

Abstract
We report the outcomes in 2 patients with acquired abducens nerve palsy with residual esotropia following superior rectus transposition and medial rectus recession who subsequently underwent inferior rectus transposition as a second procedure. Both patients showed improved abduction and reduced esotropia, with no induced cyclotorsion or vertical deviation. Inferior rectus transposition as a secondary procedure in these 2 patients with abducens nerve palsy appeared to augment the effect of prior superior rectus transposition and medial rectus recession.
Case Reports
Case 1
A 22-year-old man presented with a residual esotropia after treatment of a left abducens nerve palsy with a superior rectus transposition (SRT) and medial rectus recession (MRc). Two years earlier he had been diagnosed with a clival meningioma during a work-up for a post-traumatic headache. After surgical excision of the meningioma, he developed complete paralysis of the left abducens nerve and partial paralysis of the left facial nerve. Ocular motility testing revealed −4 abduction and 55Δ esotropia in primary position, 35Δ in right gaze, and >50Δ in left gaze. The patient underwent left SRT with loop myopexy and left MRc of 10 mm. He was then referred to the Byers Eye Institute with persistent horizontal and vertical diplopia. His best-corrected visual acuity was 20/20 in both eyes. Ocular motility testing revealed 25Δ left esotropia in primary position, orthotropia in right gaze, 8Δ left hypotropia in upgaze, 12Δ left esotropia and 8Δ left hypotropia in downgaze, and 35Δ left esotropia and 14Δ left hypotropia and −4 abduction deficit in left gaze. He reported intorsion with the double Maddox rod test. One year after his initial strabismus surgery, a left inferior rectus transposition (IRT) with loop myopexy was performed. One-month postoperatively he had a 6Δ intermittent esotropia in primary position, upgaze and downgaze, orthophoria in right gaze, 30Δ left esotropia in left gaze, 2Δ intermittent esotropia at near and −3.5 abduction deficit in his left eye (Figure 1). He reported no torsion with the double Maddox rod test.
FIG 1.
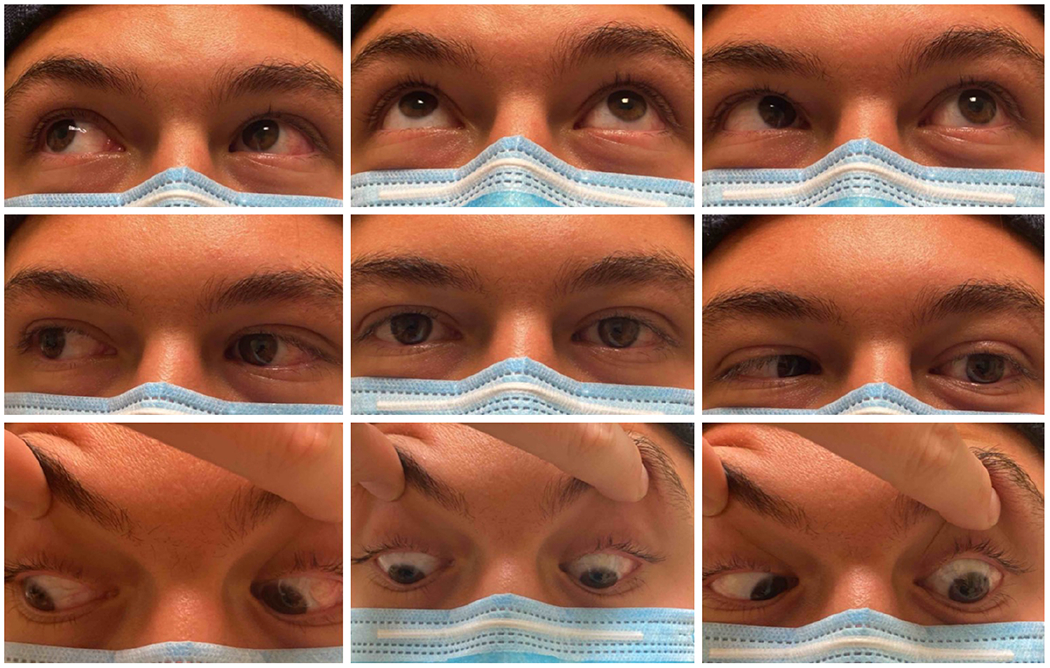
One-month postoperative ocular motility in patient 1 following inferior rectus transposition with loop myopexy. One year earlier the patient had undergone a left superior rectus transposition with loop myopexy and left medial rectus recession to correct an acquired abducens nerve palsy.
Case 2
A 23-year-old man with an acquired left abducens nerve palsy was referred to the Byers Eye Institute for consultation. Three years previously, he had developed intermittent horizonal diplopia. Neuroimaging revealed a grade 2 chondrosarcoma that was removed surgically. After neurosurgery, he developed constant horizontal diplopia. His best-corrected visual acuity was 20/20 in each eye. Ocular motility testing revealed a left esotropia of 35Δ in primary position and down gaze, 20Δ in right gaze and upgaze, >50Δ in left gaze and 25Δ at near. He had a −5 left abduction deficit. He preferred to adopt a left face turn. The patient underwent left SRT with loop myopexy and left MRc of 6 mm. One month postoperatively he had 14Δ left esotropia in primary position and downgaze, 8Δ in upgaze, 40Δ in left gaze and 8Δ at near. He was orthophoric in right gaze. The abduction deficit in the left eye had improved to −4. He reported no torsion with the double Maddox rod test.
Five months later, IRT without loop myopexy was performed as a second surgical procedure. One-month postoperatively, he had left esotropia of 6Δ in primary position and upgaze, 16δ in downgaze, 20Δ in left gaze, and 2Δ intermittent exotropia in right gaze and at near and −3 abduction in the left eye (Figure 2). He reported no torsion with the double Maddox rod test. However, mild narrowing of the palpebral fissure in the left eye was observed postoperatively.
FIG 2.

One-month postoperative ocular motility in patient 2 following inferior rectus transposition in the left eye. Five months earlier he had undergone a left superior rectus transposition with loop myopexy and a left medial rectus recession of 6 mm.
Discussion
Various surgical procedures have been used to treat patients with total abducens nerve palsies, including full or partial superior and inferior rectus transposition with or without medial rectus recession. The medial rectus muscle is generally not recessed at the same time as full transposition of both vertical rectus muscles because of the increased risk of anterior segment ischemia associated with this procedure.1–4 Full transposition of the superior rectus muscle coupled with medial rectus recession has also been described. It has a similar efficacy as full transposition of both vertical rectus muscles.2,5 Recently, Velez and colleagues6 have described full transposition of the inferior rectus muscle with or without medial rectus recession. Its efficacy in restoring ocular alignment in primary position has been reported to be similar to that of superior rectus transposition and medial rectus recession, and it can correct a concurrent vertical deviation.2,6
To our knowledge, our case series is the first to report IRT as a second procedure in patients following SRT/MRc. In both cases abduction and ocular alignment in primary position improved. After IRT, the esotropia in primary position improved from 25Δ to 6Δ in the first patient and 14Δ to 6 Δ in the second patient. The abduction deficit also improved in both patients. Loop myopexy was used in patient 1 to augment the effect of the procedure. A loop myopexy in patient 2 might have improved the outcome. A preexisting hypotropia was also corrected in patient 1. While Velez and colleagues6 used IRT as a primary surgery, we used IRT as a second procedure following SRT/MRc. IRT may have balanced the vector forces induced by SRT thereby correcting the vertical deviation. Neither patient developed torsional misalignment postoperatively. Due to the anatomical bond between the inferior rectus and the inferior tarsal muscle, IRT may cause slight narrowing of the palpebral fissure,7 as noted with patient 2. IRT improved ocular alignment in both of our patients with residual abducens nerve palsy following prior SRT/MRc.
Funding:
National Eye Institute (P30-EY026877) and Research to Prevent Blindness, New York, NY.
Footnotes
Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
Literature Search
PubMed database was searched on January 20, 2023, for English-language results using the following terms: inferior rectus transposition, sixth nerve palsy, and secondary strabismus surgery.
References
- 1.Sen S, Dhiman R, Saxena R, Phuljhele S, Sharma P. Vertical rectus transposition procedures for lateral rectus palsy: a systematic review. Indian J Ophthalmol 2019;67:1793–9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Lee YH, Lambert SR. Outcomes after superior rectus transposition and medial rectus recession versus vertical recti transposition for sixth nerve palsy. Am J Ophthalmol 2017;177:100–105. [DOI] [PubMed] [Google Scholar]
- 3.Flanders M, Qahtani F, Gans M, Beneish R. Vertical rectus muscle transposition and botulinum toxin for complete sixth nerve palsy. Can J Ophthalmol 2001;36:18–25. [DOI] [PubMed] [Google Scholar]
- 4.Nishida Y, Inatomi A, Aoki Y, et al. A muscle transposition procedure for abducens palsy, in which the halves of the vertical rectus muscle bellies are sutured onto the sclera. Jpn J Ophthalmol 2003;47:281–6. [DOI] [PubMed] [Google Scholar]
- 5.Mehendale RA, Dagi LR, Wu C, Ledoux D, Johnston S, Hunter DG. Superior rectus transposition and medial rectus recession for Duane syndrome and sixth nerve palsy. Arch Ophthalmol 2012;130:195–201. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Velez FG, Chang MY, Pineles SL. Inferior rectus transposition: a novel procedure for abducens palsy. Am J Ophthalmol 2017;177:126–30. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.American Academy of Ophthalmology. Fundamentals and Principles of Ophthalmology. 2020-2021. BSCS. [Google Scholar]