | 161 (71) | 82 (73) | 27 (63) | 52 (71) | 0.442 |
| TEE not performed, n (%) | 71 (39) | 30 (27) | 16 (37) | 21 (39) | |
| SE (n, median IQR) | 4057, 10 (0-189) | 2170, 10 (0-189) | 717, 10 (0-80) | 1170, 10 (0-90) | 0.580 |
| SE performed, n (%) | 179 (79) | 85 (76) | 33 (77) | 61 (83) | 0.661 |
| SE not performed | 49 (21) | 27 (24) | 8 (23) | 11 (17) | |
| UCA (n, median IQR) | 2032, 5 (0-60) | 1070, 5 (0-62) | 717, 5 (0-50) | 608, 5 (0-58) | 0.717 |
| UCA performed, n (%) | 151 (66) | 75 (67) | 28 (65) | 48 (66) | 0.313 |
| UCA not performed, n (%) | 77 (34) | 37 (33) | 15 (35) | 25 (34) |
*P<0.05 versus northern centers. PACS=Picture archiving and communication system, LUS=Lung ultrasound, STE=Speckle tracking-derived myocardial deformation imaging, TTE=Transthoracic echocardiography, 3D=Three dimensional, SE=Stress echocardiography, UCA=Ultrasound contrast agent, IQR=Interquartile range, TEE=Transesophageal echocardiography, CD=Compact disk
Examination booking and functional evaluations
Elective booking procedures for the echocardiographic examinations were the more frequent modality in 195 centers (86%), urgent booking in 54 centers (24%), and emergency booking in 25 centers (11%), with some centers having multiple modalities. Point-of-care ultrasound methods for the echocardiographic examinations were the more frequent modality during urgency/emergency echocardiography in 125 centers (55%), in consultancy in other departments in 85 centers (37%), and in outpatient examinations in 71 centers (31%). LUS was performed during TTE in 154 centers (67%). The principal indications were heart failure in 115 centers (75%), dyspnea in 83 centers (54%), and hemodynamic instability in the emergency department in 69 centers (45%) [Figure 2].
Figure 2.
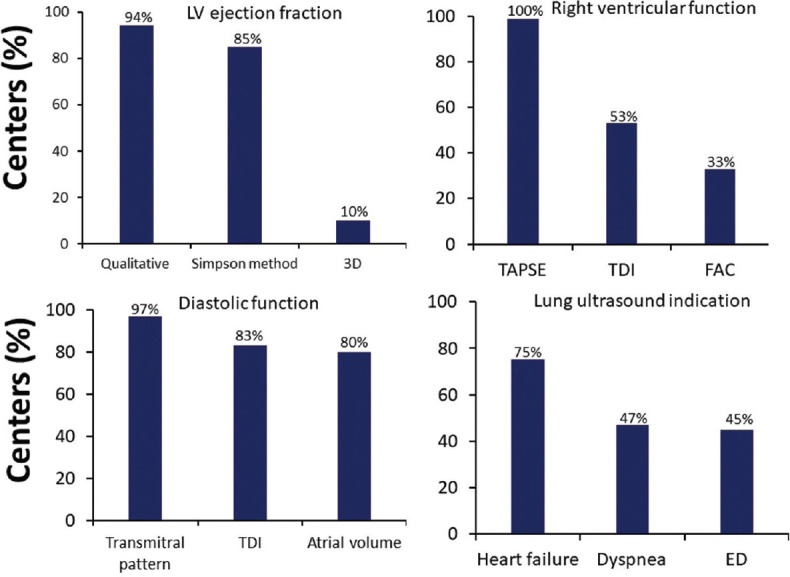
Percentage of centers that evaluated: LV EF (top on the left) using qualitative method, Simpson method or with TTE – 3D; right ventricular function (top on the right) using TAPSE, TDI, and FAC, in 75 centers (33%); diastolic function (bottom on the left) using transmitral pattern, Doppler tissue imaging of mitral annulus (TDI) and left atrial volume, and principal indication of LUS (bottom on the right) in heart failure, dyspnea, and in hemodynamic instability in ED. LV EF = Left ventricular ejection fraction, TTE 3D = Transthoracic echocardiography three-dimensional, TAPSE = Tricuspid annular plane systolic excursion, TDI = Tissue Doppler imaging, FAC = Fractional area change, LUS = Lung ultrasound, ED = Emergency department
The evaluation of LV EF was evaluated mainly using the qualitative method in 223 centers (94%), with the bidimensional Simpson method in 193 centers (85%), and with the 3D – TTE method in only 23 centers (10%). Indeed, despite 3D TTE being present in 137 centers (60%), LV volume calculation with 3D TTE was performed in 50 centers (22%) and right ventricular 3D TTE volume measurements in 19 centers (8%). On the other hand, 3D TEE was present in all centers where TEE was done TEE. LV diastolic function was done routinely in most centers (181, 80%) and analyzed in 222 centers (97%). Methods for LV diastolic function were as follows: transmitral pattern in all 222 centers, Doppler tissue imaging of mitral annulus in 189 centers (83%), and atrial volume in 184 (80%) centers.
Right ventricular function was evaluated using tricuspid annular plane systolic excursion (TAPSE) in all centers, also using tricuspid valve annular systolic velocity by tissue Doppler imaging (TDI) in 127 centers (53%), and fractional area change in 75 centers (33%).
STE was calculated in 166 centers (73%).
Echo laboratory and referral pattern
The departments involved in the survey were cardiology (179, 78.5%), internal medicine (22, 9.6%), outpatient clinic (11, 4.8%), pediatric (5, 2.2%), emergency (4, 1.8%), cardiac surgery (4, 1.8%), vascular surgery (2, 0.9%), and sport (1, 0.4%) [Figure 3].
Figure 3.
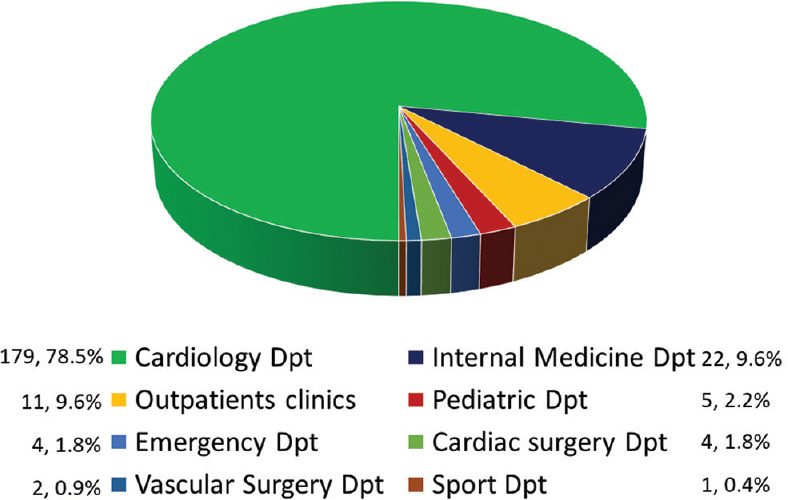
The departments (Dpt) involved in the survey
When we divided the echocardiographic laboratories afferent to cardiology (179, 78%) and noncardiology (49, 22%) units, we found significant differences in several modalities: SE (93% vs. 26%, P < 0.001), TEE (85% vs. 18%), UCA (67% vs. 43%, P < 0001), and STE (87% vs. 20%, P < 0.001). Interestingly, the incidence of LUS evaluation was similar between the cardiology and noncardiology centers (69% vs. 61%, P = NS) [Figure 4 and Table 2]. The use of PACS was significantly different in cardiology and noncardiology centers (69% vs. 51% P = 0.005). Moreover, 6 cardiology departments (6%) and 10 noncardiology departments (20%) did not archive the echocardiographic examination and did not have a reporting system.
Figure 4.
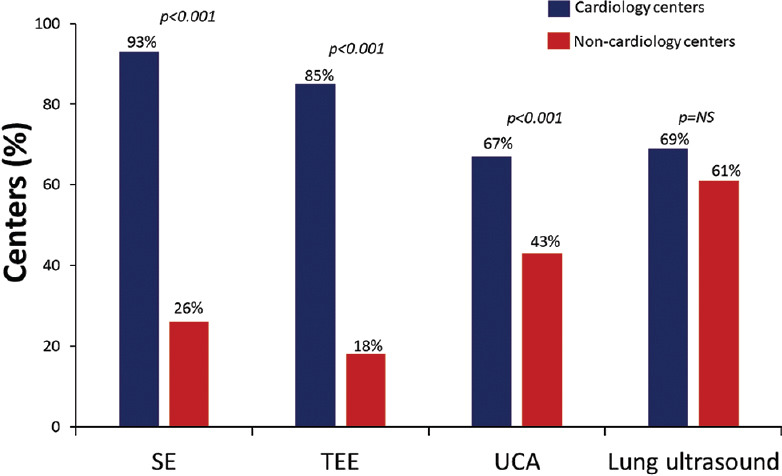
Percentage of the SE, TEE, UCA, and LUS performed in cardiology (blue bar) and noncardiology (red bar) centers. TEE = Transesophageal echocardiography, SE = Stress echocardiography, UCA = Ultrasound contrast agent, LUS = Lung ultrasound
Table 2.
Activity of cardiology and noncardiology centers
| Cardiology centers (n=179) | Noncardiology centers (n=49) | P | |
|---|---|---|---|
| Archiving imaging, n (%) | |||
| PACS | 123 (69) | 25 (51) | 0.005 |
| Hard disk/CD | 45 (25) | 14 (29) | |
| Nothing | 11 (6) | 10 (20) | |
| Ultrasound units (n, median IQR) | 887, 4 (1-24) | 132, 2 (1-6) | <0.001 |
| Portable ultrasound units (n, median IQR) | 316, 1 (0-12) | 59, 2 (0-4) | <0.001 |
| STE performed, n (%) | 156 (77) | 10 (20) | <0.001 |
| STE not performed, n (%) | 23 (13) | 39 (80) | |
| 3D TTE performed, n (%) | 127 (71) | 10 (20) | <0.001 |
| 3D TTE not performed, n (%) | 52 (29) | 39 (80) | |
| LUS performed, n (%) | 124 (69) | 30 (61) | 0.432 |
| LUS not performed, n (%) | 55 (31) | 19 (39) | |
| TEE examinations (n, median IQR) | 5295, 24 (0-126) | 202, 0 (0-60) | <0.001 |
| TEE performed, n (%) | 152 (85) | 9 (18) | <0.001 |
| TEE not performed, n (%) | 27 (15) | 40 (82) | |
| SE examinations (n, median IQR) | 3869, 10 (0-189) | 188, 0 (0-40) | <0.001 |
| SE performed, n (%) | 166 (93) | 13 (26) | <0.001 |
| SE not performed, n (%) | 13 (7) | 36 (74) | |
| UCA examinations (n, median IQR) | 1921, 8 (0-60) | 111, 1 (0-25) | <0.001 |
| UCA performed, n (%) | 130 (67) | 21 (43) | <0.001 |
| UCA not performed, n (%) | 49 (33) | 28 (57) |
PACS=Picture archiving and communication system, LUS=Lung ultrasound, STE=Speckle tracking-derived myocardial deformation imaging, TTE=Transthoracic echocardiography, 3D=Three dimensional, SE=Stress echocardiography, UCA=Ultrasound contrast agent, IQR=Interquartile range, TEE=Transesophageal echocardiography, CD=Compact disk
DISCUSSION
The present SIECVI survey involved many centers in all Italian regions and offered the opportunity to collect the amount and indications of echo-Doppler examinations. Novelties of this study were that, for the first time, SIECVI collected 101.050 TTE studies and different detailed modalities (including lung evaluation) and facilities in ultrasound units, archiving systems, and methods to obtain measurements.
During the lockdown period to oppose the coronavirus disease 2019 pandemic, cardiology divisions and echocardiographic laboratories reshaped their activities with a reduction in cardiology hospital admissions with a significant drop-off in TTE, TEE, and SE examinations.[3,4] The return to normal in terms of the number of echocardiographic examinations performed is also the result of a new organization of the echocardiography laboratories, which was previously demonstrated in a survey in 2021 during the second pandemic period.[5] In addition, the organization of echocardiographic laboratories agreed with the position papers of SIECVI,[6] which identified several measures as the most critical elements to reduce pandemic-related risks for patients and operators.[7,8]
There are significant differences in hospital infrastructure between northern versus central and southern regions of Italy: the presence of PACS systems to archive the echocardiographic images was almost double in the northern centers compared to the central and southern regions. Northern regions generally have more advanced technology and better funding.[9]
Despite this infra-structural heterogeneity, there were no differences between the centers in the echocardiographic equipment provided, volumes, and type of examinations [Table 1].
During the pandemic, there was a deferring elective procedure, with a significant reduction in elective examinations.[3] In our survey, another indicator of the return to normality is that in most of the centers, the examinations were carried out on an elective basis in 86% of the centers.
LUS has become integral to standard TTE examinations in most echocardiography laboratories. It is a useful diagnostic tool in different clinical conditions: in the first triage of symptomatic patients, in the emergency department, in the prognostic stratification and monitoring of patients with pneumonia, and in the management of patients in the intensive care unit.[10] This is largely due to the pandemic effect on echocardiography laboratories, leading to rapid and steep dissemination of LUS as a first-line examination to screen patients with suspected COVID-19 pneumonia based on the same signs (B-lines, pleural effusion, and pleural line assessment) employed for the evaluation of pulmonary congestion in heart failure.[5]
The increase in the use of LUS was similar between cardiology and noncardiology centers, possibly due to the management of heart failure in internal medicine departments and the extensive applications of LUS in rheumatology, chronic kidney disease, and intensive care unit.[10] However, significant differences are given by examinations that need a steeper learning curve and more expertise in echocardiographic imaging between cardiology and noncardiology centers, such as SE, TEE, contrast, and STE.
Cardiac point-of-care ultrasound allows rapid, focused diagnostic assessment by providers already at the bedside.[11,12] Previously, we observed a large diffusion of point-of-care cardiac ultrasound with the possibility to perform the examination not only by cardiologists but also with joint reading assessments with anesthesiologists or intensivists. This paper showed that point-of-care ultrasound methods for echocardiographic examinations were the most frequent modality during urgency/emergency echocardiography.
One of the most important advantages of 3D TTE imaging is that it allows more accurate and more reproducible measurements of LV volumes and EF compared with the two-dimensional echocardiography methodology. This advantage was recognized in the recent American Society of Echocardiography and European Association of Cardiovascular Imaging (EACVI) chamber quantification guidelines that recommend 3D TTE measurements for the left and right ventricles in laboratories with sufficient expertise.[1,13,14] Furthermore, liberal use of volumetric echocardiography for EF, STE, and UCA is recommended to improve feasibility, image quality, and information content on LV function assessed in a more quantitative way. It is probably the lack of experience and lack of familiarity with the 3D TTE method that has led to new interesting data: even though 3D TTE technology was present in 70% of the centers, measurements by 3D were performed in a minority of cases: LV volumes in 22%, right ventricular volume in 8%, and LV EF in 10% of the centers.
Disappointingly, right ventricular volume and EF measurement using 3D echocardiography was infrequently performed by most survey participants (8%). Similar data were reported in another recent EACVI survey on the multi-modality imaging assessment of the right heart,[15] in which many participants reported that RV function relies solely on the measures of tricuspid annular movement like TAPSE and TDI (S′), highlighting that the methods for assessing global right ventricular function remain underutilized.
Despite recommendations, volumetric echocardiography, right ventricular function assessment beyond TAPSE, exhaustive assessment of LV diastolic function, 3D, STE, and UCA were available in the vast majority of laboratories but applied in a small minority of patients.[13] Probably, we need a better definition of the selection of patients in whom the incremental value of these techniques is highest and compatible with the high workflow of clinically oriented laboratories. Liberal indications promulgated by recommendations are not so convincing and appealing for the practicing cardiologist in a time- and space-pressure situation. In Italy, there is no economic incentive to apply an advanced imaging technique, and cardiologists usually perform the examinations. Therefore there is less appeal for technically sweet but clinically futile image enhancement or image quantification.
CONCLUSIONS
The November 2022 snapshot of echocardiographic practice in Italy by SIECVI shows the restoration of volumes and spectrum of activities to prepandemic levels, with a significant diffuse uptake of LUS, the core TTE examination, a suboptimal diffusion of PACS recording, and conservative use of UCA, 3D, and strain. We demonstrated a gradient of technology and hospital infrastructure between Italy’s northern and central-southern regions. In addition, there was a significant difference between cardiology and noncardiology centers for second-level echocardiography examinations, such as SE and TEE.
Therefore, efforts should be made by the echocardiography community and SIECVI to define where a broader expansion of these techniques is warranted and to further promote standardization and proper training across all centers.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- 1.Galderisi M, Cosyns B, Edvardsen T, Cardim N, Delgado V, Di Salvo G, et al. Standardization of adult transthoracic echocardiography reporting in agreement with recent chamber quantification, diastolic function, and heart valve disease recommendations: An expert consensus document of the European Association of Cardiovascular Imaging. Eur Heart J Cardiovasc Imaging. 2017;18:1301–10. doi: 10.1093/ehjci/jex244. [DOI] [PubMed] [Google Scholar]
- 2.Lang RM, Badano LP, Mor-Avi V, Afilalo J, Armstrong A, Ernande L, et al. Recommendations for cardiac chamber quantification by echocardiography in adults: An update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. Eur Heart J Cardiovasc Imaging. 2015;16:233–70. doi: 10.1093/ehjci/jev014. [DOI] [PubMed] [Google Scholar]
- 3.De Rosa S, Spaccarotella C, Basso C, Calabrò MP, Curcio A, Filardi PP, et al. Reduction of hospitalizations for myocardial infarction in Italy in the COVID-19 era. Eur Heart J. 2020;41:2083–8. doi: 10.1093/eurheartj/ehaa409. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Ciampi Q, Antonini-Canterin F, Barbieri A, Barchitta A, Benedetto F, Cresti A, et al. Remodeling of activities of Italian echocardiographic laboratories during the coronavirus disease 2019 lockdown: The SIECoVId study. J Cardiovasc Med (Hagerstown) 2021;22:600–2. doi: 10.2459/JCM.0000000000001143. [DOI] [PubMed] [Google Scholar]
- 5.Ciampi Q, Antonini-Canterin F, Barbieri A, Barchitta A, Benedetto F, Cresti A, et al. Reshaping of Italian echocardiographic laboratories activities during the second wave of COVID-19 pandemic and expectations for the post-pandemic era. J Clin Med. 2021;10:3466. doi: 10.3390/jcm10163466. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Antonini-Canterin F, Pepi M, Monte IP, Trocino G, Barbieri A, Barchitta A, et al. Document addressed to cardiovascular echography operators at the time of COVID-19: A document by the “SocietàItaliana di Ecocardiografia e CardioVascular Imaging”Board 2019-2021. J Cardiovasc Echogr. 2020;30:2–4. doi: 10.4103/jcecho.jcecho_27_20. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Kirkpatrick JN, Mitchell C, Taub C, Kort S, Hung J, Swaminathan M. ASE statement on protection of patients and echocardiography service providers during the 2019 novel coronavirus outbreak: Endorsed by the American College of Cardiology. J Am Soc Echocardiogr. 2020;33:648–53. doi: 10.1016/j.echo.2020.04.001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Skulstad H, Cosyns B, Popescu BA, Galderisi M, Salvo GD, Donal E, et al. COVID-19 pandemic and cardiac imaging: EACVI recommendations on precautions, indications, prioritization, and protection for patients and healthcare personnel. Eur Heart J Cardiovasc Imaging. 2020;21:592–8. doi: 10.1093/ehjci/jeaa072. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Court of Auditors. Central Control Section on the Management of State Administrations. Interventions for the reorganization of health care in large urban areas. Resolution 12. January 2021, n. 2/2021/G. 2021 [Google Scholar]
- 10.Picano E, Scali MC, Ciampi Q, Lichtenstein D. Lung ultrasound for the cardiologist. JACC Cardiovasc Imaging. 2018;11:1692–705. doi: 10.1016/j.jcmg.2018.06.023. [DOI] [PubMed] [Google Scholar]
- 11.Kameda T, Mizuma Y, Taniguchi H, Fujita M, Taniguchi N. Point-of-care lung ultrasound for the assessment of pneumonia: A narrative review in the COVID-19 era. J Med Ultrason (2001) 2021;48:31–43. doi: 10.1007/s10396-020-01074-y. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Kirkpatrick JN, Grimm R, Johri AM, Kimura BJ, Kort S, Labovitz AJ, et al. Recommendations for echocardiography laboratories participating in cardiac point of care cardiac ultrasound (POCUS) and critical care echocardiography training: Report from the American Society of Echocardiography. J Am Soc Echocardiogr. 2020;33:409–22.e4. doi: 10.1016/j.echo.2020.01.008. [DOI] [PubMed] [Google Scholar]
- 13.Ajmone Marsan N, Michalski B, Cameli M, Podlesnikar T, Manka R, Sitges M, et al. EACVI survey on standardization of cardiac chambers quantification by transthoracic echocardiography. Eur Heart J Cardiovasc Imaging. 2020;21:119–23. doi: 10.1093/ehjci/jez297. [DOI] [PubMed] [Google Scholar]
- 14.Sitges M, Ajmone Marsan N, Cameli M, D'Andrea A, Carvalho RF, Holte E, et al. EACVI survey on the evaluation of left ventricular diastolic function. Eur Heart J Cardiovasc Imaging. 2021;22:1098–105. doi: 10.1093/ehjci/jeab087. [DOI] [PubMed] [Google Scholar]
- 15.Soliman-Aboumarie H, Joshi SS, Cameli M, Michalski B, Manka R, Haugaa K, et al. EACVI survey on the multi-modality imaging assessment of the right heart. Eur Heart J Cardiovasc Imaging. 2022;23:1417–22. doi: 10.1093/ehjci/jeac183. [DOI] [PubMed] [Google Scholar]