

Abstract
Background
Depressive symptoms are highly prevalent and have broad-ranging negative implications. Digital interventions are increasingly available in the workplace context, but supporting evidence is limited.
Objective
This study aimed to evaluate the feasibility, acceptability, and preliminary efficacy of 3 digital interventions for depressive symptoms in a sample of UK-based working adults experiencing mild to moderate symptoms.
Methods
This was a parallel, multiarm, pilot randomized controlled trial. Participants were allocated to 1 of 3 digital interventions or a waitlist control group and had 3 weeks to complete 6 to 8 short self-guided sessions. The 3 interventions are available on the Unmind mental health app for working adults and draw on behavioral activation, cognitive behavioral therapy, and acceptance and commitment therapy. Web-based assessments were conducted at baseline, postintervention (week 3), and at 1-month follow-up (week 7). Participants were recruited via Prolific, a web-based recruitment platform, and the study was conducted entirely on the web. Feasibility and acceptability were assessed using objective engagement data and self-reported feedback. Efficacy outcomes were assessed using validated self-report measures of mental health and functioning and linear mixed models with intention-to-treat principles.
Results
In total, 2003 individuals were screened for participation, of which 20.22% (405/2003) were randomized. A total of 92% (373/405) of the participants were retained in the study, 97.4% (295/303) initiated their allocated intervention, and 66.3% (201/303) completed all sessions. Moreover, 80.6% (229/284) of the participants rated the quality of their allocated intervention as excellent or good, and 79.6% (226/284) of the participants were satisfied or very satisfied with their intervention. All active groups showed improvements in well-being, functioning, and depressive and anxiety symptoms compared with the control group, which were maintained at 4 weeks. Hedges g effect sizes for depressive symptoms ranged from −0.53 (95% CI −0.25 to −0.81) to −0.74 (95% CI −0.45 to −1.03).
Conclusions
All interventions were feasible and acceptable, and the preliminary efficacy findings indicated that their use may improve depressive symptoms, well-being, and functioning. The predefined criteria for a definitive trial were met.
Trial Registration
International Standard Randomised Controlled Trial Number (ISRCTN) ISRCTN13067492; https://www.isrctn.com/ISRCTN13067492
Keywords: depression, digital intervention, randomized controlled trial, RCT, cognitive behavioral therapy, CBT, acceptance and commitment therapy, ACT, behavioral activation, BA, mobile phone
Introduction
Depression is primarily characterized by low mood, reduced functioning, and poor quality of life [1,2]. Although major depression has been the focus of much previous research, mild to moderate depressive symptoms are highly prevalent and are estimated to occur in approximately 20% to 22% of the general population across Europe, Asia, and the United States [3-5]. In addition, mild to moderate depression has been established as a precursor to and risk factor for major depression [6]. Here, we use the terms “mild” and “moderate” in line with the categories described by Kroenke et al [7] (and defined as those scoring between 5 and 14 on the Patient Health Questionnaire-8 [PHQ-8]). Mild to moderate depression can result in reduced functioning and both presenteeism and absenteeism in the workplace [8]. The economic costs associated with mild to moderate depression are thought to approach those of major depression [9], and it is now widely recognized that employers have a responsibility to support the mental health of their employees [1,10,11]. However, traditional face-to-face or therapist-guided psychological interventions, although effective [12,13], are not easily scalable in the workplace context and are subject to stigma and a perception of inefficacy [14,15]. Therefore, there is a considerable need for accessible, scalable interventions with established efficacy to be made available to working adults experiencing mild to moderate depressive symptoms.
Digital interventions can be scaled at low cost [16], and smartphone apps that deliver content designed to alleviate the symptoms of common mental health problems are now widely available. However, evidence regarding their impact is still emerging [17], and only a small proportion of commercially developed mental health apps have established efficacy [18,19], suggesting the need for more methodologically robust trials. A recent meta-analysis evaluating digital health interventions for depression included 83 randomized controlled trials (RCTs) and showed a significant medium overall effect versus control [20], whereas another meta-analysis focusing only on mobile interventions for depressive symptoms and including just 10 studies also reported moderate symptom reduction versus control [21]. The included programs were predominantly based on cognitive behavioral therapy (CBT) techniques [22], whereas other evidence-based therapeutic models for depression (such as acceptance and commitment therapy [ACT] and behavioral activation [BA]) were underrepresented and require more thorough evaluation. For example, a recent meta-analysis of digital ACT interventions for depression found limited evidence for reliable clinical changes in symptoms, and most interventions were therapist guided [23], suggesting a need for further evaluation of self-guided digital ACT programs. In addition, a recent overview of systematic reviews found that most digital interventions for depression are at least 6 weeks long [17], with less evidence for shorter, more condensed interventions, such as those included in this study. Finally, digital mental health interventions specifically designed for delivery in the workplace have not been widely evaluated, although evidence indicates that they can be effective in improving psychological well-being and work effectiveness [24].
This need for a broader evaluation of digital interventions for depression is further demonstrated by the reportedly low user adherence to such programs [25] and mixed findings for the acceptability of web-based mental health interventions in the workplace [26]. Given the association between adherence to digital interventions for depression and clinical outcomes [27], it is important to establish feasibility and acceptability. This is in line with recommendations from the UK Medical Research Council and the National Institute for Health Research on evaluating complex interventions, which state that interventions can be undermined by poor acceptability, compliance, and delivery and definitive trials evaluating efficacy can be subject to poor recruitment and retention [28,29]. An initial pilot study can establish feasibility and acceptability and allow for necessary adjustments to both intervention and study design before carrying out a definitive trial to determine efficacy or evaluating the specific dissemination of these interventions in real-world workplace settings.
Therefore, we conducted a pilot RCT evaluating the feasibility, acceptability, and preliminary efficacy of 3 brief, self-guided, stand-alone digital interventions for low mood and depressive symptoms available on the Unmind mental health platform. Unmind is a web-based and mobile app for working adults that features a range of content designed to help employees measure, manage, and improve their mental health and well-being. Although employees are granted access to Unmind via their employer, it can be used both within and outside the workplace. Unmind has previously been shown to be feasible and acceptable when used by healthy participants to manage symptoms of stress and anxiety or boost resilience [30], but it has not been evaluated for use by individuals with mild to moderate depression. As depression has been shown to negatively impact intervention engagement [31], we deemed it necessary to establish acceptability and report on app engagement in this novel study population. In addition, because the Unmind interventions in this study differ substantially from those previously evaluated, we deemed it important to evaluate them independently and not assume equivalency. Finally, as difficulties in recruiting participants into depression trials are very common [32], we aimed to test whether a previously used recruitment method would be feasible for this novel study population.
The Unmind interventions evaluated in this study are underpinned by BA [33], CBT [22], or ACT [34], three evidence-informed psychological therapies for depression. The Unmind app deliberately includes interventions that use different therapeutic modalities, giving the user free choice over which modality feels the most relevant and appealing to them. This is important, as a recent meta-analysis suggests that giving users autonomy and choice over intervention parameters leads to greater adherence and better clinical outcomes [35]. Thus, this study aimed to evaluate the feasibility and acceptability of the 3 interventions independently (using an efficient multiarm design) without directly comparing them.
Participants were randomized to 1 of the 3 interventions or to a waitlist control group. A waitlist design was selected to ensure that all participants were provided access to the evidence-based interventions evaluated. This approach was deemed the most appropriate for establishing intervention feasibility and acceptability, which was the primary aim of this study, as it does not require the use of an active control comparator. The study was not powered to evaluate efficacy outcomes; therefore, a passive control design with the potential to capture both specific and nonspecific intervention effects was considered the most appropriate for establishing preliminary indications of efficacy. Each intervention was assessed according to the predefined progression criteria for a definitive trial in a community-based sample of working adults experiencing mild to moderate depressive symptoms.
Methods
Trial Preregistration
This trial was conducted in line with the CONSORT (Consolidated Standards of Reporting Trials) 2010 guidelines, including extensions for pilot studies and multiarm trials [36-38], and reported in accordance with the CONSORT-EHEALTH (CONSORT of Electronic and Mobile Health Applications and Online Telehealth) checklist [39]. The study protocol was preregistered on ISRCTN (International Standard Randomised Controlled Trial Number; registration number ISRCTN13067492) and the Open Science Framework [40].
Ethics Approval, Informed Consent, and Participation
The trial was conducted according to the guidelines of the Declaration of Helsinki, and all procedures involving human participants were approved by the Sciences & Technology Cluster Research Ethics Committee at the University of Sussex (ethics reference number ER/KC226/4). Written informed consent was obtained from all trial participants. Participants received GB £10 (US $10.16) for completing each study assessment and GB £1 (US $1.16) for completing a brief screening assessment. All study data were anonymous, and a full description of the data protection procedures is included in the preregistered trial protocol.
Design and Setting
This study was a parallel, multiarm, pilot RCT with preassessment (time point 0 [baseline]; t0), postassessment (time point 1 [week 3]; t1), and follow-up assessment (time point 2 [week 6]; t2). Participants were randomly allocated to 1 of the 3 brief self-guided psychological interventions for low mood and depressive symptoms on the Unmind platform or to a waitlist control group in a 1:1:1:1 allocation ratio without stratification. All study procedures were conducted on the web in the United Kingdom.
Participants and Procedure
Eligible participants (1) were aged ≥18 years; (2) were based in the United Kingdom; (3) were fluent in English; (4) were currently in full-time or part-time employment; (5) had access to the internet; (6) had an active Prolific account; and (7) scored between 5 and 14 on the PHQ-8 (refer to the Secondary Outcome Measures section [41]), indicating mild to moderate depressive symptoms. Additional criteria included interest in, and willingness to use, the study interventions and willingness to be randomized. Individuals reporting a diagnosis of bipolar disorder, schizophrenia or other psychotic spectrum disorder, alcohol or substance use disorder, or neurocognitive disorder were excluded. Current engagement with psychological therapy for low mood or depression via a health care professional and current or previous engagement with the Unmind platform or an Unmind study were not permitted.
Participants were recruited via Prolific, and all study assessments were completed on the web via Qualtrics. Prolific is a web-based recruitment platform that has been empirically tested across key attributes such as response rates and data quality [42]. It allows researchers to advertise studies to a large and diverse participant pool (>119,000 as of February 2023), with existing demographic information per individual that can be used for initial screening. Prolific is available for individuals aged at least 18 years from most Organization for Economic Co-operation and Development countries, and participants undergo various verification and technical (eg, IP address) checks before acceptance on the platform. Individuals who met Prolific’s automated initial screening criteria (based in the United Kingdom, fluent in English, employed, and having not participated in previous studies assessing the Unmind platform) were invited to take part in a study to evaluate the impact of completing 1 of the several interventions (each of which is comprised of between 6 and 8 sessions) for symptoms of low mood, featured on the Unmind mental health app. Following informed consent, participants were directed to a brief screening questionnaire to assess study-specific eligibility criteria. Study screening was separated by sex and age bracket, with the aim of recruiting a sample demographically similar to the UK working population. Eligibility was assessed using a script programmed by the authors that automatically checked all participant responses against the eligibility criteria.
All eligible individuals were then invited to complete the baseline assessment (t0), which was preceded by the full study consent form and included a battery of measures to assess current mental health and well-being as well as demographic and treatment history data. The baseline assessment was closed once the desired sample size was achieved. Participants were then randomized into 1 of the 4 groups via the Qualtrics “randomizer” feature, which uses block randomization with variable block sizes to generate balanced groups. It was not possible to blind the participants to group assignments. The research team remained blind to the group assignment for the duration of data collection but was unblinded during the analysis. At the end of the baseline assessment, participants assigned to the intervention arms were presented with an instruction video explaining how to access their intervention, including the use of a unique anonymous ID to sign up on the Unmind platform. A written version of these instructions was also provided via Prolific. Participants then had 3 weeks to complete their allocated intervention and were sent a weekly intervention reminder message via Prolific’s anonymous messaging system. At the end of the intervention period, access to the Unmind platform was withdrawn. Participants were then sent an email invitation to complete the post (t1) assessment and a further email invitation 4 weeks after for the final follow-up (t2) assessment, via Prolific. Each invitation was followed by a reminder message 3 days later. The t1 and t2 assessments included measures of mental health and well-being conducted at t0 plus a feedback questionnaire that included questions adapted from the Mobile App Rating Scale (MARS) [43] (intervention groups only, t1). On the completion of t2, the control group was given access to the Unmind platform for 3 weeks.
Interventions
Overview
Unmind is a digital platform designed to help working adults measure, manage, and improve their mental health and well-being and has previously been described in detail [30]. This study evaluated 3 brief interventions (known as courses) available on the Unmind platform, accessible via web-based or mobile apps, intended to help users manage and improve low mood and depressive symptoms and designed to be completed over the course of several days or weeks (Figure 1). The versions of the Unmind app that were live during the 3-week intervention period were 2.90.0 to 2.92.0, and no major app changes or updates were launched. Participants had access to a modified version of the Unmind platform with only their allocated intervention available:
Figure 1.
Screenshots of the Finding Happiness course on the Unmind platform.
Activate Your Mood
Activate Your Mood (AYM) is a BA-based course consisting of eight 10-minute sessions designed to help the user understand the links between their behavior and mood and to increase their levels of activity, with the aim of improving mood. Activities encouraged between sessions include a mood diary, activity monitoring, and activity scheduling. Participants were advised to complete 1 session every other day.
Mind Your Mood
Mind Your Mood (MYM) is rooted in CBT for depression and consists of six 10-minute sessions. The course encourages the user to understand the link between cognition and mood and empowers them to spot and challenge negative thoughts. Advised activities between sessions include spotting and challenging negative thoughts and tackling rumination.
Finding Happiness
Finding Happiness (FH) is an ACT-based course and consists of 7 sessions of 10 to 18 minutes each. By examining behavior, clarifying values, and designing experiments, FH aims to help users expand their sense of meaning and purpose in the world, thereby improving their mood. Each session includes an experiential exercise (eg, mindfulness), and users were encouraged to practice these between sessions.
Outcomes
Primary Outcome Measures
In line with the guidelines for pilot studies evaluating complex interventions [44,45], the following primary outcomes were assessed via a combination of objective data (including app use data) and self-report feedback data collected at t1 and t2. Feedback data were largely based on questions adapted from the MARS—the most widely used, validated scale for evaluating the quality and content of mental health apps [43].
Feasibility: recruitment rate, intervention uptake, and retention (at t1 and t2)
Acceptability: intervention adherence (completion rate, defined as the proportion of participants completing all sessions of their allocated course within the intervention period), activity adherence (the self-reported completion rate for all additional intervention activities to be completed between sessions), participant satisfaction (“How satisfied are you with the Unmind Course you were asked to complete overall?”), and reasons for nonadherence (2 multiselect questions)
Engagement: average intervention sessions completed in each group, average number of between-session activities completed, and select questions adapted from sections A and B of the MARS at t1
Transferability of the intervention to other settings or populations: assessed by select questions adapted from section E of the MARS at t1
Relevance: assessed using subjective feedback data gathered at t1 (“Would you agree that the Unmind Course was relevant to your personal experience?”)
Bad effects: the proportion of participants who reported experiencing bad effects or lasting bad effects from the intervention (as described in the study by Carlisle et al [35]) and the proportion of participants whose PHQ-8 scores increased above the minimally clinically important difference for the PHQ-8 (≥5 points [46]), assessed at t1 and t2
Secondary Outcome Measures
To determine the preliminary efficacy of each intervention, changes in depression and anxiety symptoms, well-being, and health-related productivity loss were assessed as secondary outcomes using data collected at t0, t1 (primary end point), and t2 via the following validated questionnaires:
The PHQ-8 [41] is an 8-item scale that screens for the presence and severity of depression, with scores ranging from 0 to 24. The PHQ-8 has excellent internal consistency (Cronbach α=.89) and excellent test-retest reliability [47].
The Generalized Anxiety Disorder-7 (GAD-7) scale [48] is a 7-item scale that screens for the presence and severity of an anxiety disorder, with scores ranging from 0 to 21. The GAD-7 has excellent reliability and internal consistency (Cronbach α=.89 [48,49]).
The Short Warwick-Edinburgh Mental Well-being Scale (SWEMWBS) [50], a short 7-item version of the original 14-item Warwick-Edinburgh Mental Well-being Scale, was designed to measure aspects of mental well-being primarily related to functioning [51]. The scores range from 7 to 35. The SWEMWBS has high internal consistency (Cronbach α=.84 in the general population).
The Unmind Index is a 26-item self-report measure designed to capture the key components of positive mental well-being and specific symptoms of mental illness [52]. Scores were normalized and standardized to population norms, with a mean of 100 and an SD of 15. The Unmind Index shows excellent internal consistency for overall well-being (McDonald hierarchical ω=0.92) and all subscales (Cronbach α=.83-.92).
The Work Productivity and Activity Impairment Scale (WPAI) questionnaire [53] is a 6-item self-report measure of health-related work productivity loss for the employed population. This study used the specific health problem version (WPAI:SHP), which asks respondents questions concerning impairment owing to “low mood.” The WPAI provides 4 scores, indicating the degree of absenteeism, presenteeism (impairment while working), overall work impairment (the impact of both absenteeism and presenteeism), and overall activity impairment owing to low mood. Scores are expressed as percentages, and the WPAI has demonstrated sufficient construct validity and test-retest reliability (with correlation coefficients ranging from 0.71-0.87 for overall productivity loss) [53].
Progression Criteria
Progression criteria for a definitive trial were predefined in line with recent recommendations [54] and included full recruitment within 1 month, ≥30% intervention completion rates for interventions, ≥50% of participants reporting being “satisfied” or “very satisfied” with the brief intervention and rating the quality as “good” or “excellent,” and between-group effect sizes for secondary outcomes including at least a small effect (Hedges g ≥0.2) for change in PHQ-8 scores at t1 (intervention vs control).
Statistical Analyses
A sample size calculation indicated that approximately 100 participants per group were required to estimate feasibility outcomes with a margin of error ≤10%, based on a conservative estimate of 50% for retention and adherence. This is consistent with guidelines suggesting that 60 to 100 participants per intervention arm are optimal for estimating binary outcomes in pilot studies, such as the recruitment and completion rate outlined in the Progression Criteria section [55]. We, therefore, aimed to recruit 400 participants. The PHQ-8 score distribution of a previous UK study sample recruited via Prolific was used as a reference to estimate the appropriate number of participants required for screening (n=2000; [52]).
The primary outcomes were reported using descriptive statistics and appropriate measures of central tendency, and Fisher exact or ANOVA tests were used to compare between groups, as appropriate. Objective in-app use data were provided by Unmind, the creator of the interventions evaluated. For simplicity, the intervention sessions were only characterized as complete if all components of the session were played. Thus, for each participant, the intervention engagement ranged from 0 sessions complete to all sessions complete. Use data also included the duration of each session completed by each participant. Descriptive statistics were used to characterize engagement and stratify participants according to whether they completed, started but did not complete, or failed to start their allocated intervention.
The secondary efficacy outcomes were assessed using an intention-to-treat (ITT) approach (in which all randomized participants were included in the statistical analysis, regardless of intervention engagement or attrition) and linear mixed effects (LME) models. Each LME included “time point” as a within-subjects factor (levels: t0, t1, and t2), “group” as a between-subjects factor, and their interaction as fixed effects, with a separate baseline for each participant. The time point was coded as a categorical variable to avoid enforcing a linear relationship with outcomes. For each model fit, residuals were checked via quantile-quantile plots to assess the model assumptions and goodness of fit. For each outcome, we plotted the estimated marginal means (EMMs) for each time point and intervention arm with SEs and reported between-group contrasts (with 95% CIs) comparing changes from t0 to t1 and t0 to t2 for each intervention arm relative to the control group (with P values). We also reported a standardized effect size (Hedges g with 95% CI) for each between-group contrast. Hedges g was calculated using EMMs and pooled SDs. The 95% CIs were calculated using equations 15 and 16 from the study by Nakagawa and Cuthill [56].
Exploratory analyses examined the proportion of individuals that experienced a clinically important change in PHQ-8 score, defined according to Löwe et al [57] as a change of ≥5 from baseline and a change in subscale scores for the Unmind Index, as per the study protocol.
Owing to a technical error, planned per-protocol analyses of the secondary outcomes could not be conducted. All other preregistered primary and secondary outcomes were reported, except for the analysis of qualitative feedback. The protocol deviations are detailed in Multimedia Appendix 1.
Results
Participants
Recruitment and data collection took place between September and November 2021. A total of 405 eligible participants completed the baseline survey (Figure 2). The demographics and use of other interventions are presented in Table 1. The sample was 54.8% (222/405) female, 88.1% (357/405) White, and had a mean age of 36.9 (SD 9.5) years, which is reasonably consistent with the UK general population [58]. Baseline scores on measures of mental health, well-being, and functioning are presented in Table 2 and indicate that, on average, participants experienced mild symptoms of depression and anxiety and had below-average well-being when compared with population norms [41,48], and the majority of the participants had not accessed treatment in the last 6 months. WPAI scores showed impaired work and activity functioning owing to low mood but low rates of absenteeism. The baseline scores on the subscales of the Unmind Index are shown in Multimedia Appendix 2.
Figure 2.
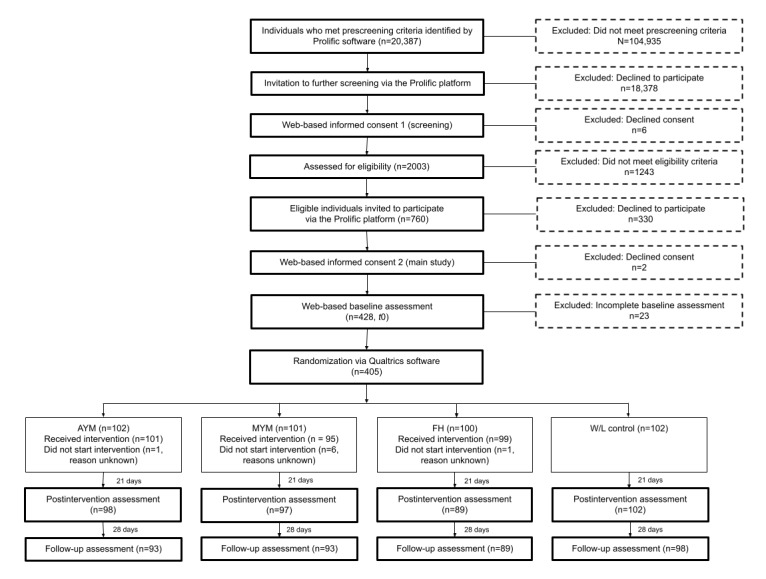
CONSORT (Consolidated Standards of Reporting Trials) flow diagram. AYM: Activate Your Mood; FH: Finding Happiness; MYM: Mind Your Mood; W/L: waitlist; t0: time point 0 (baseline).
Table 1.
Participant demographics and intervention use.
| Variable | Overall (n=405) | Study arm | |||||||||
|
|
|
Activate Your Mood (n=102) | Mind Your Mood (n=101) | Finding Happiness (n=100) | Control (n=102) | ||||||
| Age (years), mean (SD; range) | 36.9 (9.5; 18.0-67.0) | 35.7 (8.8; 18.0-62.0) | 36.7 (10.7; 20.0-67.0) | 38.2 (9.6; 19.0-63.0) | 36.9 (8.7; 19.0-59.0) | ||||||
| Sex, n (%) | |||||||||||
|
|
Female | 222 (54.8) | 61 (59.8) | 51 (50.5) | 54 (54) | 56 (54.9) | |||||
|
|
Male | 183 (45.2) | 41 (40.2) | 50 (49.5) | 46 (46) | 46 (45.1) | |||||
| Gender identity same as registered sex at birth, n (%) | |||||||||||
|
|
Yes | 404 (99.8) | 101 (99) | 101 (100) | 100 (100) | 102 (100) | |||||
| Ethnicity, n (%) | |||||||||||
|
|
Asian | 22 (5.4) | 6 (5.9) | 8 (7.9) | 3 (3) | 5 (4.9) | |||||
|
|
Black | 13 (3.2) | 6 (5.9) | 1 (1) | 3 (3) | 3 (2.9) | |||||
|
|
Mixed or multiple | 13 (3.2) | 6 (5.9) | 4 (4) | 0 (0) | 3 (2.9) | |||||
|
|
White | 357 (88.1) | 84 (82.4) | 88 (87.1) | 94 (94) | 91 (89.2) | |||||
| Employment, n (%) | |||||||||||
|
|
Full-time employee | 282 (69.6) | 70 (68.6) | 68 (67.3) | 71 (71) | 73 (71.6) | |||||
|
|
Part-time employee | 83 (20.5) | 21 (20.6) | 22 (21.8) | 19 (19.0) | 21 (20.6) | |||||
|
|
Self-employed or contractor | 40 (9.9) | 11 (10.8) | 11 (10.9) | 10 (10) | 8 (7.8) | |||||
| Industry, n (%) | |||||||||||
|
|
Agriculture, forestry, or mining | 4 (1) | 1 (1) | 1 (1) | 0 (0) | 2 (2) | |||||
|
|
Industrials | 25 (6.2) | 6 (5.9) | 7 (6.9) | 8 (8) | 4 (3.9) | |||||
|
|
Energy or utilities | 8 (2) | 0 (0) | 2 (2) | 2 (2) | 4 (3.9) | |||||
|
|
Transport or logistics | 13 (3.2) | 3 (2.9) | 3 (3) | 3 (3) | 4 (3.9) | |||||
|
|
Media or creative industries | 15 (3.7) | 5 (4.9) | 5 (5) | 5 (5) | 0 (0) | |||||
|
|
Data infrastructure or telecommunications | 9 (2.2) | 2 (2) | 3 (3) | 1 (1) | 3 (2.9) | |||||
|
|
Health care | 58 (14.3) | 19 (18.6) | 14 (13.9) | 15 (15) | 10 (9.8) | |||||
|
|
Education | 74 (18.3) | 18 (17.6) | 13 (12.9) | 15 (15) | 28 (27.5) | |||||
|
|
Life sciences | 8 (2) | 3 (2.9) | 2 (2) | 2 (2) | 1 (1) | |||||
|
|
Retail or e-commerce | 35 (8.6) | 6 (5.9) | 9 (8.9) | 14 (14) | 6 (5.9) | |||||
|
|
Hospitality, food, leisure, or travel | 15 (3.7) | 6 (5.9) | 3 (3) | 3 (3) | 3 (2.9) | |||||
|
|
Public or social service | 67 (16.5) | 13 (12.7) | 20 (19.8) | 19 (19) | 15 (14.7) | |||||
|
|
Finance, insurance, or real estate | 39 (9.6) | 9 (8.8) | 11 (10.9) | 9 (9) | 10 (9.8) | |||||
|
|
Professional services | 35 (8.6) | 11 (10.8) | 8 (7.9) | 4 (4) | 12 (11.8) | |||||
| Long-term leave, n (%) | |||||||||||
|
|
Yes (general sick leave) | 3 (0.7) | 1 (1) | 0 (0) | 1 (1) | 1 (1) | |||||
|
|
Yes (sick leave due to low mood) | 2 (0.5) | 0 (0) | N/Aa | 1 (1) | 1 (1) | |||||
|
|
Yes (any other reason) | 8 (2) | 0 (0) | 3 (3) | 4 (4) | 1 (1) | |||||
| Education, n (%) | |||||||||||
|
|
No formal qualifications | 1 (0.2) | 0 (0) | 0 (0) | 1 (1) | 0 (0) | |||||
|
|
High school education | 148 (36.5) | 37 (36.3) | 35 (34.7) | 42 (42) | 34 (33.3) | |||||
|
|
University degree | 162 (40) | 47 (46.1) | 40 (39.6) | 39 (39) | 36 (35.3) | |||||
|
|
Postgraduate degree | 94 (23.2) | 18 (17.6) | 26 (25.7) | 18 (18) | 32 (31.4) | |||||
| Intervention use in the last 6 months, n (%) | |||||||||||
|
|
Use of mental health apps | 36 (8.9) | 11 (10.8) | 8 (7.9) | 5 (5) | 12 (11.8) | |||||
|
|
Accessed employer support | 13 (3.2) | 2 (2) | 3 (3) | 7 (7) | 1 (1) | |||||
|
|
Accessed health care professional support | 34 (8.4) | 12.0 (11.8) | 9 (8.9) | 7 (7) | 6 (5.9) | |||||
|
|
Use of antidepressants | 51 (12.6) | 16.0 (15.7) | 16 (15.8) | 8 (8) | 11 (10.8) | |||||
|
|
Accessed psychological therapy | 36 (8.9) | 13 (12.7) | 9 (8.9) | 7 (7) | 7 (6.9) | |||||
|
|
Accessed other interventions | 21 (5.2) | 7 (6.9) | 4 (4) | 7 (7) | 3 (2.9) | |||||
| Intervention use at baseline, n (%) | |||||||||||
|
|
Use of mental health apps | 9 (2.2) | 2 (2) | 2 (2) | 2 (2) | 3 (2.9) | |||||
|
|
Use of antidepressants | 47 (11.6) | 14 (13.7) | 14 (13.9) | 8 (8) | 11 (10.8) | |||||
|
|
Accessing other interventions | 8 (2) | 3 (2.9) | 2 (2) | 1 (1) | 2 (2) | |||||
|
|
Accessing other self-help resources | 25 (6.2) | 7 (6.9) | 8 (8) | 5 (5) | 5 (5) | |||||
aN/A: not applicable.
Table 2.
Baseline mental health, well-being, and functioning scores.
| Variable | Overall (n=405) | Study arm | |||||||||
|
|
|
Activate Your Mood (n=102) | Mind Your Mood (n=101) | Finding Happiness (n=100) | Control (n=102) | ||||||
| Patient Health Questionnaire-8 | |||||||||||
|
|
Value, mean (SD) | 8.7 (2.6) | 8.6 (2.7) | 8.7 (2.4) | 9.1 (2.6) | 8.6 (2.7) | |||||
|
|
Value, median (IQR; range) | 8.0 (7.0-11.0; 5.0-14.0) | 8.0 (6.0-11.0; 5.0-14.0) | 8.0 (7.0-11.0; 5.0-14.0) | 9.0 (7.0-11.0; 5.0-14.0) | 8.0 (6.0-11.0; 5.0-14.0) | |||||
| Generalized Anxiety Disorder-7 | |||||||||||
|
|
Value, mean (SD) | 7.6 (4.0) | 7.7 (3.8) | 7.7 (3.7) | 7.3 (4.0) | 7.8 (4.5) | |||||
|
|
Value, median (IQR; range) | 7.0 (5.0-10.0; 0.0-20.0) | 7.0 (5.0-10.0; 1.0-19.0) | 7.0 (5.0-10.0; 2.0-18.0) | 7.0 (4.8-9.0; 0.0-20.0) | 7.0 (4.0-10.8; 1.0-20.0) | |||||
| Short Warwick-Edinburgh Mental Well-being Scale | |||||||||||
|
|
Value, mean (SD) | 19.4 (2.5) | 19.3 (2.4) | 19.4 (2.5) | 19.3 (2.3) | 19.8 (2.8) | |||||
|
|
Value, median (IQR; range) | 19.3 (18.0-20.7; 13.3-29.3) | 18.9 (18.0-20.0; 13.3-27.0) | 19.3 (17.4-20.7; 14.1-25.0) | 19.3 (17.4-20.7; 15.3-26.0) | 19.3 (18.0-21.5; 14.8-29.3) | |||||
| Unmind Index | |||||||||||
|
|
Value, mean (SD) | 93.8 (7.4) | 93.2 (6.8) | 93.6 (7.6) | 93.3 (6.9) | 95.2 (8.0) | |||||
|
|
Value, median (IQR; range) | 93.4 (89.0-98.1; 74.5-117.2) | 93.4 (87.9-97.3; 77.8-111.7) | 92.6 (89.5-98.5; 75.4-113.7) | 92.8 (89.0-98.0; 74.5-114.6) | 95.8 (90.1-99.1; 79.4-117.2) | |||||
| WPAIa absenteeism | |||||||||||
|
|
Value, mean (SD) | 4.2 (11.5) | 3.9 (11.8) | 5.3 (13.9) | 4.0 (9.5) | 3.6 (10.4) | |||||
|
|
Value, median (IQR; range) | 0.0 (0.0-2.6; 0.0-100.0) | 0.0 (0.0-2.7; 0.0-100.0) | 0.0 (0.0-1.4; 0.0-100.0) | 0.0 (0.0-3.6; 0.0-54.5) | 0.0 (0.0-1.7; 0.0-75.0) | |||||
| WPAI presenteeism | |||||||||||
|
|
Value, mean (SD) | 41.2 (20.3) | 43.5 (21.6) | 39.5 (20.4) | 39.9 (18.2) | 41.8 (20.8) | |||||
|
|
Value, median (IQR; range) | 40.0 (30.0-60.0; 0.0-90.0) | 40.0 (30.0-60.0; 0.0-80.0) | 40.0 (30.0-55.0; 0.0-90.0) | 40.0 (30.0-50.0; 0.0-90.0) | 40.0 (30.0-60.0; 0.0-90.0) | |||||
| WPAI work impairment | |||||||||||
|
|
Value, mean (SD) | 42.6 (21.3) | 44.8 (22.2) | 41.1 (21.7) | 41.4 (19.7) | 42.9 (21.5) | |||||
|
|
Value, median (IQR; range) | 40.0 (30.0-60.0; 0.0-97.5) | 46.2 (30.0-61.9; 0.0-87.5) | 40.0 (30.0-57.5; 0.0-92.0) | 40.0 (30.0-53.7; 0.0-92.7) | 40.0 (30.0-60.0; 0.0-97.5) | |||||
| WPAI activity impairment | |||||||||||
|
|
Value, mean (SD) | 44.1 (21.7) | 45.2 (20.5) | 45.8 (22.6) | 43.4 (20.9) | 42.1 (22.8) | |||||
|
|
Value, median (IQR; range) | 40.0 (30.0-60.0; 0.0-100.0) | 50.0 (30.0-60.0; 0.0-80.0) | 50.0 (30.0-60.0; 10.0-100.0) | 40.0 (30.0-60.0; 0.0-90.0) | 40.0 (20.0-60.0; 0.0-90.0) | |||||
aWPAI: Work Productivity and Activity Impairment Scale.
Primary Outcomes
Feasibility (Recruitment and Retention)
The participants were recruited in September 2021. A total of 760 eligible individuals were identified, and 405 individuals completed the baseline assessment within 48 hours. The intervention uptake and retention across the study and the reasons for ineligibility are shown in Figure 2. Overall, 95.3% (386/405) of the participants completed the t1 assessment, and 92.1% (373/405) of the participants completed the t2 assessment. The intervention update was high, with only 8 participants failing to initiate their assigned intervention across the 3 groups. Retention was significantly different between the study groups at t1 (P=.002), with FH being the lowest (89/100, 89%). There was no difference in retention between the groups at t2 (P=.27).
Acceptability and Engagement (Adherence, Satisfaction, and Feedback)
The objective adherence data obtained from the Unmind platform database are summarized in Table 3. Overall, 97.4% (295/303) of the participants started their allocated intervention, and 66.3% (201/303) of the participants completed all relevant sessions. Of those who initiated their intervention, 68.1% (201/295) went on to complete it. The mean time spent on sessions was 72.3 (SD 34.6) minutes (Table 3). This differed significantly between the intervention groups (F2,292=77.95; P<.001). Intervention completers spent a mean of 86.9 (SD 25.3) minutes engaging with sessions, again with a significant difference between the groups (F2,192=3019; P<.001). The mean number of days taken to complete was 14.3 (SD 5.7), with a significant difference between the groups (F2,192=8.21; P<.001; Table 3). Completion of the between-session activities was self-reported (Table 3). Overall, 70.4% (200/284) of the participants reported completing all recommended activities between sessions, with no significant difference between the groups (P=.30).
Table 3.
Intervention adherence.
| Variable | Overall (n=303) | Study arm | |||
|
|
|
AYMa (n=102) | MYMb (n=101) | FHc (n=100) | |
| Started interventiond | |||||
|
|
Participants, n | 295 | 101 | 95 | 99 |
|
|
Participants randomized, % (95% CI) | 97.4 (94.9-98.9) | 99 (94.7-100.0) | 94.1 (87.5-97.8) | 99 (94.6-100.0) |
| Completersd | |||||
|
|
Participants, n | 201 | 59 | 74 | 68 |
|
|
Participants randomized, % (95% CI) | 66.3 (60.7-71.6) | 57.8 (47.7-67.6) | 73.3 (63.5-81.6) | 68 (57.9-77.0) |
|
|
Participants starting intervention, % (95% CI) | 68.1 (62.6-73.2) | 58.4 (48.2-68.1) | 77.9 (68.2-85.8) | 68.7 (58.6-77.6) |
|
|
Days to complete intervention, mean (SD) | 14.3 (5.7) | 16.7 (4.3) | 13.4 (4.9) | 13.0 (6.9) |
|
|
Time (minutes) on sessions, mean (SD) | 86.9 (25.3) | 76.3 (1.6) | 64.2 (0.8) | 120.1 (7.4) |
| Partial completersd | |||||
|
|
Participants, n | 94 | 42 | 21 | 31 |
|
|
Participants randomized, % (95% CI) | 31.9 (26.8-37.4) | 41.2 (31.5-51.4) | 20.8 (13.4-30.0) | 31 (22.1-41.0) |
| Number of sessions completed (all participants)d, mean (SD) | 5.6 (2.3) | 6.0 (2.7) | 5.2 (1.7) | 5.7 (2.4) | |
| Time on course sessions (all participants)d, mean (SD) | 72.3 (34.6) | 59.5 (23.3) | 56.0 (17.2) | 100.9 (38.8) | |
| Completed all activities | |||||
|
|
Participants, n | 200 | 74 | 68 | 58 |
|
|
Participants randomized, % (95% CI) | 66 (60.4-71.3) | 72.5 (62.8-80.9) | 66.7 (62.8-80.9) | 58 (47.7-67.8) |
|
|
Participants starting intervention, % (95% CI) | 67.8 (62.1-73.1) | 73.3 (63.5-81.6) | 71.6 (61.4-80.4) | 58.6 (48.2-68.4) |
aAYM: Activate Your Mood.
bMYM: Mind Your Mood.
cFH: Finding Happiness.
dObjective adherence data obtained from the Unmind platform database.
The subjective feedback data for the intervention group participants completing the t1 assessment are presented in Table 4. Overall, 79.6% (226/284) of the participants reported being either “satisfied” or “very satisfied” with their allocated course, 56.3% (160/284) of the participants rated the course design as “moderately” or “highly interesting and fun,” and 61.9% (176/284) of the participants rated the course content as “moderately” or “highly interesting and fun.” In total, 90.8% (258/284) of the participants said that they were able to use the app immediately or that it was easy to learn how to use it. In total, 80.6% (229/284) of the participants agreed that the quality of their allocated course was either “good” or “excellent.” Ratings did not significantly differ between the groups (all P>.05; Table 4). The reported reasons for session and activity noncompletion are shown in Multimedia Appendix 3.
Table 4.
Participant feedback.
| Participant feedback | Overall (n=284; time point 1), n (%) | AYMa (n=98), n (%) | MYMb (n=97), n (%) | FHc (n=89), n (%) | P valued | ||
| Design of intervention | .66 | ||||||
|
|
Dull, not fun, or interesting at all | 2 (0.7) | 0 (0) | 1 (1.0) | 1 (1.1) |
|
|
|
|
Mostly boring | 19 (6.7) | 5 (5.1) | 7 (7.2) | 7 (7.9) |
|
|
|
|
Okay, fun enough | 103 (36.3) | 37 (37.8) | 32 (33.0) | 34 (38.2) |
|
|
|
|
Moderately interesting and fun | 123 (43.3) | 42 (42.9) | 48 (49.5) | 33 (37.1) |
|
|
|
|
Highly interesting and fun | 37 (13.0) | 14 (14.3) | 9 (9.3) | 14 (15.7) |
|
|
| Content of intervention | .32 | ||||||
|
|
Dull, not fun, or interesting at all | 3 (1.1) | 0 (0) | 1 (1.0) | 2 (2.2) |
|
|
|
|
Mostly boring | 20 (7.0) | 3 (3.1) | 7 (7.2) | 10 (11.2) |
|
|
|
|
Okay, fun enough | 85 (29.9) | 30 (30.6) | 32 (33.0) | 23 (25.8) |
|
|
|
|
Moderately interesting and fun | 124 (43.7) | 47 (48.0) | 37 (38.1) | 40 (44.9) |
|
|
|
|
Highly interesting and fun | 52 (18.3) | 18 (18.4) | 20 (20.6) | 14 (15.7) |
|
|
| Ease of intervention use | .22 | ||||||
|
|
No (limited instructions, confusing menu labels or icons, and complicated) | 5 (1.8) | 2 (2.0) | 3 (3.1) | 0 (0) |
|
|
|
|
Usable after a lot of time and effort | 5 (1.8) | 1 (1.0) | 3 (3.1) | 1 (1.1) |
|
|
|
|
Usable after some time and effort | 16 (5.6) | 9 (9.2) | 3 (3.1) | 4 (4.5) |
|
|
|
|
Easy to learn how to use the app | 124 (43.7) | 38 (38.8) | 39 (40.2) | 47 (52.8) |
|
|
|
|
Able to use the app immediately | 134 (47.2) | 48 (49.0) | 49 (50.5) | 37 (41.6) |
|
|
| Likelihood of recommending intervention | .93 | ||||||
|
|
I would not recommend it to anyone | 9 (3.2) | 3 (3.1) | 4 (4.1) | 2 (2.2) |
|
|
|
|
There are very few people I would recommend it to | 23 (8.1) | 8 (8.2) | 7 (7.2) | 8 (9.0) |
|
|
|
|
There are several people whom I would recommend it to | 105 (37.0) | 35 (35.7) | 39 (40.2) | 31 (34.8) |
|
|
|
|
There are many people I would recommend it to | 77 (27.1) | 29 (29.6) | 21 (21.6) | 27 (30.3) |
|
|
|
|
I would recommend it to everyone experiencing low mood | 70 (24.6) | 23 (23.5) | 26 (26.8) | 21 (23.6) |
|
|
| Relevance of intervention | .61 | ||||||
|
|
Strongly agree | 54 (19.0) | 15 (15.3) | 21 (21.6) | 18 (20.2) |
|
|
|
|
Agree | 162 (57.0) | 61 (62.2) | 54 (55.7) | 47 (52.8) |
|
|
|
|
Neither agree nor disagree | 41 (14.4) | 12 (12.2) | 15 (15.5) | 14 (15.7) |
|
|
|
|
Disagree | 19 (6.7) | 6 (6.1) | 4 (4.1) | 9 (10.1) |
|
|
|
|
Strongly disagree | 8 (2.8) | 4 (4.1) | 3 (3.1) | 1 (1.1) |
|
|
| Satisfaction with intervention | .34 | ||||||
|
|
Very satisfied | 83 (29.2) | 33 (33.7) | 22 (22.7) | 28 (31.5) |
|
|
|
|
Satisfied | 143 (50.4) | 47 (48.0) | 57 (58.8) | 39 (43.8) |
|
|
|
|
Neither satisfied nor dissatisfied | 47 (16.5) | 15 (15.3) | 15 (15.5) | 17 (19.1) |
|
|
|
|
Dissatisfied | 10 (3.5) | 3 (3.1) | 2 (2.1) | 5 (5.6) |
|
|
|
|
Very dissatisfied | 1 (0.4) | 0 (0) | 1 (1.0) | 0 (0) |
|
|
| Quality of intervention | .85 | ||||||
|
|
Excellent | 109 (38.4) | 39 (39.8) | 34 (35.1) | 36 (40.4) |
|
|
|
|
Good | 120 (42.3) | 40 (40.8) | 44 (45.4) | 36 (40.4) |
|
|
|
|
Okay | 52 (18.3) | 19 (19.4) | 18 (18.6) | 15 (16.9) |
|
|
|
|
Poor | 3 (1.1) | 0 (0) | 1 (1.0) | 2 (2.2) |
|
|
| Bad effects in intervention (yes) | 3 (1.1) | 0 (0) | 2 (2.1) | 1 (1.1) | .42 | ||
| Bad effects at follow-up (yes) | 2 (0.7) | 1 (1.1) | 1 (1.1) | 0 (0) | .41 | ||
aAYM: Activate Your Mood.
bMYM: Mind Your Mood.
cFH: Finding Happiness.
dFisher exact test.
Transferability and Relevance
The perceived transferability and relevance of the interventions were assessed using the t1 subjective feedback questionnaire. Overall, 51.8% (147/284) of the participants completing the assessment said that they would recommend their allocated intervention to many or all people if they were experiencing low mood, and 76.1% (216/284) of the participants agreed or strongly agreed that it was relevant to them. The ratings are summarized in Table 4 and did not differ significantly by group.
Bad Effects
In total, 98.9% (281/284) of the intervention group participants completing the postintervention assessment reported no bad effects at t1, and 99.3% (282/284) of those completing the t2 assessment reported no lasting bad effects, with no significant difference between the groups (t1: P=.42 and t2: P=.41; Table 4). Increases in PHQ-8 scores meeting the definition of meaningful deterioration (an increase ≥5 from baseline) were also assessed as a measure of bad effects. In total, 1% (1/98), 3% (3/97), and 5% (4/89) of the participants completing the t1 assessment met the criteria in each of the intervention groups (AYM, MYM, and FH, respectively). Moreover, 5% (5/93), 5% (5/93), and 2% (2/89) of the participants met the criteria at follow-up. In contrast, 12.7% (13/102) of the control group participants completing the t1 assessment met the criteria for a clinically significant increase in scores, and 12% (12/98) of the control group participants met the criteria at t2. Fisher test showed that the difference between groups was significant at both time points (P=.001 and P=.04). Post hoc omnibus tests showed the difference to be between the control group and each of the intervention arms at t1 (AYM: P=.001; MYM: P=.004; FH: P<.001) and between the control group and FH at t2 (P=.08).
Secondary Outcomes
Changes in measures of mood, anxiety, well-being, and functioning were evaluated for the ITT sample. EMMs obtained from the LME analyses for each outcome measure are shown in Figure 3. The contrast and between-group effect sizes are presented in Table 5. All intervention groups reported a significant reduction in depression (PHQ-8) and anxiety (GAD-7) scores at t1, maintained at t2, and a significant increase in well-being (SWEMWBS and Unmind Index) at t1, maintained at t2, when compared with the control group (all P<.05; Table 5). The between-group Hedges g effect sizes were in the medium range for change in depression and anxiety scores for all intervention groups at t1 and the small to medium ranges at t2. Large effects were identified for change in well-being according to the SWEMWBS or Unmind Index for the AYM and FH intervention groups at t1 and maintained at t2 according to the Unmind Index (Table 5).
Figure 3.
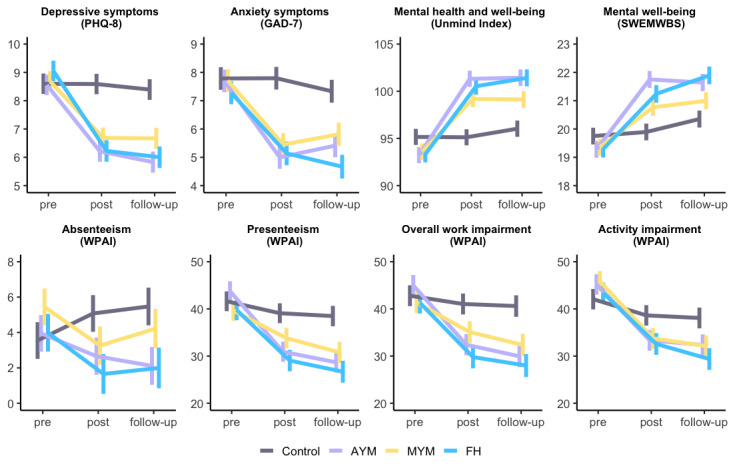
Plots showing estimated marginal means obtained from linear mixed effects models for secondary efficacy outcomes. Error bars represent SE of the mean. AYM: Activate Your Mood; FH: Finding Happiness; GAD-7: Generalized Anxiety Disorder-7; MYM: Mind Your Mood; PHQ-8: Patient Health Questionnaire-8; SWEMWBS: Short Warwick-Edinburgh Mental Well-being Scale; WPAI: Work Productivity and Activity Impairment Scale.
Table 5.
Linear mixed effects model contrasts and between-group (intervention vs control) effect sizes for secondary efficacy outcomes.
| Outcome | t1a minus t0b | t2c minus t0 | ||||||||||||
|
|
Estimate (SE; 95% CI) | P value | Hedges g (95% CI) | Estimate (SE; 95% CI) | P value | Hedges g (95% CI) | ||||||||
| Patient Health Questionnaire-8 | ||||||||||||||
|
|
AYMd | −2.34 (0.53; −3.36 to −1.31) | <.001 | −0.62 (−0.91 to −0.34) | −2.52 (0.53; −3.57 to −1.48) | <.001 | −0.66 (−0.95 to −0.38) | |||||||
|
|
MYMe | −1.99 (0.53; −3.02 to −0.96) | <.001 | −0.53 (−0.81 to −0.25) | −1.81 (0.53; −2.85 to −0.77) | <.001 | −0.48 (−0.76 to −0.20) | |||||||
|
|
FHf | −2.82 (0.54; −3.86 to −1.77) | <.001 | −0.74 (−1.03 to −0.45) | −2.84 (0.54; −3.90 to −1.79) | <.001 | −0.74 (−1.03 to −0.46) | |||||||
| Generalized Anxiety Disorder-7 | ||||||||||||||
|
|
AYM | −2.71 (0.52; −3.72 to −1.69) | <.001 | −0.73 (−1.01 to −0.44) | −1.83 (0.53; −2.87 to −0.80) | <.001 | −0.49 (−0.77 to −0.21) | |||||||
|
|
MYM | −2.28 (0.52; −3.29 to −1.26) | <.001 | −0.61 (−0.90 to −0.33) | −1.45 (0.53; −2.48 to −0.42) | .006 | −0.38 (−0.66 to −0.11) | |||||||
|
|
FH | −2.15 (0.53; −3.19 to −1.11) | <.001 | −0.57 (−0.85 to −0.29) | −2.16 (0.53; −3.21 to −1.12) | <.001 | −0.57 (−0.85 to −0.29) | |||||||
| Short Warwick-Edinburgh Mental Well-being Scale | ||||||||||||||
|
|
AYM | 2.32 (0.41; 1.5 to 3.1) | <.001 | 0.80 (0.52 to 1.09) | 1.76 (0.41; 1.0 to 2.6) | <.001 | 0.60 (0.32 to 0.88) | |||||||
|
|
MYM | 1.27 (0.41; 0.47 to 2.1) | .002 | 0.44 (0.16 to 0.72) | 1.04 (0.41; 0.23 to 1.9) | .01 | 0.35 (0.08 to 0.63) | |||||||
|
|
FH | 1.80 (0.41; 1.0 to 2.6) | <.001 | 0.61 (0.33 to 0.90) | 2.00 (0.42; 1.2 to 2.8) | <.001 | 0.68 (0.39 to 0.96) | |||||||
| Unmind Index | ||||||||||||||
|
|
AYM | 8.12 (1.13; 5.92 to 10.33) | <.001 | 1.01 (0.72 to 1.3) | 7.33 (1.15; 5.09 to 9.57) | <.001 | 0.89 (0.61 to 1.18) | |||||||
|
|
MYM | 5.62 (1.13; 3.41 to 7.83) | <.001 | 0.70 (0.41 to 0.98) | 4.67 (1.15; 2.42 to 6.91) | <.001 | 0.57 (0.29 to 0.85) | |||||||
|
|
FH | 7.25 (1.15; 5.00 to 9.50) | <.001 | 0.89 (0.59 to 1.18) | 7.22 (1.16; 4.96 to 9.49) | <.001 | 0.88 (0.59 to 1.17) | |||||||
| WPAIg absenteeism | ||||||||||||||
|
|
AYM | −2.82 (1.68; −6.10 to 0.47) | .09 | −0.23 (−0.51 to 0.04) | −3.76 (1.71; −7.09 to −0.43) | .03 | −0.31 (−0.59 to −0.03) | |||||||
|
|
MYM | −3.71 (1.70; −7.02 to −0.40) | .03 | −0.31 (−0.59 to −0.03) | −3.14 (1.73; −6.53 to 0.24) | .07 | −0.25 (−0.53 to 0.02) | |||||||
|
|
FH | −3.86 (1.73; −7.24 to −0.47) | .03 | −0.31 (−0.59 to −0.03) | −3.91 (1.77; −7.36 to −0.47) | .03 | −0.31 (−0.59 to −0.03) | |||||||
| WPAI presenteeism | ||||||||||||||
|
|
AYM | −10.31 (3.34; −16.82 to −3.79) | .002 | −0.43 (−0.71 to −0.15) | −11.93 (3.39; −18.56 to −5.31) | <.001 | −0.49 (−0.77 to −0.21) | |||||||
|
|
MYM | −3.28 (3.36; −9.83 to 3.29) | .33 | −0.14 (−0.41 to 0.14) | −5.69 (3.44; −12.40 to 1.03) | .10 | −0.23 (−0.51 to 0.05) | |||||||
|
|
FH | −8.19 (3.43; −14.89 to −1.48) | .02 | −0.34 (−0.62 to −0.06) | −9.94 (3.51; −16.78 to −3.10) | .005 | −0.40 (−0.68 to −0.12) | |||||||
| WPAI overall impairment | ||||||||||||||
|
|
AYM | −10.82 (3.42; −17.49 to −4.16) | .002 | −0.44 (−0.72 to −0.16) | −12.84 (3.48; −19.62 to −6.05) | <.001 | −0.52 (−0.80 to −0.24) | |||||||
|
|
MYM | −4.49 (3.44; −11.20 to 2.22) | .19 | −0.18 (−0.46 to 0.09) | −6.80 (3.52; −13.67 to 0.08) | .05 | −0.27 (−0.55 to 0.01) | |||||||
|
|
FH | −9.75 (3.52; −16.61 to −2.89) | .006 | −0.39 (−0.67 to −0.11) | −11.09 (3.59; −18.10 to −4.09) | .002 | −0.44 (−0.72 to −0.15) | |||||||
| WPAI activity impairment | ||||||||||||||
|
|
AYM | −8.42 (3.34; −14.94 to −1.90) | .01 | −0.35 (−0.63 to −0.08) | −8.87 (3.39; −15.49 to −2.25) | .009 | −0.37 (−0.64 to −0.09) | |||||||
|
|
MYM | −8.66 (3.35; −15.20 to −2.12) | .01 | −0.36 (−0.64 to −0.08) | −9.74 (3.40; −16.36 to −3.11) | .004 | −0.40 (−0.68 to −0.12) | |||||||
|
|
FH | −7.40 (3.41; −14.05 to −0.75) | .03 | −0.31 (−0.59 to −0.03) | −10.05 (3.43; −16.74 to −3.36) | .003 | −0.41 (−0.69 to −0.13) | |||||||
at1: time point 1 (week 3).
bt0: time point 0 (baseline).
ct2: time point 2 (week 6).
dAYM: Activate Your Mood.
eAYM: Mind Your Mood.
fFH: Finding Happiness.
gWPAI: Work Productivity and Activity Impairment Scale.
All 3 intervention groups reported a significant reduction in activity impairment owing to low mood at t1, which was maintained at t2 (all P<.05; Table 5). Both the AYM and FH groups reported a significant reduction in presenteeism and overall work impairment at t1, which was maintained at t2 (all P<.05). Some significant reductions in absenteeism were reported (P=.03; Table 5), but a large proportion of participants who completed the WPAI reported no absenteeism at baseline for the previous week (277/382, 72.5%). The between-group Hedges g effect sizes were predominantly small at t1 and t2 for WPAI outcomes (Table 5).
Subgroup Analyses and Exploratory Outcomes
Clinically Important Change
A total of 36.5% (148/405) of participants had a baseline PHQ-8 score >9, indicating that they would likely meet criteria for depression, and were therefore evaluated for clinically important change, defined as a change in score ≥5 points as per the study by Löwe et al [57]. In the AYM group, 41% (14/34) of the participants reached the threshold for clinically significant change at t1, increasing to 53% (18/34) by follow-up. In total, 35% (13/37) of the MYM participants reached a clinically significant change at t1, which increased to 41% (15/37) at t2. Moreover, 44% (17/39) of the FH participants reached this threshold by t1, which decreased slightly to 41% (16/39) at t2. Only 8% (3/39) of the control group experienced a clinically significant change by t1, which increased to 21% (8/39) at t2. There was a significant difference in the rates of clinical change between the groups at t1 (P=.002) and t2 (P=.04). Post hoc tests showed the difference to be between the control group and each of the intervention arms at t1 and the control group and AYM at t2.
Change in Unmind Index Subscale Scores
The Unmind Index is a measure of mental health and well-being, comprising 7 subscales [52]. Changes in the subscale scores were investigated as exploratory outcomes in the ITT sample using LMEs. Significantly greater changes in subscale scores were identified for each course versus control at the postintervention assessment and were maintained at follow-up (all P<.05). The only nonsignificant interaction was on the Sleep subscale (MYM vs control at t2; P=.07), and effect sizes were predominantly in the small to medium range (Multimedia Appendices 4 and 5).
Discussion
Principal Findings
This study evaluated the feasibility, acceptability, and preliminary efficacy of 3 brief digital interventions for depressive symptoms in working adults. Participants were a mildly symptomatic, largely untreated group, with below-average well-being and considerably impaired workplace functioning but low absenteeism when compared with other populations experiencing depressive symptoms [8]. All 3 interventions were found to be feasible and acceptable to this group. This was a pilot study and therefore not powered for formal hypothesis testing, but significant improvements in mental health and well-being were observed for all intervention groups compared with the waitlist control group. The between-group effect sizes ranged from small to large, and all predefined progression criteria for a definitive trial were met.
Engagement with the study interventions was high, with an overall completion rate of 66.3%, and participants spent an average of >70 minutes engaging with their allocated intervention. In addition, 70.4% (200/284) of the participants self-reported completing all additional between-session activities. This completion rate exceeded the minimum of 30% specified in our progression criteria and was higher than the 53% completion rate reported in a recent meta-analysis of digital interventions for depression, where the average number of intervention sessions was 7.3, which is comparable with this study [20]. However, the completion rate differed by intervention group and was the lowest for AYM (58%). Possible reasons for this include differences in intervention design, with AYM consisting of 8 short sessions, compared with MYM and FH, which comprise 6 and 7 sessions, respectively. AYM was the only intervention to advise a 1-day gap between sessions and contained the most extensive program of between-session activities. The reported reasons for session noncompletion support the notion that the additional time commitment associated with AYM contributed to fewer participants completing all relevant sessions. The lack of time, forgetting to engage, and reduced motivation were the most frequently reported reasons for activity noncompletion, which is in line with previous reports of barriers to engagement with digital mental health interventions [59].
Despite the differences in completion rates between interventions, there were no significant differences in subjective feedback ratings. Interestingly, ratings pertaining to how “interesting or fun” participants found the intervention content and design were considerably lower than ratings of intervention quality, ease of use, and overall satisfaction. This discrepancy may, at least in part, be because of the nature of depressive symptoms, which can include reduced capacity for interest and enjoyment and nonreactivity of mood [2]. Therefore, the ratings of interest and fun may have captured participant symptomatology rather than intervention acceptability. Although these interventions were not necessarily intended to be “fun,” increasing participant interest through an improved app design may be one area in which acceptability and engagement could be maximized in the future. Very few bad effects were reported, and the proportion of participants in the intervention groups that experienced a clinically important increase in scores was lower than the expected level of deterioration following in-person psychotherapy [60].
Preliminary efficacy findings showed a significant reduction in depressive symptoms for all 3 intervention groups when compared with a waitlist control group, with improvements maintained at the 4-week follow-up. The between-group Hedges g effect sizes were predominantly in the medium range, with CIs ranging from small to large. Although preliminary, this is broadly in line with several recent meta-analyses that evaluated digital interventions for symptoms of depression [17,20,61]. However, there are several reasons for the promising effect sizes reported in this study. First, studies that focus on mild to moderate depression and those that include self-guided interventions (without human support) tend to report smaller effect sizes [20,21]. Second, most trials included in previous meta-analyses involved longer interventions, suggesting that the current interventions may have a similar impact at a smaller effective dose. Finally, the moderate effect size for symptoms of depression following the FH intervention compares favorably with previous evaluations of ACT-based interventions that largely report small effects [23].
In addition to symptoms of depression, all intervention groups reported significant reductions in anxiety compared with the control group, and between-group effect sizes were in the medium range and maintained at follow-up. Mental well-being also significantly improved for all intervention groups, with the Unmind Index showing large effects for FH and AYM. To date, few studies on digital interventions for depressive symptoms have included well-being as an outcome, making it difficult to compare these findings with previous work, although some studies have reported small beneficial effects on quality of life. Capturing well-being outcomes may be important for understanding the broader impact of interventions beyond diagnostic symptomatology, as it provides insight into a wider range of constructs related to mental health than diagnostic tests alone [52], and mental well-being is known to have a considerable impact on various health and social outcomes [62]. Importantly, the replication of these analyses in a definitive trial is necessary to determine whether a sustained improvement in overall well-being can be achieved with digital interventions for depressive symptoms.
Reported rates of presenteeism, overall work impairment, and impairment in regular activity were significantly improved at both postintervention and follow-up for 2 of the 3 interventions. This is broadly consistent with previous studies reporting small improvements in workplace functioning following digital mental health interventions for employees [24,63]. However, few studies have specifically evaluated the impact of digital interventions for depression on workplace outcomes, suggesting a need for further research. Significant effects were also identified for absenteeism, but given the very low baseline rate, the results should be interpreted with caution and require replication. Depression is reported to be the medical condition with the greatest negative impact on time management and productivity [64], and presenteeism accounts for most of the associated cost to employers [65,66]. If replicated in a definitive trial, the reductions in presenteeism identified for FH and AYM could have important economic implications, the extent of which should be examined in the context of a definitive RCT. Although changes in presenteeism for the MYM group did not reach significance in this pilot study, scores did reduce over the study period, and changes in functioning can lag behind clinical outcomes [67]. Therefore, further evaluation of changes in presenteeism and other measures of functioning in a definitive trial is warranted for all 3 intervention groups.
The implementation of interventions specifically targeting individuals with early, milder depressive symptoms—known as indicated prevention—could help prevent symptoms from developing into more severe depressive episodes, offering personal benefit to affected individuals and reducing costs to employers. Although early evidence suggests that indicated prevention interventions for depression can produce small beneficial effects [68], outcomes in workplace settings have been mixed [69]. The findings of this study, although preliminary, suggest that the interventions evaluated in this study could have potential preventative effects by reducing the progression of depressive symptoms among employees with mild to moderate symptoms. However, further research is required to test the efficacy and effectiveness of these interventions in workplace settings and to use more rigorous diagnostic tools to test for the incidence of depression.
The Unmind app includes 3 interventions designed to tackle depressive symptoms based on CBT, BA, or ACT to provide users with choice over which therapeutic modality they feel appeals most to them. Providing a choice of interventions has been found to be associated with improved clinical outcomes and greater engagement [35,70] and thus may further ensure that the needs of adults with depressive symptoms are met. In future versions of the Unmind app, it might be possible to ask users questions that can enable the app to recommend a specific therapeutic modality deemed most suited to them, via built-in algorithms. Although a meta-analysis of psychotherapies for adult depression found generally comparable effects for these 3 modalities, the authors reported high levels of heterogeneity and a high risk of bias for most studies [71]. In addition, in a recent meta-analysis of digital interventions for depression, 74% of the included trials were based on CBT, suggesting that evidence for other therapeutic modalities is still emerging [20]. Indeed, recent meta-analyses of ACT-based [23] and BA-based [61] digital interventions concluded that more evidence is needed. Studies such as this study, which include interventions that use a variety of therapeutic modalities, may therefore help improve our understanding of non–CBT-based digital interventions for depression.
Strengths and Limitations
This study has several strengths. All procedures were preregistered, and the CONSORT guidelines were followed throughout. Participant retention was very high, meaning there was little missing data and, therefore, a low risk of bias in our estimations of intervention effects. Intervention engagement was measured objectively, which is important given the evidence of inflated rates of self-reported digital intervention use in a study setting [72]. All measures of mental health, well-being, and functioning were validated by self-report assessments, and the intervention feedback questions were adapted from an established assessment of mobile app quality.
However, this study recruited participants exclusively from Prolific; therefore, participants were a self-selected group likely to be highly motivated to engage with research and open to using a digital, app-based intervention. In addition, the completion of the study assessments was incentivized. Therefore, it remains unknown whether the findings of this study can be generalized to the wider UK working population experiencing symptoms of depression. The extent to which the wider population would be open to using app-based interventions remains unknown. In addition, it was not possible to blind participants to group allocation, as is usually the case with web-based trials. To capture feasibility and acceptability outcomes, we adapted questions from the original expert-rater version of the MARS rather than the newer user-specific version [73], which would have been a more appropriate means of gathering intervention feedback in this study. To reduce participant burden, we also included only a subset of questions from the MARS that were deemed to be the most relevant and not the full scale. This included feasibility outcomes identified as being important for evaluating complex interventions [45] but excluded factors such as intervention esthetics.
We also noted that absenteeism rates in our study sample were low at baseline, and regression model diagnosis using quantile-quantile plots indicated that the residuals were not normally distributed. Therefore, any efficacy findings pertaining to absenteeism should be interpreted with caution. We were also unable to conduct planned exploratory analyses to evaluate the impact of intervention engagement because of a technical error. This study used a waitlist, passive control group design, meaning that inferences cannot be made about intervention mechanisms of action at this stage, although we note that such an evaluation was not the aim of this study. Furthermore, this was a pilot trial with the primary aim of evaluating intervention feasibility and acceptability and was not powered for formal hypothesis testing. Therefore, replication of the efficacy analyses reported in this study in a larger definitive RCT is essential, and the efficacy findings in this study should be interpreted with appropriate caution. Finally, although this study recruited working adults, the study interventions were not evaluated in a workplace setting, and it remains unknown whether the findings reported in this study would translate to such settings. Further evaluation using real-world effectiveness trials is required.
Conclusions
This pilot study demonstrates the feasibility and acceptability of 3 brief digital interventions available on the Unmind app to help tackle the low mood and depressive symptoms experienced by working adults. Preliminary efficacy findings indicate that the use of the interventions evaluated may support improvements in depression, anxiety, well-being, and functioning, according to validated self-report measures. The between-group effect sizes associated with the interventions were broadly in line with those reported in the existing RCT literature examining self-guided digital interventions for depression. Indications of significantly reduced presenteeism provide a rationale for further examination of changes in functioning and the possible associated economic implications for employers. Importantly, a definitive trial to establish the efficacy of these digital interventions is warranted, as all predefined progression criteria were met.
Acknowledgments
This study was funded by Unmind Ltd, the creator of the interventions evaluated.
Abbreviations
- ACT
acceptance and commitment therapy
- AYM
Activate Your Mood
- BA
behavioral activation
- CBT
cognitive behavioral therapy
- CONSORT
Consolidated Standards of Reporting Trials
- CONSORT-EHEALTH
Consolidated Standards of Reporting Trials of Electronic and Mobile Health Applications and Online Telehealth
- EMM
estimated marginal mean
- FH
Finding Happiness
- GAD-7
Generalized Anxiety Disorder-7
- ISRCTN
International Standard Randomised Controlled Trial Number
- ITT
intention-to-treat
- LME
linear mixed effects
- MARS
Mobile App Rating Scale
- MYM
Mind Your Mood
- PHQ-8
Patient Health Questionnaire-8
- RCT
randomized controlled trial
- SWEMWBS
Short Warwick-Edinburgh Mental Well-being Scale
- t0
time point 0 (baseline)
- t1
time point 1 (week 3)
- t2
time point 2 (week 6)
- WPAI
Work Productivity and Activity Impairment Scale
Protocol deviations.
Baseline scores on the subscales of the Unmind Index measure of mental health and well-being.
Reported reasons for session and activity noncompletion, obtained at t1 (time point 1; week 3).
Plots of estimated marginal means obtained from the linear mixed effects models for the 7 subscales of the Unmind Index.
Contrasts and between-group (intervention vs control) effect size calculations from linear mixed effects models applied to each of the 7 Unmind Index subscales.
CONSORT-eHEALTH checklist (V 1.6.1).
Data Availability
The data sets generated and analyzed during this study are available from the corresponding author on reasonable request.
Footnotes
Authors' Contributions: RWT, ME, HB, and KC designed the study. RWT and RM collected the data. RWT analyzed the data with input from ME. RWT and RM wrote the initial draft of the manuscript. All authors discussed the interpretation of the findings, contributed to the final manuscript, and approved the final manuscript.
Conflicts of Interest: RWT was employed by Unmind Ltd at the time this work was conducted. RM, ME, and HB are employed by and own share options at Unmind Ltd. KC is a formal academic collaborator and receives financial compensation to provide scientific and research consulting services to Unmind Ltd.
References
- 1.Whiteford HA, Degenhardt L, Rehm J, Baxter AJ, Ferrari AJ, Erskine HE, Charlson FJ, Norman RE, Flaxman AD, Johns N, Burstein R, Murray CJ, Vos T. Global burden of disease attributable to mental and substance use disorders: findings from the Global Burden of Disease Study 2010. Lancet. 2013 Nov 09;382(9904):1575–86. doi: 10.1016/S0140-6736(13)61611-6.S0140-6736(13)61611-6 [DOI] [PubMed] [Google Scholar]
- 2.The ICD-10 classification of mental and behavioural disorders: clinical descriptions and diagnostic guidelines. World Health Organization. 1992. Jan 01, [2021-04-26]. https://apps.who.int/iris/handle/10665/37958 .
- 3.Kocalevent RD, Hinz A, Brähler E. Standardization of the depression screener patient health questionnaire (PHQ-9) in the general population. Gen Hosp Psychiatry. 2013 Sep;35(5):551–5. doi: 10.1016/j.genhosppsych.2013.04.006.S0163-8343(13)00127-8 [DOI] [PubMed] [Google Scholar]
- 4.Shin C, Ko YH, An H, Yoon HK, Han C. Normative data and psychometric properties of the patient health questionnaire-9 in a nationally representative Korean population. BMC Psychiatry. 2020 Apr 30;20(1):194. doi: 10.1186/s12888-020-02613-0. https://bmcpsychiatry.biomedcentral.com/articles/10.1186/s12888-020-02613-0 .10.1186/s12888-020-02613-0 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Wittayanukorn S, Qian J, Hansen RA. Prevalence of depressive symptoms and predictors of treatment among U.S. adults from 2005 to 2010. Gen Hosp Psychiatry. 2014 May;36(3):330–6. doi: 10.1016/j.genhosppsych.2013.12.009.S0163-8343(13)00374-5 [DOI] [PubMed] [Google Scholar]
- 6.Zhang R, Peng X, Song X, Long J, Wang C, Zhang C, Huang R, Lee TM. The prevalence and risk of developing major depression among individuals with subthreshold depression in the general population. Psychol Med (forthcoming) 2022 Feb 14;:1–10. doi: 10.1017/S0033291722000241.S0033291722000241 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Kroenke K, Spitzer RL, Williams JB. The PHQ-9: validity of a brief depression severity measure. J Gen Intern Med. 2001 Sep;16(9):606–13. doi: 10.1046/j.1525-1497.2001.016009606.x. https://europepmc.org/abstract/MED/11556941 .jgi01114 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Beck A, Crain AL, Solberg LI, Unützer J, Glasgow RE, Maciosek MV, Whitebird R. Severity of depression and magnitude of productivity loss. Ann Fam Med. 2011 Jul;9(4):305–11. doi: 10.1370/afm.1260. http://www.annfammed.org/cgi/pmidlookup?view=long&pmid=21747101 .9/4/305 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Cuijpers P, Smit F, Oostenbrink J, de Graaf R, Ten Have M, Beekman A. Economic costs of minor depression: a population-based study. Acta Psychiatr Scand. 2007 Mar;115(3):229–36. doi: 10.1111/j.1600-0447.2006.00851.x.ACP851 [DOI] [PubMed] [Google Scholar]
- 10.Work-related stress, anxiety or depression statistics in Great Britain, 2019. Health and Safety Executive. 2020. [2021-09-01]. https://www.hse.gov.uk/statistics/causdis/stress.pdf .
- 11.Johnston DA, Harvey SB, Glozier N, Calvo RA, Christensen H, Deady M. The relationship between depression symptoms, absenteeism and presenteeism. J Affect Disord. 2019 Sep 01;256:536–40. doi: 10.1016/j.jad.2019.06.041.S0165-0327(19)30028-X [DOI] [PubMed] [Google Scholar]
- 12.Bai Z, Luo S, Zhang L, Wu S, Chi I. Acceptance and commitment therapy (ACT) to reduce depression: a systematic review and meta-analysis. J Affect Disord. 2020 Jan 01;260:728–37. doi: 10.1016/j.jad.2019.09.040.S0165-0327(19)31302-3 [DOI] [PubMed] [Google Scholar]
- 13.Santoft F, Axelsson E, Öst LG, Hedman-Lagerlöf M, Fust J, Hedman-Lagerlöf E. Cognitive behaviour therapy for depression in primary care: systematic review and meta-analysis. Psychol Med. 2019 Jun;49(8):1266–74. doi: 10.1017/S0033291718004208.S0033291718004208 [DOI] [PubMed] [Google Scholar]
- 14.Cuijpers P, van Straten A, Warmerdam L, van Rooy MJ. Recruiting participants for interventions to prevent the onset of depressive disorders: possible ways to increase participation rates. BMC Health Serv Res. 2010 Jun 25;10:181. doi: 10.1186/1472-6963-10-181. https://bmchealthservres.biomedcentral.com/articles/10.1186/1472-6963-10-181 .1472-6963-10-181 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Lipschitz J, Miller CJ, Hogan TP, Burdick KE, Lippin-Foster R, Simon SR, Burgess J. Adoption of mobile apps for depression and anxiety: cross-sectional survey study on patient interest and barriers to engagement. JMIR Ment Health. 2019 Jan 25;6(1):e11334. doi: 10.2196/11334. https://mental.jmir.org/2019/1/e11334/ v6i1e11334 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Rogers MA, Lemmen K, Kramer R, Mann J, Chopra V. Internet-delivered health interventions that work: systematic review of meta-analyses and evaluation of website availability. J Med Internet Res. 2017 Mar 24;19(3):e90. doi: 10.2196/jmir.7111. https://www.jmir.org/2017/3/e90/ v19i3e90 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Khademian F, Aslani A, Bastani P. The effects of mobile apps on stress, anxiety, and depression: overview of systematic reviews. Int J Technol Assess Health Care. 2020 Dec 14;37:e4. doi: 10.1017/S0266462320002093.S0266462320002093 [DOI] [PubMed] [Google Scholar]
- 18.Bauer M, Glenn T, Geddes J, Gitlin M, Grof P, Kessing LV, Monteith S, Faurholt-Jepsen M, Severus E, Whybrow PC. Smartphones in mental health: a critical review of background issues, current status and future concerns. Int J Bipolar Disord. 2020 Jan 10;8(1):2. doi: 10.1186/s40345-019-0164-x. https://europepmc.org/abstract/MED/31919635 .10.1186/s40345-019-0164-x [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Lau N, O'Daffer A, Colt S, Yi-Frazier J, Palermo T, Rosenberg A. Popular smartphone apps to improve wellness and reduce stress: science or snake oil? (RP402) J Pain Symptom Manage. 2020 Jul;60(1):214–5. doi: 10.1016/j.jpainsymman.2020.04.070. https://www.jpsmjournal.com/article/S0885-3924(20)30289-X/fulltext . [DOI] [Google Scholar]
- 20.Moshe I, Terhorst Y, Philippi P, Domhardt M, Cuijpers P, Cristea I, Pulkki-Råback L, Baumeister H, Sander LB. Digital interventions for the treatment of depression: a meta-analytic review. Psychol Bull. 2021 Aug;147(8):749–86. doi: 10.1037/bul0000334.2022-09577-001 [DOI] [PubMed] [Google Scholar]
- 21.Serrano-Ripoll MJ, Zamanillo-Campos R, Fiol-DeRoque MA, Castro A, Ricci-Cabello I. Impact of smartphone app-based psychological interventions for reducing depressive symptoms in people with depression: systematic literature review and meta-analysis of randomized controlled trials. JMIR Mhealth Uhealth. 2022 Jan 27;10(1):e29621. doi: 10.2196/29621. https://mhealth.jmir.org/2022/1/e29621/ v10i1e29621 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Beck AT. Cognitive Therapy and the Emotional Disorders. Oxford, UK: International Universities Press; 1976. [Google Scholar]
- 23.Thompson EM, Destree L, Albertella L, Fontenelle LF. Internet-based acceptance and commitment therapy: a transdiagnostic systematic review and meta-analysis for mental health outcomes. Behav Ther. 2021 Mar;52(2):492–507. doi: 10.1016/j.beth.2020.07.002.S0005-7894(20)30100-3 [DOI] [PubMed] [Google Scholar]
- 24.Carolan S, Harris PR, Cavanagh K. Improving employee well-being and effectiveness: systematic review and meta-analysis of web-based psychological interventions delivered in the workplace. J Med Internet Res. 2017 Jul 26;19(7):e271. doi: 10.2196/jmir.7583. https://www.jmir.org/2017/7/e271/ v19i7e271 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Linardon J, Fuller-Tyszkiewicz M. Attrition and adherence in smartphone-delivered interventions for mental health problems: a systematic and meta-analytic review. J Consult Clin Psychol. 2020 Jan;88(1):1–13. doi: 10.1037/ccp0000459.2019-66487-001 [DOI] [PubMed] [Google Scholar]
- 26.Scheutzow J, Attoe C, Harwood J. Acceptability of web-based mental health interventions in the workplace: systematic review. JMIR Ment Health. 2022 May 11;9(5):e34655. doi: 10.2196/34655. https://mental.jmir.org/2022/5/e34655/ v9i5e34655 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Fuhr K, Schröder J, Berger T, Moritz S, Meyer B, Lutz W, Hohagen F, Hautzinger M, Klein JP. The association between adherence and outcome in an internet intervention for depression. J Affect Disord. 2018 Mar 15;229:443–9. doi: 10.1016/j.jad.2017.12.028.S0165-0327(17)32480-1 [DOI] [PubMed] [Google Scholar]
- 28.Craig P, Dieppe P, Macintyre S, Michie S, Nazareth I, Petticrew M. Developing and evaluating complex interventions: the new medical research council guidance. Int J Nurs Stud. 2013 May;50(5):587–92. doi: 10.1016/j.ijnurstu.2012.09.010. https://core.ac.uk/reader/12828016?utm_source=linkout .S0020-7489(12)00306-9 [DOI] [PubMed] [Google Scholar]
- 29.Skivington K, Matthews L, Simpson SA, Craig P, Baird J, Blazeby JM, Boyd KA, Craig N, French DP, McIntosh E, Petticrew M, Rycroft-Malone J, White M, Moore L. A new framework for developing and evaluating complex interventions: update of medical research council guidance. BMJ. 2021 Sep 30;374:n2061. doi: 10.1136/bmj.n2061. http://www.bmj.com/lookup/pmidlookup?view=long&pmid=34593508 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Economides M, Bolton H, Male R, Cavanagh K. Feasibility and preliminary efficacy of web-based and mobile interventions for common mental health problems in working adults: multi-arm randomized pilot trial. JMIR Form Res. 2022 Mar 03;6(3):e34032. doi: 10.2196/34032. https://formative.jmir.org/2022/3/e34032/ v6i3e34032 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Lipschitz JM, Van Boxtel R, Torous J, Firth J, Lebovitz JG, Burdick KE, Hogan TP. Digital mental health interventions for depression: scoping review of user engagement. J Med Internet Res. 2022 Oct 14;24(10):e39204. doi: 10.2196/39204. https://www.jmir.org/2022/10/e39204/ v24i10e39204 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Hughes-Morley A, Young B, Waheed W, Small N, Bower P. Factors affecting recruitment into depression trials: systematic review, meta-synthesis and conceptual framework. J Affect Disord. 2015 Feb 01;172:274–90. doi: 10.1016/j.jad.2014.10.005. https://linkinghub.elsevier.com/retrieve/pii/S0165-0327(14)00627-2 .S0165-0327(14)00627-2 [DOI] [PubMed] [Google Scholar]
- 33.Jacobson NS, Martell CR, Dimidjian S. Behavioral activation treatment for depression: returning to contextual roots. Clin Psychol: Sci Pract. 2006 May 11;8(3):255–70. doi: 10.1093/clipsy.8.3.255. https://onlinelibrary.wiley.com/doi/abs/10.1093/clipsy.8.3.255 . [DOI] [Google Scholar]
- 34.Hayes SC, Strosahl KD, Wilson KG. Acceptance and Commitment Therapy: An Experiential Approach to Behavior Change. New York, NY, USA: The Guilford Press; 1999. [Google Scholar]
- 35.Carlisle S, Ayling K, Jia R, Buchanan H, Vedhara K. The effect of choice interventions on retention-related, behavioural and mood outcomes: a systematic review with meta-analysis. Health Psychol Rev. 2022 Jun;16(2):220–56. doi: 10.1080/17437199.2021.1962386. [DOI] [PubMed] [Google Scholar]
- 36.Eldridge SM, Chan CL, Campbell MJ, Bond CM, Hopewell S, Thabane L, Lancaster GA, PAFS consensus group CONSORT 2010 statement: extension to randomised pilot and feasibility trials. BMJ. 2016 Oct 24;355:i5239. doi: 10.1136/bmj.i5239. http://www.bmj.com/lookup/pmidlookup?view=long&pmid=27777223 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Juszczak E, Altman DG, Hopewell S, Schulz K. Reporting of multi-arm parallel-group randomized trials: extension of the CONSORT 2010 statement. JAMA. 2019 Apr 23;321(16):1610–20. doi: 10.1001/jama.2019.3087.2731183 [DOI] [PubMed] [Google Scholar]
- 38.Schulz KF, Altman DG, Moher D, CONSORT Group CONSORT 2010 statement: updated guidelines for reporting parallel group randomised trials. BMJ. 2010 Mar 23;340:c332. doi: 10.1136/bmj.c332. https://europepmc.org/abstract/MED/20332509 .bmj.c332 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Eysenbach G, CONSORT-EHEALTH Group CONSORT-EHEALTH: improving and standardizing evaluation reports of web-based and mobile health interventions. J Med Internet Res. 2011 Dec 31;13(4):e126. doi: 10.2196/jmir.1923. https://www.jmir.org/2011/4/e126/ v13i4e126 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Taylor R. Feasibility and preliminary efficacy of digital interventions for depressive symptoms in working adults: a multi-arm randomised pilot trial. Open Science Framework. 2021. Sep 21, [2023-05-15]. https://osf.io/4gruv/ [DOI] [PMC free article] [PubMed]
- 41.Kroenke K, Strine TW, Spitzer RL, Williams JB, Berry JT, Mokdad AH. The PHQ-8 as a measure of current depression in the general population. J Affect Disord. 2009 Apr;114(1-3):163–73. doi: 10.1016/j.jad.2008.06.026.S0165-0327(08)00282-6 [DOI] [PubMed] [Google Scholar]
- 42.Peer E, Brandimarte L, Samat S, Acquisti A. Beyond the Turk: alternative platforms for crowdsourcing behavioral research. J Exp Soc Psychol. 2017 May;70:153–63. doi: 10.1016/j.jesp.2017.01.006. https://www.sciencedirect.com/science/article/abs/pii/S0022103116303201 . [DOI] [Google Scholar]
- 43.Stoyanov SR, Hides L, Kavanagh DJ, Zelenko O, Tjondronegoro D, Mani M. Mobile app rating scale: a new tool for assessing the quality of health mobile apps. JMIR Mhealth Uhealth. 2015 Mar 11;3(1):e27. doi: 10.2196/mhealth.3422. https://mhealth.jmir.org/2015/1/e27/ v3i1e27 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Crawford MJ, Thana L, Farquharson L, Palmer L, Hancock E, Bassett P, Clarke J, Parry GD. Patient experience of negative effects of psychological treatment: results of a national survey†. Br J Psychiatry. 2016 Mar;208(3):260–5. doi: 10.1192/bjp.bp.114.162628. http://hdl.handle.net/10044/1/26121 .S0007125000279427 [DOI] [PubMed] [Google Scholar]
- 45.O'Cathain A, Croot L, Duncan E, Rousseau N, Sworn K, Turner KM, Yardley L, Hoddinott P. Guidance on how to develop complex interventions to improve health and healthcare. BMJ Open. 2019 Aug 15;9(8):e029954. doi: 10.1136/bmjopen-2019-029954. https://bmjopen.bmj.com/lookup/pmidlookup?view=long&pmid=31420394 .bmjopen-2019-029954 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46.Löwe B, Kroenke K, Herzog W, Gräfe K. Measuring depression outcome with a brief self-report instrument: sensitivity to change of the Patient Health Questionnaire (PHQ-9) J Affect Disord. 2004 Jul;81(1):61–6. doi: 10.1016/S0165-0327(03)00198-8.S0165032703001988 [DOI] [PubMed] [Google Scholar]
- 47.Arroll B, Goodyear-Smith F, Crengle S, Gunn J, Kerse N, Fishman T, Falloon K, Hatcher S. Validation of PHQ-2 and PHQ-9 to screen for major depression in the primary care population. Ann Fam Med. 2010 Jul;8(4):348–53. doi: 10.1370/afm.1139. http://www.annfammed.org/cgi/pmidlookup?view=long&pmid=20644190 .8/4/348 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48.Spitzer RL, Kroenke K, Williams JB, Löwe B. A brief measure for assessing generalized anxiety disorder: the GAD-7. Arch Intern Med. 2006 May 22;166(10):1092–7. doi: 10.1001/archinte.166.10.1092.166/10/1092 [DOI] [PubMed] [Google Scholar]
- 49.Löwe B, Decker O, Müller S, Brähler E, Schellberg D, Herzog W, Herzberg PY. Validation and standardization of the Generalized Anxiety Disorder Screener (GAD-7) in the general population. Med Care. 2008 Mar;46(3):266–74. doi: 10.1097/MLR.0b013e318160d093.00005650-200803000-00006 [DOI] [PubMed] [Google Scholar]
- 50.Tennant R, Hiller L, Fishwick R, Platt S, Joseph S, Weich S, Parkinson J, Secker J, Stewart-Brown S. The Warwick-Edinburgh Mental Well-being Scale (WEMWBS): development and UK validation. Health Qual Life Outcomes. 2007 Nov 27;5:63. doi: 10.1186/1477-7525-5-63. https://hqlo.biomedcentral.com/articles/10.1186/1477-7525-5-63 .1477-7525-5-63 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 51.Stewart-Brown S, Tennant A, Tennant R, Platt S, Parkinson J, Weich S. Internal construct validity of the Warwick-Edinburgh Mental Well-being Scale (WEMWBS): a Rasch analysis using data from the Scottish health education population survey. Health Qual Life Outcomes. 2009 Feb 19;7:15. doi: 10.1186/1477-7525-7-15. https://hqlo.biomedcentral.com/articles/10.1186/1477-7525-7-15 .1477-7525-7-15 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 52.Sierk A, Travers E, Economides M, Loe BS, Sun L, Bolton H. A new digital assessment of mental health and well-being in the workplace: development and validation of the unmind index. JMIR Ment Health. 2022 Jan 17;9(1):e34103. doi: 10.2196/34103. https://mental.jmir.org/2022/1/e34103/ v9i1e34103 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 53.Reilly MC, Zbrozek AS, Dukes EM. The validity and reproducibility of a work productivity and activity impairment instrument. Pharmacoeconomics. 1993 Nov;4(5):353–65. doi: 10.2165/00019053-199304050-00006. [DOI] [PubMed] [Google Scholar]
- 54.Mbuagbaw L, Kosa SD, Lawson DO, Stalteri R, Olaiya OR, Alotaibi A, Thabane L. The reporting of progression criteria in protocols of pilot trials designed to assess the feasibility of main trials is insufficient: a meta-epidemiological study. Pilot Feasibility Stud. 2019 Nov 03;5:120. doi: 10.1186/s40814-019-0500-z. https://pilotfeasibilitystudies.biomedcentral.com/articles/10.1186/s40814-019-0500-z .500 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 55.Teare MD, Dimairo M, Shephard N, Hayman A, Whitehead A, Walters SJ. Sample size requirements to estimate key design parameters from external pilot randomised controlled trials: a simulation study. Trials. 2014 Jul 03;15:264. doi: 10.1186/1745-6215-15-264. https://trialsjournal.biomedcentral.com/articles/10.1186/1745-6215-15-264 .1745-6215-15-264 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 56.Nakagawa S, Cuthill IC. Effect size, confidence interval and statistical significance: a practical guide for biologists. Biol Rev Camb Philos Soc. 2007 Nov;82(4):591–605. doi: 10.1111/j.1469-185X.2007.00027.x.BRV27 [DOI] [PubMed] [Google Scholar]
- 57.Löwe B, Unützer J, Callahan CM, Perkins AJ, Kroenke K. Monitoring depression treatment outcomes with the Patient Health Questionnaire-9. Med Care. 2004 Dec;42(12):1194–201. doi: 10.1097/00005650-200412000-00006.00005650-200412000-00006 [DOI] [PubMed] [Google Scholar]
- 58.Population estimates for the UK, England and Wales, Scotland and Northern Ireland: mid-2019. Office for National Statistics. 2020. [2023-05-15]. https://www.ons.gov.uk/peoplepopulationandcommunity/populationandmigration/populationestimates/bulletins/annualmidyearpopulationestimates/mid2019estimates .
- 59.Borghouts J, Eikey E, Mark G, De Leon C, Schueller SM, Schneider M, Stadnick N, Zheng K, Mukamel D, Sorkin DH. Barriers to and facilitators of user engagement with digital mental health interventions: systematic review. J Med Internet Res. 2021 Mar 24;23(3):e24387. doi: 10.2196/24387. https://www.jmir.org/2021/3/e24387/ v23i3e24387 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 60.Lambert M. Presidential address: what we have learned from a decade of research aimed at improving psychotherapy outcome in routine care. Psychother Res. 2007 Jan;17(1):1–14. doi: 10.1080/10503300601032506. https://www.tandfonline.com/doi/abs/10.1080/10503300601032506 . [DOI] [Google Scholar]
- 61.Han A, Kim TH. Effects of internet-delivered behavioral activation on individuals with depressive symptoms: a systematic review and meta-analysis. J Psychiatr Res. 2022 Aug;152:104–18. doi: 10.1016/j.jpsychires.2022.05.031. https://linkinghub.elsevier.com/retrieve/pii/S0022-3956(22)00285-0 .S0022-3956(22)00285-0 [DOI] [PubMed] [Google Scholar]
- 62.Huppert FA. Positive mental health in individuals and populations. In: Huppert FA, Baylis N, Keverne B, editors. The Science of Well-Being. Oxford, UK: Oxford University Press; 2005. pp. 306–40. [Google Scholar]
- 63.Stratton E, Jones N, Peters SE, Torous J, Glozier N. Digital mHealth interventions for employees: systematic review and meta-analysis of their effects on workplace outcomes. J Occup Environ Med. 2021 Aug 01;63(8):e512–25. doi: 10.1097/JOM.0000000000002267.00043764-900000000-97861 [DOI] [PubMed] [Google Scholar]
- 64.Burton WN, Pransky G, Conti DJ, Chen CY, Edington DW. The association of medical conditions and presenteeism. J Occup Environ Med. 2004 Jun;46(6 Suppl):S38–45. doi: 10.1097/01.jom.0000126687.49652.44.00043764-200406001-00005 [DOI] [PubMed] [Google Scholar]
- 65.Evans-Lacko S, Knapp M. Global patterns of workplace productivity for people with depression: absenteeism and presenteeism costs across eight diverse countries. Soc Psychiatry Psychiatr Epidemiol. 2016 Nov;51(11):1525–37. doi: 10.1007/s00127-016-1278-4. https://europepmc.org/abstract/MED/27667656 .10.1007/s00127-016-1278-4 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 66.Stewart WF, Ricci JA, Chee E, Hahn SR, Morganstein D. Cost of lost productive work time among US workers with depression. JAMA. 2003 Jun 18;289(23):3135–44. doi: 10.1001/jama.289.23.3135.289/23/3135 [DOI] [PubMed] [Google Scholar]
- 67.Henderson M, Harvey SB, Overland S, Mykletun A, Hotopf M. Work and common psychiatric disorders. J R Soc Med. 2011 May;104(5):198–207. doi: 10.1258/jrsm.2011.100231. https://europepmc.org/abstract/MED/21558098 .104/5/198 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 68.Edge D, Watkins ER, Limond J, Mugadza J. The efficacy of self-guided internet and mobile-based interventions for preventing anxiety and depression - a systematic review and meta-analysis. Behav Res Ther. 2023 May;164:104292. doi: 10.1016/j.brat.2023.104292. https://linkinghub.elsevier.com/retrieve/pii/S0005-7967(23)00041-4 .S0005-7967(23)00041-4 [DOI] [PubMed] [Google Scholar]
- 69.Nigatu YT, Huang J, Rao S, Gillis K, Merali Z, Wang J. Indicated prevention interventions in the workplace for depressive symptoms: a systematic review and meta-analysis. Am J Prev Med. 2019 Jan;56(1):e23–33. doi: 10.1016/j.amepre.2018.08.027.S0749-3797(18)32273-6 [DOI] [PubMed] [Google Scholar]
- 70.Karyotaki E, Efthimiou O, Miguel C, Bermpohl FM, Furukawa TA, Cuijpers P, Individual Patient Data Meta-Analyses for Depression (IPDMA-DE) Collaboration. Riper H, Patel V, Mira A, Gemmil AW, Yeung AS, Lange A, Williams AD, Mackinnon A, Geraedts A, van Straten A, Meyer B, Björkelund C, Knaevelsrud C, Beevers CG, Botella C, Strunk DR, Mohr DC, Ebert DD, Kessler D, Richards D, Littlewood E, Forsell E, Feng F, Wang F, Andersson G, Hadjistavropoulos H, Christensen H, Ezawa ID, Choi I, Rosso IM, Klein JP, Shumake J, Garcia-Campayo J, Milgrom J, Smith J, Montero-Marin J, Newby JM, Bretón-López J, Schneider J, Vernmark K, Bücker L, Sheeber LB, Warmerdam L, Farrer L, Heinrich M, Huibers MJ, Kivi M, Kraepelien M, Forand NR, Pugh N, Lindefors N, Lintvedt O, Zagorscak P, Carlbring P, Phillips R, Johansson R, Kessler RC, Brabyn S, Perini S, Rauch SL, Gilbody S, Moritz S, Berger T, Pop V, Kaldo V, Spek V, Forsell Y. Internet-based cognitive behavioral therapy for depression: a systematic review and individual patient data network meta-analysis. JAMA Psychiatry. 2021 Apr 01;78(4):361–71. doi: 10.1001/jamapsychiatry.2020.4364. https://europepmc.org/abstract/MED/33471111 .2774861 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 71.Cuijpers P, Karyotaki E, de Wit L, Ebert DD. The effects of fifteen evidence-supported therapies for adult depression: a meta-analytic review. Psychother Res. 2020 Mar;30(3):279–93. doi: 10.1080/10503307.2019.1649732. [DOI] [PubMed] [Google Scholar]
- 72.Flett JA, Fletcher BD, Riordan BC, Patterson T, Hayne H, Conner TS. The peril of self-reported adherence in digital interventions: a brief example. Internet Interv. 2019 Dec;18:100267. doi: 10.1016/j.invent.2019.100267. https://linkinghub.elsevier.com/retrieve/pii/S2214-7829(19)30039-9 .S2214-7829(19)30039-9 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 73.Stoyanov SR, Hides L, Kavanagh DJ, Wilson H. Development and validation of the user version of the mobile application rating scale (uMARS) JMIR Mhealth Uhealth. 2016 Jun 10;4(2):e72. doi: 10.2196/mhealth.5849. https://mhealth.jmir.org/2016/2/e72/ v4i2e72 [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Protocol deviations.
Baseline scores on the subscales of the Unmind Index measure of mental health and well-being.
Reported reasons for session and activity noncompletion, obtained at t1 (time point 1; week 3).
Plots of estimated marginal means obtained from the linear mixed effects models for the 7 subscales of the Unmind Index.
Contrasts and between-group (intervention vs control) effect size calculations from linear mixed effects models applied to each of the 7 Unmind Index subscales.
CONSORT-eHEALTH checklist (V 1.6.1).
Data Availability Statement
The data sets generated and analyzed during this study are available from the corresponding author on reasonable request.