

Abstract
Background
Adolescent alcohol and drug use (ADU) is a significant public health challenge. Uganda, one of the poorest countries in Sub-Saharan Africa (SSA), has the second-highest rate of per capita alcohol consumption in SSA, and over one-third of Ugandan adolescents have used alcohol in their lifetime (over 50% of them engage in heavy episodic drinking). These estimates further increase in fishing villages, a key HIV-vulnerable population, where ADU is normative. However, few studies have assessed ADU among adolescents and youths living with HIV despite their increased risk for ADU and its impact on engagement in HIV care. Moreover, data on risk and resilience factors for ADU are scarce as only few studies evaluating ADU interventions in SSA have reported positive outcomes. The majority have been implemented in school settings, potentially excluding adolescents in fishing communities with high school dropout rates, and none have targeted risk factors including poverty and mental health, which are rampant among adolescents and youths living with HIV and their families, undermine their coping skills and resources, and have been associated with increased risk for ADU among them.
Objective
We propose a mixed methods study with a sample of 200 adolescents and youths living with HIV (aged 18-24 years) seen at 6 HIV clinics in southwestern Uganda’s fishing communities to (1) examine the prevalence and consequences of ADU and identify the multilevel risk and resilience factors associated with ADU among them and (2) explore the feasibility and short-term effects of an economic empowerment intervention on ADU among them.
Methods
This study comprises four components: (1) focus group discussions (FGDs) with adolescents and youths living with HIV (n=20) and in-depth qualitative interviews with health providers (n=10) from 2 randomly selected clinics; (2) a cross-sectional survey with 200 adolescents and youths living with HIV; (3) a randomized controlled trial with a subgroup of adolescents and youths living with HIV (n=100); and (4) 2 postintervention FGD with adolescents and youths living with HIV (n=10 per group).
Results
Participant recruitment for the first qualitative phase has completed. As of May 4, 2023, ten health providers from 6 clinics have been recruited, provided written consent to participate, and participated in in-depth qualitative interviews. Two FGDs was conducted with 20 adolescents and youths living with HIV from 2 clinics. Data transcription, translation, and analysis of qualitative data has commenced. The cross-sectional survey will commence shortly after and dissemination of the main study findings is targeted for 2024.
Conclusions
Our findings will advance our understanding of ADU among adolescents and youths living with HIV and inform the design of future interventions to address ADU among them.
Trial Registration
ClinicalTrials.gov NCT05597865; https://clinicaltrials.gov/ct2/show/NCT05597865
International Registered Report Identifier (IRRID)
PRR1-10.2196/46486
Keywords: adolescents living with HIV, alcohol, Sub-Saharan Africa, substance use, Uganda
Introduction
Overview
Adolescent alcohol and drug use (ADU) is a growing public health concern globally, especially in low-resource settings such as Sub-Saharan Africa (SSA), where the epidemics of ADU and HIV/AIDS are co-occurring. ADU plays a significant role in the epidemiology of HIV among adolescents and young adults in SSA, who accounted for over 40% of new infections globally in 2019 [1]. ADU is associated with higher rates of HIV risk behaviors, such as condomless sex [2] and lower rates of HIV testing [3-5]. Among adolescents and youth living with HIV, ADU is a significant barrier to achieving positive HIV treatment outcomes, including enrollment and retention in HIV care [6], adherence to antiretroviral therapy (ART) [7-9], and viral suppression [8,10]. Among HIV-infected adults, it has been shown that alcohol and drug misuse increase AIDS mortality, even among virally suppressed and medication-adherent persons [11-13]. Uganda, one of the poorest countries in SSA, has high rates of HIV/AIDS (6.2%) [14] and alcohol use [15], and illicit drug use is on the increase [16]. Previous studies have reported high rates of alcohol consumption among adults living with HIV [17-19]. Fishing communities, a key vulnerable population in Uganda [20], have high levels of ADU, including among adolescents and youths [16,21-23], which lead to poor HIV prevention and care outcomes.
ADU onset typically occurs in adolescence as an experimental behavior that may escalate into problematic use and disorders [24,25]. Adolescence is a period characterized by the exploration of new roles, identities, and behaviors, including experimentation with ADU [26]. A multitude of factors influence ADU, and these include individual factors (eg, sensation seeking, impulsivity, and mental health) [27-32], interpersonal factors (eg, peer pressure, parental drug use, and poor parental monitoring) [33-43], and structural factors (eg, availability of alcohol and drugs, exposure to ADU marketing, community drug use attitudes, laws and policies, and structural barriers that contribute to poverty) [33,38]. Adolescents and youths living with HIV also experiment with ADU, which may escalate into problematic ADU.
Adolescents and youths living with HIV face numerous HIV-related psychosocial challenges, including HIV stigma, bereavement, chronic pain, relationship stress, and poverty, which heighten their risk for ADU [44-46]. Indeed, research reports indicate a higher burden of mental health problems among adolescents and youths living with HIV [45,47-50], which may lead to ADU. The co-occurrence of mental health problems and ADU is common, including among adolescents and youths living with HIV [49,51-57]. Both ADU and mental health difficulties are associated with nonadherence to ART [48,58-60] and risky sexual behaviors among adolescents and youths living with HIV [59,61-63], which could lead to secondary transmission of HIV and ART resistance due to nonadherence [64-66]. Poor mental health and poverty, which are rampant in poor countries, are significant risk factors for ADU. Poor mental health [54,67,68] and poverty [69-71] are rampant among HIV-affected households, and both are significant risk factors for acquiring HIV [72] and for poor HIV treatment outcomes [73,74]. Adolescents and youths living with HIV living in poverty-stricken households face greater challenges in accessing and sustaining HIV treatment due to economic factors, such as lack of money preventing access to transportation to clinics [75,76] and insufficient resources to afford food leading to inadequate meals to support medication adherence [77-79], which could lead to psychological distress and consequently, ADU [80]. Poverty adversely affects the quality of family relationships, including parent-child communication, involvement [81-83], and parenting skills [84,85], which increases susceptibility to emotional and behavioral challenges and increases risk for ADU [41,43,82,86-90].
Several studies have examined the risk and resilience factors for ADU [91] but few interventions targeting ADU have been tested in SSA. Efforts to prevent ADU are rooted predominantly in the substance use risk reduction and protection enhancement model [91] and require understanding of the risk and resilience factors for ADU. These interventions largely target individual and interpersonal risk factors for ADU, with a focus on providing participants with information on ADU and its consequences or building life skills. In SSA, only 1 intervention targeted the family [92], an important developmental context for adolescents, with a focus on enhancing parenting skills. Yet, none of these interventions has targeted risk factors, such as poverty and mental health, that are widespread in SSA and may undermine the resources and coping skills of adolescents and youths living with HIV.
Despite our knowledge of the higher risk for ADU among adolescents and youths living with HIV [93-96], there is lack of evidence-based interventions targeting ADU risk among adolescents and youths living with HIV. Only 10 ADU interventions have been evaluated in SSA [27,92,97-104] and only a few have been successful [27,98,99,101,103,104]. Most have been ineffective in preventing or reducing ADU, and none of these interventions have targeted adolescents and youths living with HIV. The majority of these interventions are largely school-based [27,100-104], which may exclude adolescents in fishing communities that have high rates of school dropout. These interventions also focused on individual and intrapersonal risk factors for ADU without paying attention to structural risk and resilience factors for ADU. The few existing studies on ADU among adolescents and youths living with HIV have been conducted in high-income countries. These studies focused on younger adolescents, yet ADU typically emerges and escalates in middle-to-late adolescence. Further, these studies rely on self-reports of ADU, which can be undermined by underreporting of ADU.
Economic empowerment (EE) interventions have the potential to prevent ADU among adolescents and youths living with HIV by reducing poverty and its associated mental impacts and bolster adolescents and youths living with HIV and their families’ resources to overcome the challenges associated with HIV. In our previous studies, we have used EE strategies to reduce poverty and improve mental health and HIV care outcomes (eg, medication adherence) among adolescents and youths living with HIV and other AIDS-affected adolescents in Uganda [73,82,105-108]. In this application, we propose to build on this growing evidence by examining the feasibility of using EE to address ADU among adolescents and youths living with HIV.
This study will investigate the epidemiology, underlying risk, and resilience factors for ADU among adolescents and youths living with HIV and evaluate the effects of an EE intervention on ADU among adolescents and youths living with HIV. The specific aims of the study are as follows.
Aim 1a: Examine the prevalence and consequences of ADU in a cohort of 200 adolescents and youths living with HIV (aged 18-24 years) seen at 6 HIV clinics in southwestern Uganda. We will use adolescent self-reports and biological measures of ADU (urine).
Aim 1b: Using a mixed methods approach, identify the multilevel (individual, interpersonal, community, and structural) factors associated with ADU among adolescents and youths living with HIV.
Aim 2: Using a subset of the sample, explore the feasibility and short-term effects of an EE intervention on ADU among adolescents and youths living with HIV.
Theoretical Framework
Our conceptual approach is informed by the socioecological model (SEM) [109], social causation and drift theories [110], and asset theory [111,112]. We have applied the SEM as a basis for investigating the contextually relevant risk and resilience factors for ADU. SEM posits that environmental factors fall into 4 broad domains: micro-, meso-, exo-, and macrosystems, and interactions within and between these domains determine behavior. This model has demonstrated effectiveness in identifying risk and resilience factors for prevention planning and intervention for ADU [113-117]. Social causation and social drift theories suggest that alcohol consumption problem may be both a response to and a driver of poverty [118]. Acute and chronic stress associated with living in a poverty-impacted environment increases the likelihood of ADU, which causes further material and economic deprivation, hence fueling the cycle of alcohol misuse, and contributing to downward social mobility. Our conceptual framework describes the hypothesized relationship among the intervention targets, poverty, poor mental health, and alcohol use. This has been adapted from Jones and Sumnall [119] (Figure 1). Research in Uganda has reported a higher burden of alcohol and drug abuse among poor populations [120], and many poverty-impacted Ugandan households engage in informal alcohol production for income-generating purposes [121]. Impoverished youths are burdened with hopelessness due to lack of opportunities for improvement in their economic well-being [122,123]. As a result, for impoverished adolescents and youths living with HIV, they may be inclined to spend on instant pleasures, such as alcohol and drugs, as a coping mechanism since they are less likely to believe they can afford the costs associated with accessing and maintaining long-term care for HIV. Our proposed EE intervention is based on Asset theory [124] and is intended to improve economic well-being, relieve poverty and its related consequences, such as poor mental health [106,125], and create a more hopeful and optimistic outlook for the future, thus reducing engagement in risk-taking behaviors like ADU by adolescents and youths living with HIV. The proposed EE will be one of the first studies to examine the impact of EE interventions on reducing ADU among adolescents and youths living with HIV in poverty-impacted communities.
Figure 1.

Conceptual model.
Methods
Overall Study Design
This mixed methods study comprises the following four components: (1) focus group discussions (FGDs) with adolescents and youths living with HIV (n=20) and in-depth qualitative interviews (QIs) with health providers (n=10) from 2 randomly selected clinics; (2) a cross-sectional survey (CS) with 200 adolescents and youths living with HIV; (3) a randomized controlled trial (RCT) with a subgroup of adolescents and youths living with HIV (n=100); and (4) 2 postintervention FGDs with adolescents and youths living with HIV (n=10 per study group). Figure 2 depicts the study components and expected number of participants in each component.
Figure 2.
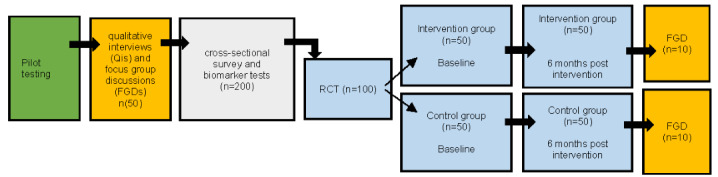
Study components and participant flow through the study. RCT: randomized controlled trial.
Study Sites and Participants
The study will be conducted in 6 randomly selected HIV clinics located in fishing districts within the Greater Masaka region of Southwestern Uganda—a region heavily affected by HIV (12% prevalence vs 6.2% national average) [126] with high rates of household poverty and alcohol use [127,128]. The target populations for this study are adolescents and youths living with HIV and health care providers at the selected HIV clinics. We will specifically target HIV clinics located in fishing districts with known HIV hot spots that are accredited by the Uganda Ministry of Health as a provider of ART and currently have established services for adolescents and youths living with HIV.
Inclusion Criteria
For the overall study, the inclusion criteria for adolescents and youths living with HIV are: (1) male or female adolescents and youths living with HIV aged 18-24 years; (2) medically diagnosed with HIV and aware of their HIV status; and (3) enrolled in care at one of the selected HIV clinics. Additionally, we will recruit 1-2 health care providers (psychosocial counselors, nurses, clinical officers, or doctors) from each of the selected clinics. For the RCT, a subsample of adolescents and youths living with HIV (n=100) with a positive self-report for ADU will be randomly selected and randomly assigned at the clinic level (3 clinics per group) to either the intervention group (n=50) or control group (n=50). A subsample of adolescents and youths living with HIV from both the control (n=10) and intervention groups (n=10) will be selected to participate in 2 FGDs at the end of the intervention. Overall, we will exclude any potential participant with significant cognitive impairments that interfere with their understanding of the informed consent process or who is unable or unwilling to consent. For the RCT and postintervention FGDs, we will exclude any adolescents and youths living with HIV with a negative self-report for ADU. However, given the minimum and maximum detection times for different drugs of abuse in the urine, we will not exclude those with a positive self-report but negative urine test results from being included in the RCT.
Participant Recruitment and Consent
Recruitment strategies will build on Reach the Youth Uganda (local implementing partner) and ICHAD’s (International Center for Child Health and Development) long-standing relationships (>15 years) with 39 health clinics in the greater Masaka region. We will capitalize on recruitment procedures tested in previous SUUBI (Luganda word for Hope) studies that involve collaborating with health clinics in the region (namely Suubi+Adherence: 1R01HD074949-01, Suubi+Adherence-R2: R01HD074949-07, and Suubi4Stigma: R21MH121141) [129-131]. All participants will be recruited from the selected HIV clinics. For the CS, 200 adolescents and youths living with HIV will be recruited from across 6 clinics located in the greater Masaka region. The designated study contact at each health clinic will present the project to all eligible adolescents and youths living with HIV aged 18-24 years during their clinic visits. If there is interest, they will provide verbal consent to be contacted by the research study team. The study coordinator will contact interested adolescents and youths living with HIV to inform them about the required extent of participation, the risks and benefits of participating, and to ask any questions. Written informed consent will be obtained from adolescents and youths living with HIV aged 18-24 years and from health care providers aged more than 18 years to participate. The written consent documents will emphasize the following elements: (1) participation in the study is voluntary; (2) responses to study questions are confidential; (3) participants can terminate their participation at any time, and their decision to withdraw from the study will not affect their access to services they are currently receiving in any way; and (4) participants may be contacted to participate in the RCT if eligible. A screening tool will be developed to assess whether participants meet the study inclusion criteria.
Ethics Approval
We have obtained approval for the study procedures from the institutional ethics and institutional review boards at the Washington University in St. Louis (202301145) on January 31, 2023 (with an amendment approved on March 2, 2023); the University of Michigan (HUM00223732) on February 23, 2023 and from the in-country local institutional review boards in Uganda: Uganda Virus Research Institute (GC/127/933) on January 16, 2023, and Uganda National Council of Science and Technology (HS2683ES) on March 2, 2023. The study has been registered with ClinicalTrials.gov (NCT05597865) as of October 28, 2022. The dissemination of the main study findings is targeted for 2024. Participants’ data will be protected by a certificate of confidentiality, which protects the privacy of research subjects by prohibiting the disclosure of identifiable, sensitive research information to individuals not involved in the research unless the participant consents.
Data Collection and Assessments
After pilot testing of data collection interview tools, 2 separate FGDs will be conducted with adolescents and youths living with HIV (n=20) and in-depth QIs will be conducted with health providers (n=10). Adolescents and youths living with HIV will be recruited from 2 randomly selected clinics, with 10 participants per FGD. The FGDs and QIs will explore participants’ perceptions of the multilevel risk and resilience factors associated with ADU and recommendations for culturally appropriate ADU interventions for adolescents and youths living with HIV. Data from the qualitative phase will inform assessments to be conducted in the CS. For the CS, 200 adolescents and youths living with HIV will complete an interviewer-administered survey comprising questions assessing their alcohol and drug consumption patterns and frequency, as well as exposure to multilevel (individual, interpersonal, community, and societal) factors that may be associated with risky and hazardous drinking and drug use among adolescents and youths living with HIV. To reduce social desirability bias, questions on ADU will be self-administered using audio computer–assisted interviewing. We refer to the social ecological framework [132] to guide data collection on the multiple levels of influence that are associated with harmful alcohol and drug use among adolescents and youths living with HIV (see Table 1 for socioecological framework and additional measures that will be collected at each time point). Questions assessing the presence of common mental disorders and other physical health conditions will be included.
Table 1.
List of measures and time points collected during the study.
| Category | Measure | Time point |
| Individual level of socioecological framework | Sociodemographic: gender, age, orphanhood status, education, income and unemployment, food insecurity [133], experienced homelessness, refugee, day and boarding school, and urban and rural residence. Mental health: depression [134], hopelessness [135], optimism [136], stress [137], pain [138], and history of substance abuse [139]. | Cross-sectional survey, qualitative interview, focus group discussion, randomized controlled trial |
| Interpersonal and relationship levels of socioecological framework |
Loneliness [140], number of close friends, bullying, interpersonal violence [141,142], social support [143], family cohesion [144,145], childhood abuse and trauma [146], family history of substance abuse [139], and sexual risk-taking [147] | Cross-sectional survey, qualitative interview, focus group discussion, randomized controlled trial |
| Community level of socioecological framework | Community norms and access to alcohol and illegal drugs | Cross-sectional survey, qualitative interview, focus group discussion, randomized controlled trial |
| Society level of socioecological framework | Educational campaigns, price and supply of alcohol, and social stigma [148] | Cross-sectional survey, qualitative interview, focus group discussion, randomized controlled trial |
| Biomarkers | Urine alcohol and drug tests | Cross-sectional survey, randomized controlled trial |
| Savings deposits | Savings | Randomized controlled trial |
| Assessments | Self-reported alcohol and drug use [139], viral load from clinic records, self-reported adherence [149], depressive symptoms [134], hopelessness [135], physical health conditions, and sexual risk-taking [147] | Randomized controlled trial |
Urine tests for ADU will be conducted for all 200 adolescents and youths living with HIV who participate in the CS and for the 100 who participate in the RCT (at the 2 time points: baseline and postintervention). A trained research assistant will collect and test a urine specimen from each participant. The urine sample will be tested for up to 16 classes of the most commonly abused illicit drugs using the T-Cup 16 panel Compact Instant Drug Test Cup at the study site. The T-Cup can detect alcohol in the urine from as early as 8 hours to up to 80 hours after consumption. Minimum and maximum detection times for illicit drugs of abuse range from 1 hour to 40 days, depending on the drug.
Randomized Controlled Trial: Intervention Conditions
For the RCT, 100 adolescents and youths living with HIV with a positive self-report or urine ADU test (based on data from the CS) will be randomly recruited from the 6 clinics and randomly assigned at the clinic level (3 clinics per group) to either the control (n=50) or intervention (n=50) group. The intervention will be delivered over a period of 6 months, with assessments at baseline and 6 months (end of intervention). Upon completion of the RCT, adolescents and youths living with HIV will be randomly selected to participate in 2 FGDs (n=10 from control group and n=10 from intervention group). Adolescents and youths living with HIV in the intervention group will share how the intervention affected their alcohol and drug use as well as their recommendations on how to improve the intervention to be more culturally appropriate and effective in reducing ADU among adolescents and youths living with HIV in Uganda, while adolescents and youths living with HIV in the control group will share their experiences with ADU risk reduction sessions and how this influenced their ADU.
Description of the Control Condition
Adolescents and youths living with HIV in the control condition will receive 4 ADU risk reduction sessions tailored for adolescents and youths living with HIV. Working with author JM (consultant), we plan to adapt, expand, and tailor the Program for Appropriate Technology in Health (PATH) Life Planning Skills curriculum (Unit 11 on substance use) [150] to include issues specific to adolescents and youths living with HIV. We will train research assistants, using an adapted facilitator’s manual, to deliver the adapted curriculum. As part of the RCT, adolescents and youths living with HIV will complete a questionnaire (at baseline and at the end of the intervention) on their alcohol and drug use behaviors (self-reported and biologically measured) and risk and resilience behaviors.
Description of the Intervention Group
In addition to the adapted ADU training module that the control group will receive, adolescents and youths living with HIV in the intervention arm will receive 4 financial literacy training sessions and a youth development savings account (YDA) for long-term savings. Although akin to conditional cash transfer interventions, which have become increasingly popular in the social development field by enabling individuals to meet basic needs while incentivizing prosocial behaviors [82,107,151-153], EE interventions that apply matched savings accounts go beyond incentivizing behavior. They emphasize long-term investment and promote lifelong financial inclusion by forming savings habits and establishing partnerships between the participants and local financial institutions and the actual intervention program. For the proposed study, the EE intervention will be in the form of a YDA, where savings are housed at a local bank and deposits made by the adolescent are matched by the intervention to encourage savings. YDAs yield positive effects, including creating a greater sense of security, self-confidence, and future orientation for young people [82,107,151-153]. Each adolescent and youth living with HIV in the EE intervention will receive a YDA held in their own name in a bank registered by the Central Bank (Bank of Uganda). We will form partnerships with national banks operating in the study area. The account will then be matched with money from the program. The maximum adolescent’s contribution to be matched by the program will be an equivalent of US $20 per month per adolescent or US $120 for the 6-month intervention period. Our previous studies indicate that the partner financial institutions have multiple and easily accessible deposit locations in the study area and that participants can save these amounts [82,107,151-153]. Therefore, adolescents and youths living with HIV who save the maximum amount will have a total of US $240 at the end of the intervention (US $120 in savings and US $120 from the match: a 1:1 match).
As in the studies that inform this application, each month a bank account statement will be generated for every adolescent and youth living with HIV to note their accumulated savings. The statements are intended to act as “moral boosters” for the enrolled adolescents and youths living with HIV. Unique to this study is our innovative spending model, which empowers participants to make informed financial decisions. During the intervention period, adolescents and youths living with HIV will have direct access to both their personal savings deposited in the accounts as well as the match provided by the study. This is different from our previous studies that required the participants’ own savings and the match to be maintained in separate accounts and to get approval by the research team to access the match [82,107,151-153]. This added unconditional component provides adolescents and youths living with HIV with a safety net to address short-term medical needs and financial and consumption emergencies if they arise. Participants will be provided with financial literacy sessions and mentorship tailored specifically to the needs of adolescents and youths living with HIV and ADU. We expect adolescents and youths living with HIV to be equipped with the knowledge to make well-informed consumption and expenditure decisions but also to feel supported in case of immediate medical needs. The research team will monitor, but not restrict, how participants spend their money. Additionally, the study team will have access to and review participants’ bank statements to ascertain deposit and withdrawal frequency. Participants will be encouraged to use financial diaries to record their expenditures.
Analysis of CS Data
Frequency distributions and summary statistics for the outcome and all predictor variables will be derived. The prevalence of ADU from both biological tests and self-reports, assessed using the Smoking and Substance Involvement Screening Test (NIDA-Modified ASSIST) [139] among adolescents and youths living with HIV, will be calculated by dividing the number who tested positive for ADU by the total number of participants tested and dividing the number screened to be of moderate or high risk in self-reported data by the total number of participants who completed the survey. To determine which multilevel factors are associated with substance misuse, we will fit logistic regression models comprising the outcome (ADU) and potential risk factors with standard errors adjusted for clustering by clinics.
Analysis of RCT Data
Primary Outcome Measures
Our primary outcomes are feasibility and acceptability of the intervention. Feasibility will be determined by the proportion of participants who enrolled or refused to participate in the intervention. In addition, we will measure the willingness of local partners to assist with recruitment, reasons for refusal, enrollment, and ineligibility. Acceptability will be determined by measuring retention rates at 6 months, the proportion of participants that adhered to study procedures, intervention attendance and engagement, and the extent to which the intervention is acceptable and appealing to study participants.
Secondary Outcome Measures
Changes in ADU and mental health functioning are our secondary outcomes. Our primary hypothesis is that participants in the intervention group will have a lower odds of ADU compared to participants in the control group at the end of the intervention. Our secondary hypothesis is that adolescents and youths living with HIV in the intervention group will have better mental health outcomes, including lower levels of depressive symptoms, less hopelessness, improved adherence, better viral suppression, and improved economic outcomes than adolescents and youths living with HIV in the control group. To test these hypotheses, we will fit 3-level mixed-effects models. Each model will comprise the outcome and fixed categorical effects for study group (intervention vs control), time (baseline and 6-months), and a group-by-time interaction term. Random intercepts will be fitted at the clinic and person levels, with unstructured correlations among subjects’ repeated measures. Robust Huber-White standard errors and test statistics will be computed for each model. We will assess the omnibus effects of study group, time, and their interaction. Postestimation analyses will be conducted to assess time within group simple effects and group within time simple effects.
Qualitative Data Analysis
Interviews will be transcribed and uploaded to NVivo 12 (QSR International) [154]. Analytical induction techniques [155] will be used for coding. Ten interview transcripts will be randomly selected, read multiple times, and independently coded by the team using sensitizing concepts to identify emergent themes (open coding) [156]. Broader themes will be broken down into smaller, more specific units until no further subcategory is necessary. Analytic memos will be written to further develop categories, themes, and subthemes and to integrate the ideas that emerge from the data [156,157]. Codes and the inclusion and exclusion criteria for assigning codes will be discussed as a team to create the final codebook in NVivo 12. Each transcript will then be independently coded by 2 investigators using the codebook. Intercoder reliability will be established. A level of agreement ranging from 66% to 97% based on level of coding indicates good reliability [158]. Disagreements will be resolved through team discussions. The secondary analysis will compare and contrast themes and categories within and across groups to identify similarities, differences, and relationships among the findings. Member checking, peer debriefing, and an audit trail will be used to ensure rigor [159].
Results
Recruitment of participants for the first qualitative phase has commenced. As of May 4, 2023, ten health providers from 6 clinics have been recruited, provided written consent to participate, and participated in in-depth QIs. Two FGDs was conducted with 20 adolescents and youths living with HIV from 2 clinics. Data collection for the qualitative phase has completed and transcription, translation, and analysis of qualitative data will commence immediately thereafter. The CS will begin shortly after the qualitative phase. Data collection will continue over the next year, and dissemination of the main study findings is targeted for 2024.
Discussion
This will be one of the first studies to examine the impact of EE interventions on reducing alcohol and drug use among adolescents and youths living with HIV in poverty-impacted communities. This study will advance our understanding of the epidemiology, underlying risk factors, and consequences of ADU among adolescents and youths living with HIV in high-risk environments and evaluate a culturally tailored intervention that could prevent harmful ADU and improve the overall and long-term health and well-being of adolescents and youths living with HIV. We specifically target adolescents and youths living with HIV living in fishing communities—known HIV hot spots that typically have high levels of poverty as well as ADU. Study findings will contribute to our understanding of the epidemiology, risk and resilience factors, and consequences of ADU among adolescents and youths living with HIV in order to inform the development of effective ADU prevention interventions. We envision that the findings will also inform the design of longitudinal studies to evaluate the long-term effects of an EE intervention on ADU among adolescents and youths living with HIV.
There is a scarcity of evidence-based interventions for addressing ADU among youth in resource-limited settings. Only a few ADU interventions evaluated in SSA have targeted the family context [92]. No study has targeted poverty and its attendant impacts (eg, mental health) as a risk factor for ADU. In this proposal, we will examine the feasibility, acceptability, and short-term effects of an EE intervention to reduce and prevent risky and hazardous alcohol and drug use. Our intervention targets the most commonly occurring risk factors for ADU (ie, poverty and mental health problems). This will be one of the first studies to examine the impact of EE interventions on reducing alcohol and drug use among adolescents and youths living with HIV in poverty-impacted communities. The proposed EE intervention is based on Asset theory [124] and is intended to improve economic well-being, create a more hopeful and optimistic outlook for the future, and thus reduce engagement in risk-taking behaviors by adolescents and youths living with HIV, including ADU. However, our findings should be interpreted with some limitations. Given our target population, our findings may not be generalizable to adolescents and youths living with HIV populations in more urban or developed areas, and to younger or older age groups. This is a small feasibility study, so our study is not powered to detect significant changes but will provide preliminary data for a larger-scale study with sufficient power.
Acknowledgments
We would like to thank our staff and volunteers at the International Center for Child Health and Development (ICHAD) Uganda and Reach the Youth Uganda for their respective contributions to study preparation. In addition, we are grateful to the participating health care clinics and participating youth for agreeing to participate in the study. The study outlined in this protocol is supported by the National Institute on Alcohol Abuse and Alcoholism (NIAAA) under award number 1R21AA030225-01 (multiple principal investigators: MM, PhD and RB, PhD). NIAAA has no role in the study design, data collection, analysis, interpretation of findings, and manuscript preparation. The content is solely the responsibility of the authors and does not necessarily represent the official views of NIAAA or the National Institutes of Health.
Abbreviations
- ADU
alcohol and drug use
- ART
antiretroviral therapy
- CS
cross-sectional survey
- EE
economic empowerment
- FGD
focus group discussion
- ICHAD
International Center for Child Health and Development
- PATH
Program for Appropriate Technology in Health
- QI
qualitative interviews
- RCT
randomized controlled trial
- SEM
socioecological model
- SSA
Sub-Saharan Africa
- YDA
youth development savings account
Summary statement for grant reviewed by Center for Scientific Review Special Emphasis Panel Member Conflict: HIV/AIDS Related Behavioral Research.
Data Availability
Data sharing is not applicable to this study as no data sets were generated or analyzed during this study. However, the data sets generated during this study will be available in the National Institute of Mental Health Data Archive.
Footnotes
Conflicts of Interest: None declared.
References
- 1.Adolescent HIV Prevention: HIV in adolescents. United Nations International Children's Emergency Fund. 2020. [2021-06-22]. https://data.unicef.org/topic/hivaids/adolescents-young-people/
- 2.Choudhry V, Agardh A, Stafström Martin, Östergren Per-Olof. Patterns of alcohol consumption and risky sexual behavior: a cross-sectional study among Ugandan university students. BMC Public Health. 2014 Feb 06;14:128. doi: 10.1186/1471-2458-14-128. https://bmcpublichealth.biomedcentral.com/articles/10.1186/1471-2458-14-128 .1471-2458-14-128 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Walter AW, Lundgren L, Umez-Eronini A, Ritter GA. Alcohol Use and HIV Testing in a National Sample of Women. AIDS Behav. 2016 Jan;20 Suppl 1(0 1):S84–96. doi: 10.1007/s10461-015-1144-5. https://europepmc.org/abstract/MED/26238036 .10.1007/s10461-015-1144-5 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Bengtson AM, L'Engle K, Mwarogo P, King'ola N. Levels of alcohol use and history of HIV testing among female sex workers in Mombasa, Kenya. AIDS Care. 2014;26(12):1619–24. doi: 10.1080/09540121.2014.938013. https://europepmc.org/abstract/MED/25040114 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Fatch R, Bellows B, Bagenda F, Mulogo E, Weiser S, Hahn JA. Alcohol consumption as a barrier to prior HIV testing in a population-based study in rural Uganda. AIDS Behav. 2013 Jun;17(5):1713–23. doi: 10.1007/s10461-012-0282-2. https://europepmc.org/abstract/MED/22878790 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Enane LA, Davies MA, Leroy V, Edmonds A, Apondi E, Adedimeji A, Vreeman RC. Traversing the cascade: urgent research priorities for implementing the 'treat all' strategy for children and adolescents living with HIV in sub-Saharan Africa. J Virus Erad. 2018 Nov 15;4(Suppl 2):40–46. doi: 10.1016/S2055-6640(20)30344-7. https://europepmc.org/abstract/MED/30515313 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Denison JA, Packer C, Stalter RM, Banda H, Mercer S, Nyambe N, Katayamoyo P, Mwansa JK, McCarraher DR. Factors Related to Incomplete Adherence to Antiretroviral Therapy among Adolescents Attending Three HIV Clinics in the Copperbelt, Zambia. AIDS Behav. 2018 Mar;22(3):996–1005. doi: 10.1007/s10461-017-1944-x.10.1007/s10461-017-1944-x [DOI] [PubMed] [Google Scholar]
- 8.Kim MH, Mazenga AC, Yu X, Ahmed S, Paul ME, Kazembe PN, Abrams EJ. High self-reported non-adherence to antiretroviral therapy amongst adolescents living with HIV in Malawi: barriers and associated factors. J Int AIDS Soc. 2017 Mar 30;20(1):21437. doi: 10.7448/IAS.20.1.21437. https://europepmc.org/abstract/MED/28406275 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Kalichman S, Mathews C, Banas E, Kalichman M. Alcohol-related intentional nonadherence to antiretroviral therapy among people living with HIV, Cape Town, South Africa. AIDS Care. 2019 Aug;31(8):951–957. doi: 10.1080/09540121.2019.1587357. https://europepmc.org/abstract/MED/30884956 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Haas AD, Technau KG, Pahad S, Braithwaite K, Madzivhandila M, Sorour G, Sawry S, Maxwell N, von Groote P, Tlali M, Davies MA, Egger M, IeDEA Southern Africa Collaboration Mental health, substance use and viral suppression in adolescents receiving ART at a paediatric HIV clinic in South Africa. J Int AIDS Soc. 2020 Dec;23(12):e25644. doi: 10.1002/jia2.25644. https://boris.unibe.ch/id/eprint/149988 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Petoumenos K, Law MG. Smoking, alcohol and illicit drug use effects on survival in HIV-positive persons. Curr Opin HIV AIDS. 2016 Sep;11(5):514–520. doi: 10.1097/COH.0000000000000306. [DOI] [PubMed] [Google Scholar]
- 12.Probst C, Parry CDH, Rehm J. HIV/AIDS mortality attributable to alcohol use in South Africa: a comparative risk assessment by socioeconomic status. BMJ Open. 2018 Feb 21;8(2):e017955. doi: 10.1136/bmjopen-2017-017955. https://bmjopen.bmj.com/lookup/pmidlookup?view=long&pmid=29467131 .bmjopen-2017-017955 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Cohn SE, Jiang H, McCutchan JA, Koletar SL, Murphy RL, Robertson KR, de St Maurice AM, Currier JS, Williams PL. Association of ongoing drug and alcohol use with non-adherence to antiretroviral therapy and higher risk of AIDS and death: results from ACTG 362. AIDS Care. 2011 Jun;23(6):775–85. doi: 10.1080/09540121.2010.525617. https://europepmc.org/abstract/MED/21293986 .933017317 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Uganda population-based HIV impact assessment: UPHIA 2016-2017. World Health Organization African Region. 2018. [2023-05-22]. https://www.afro.who.int/sites/default/files/2017-08/UPHIA%20Uganda%20factsheet.pdf .
- 15.Total alcohol consumption per capita (liters of pure alcohol, projected estimates, 15+ years of age) World Health Organization and Global Health Observatory Data. [2023-05-22]. https://data.worldbank.org/indicator/SH.ALC.PCAP.LI .
- 16.Kuteesa MO, Weiss HA, Cook S, Seeley J, Ssentongo JN, Kizindo R, Ngonzi P, Sewankambo M, Webb EL. Epidemiology of Alcohol Misuse and Illicit Drug Use Among Young People Aged 15-24 Years in Fishing Communities in Uganda. Int J Environ Res Public Health. 2020 Apr 01;17(7):2401. doi: 10.3390/ijerph17072401. https://www.mdpi.com/resolver?pii=ijerph17072401 .ijerph17072401 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Hahn JA, Fatch R, Kabami J, Mayanja B, Emenyonu NI, Martin J, Bangsberg DR. Self-Report of Alcohol Use Increases When Specimens for Alcohol Biomarkers Are Collected in Persons With HIV in Uganda. J Acquir Immune Defic Syndr. 2012 Dec 01;61(4):e63–4. doi: 10.1097/QAI.0b013e318267c0f1. https://europepmc.org/abstract/MED/23138732 .00126334-201212010-00020 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Hahn JA, Emenyonu NI, Fatch R, Muyindike WR, Kekiibina A, Carrico AW, Woolf-King S, Shiboski S. Declining and rebounding unhealthy alcohol consumption during the first year of HIV care in rural Uganda, using phosphatidylethanol to augment self-report. Addiction. 2016 Feb;111(2):272–9. doi: 10.1111/add.13173. https://europepmc.org/abstract/MED/26381193 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Wandera B, Tumwesigye NM, Nankabirwa JI, Kambugu AD, Parkes-Ratanshi R, Mafigiri DK, Kapiga S, Sethi AK. Alcohol Consumption among HIV-Infected Persons in a Large Urban HIV Clinic in Kampala Uganda: A Constellation of Harmful Behaviors. PLoS One. 2015;10(5):e0126236. doi: 10.1371/journal.pone.0126236. https://dx.plos.org/10.1371/journal.pone.0126236 .PONE-D-14-42114 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Uganda Population-based HIV Impact Assessment (UPHIA) 2016-2017: Final Report. Ministry of Health Uganda. 2019. [2023-05-22]. https://phia.icap.columbia.edu/uganda-phia-final-report/
- 21.Kapesa A, Basinda N, Nyanza EC, Mushi MF, Jahanpour O, Ngallaba SE. Prevalence of HIV infection and uptake of HIV/AIDS services among fisherfolk in landing Islands of Lake Victoria, north western Tanzania. BMC Health Serv Res. 2018 Dec 18;18(1):980. doi: 10.1186/s12913-018-3784-4. https://bmchealthservres.biomedcentral.com/articles/10.1186/s12913-018-3784-4 .10.1186/s12913-018-3784-4 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Smolak A. A meta-analysis and systematic review of HIV risk behavior among fishermen. AIDS Care. 2014;26(3):282–91. doi: 10.1080/09540121.2013.824541. [DOI] [PubMed] [Google Scholar]
- 23.Kissling E, Allison EH, Seeley JA, Russell S, Bachmann M, Musgrave SD, Heck S. Fisherfolk are among groups most at risk of HIV: cross-country analysis of prevalence and numbers infected. AIDS. 2005 Nov 18;19(17):1939–46. doi: 10.1097/01.aids.0000191925.54679.94.00002030-200511180-00001 [DOI] [PubMed] [Google Scholar]
- 24.Burke KC, Burke JD, Rae DS, Regier DA. Comparing age at onset of major depression and other psychiatric disorders by birth cohorts in five US community populations. Arch Gen Psychiatry. 1991 Sep;48(9):789–95. doi: 10.1001/archpsyc.1991.01810330013002. [DOI] [PubMed] [Google Scholar]
- 25.Kessler RC, Angermeyer M, Anthony JC, Graaf Ron D E, Demyttenaere K, Gasquet I, DE Girolamo Giovanni, Gluzman S, Gureje O, Haro JM, Kawakami N, Karam A, Levinson D, Medina Mora Maria Elena, Oakley Browne Mark A, Posada-Villa J, Stein DJ, Adley Tsang Cheuk Him, Aguilar-Gaxiola S, Alonso J, Lee S, Heeringa S, Pennell BE, Berglund P, Gruber MJ, Petukhova M, Chatterji S, Ustün T Bedirhan. Lifetime prevalence and age-of-onset distributions of mental disorders in the World Health Organization's World Mental Health Survey Initiative. World Psychiatry. 2007 Oct;6(3):168–76. https://europepmc.org/abstract/MED/18188442 . [PMC free article] [PubMed] [Google Scholar]
- 26.Kessler RC, Amminger GP, Aguilar-Gaxiola S, Alonso J, Lee S, Ustün T Bedirhan. Age of onset of mental disorders: a review of recent literature. Curr Opin Psychiatry. 2007 Jul;20(4):359–64. doi: 10.1097/YCO.0b013e32816ebc8c. https://europepmc.org/abstract/MED/17551351 .00001504-200707000-00010 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Cupp PK, Zimmerman RS, Bhana A, Feist-Price S, Dekhtyar O, Karnell A, Ramsoomar L. Combining and adapting American school-based alcohol and HIV prevention programmes in South Africa: the HAPS project. Vulnerable Child Youth Stud. 2008;3(2):134–142. doi: 10.1080/17450120701867553. [DOI] [Google Scholar]
- 28.Francis JM, Myers B, Nkosi S, Petersen Williams Petal, Carney T, Lombard C, Nel E, Morojele N. The prevalence of religiosity and association between religiosity and alcohol use, other drug use, and risky sexual behaviours among grade 8-10 learners in Western Cape, South Africa. PLoS One. 2019;14(2):e0211322. doi: 10.1371/journal.pone.0211322. https://dx.plos.org/10.1371/journal.pone.0211322 .PONE-D-18-10941 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.McGill E, Petticrew M, Marks D, McGrath M, Rinaldi C, Egan M. Applying a complex systems perspective to alcohol consumption and the prevention of alcohol-related harms in the 21st century: a scoping review. Addiction. 2021 Sep;116(9):2260–2288. doi: 10.1111/add.15341. [DOI] [PubMed] [Google Scholar]
- 30.Nyundo A, Manu A, Regan M, Ismail A, Chukwu A, Dessie Y, Njau T, Kaaya SF, Smith Fawzi Mary C. Factors associated with depressive symptoms and suicidal ideation and behaviours amongst sub-Saharan African adolescents aged 10-19 years: cross-sectional study. Trop Med Int Health. 2020 Jan;25(1):54–69. doi: 10.1111/tmi.13336. https://onlinelibrary.wiley.com/doi/10.1111/tmi.13336 . [DOI] [PubMed] [Google Scholar]
- 31.Schulenberg JE, Maggs JL. A developmental perspective on alcohol use and heavy drinking during adolescence and the transition to young adulthood. J Stud Alcohol Suppl. 2002 Mar;(14):54–70. doi: 10.15288/jsas.2002.s14.54. [DOI] [PubMed] [Google Scholar]
- 32.Wallace JM, Yamaguchi R, Bachman JG, O'Malley PM, Schulenberg JE, Johnston LD. Religiosity and Adolescent Substance Use: The Role of Individual and Contextual Influences. Social Problems. 2007 May;54(2):308–327. doi: 10.1525/sp.2007.54.2.308. [DOI] [Google Scholar]
- 33.Brooks-Russell A, Simons-Morton B, Haynie D, Farhat T, Wang J. Longitudinal relationship between drinking with peers, descriptive norms, and adolescent alcohol use. Prev Sci. 2014 Aug;15(4):497–505. doi: 10.1007/s11121-013-0391-9. https://europepmc.org/abstract/MED/23564529 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Bouchard M, Gallupe O, Dawson K, Anamali M. No place like home? Availability, opportunity, and substance use in adolescence. Journal of Youth Studies. 2017 Dec 27;21(6):747–764. doi: 10.1080/13676261.2017.1420760. [DOI] [Google Scholar]
- 35.Ghuman S, Meyer-Weitz A, Knight S. Prevalence patterns and predictors of alcohol use and abuse among secondary school students in southern KwaZulu-Natal, South Africa: demographic factors and the influence of parents and peers. South African Family Practice. 2014 Aug 15;54(2):132–138. doi: 10.1080/20786204.2012.10874192. [DOI] [Google Scholar]
- 36.Leung RK, Toumbourou JW, Hemphill SA. The effect of peer influence and selection processes on adolescent alcohol use: a systematic review of longitudinal studies. Health Psychol Rev. 2014;8(4):426–57. doi: 10.1080/17437199.2011.587961. [DOI] [PubMed] [Google Scholar]
- 37.Manu E, Douglas M, Ntsaba MJ. Contextual influences of illicit adolescent marijuana cultivation and trading in the Inqguza Hill local municipality of South Africa: implications for public health policy. Subst Abuse Treat Prev Policy. 2021 Jan 07;16(1):6. doi: 10.1186/s13011-020-00338-7. https://substanceabusepolicy.biomedcentral.com/articles/10.1186/s13011-020-00338-7 .10.1186/s13011-020-00338-7 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Muchiri BW, Dos Santos MML. Family management risk and protective factors for adolescent substance use in South Africa. Subst Abuse Treat Prev Policy. 2018 Jun 19;13(1):24. doi: 10.1186/s13011-018-0163-4. https://substanceabusepolicy.biomedcentral.com/articles/10.1186/s13011-018-0163-4 .10.1186/s13011-018-0163-4 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Obadeji A, Kumolalo BF, Oluwole LO, Ajiboye AS, Dada MU, Ebeyi RC. Substance Use among Adolescent High School Students in Nigeria and Its Relationship with Psychosocial Factors. J Res Health Sci. 2020 Jun 06;20(2):e00480. doi: 10.34172/jrhs.2020.15. https://europepmc.org/abstract/MED/32814700 .5386 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Ogunsola OO, Fatusi AO. Risk and protective factors for adolescent substance use: a comparative study of secondary school students in rural and urban areas of Osun State, Nigeria. Int J Adolesc Med Health. 2016 Jan 29;29(3):20150096. doi: 10.1515/ijamh-2015-0096./j/ijamh.2017.29.issue-3/ijamh-2015-0096/ijamh-2015-0096.xml [DOI] [PubMed] [Google Scholar]
- 41.Ryan SM, Jorm AF, Lubman DI. Parenting factors associated with reduced adolescent alcohol use: a systematic review of longitudinal studies. Aust N Z J Psychiatry. 2010 Sep;44(9):774–83. doi: 10.1080/00048674.2010.501759. [DOI] [PubMed] [Google Scholar]
- 42.Tyler KA, Handema R, Schmitz RM, Phiri F, Kuyper KS, Wood C. Multi-Level Risk and Protective Factors for Substance Use Among Zambian Street Youth. Subst Use Misuse. 2016 Jun 06;51(7):922–31. doi: 10.3109/10826084.2016.1156702. https://europepmc.org/abstract/MED/27144671 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Yap MBH, Cheong TWK, Zaravinos-Tsakos F, Lubman DI, Jorm AF. Modifiable parenting factors associated with adolescent alcohol misuse: a systematic review and meta-analysis of longitudinal studies. Addiction. 2017 Jul;112(7):1142–1162. doi: 10.1111/add.13785. [DOI] [PubMed] [Google Scholar]
- 44.Kang E, Mellins CA, Dolezal C, Elkington KS, Abrams EJ. DISADVANTAGED NEIGHBORHOOD INFLUENCES ON DEPRESSION AND ANXIETY IN YOUTH WITH PERINATALLY ACQUIRED HUMAN IMMUNODEFICIENCY VIRUS: HOW LIFE STRESSORS MATTER. J Community Psychol. 2011 Nov 01;39(8):956–971. doi: 10.1002/jcop.20483. https://europepmc.org/abstract/MED/23472046 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.Mellins CA, Malee KM. Understanding the mental health of youth living with perinatal HIV infection: lessons learned and current challenges. J Int AIDS Soc. 2013 Jun 18;16(1):18593. doi: 10.7448/IAS.16.1.18593. https://europepmc.org/abstract/MED/23782478 .18593 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46.Mutumba M, Bauermeister JA, Musiime V, Byaruhanga J, Francis K, Snow RC, Tsai AC. Psychosocial challenges and strategies for coping with HIV among adolescents in Uganda: a qualitative study. AIDS Patient Care STDS. 2015 Feb;29(2):86–94. doi: 10.1089/apc.2014.0222. http://hdl.handle.net/2027.42/140199 . [DOI] [PubMed] [Google Scholar]
- 47.Scharko AM. DSM psychiatric disorders in the context of pediatric HIV/AIDS. AIDS Care. 2006 Jul;18(5):441–5. doi: 10.1080/09540120500213487.N038575824805227 [DOI] [PubMed] [Google Scholar]
- 48.Brown LK, Whiteley L, Harper GW, Nichols S, Nieves A, ATN 086 Protocol Team for The Adolescent Medicine Trials Network for HIV/AIDS Interventions Psychological symptoms among 2032 youth living with HIV: a multisite study. AIDS Patient Care STDS. 2015 Apr;29(4):212–9. doi: 10.1089/apc.2014.0113. http://hdl.handle.net/2027.42/140176 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49.Malee KM, Tassiopoulos K, Huo Y, Siberry G, Williams PL, Hazra R, Smith RA, Allison SM, Garvie PA, Kammerer B, Kapetanovic S, Nichols S, Van Dyke R, Seage GR, Mellins CA, Pediatric HIV/AIDS Cohort Study Team Mental health functioning among children and adolescents with perinatal HIV infection and perinatal HIV exposure. AIDS Care. 2011 Dec;23(12):1533–44. doi: 10.1080/09540121.2011.575120. https://europepmc.org/abstract/MED/21702707 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 50.Louthrenoo O, Oberdorfer P, Sirisanthana V. Psychosocial functioning in adolescents with perinatal HIV infection receiving highly active antiretroviral therapy. J Int Assoc Provid AIDS Care. 2014;13(2):178–83. doi: 10.1177/2325957413488171. https://journals.sagepub.com/doi/10.1177/2325957413488171?url_ver=Z39.88-2003&rfr_id=ori:rid:crossref.org&rfr_dat=cr_pub0pubmed .2325957413488171 [DOI] [PubMed] [Google Scholar]
- 51.Kessler RC, Aguilar-Gaxiola S, Andrade L, Bijl RV, Borges G, Caraveo-Anduaga JJ, DeWit DJ, Kolody B, Merikangas KR, Molnar BE, Vega WA, Walters EE, Wittchen HU, Ustun TB. Mental-substance comorbidities in the ICPE surveys. Psychiatr Fennica. 2001;32(Suppl 2):62–79. [Google Scholar]
- 52.Elkington KS, Bauermeister JA, Zimmerman MA. Psychological distress, substance use, and HIV/STI risk behaviors among youth. J Youth Adolesc. 2010 May;39(5):514–27. doi: 10.1007/s10964-010-9524-7. https://europepmc.org/abstract/MED/20229264 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 53.Williams PL, Leister E, Chernoff M, Nachman S, Morse E, Di Poalo V, Gadow KD. Substance use and its association with psychiatric symptoms in perinatally HIV-infected and HIV-affected adolescents. AIDS Behav. 2010 Oct;14(5):1072–82. doi: 10.1007/s10461-010-9782-0. https://europepmc.org/abstract/MED/20725774 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 54.Dessauvagie AS, Jörns-Presentati A, Napp AK, Stein DJ, Jonker D, Breet E, Charles W, Swart RL, Lahti M, Suliman S, Jansen R, van den Heuvel LL, Seedat S, Groen G. The prevalence of mental health problems in sub-Saharan adolescents living with HIV: a systematic review. Glob Ment Health (Camb) 2020;7:e29. doi: 10.1017/gmh.2020.18. https://europepmc.org/abstract/MED/33489245 .S2054425120000187 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 55.Remien RH, Stirratt MJ, Nguyen N, Robbins RN, Pala AN, Mellins CA. Mental health and HIV/AIDS: the need for an integrated response. AIDS. 2019 Jul 15;33(9):1411–1420. doi: 10.1097/QAD.0000000000002227. https://europepmc.org/abstract/MED/30950883 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 56.Vreeman RC, McCoy BM, Lee S. Mental health challenges among adolescents living with HIV. J Int AIDS Soc. 2017 May 16;20(Suppl 3):21497. doi: 10.7448/IAS.20.4.21497. https://europepmc.org/abstract/MED/28530045 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 57.Woollett N, Cluver L, Bandeira M, Brahmbhatt H. Identifying risks for mental health problems in HIV positive adolescents accessing HIV treatment in Johannesburg. J Child Adolesc Ment Health. 2017 May;29(1):11–26. doi: 10.2989/17280583.2017.1283320. [DOI] [PubMed] [Google Scholar]
- 58.Mellins CA, Brackis-Cott E, Dolezal C, Abrams EJ. The role of psychosocial and family factors in adherence to antiretroviral treatment in human immunodeficiency virus-infected children. Pediatr Infect Dis J. 2004 Nov;23(11):1035–41. doi: 10.1097/01.inf.0000143646.15240.ac.00006454-200411000-00012 [DOI] [PubMed] [Google Scholar]
- 59.Mellins CA, Tassiopoulos K, Malee K, Moscicki AB, Patton D, Smith R, Usitalo A, Allison SM, Van Dyke R, Seage GR, Pediatric HIV/AIDS Cohort Study Behavioral health risks in perinatally HIV-exposed youth: co-occurrence of sexual and drug use behavior, mental health problems, and nonadherence to antiretroviral treatment. AIDS Patient Care STDS. 2011 Jul;25(7):413–22. doi: 10.1089/apc.2011.0025. https://europepmc.org/abstract/MED/21992620 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 60.Naar-King S, Templin T, Wright K, Frey M, Parsons JT, Lam P. Psychosocial factors and medication adherence in HIV-positive youth. AIDS Patient Care STDS. 2006 Jan;20(1):44–7. doi: 10.1089/apc.2006.20.44. [DOI] [PubMed] [Google Scholar]
- 61.Elkington KS, Bauermeister JA, Santamaria EK, Dolezal C, Mellins CA. Substance use and the development of sexual risk behaviors in youth perinatally exposed to HIV. J Pediatr Psychol. 2015 May;40(4):442–54. doi: 10.1093/jpepsy/jsu103. https://europepmc.org/abstract/MED/25476800 .jsu103 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 62.Elkington KS, Teplin LA, Mericle AA, Welty LJ, Romero EG, Abram KM. HIV/sexually transmitted infection risk behaviors in delinquent youth with psychiatric disorders: a longitudinal study. J Am Acad Child Adolesc Psychiatry. 2008 Aug;47(8):901–11. doi: 10.1097/CHI.0b013e318179962b. https://europepmc.org/abstract/MED/18645421 .S0890-8567(08)60057-X [DOI] [PMC free article] [PubMed] [Google Scholar]
- 63.Fair C, Wiener L, Zadeh S, Albright J, Mellins CA, Mancilla M, Tepper V, Trexler C, Purdy J, Osherow J, Lovelace S, Kapetanovic S. Reproductive health decision-making in perinatally HIV-infected adolescents and young adults. Matern Child Health J. 2013 Jul;17(5):797–808. doi: 10.1007/s10995-012-1070-3. https://europepmc.org/abstract/MED/22736033 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 64.Wilson DP, Law MG, Grulich AE, Cooper DA, Kaldor JM. Relation between HIV viral load and infectiousness: a model-based analysis. Lancet. 2008 Jul 26;372(9635):314–20. doi: 10.1016/S0140-6736(08)61115-0.S0140-6736(08)61115-0 [DOI] [PubMed] [Google Scholar]
- 65.Bangsberg DR. Preventing HIV antiretroviral resistance through better monitoring of treatment adherence. J Infect Dis. 2008 May 15;197 Suppl 3:S272–8. doi: 10.1086/533415. [DOI] [PubMed] [Google Scholar]
- 66.Little SJ, Holte S, Routy JP, Daar ES, Markowitz M, Collier AC, Koup RA, Mellors JW, Connick E, Conway B, Kilby M, Wang L, Whitcomb JM, Hellmann NS, Richman DD. Antiretroviral-drug resistance among patients recently infected with HIV. N Engl J Med. 2002 Aug 08;347(6):385–94. doi: 10.1056/NEJMoa013552.347/6/385 [DOI] [PubMed] [Google Scholar]
- 67.Jörns-Presentati Astrid, Napp AK, Dessauvagie AS, Stein DJ, Jonker D, Breet E, Charles W, Swart RL, Lahti M, Suliman S, Jansen R, van den Heuvel LL, Seedat S, Groen G. The prevalence of mental health problems in sub-Saharan adolescents: A systematic review. PLoS One. 2021;16(5):e0251689. doi: 10.1371/journal.pone.0251689. https://dx.plos.org/10.1371/journal.pone.0251689 .PONE-D-20-27670 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 68.Marwick KFM, Kaaya SF. Prevalence of depression and anxiety disorders in HIV-positive outpatients in rural Tanzania. AIDS Care. 2010 Apr;22(4):415–9. doi: 10.1080/09540120903253981.919055798 [DOI] [PubMed] [Google Scholar]
- 69.Collins DL, Leibbrandt M. The financial impact of HIV/AIDS on poor households in South Africa. AIDS. 2007 Nov;21 Suppl 7:S75–81. doi: 10.1097/01.aids.0000300538.28096.1c.00002030-200711007-00009 [DOI] [PubMed] [Google Scholar]
- 70.Hosegood V, Preston-Whyte E, Busza J, Moitse S, Timaeus IM. Revealing the full extent of households' experiences of HIV and AIDS in rural South Africa. Soc Sci Med. 2007 Sep;65(6):1249–59. doi: 10.1016/j.socscimed.2007.05.002. https://linkinghub.elsevier.com/retrieve/pii/S0277-9536(07)00264-X .S0277-9536(07)00264-X [DOI] [PMC free article] [PubMed] [Google Scholar]
- 71.Masanjala W. The poverty-HIV/AIDS nexus in Africa: a livelihood approach. Soc Sci Med. 2007 Mar;64(5):1032–41. doi: 10.1016/j.socscimed.2006.10.009.S0277-9536(06)00520-X [DOI] [PubMed] [Google Scholar]
- 72.Marais BJ, Esser M, Godwin S, Rabie H, Cotton MF. Poverty and human immunodeficiency virus in children: a view from the Western Cape, South Africa. Ann N Y Acad Sci. 2008;1136:21–7. doi: 10.1196/annals.1425.012.annals.1425.012 [DOI] [PubMed] [Google Scholar]
- 73.Bermudez LG, Ssewamala FM, Neilands TB, Lu L, Jennings L, Nakigozi G, Mellins CA, McKay M, Mukasa M. Does Economic Strengthening Improve Viral Suppression Among Adolescents Living with HIV? Results From a Cluster Randomized Trial in Uganda. AIDS Behav. 2018 Nov;22(11):3763–3772. doi: 10.1007/s10461-018-2173-7. https://europepmc.org/abstract/MED/29846836 .10.1007/s10461-018-2173-7 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 74.Ssewamala FM, Dvalishvili D, Mellins CA, Geng EH, Makumbi F, Neilands TB, McKay M, Damulira C, Nabunya P, Sensoy Bahar Ozge, Nakigozi G, Kigozi G, Byansi W, Mukasa M, Namuwonge F. The long-term effects of a family based economic empowerment intervention (Suubi+Adherence) on suppression of HIV viral loads among adolescents living with HIV in southern Uganda: Findings from 5-year cluster randomized trial. PLoS One. 2020;15(2):e0228370. doi: 10.1371/journal.pone.0228370. https://dx.plos.org/10.1371/journal.pone.0228370 .PONE-D-19-19448 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 75.Ramadhani HO, Thielman NM, Landman KZ, Ndosi EM, Gao F, Kirchherr JL, Shah R, Shao HJ, Morpeth SC, McNeill JD, Shao JF, Bartlett JA, Crump JA. Predictors of incomplete adherence, virologic failure, and antiviral drug resistance among HIV-infected adults receiving antiretroviral therapy in Tanzania. Clin Infect Dis. 2007 Dec 01;45(11):1492–8. doi: 10.1086/522991.CID50783 [DOI] [PubMed] [Google Scholar]
- 76.Tuller DM, Bangsberg DR, Senkungu J, Ware NC, Emenyonu N, Weiser SD. Transportation costs impede sustained adherence and access to HAART in a clinic population in southwestern Uganda: a qualitative study. AIDS Behav. 2010 Aug;14(4):778–84. doi: 10.1007/s10461-009-9533-2. https://europepmc.org/abstract/MED/19283464 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 77.Weiser S, Wolfe W, Bangsberg D, Thior I, Gilbert P, Makhema J, Kebaabetswe P, Dickenson D, Mompati K, Essex M, Marlink R. Barriers to antiretroviral adherence for patients living with HIV infection and AIDS in Botswana. J Acquir Immune Defic Syndr. 2003 Nov 01;34(3):281–8. doi: 10.1097/00126334-200311010-00004. [DOI] [PubMed] [Google Scholar]
- 78.Weiser SD, Tuller DM, Frongillo EA, Senkungu J, Mukiibi N, Bangsberg DR. Food insecurity as a barrier to sustained antiretroviral therapy adherence in Uganda. PLoS One. 2010 Apr 28;5(4):e10340. doi: 10.1371/journal.pone.0010340. https://dx.plos.org/10.1371/journal.pone.0010340 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 79.Young S, Wheeler AC, McCoy SI, Weiser SD. A review of the role of food insecurity in adherence to care and treatment among adult and pediatric populations living with HIV and AIDS. AIDS Behav. 2014 Oct;18 Suppl 5(0 5):S505–15. doi: 10.1007/s10461-013-0547-4. https://europepmc.org/abstract/MED/23842717 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 80.Lund C, Breen A, Flisher AJ, Kakuma R, Corrigall J, Joska JA, Swartz L, Patel V. Poverty and common mental disorders in low and middle income countries: A systematic review. Soc Sci Med. 2010 Aug;71(3):517–528. doi: 10.1016/j.socscimed.2010.04.027. https://europepmc.org/abstract/MED/20621748 .S0277-9536(10)00357-6 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 81.Nabunya P, Ssewamala FM, Ilic V. Family Economic Strengthening and Parenting Stress Among Caregivers of AIDS-Orphaned Children: Results from a Cluster Randomized Clinical Trial in Uganda. Child Youth Serv Rev. 2014 Sep 01;44:417–421. doi: 10.1016/j.childyouth.2014.07.018. https://europepmc.org/abstract/MED/25136142 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 82.Ismayilova L, Ssewamala FM, Karimli L. Family support as a mediator of change in sexual risk-taking attitudes among orphaned adolescents in rural Uganda. J Adolesc Health. 2012 Mar;50(3):228–35. doi: 10.1016/j.jadohealth.2011.06.008. https://europepmc.org/abstract/MED/22325127 .S1054-139X(11)00214-X [DOI] [PMC free article] [PubMed] [Google Scholar]
- 83.Ssewamala FM, Karimli L, Chang-Keun H, Ismayilova L. Social Capital, Savings, and Educational Performance of Orphaned Adolescents in Sub-Saharan Africa. Child Youth Serv Rev. 2010 Dec 01;32(12):1704–1710. doi: 10.1016/j.childyouth.2010.07.013. https://europepmc.org/abstract/MED/20948971 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 84.Ismayilova L, Karimli L. Harsh Parenting and Violence Against Children: A Trial with Ultrapoor Families in Francophone West Africa. J Clin Child Adolesc Psychol. 2020;49(1):18–35. doi: 10.1080/15374416.2018.1485103. [DOI] [PubMed] [Google Scholar]
- 85.Lachman J, Wamoyi J, Spreckelsen T, Wight D, Maganga J, Gardner F. Combining parenting and economic strengthening programmes to reduce violence against children: a cluster randomised controlled trial with predominantly male caregivers in rural Tanzania. BMJ Glob Health. 2020 Jul;5(7):e002349. doi: 10.1136/bmjgh-2020-002349. https://gh.bmj.com/lookup/pmidlookup?view=long&pmid=32641291 .bmjgh-2020-002349 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 86.Amerikaner M, Monks G, Wolfe P, Thomas S. Family interaction and individual psychological health. J Couns Dev. 1994;72(6):614–620. doi: 10.1002/j.1556-6676.1994.tb01691.x. [DOI] [Google Scholar]
- 87.Kotchick BA, Dorsey S, Miller KS, Forehand R. Adolescent sexual risk-taking behavior in single-parent ethnic minority families. J Fam Psychol. 1999;13(1):93–102. doi: 10.1037/0893-3200.13.1.93. [DOI] [Google Scholar]
- 88.McNeely C, Shew ML, Beuhring T, Sieving R, Miller BC, Blum RW. Mothers' influence on the timing of first sex among 14- and 15-year-olds. J Adolesc Health. 2002 Sep;31(3):256–65. doi: 10.1016/s1054-139x(02)00350-6.S1054139X02003506 [DOI] [PubMed] [Google Scholar]
- 89.Miller KS, Forehand R, Kotchick BA. Adolescent sexual behavior in two ethnic minority groups: a multisystem perspective. Adolescence. 2000;35(138):313–33. [PubMed] [Google Scholar]
- 90.Resnick MD, Bearman PS, Blum RW, Bauman KE, Harris KM, Jones J, Tabor J, Beuhring T, Sieving RE, Shew M, Ireland M, Bearinger LH, Udry JR. Protecting adolescents from harm. Findings from the National Longitudinal Study on Adolescent Health. JAMA. 1997 Sep 10;278(10):823–32. doi: 10.1001/jama.278.10.823. [DOI] [PubMed] [Google Scholar]
- 91.Hawkins JD, Arthur MW, Catalano RF. Preventing substance abuse. Crime and Justice. 1995;19:343–427. doi: 10.1086/449234. [DOI] [Google Scholar]
- 92.Cluver L, Meinck F, Yakubovich A, Doubt J, Redfern A, Ward C, Salah N, De Stone S, Petersen T, Mpimpilashe P, Romero RH, Ncobo L, Lachman J, Tsoanyane S, Shenderovich Y, Loening H, Byrne J, Sherr L, Kaplan L, Gardner F. Reducing child abuse amongst adolescents in low- and middle-income countries: A pre-post trial in South Africa. BMC Public Health. 2016 Jul 13;16(1):567. doi: 10.1186/s12889-016-3262-z. https://bmcpublichealth.biomedcentral.com/articles/10.1186/s12889-016-3262-z .10.1186/s12889-016-3262-z [DOI] [PMC free article] [PubMed] [Google Scholar]
- 93.Gavin L, Galavotti C, Dube H, McNaghten AD, Murwirwa M, Khan R, St Louis M. Factors associated with HIV infection in adolescent females in Zimbabwe. J Adolesc Health. 2006 Oct;39(4):596.e11–8. doi: 10.1016/j.jadohealth.2006.03.002.S1054-139X(06)00082-6 [DOI] [PubMed] [Google Scholar]
- 94.Jaspan HB, Berwick JR, Myer L, Mathews C, Flisher AJ, Wood R, Bekker LG. Adolescent HIV prevalence, sexual risk, and willingness to participate in HIV vaccine trials. J Adolesc Health. 2006 Nov;39(5):642–8. doi: 10.1016/j.jadohealth.2006.05.016.S1054-139X(06)00196-0 [DOI] [PubMed] [Google Scholar]
- 95.Test FS, Mehta SD, Handler A, Mutimura E, Bamukunde AM, Cohen M. Gender inequities in sexual risks among youth with HIV in Kigali, Rwanda. Int J STD AIDS. 2012 Jun;23(6):394–9. doi: 10.1258/ijsa.2011.011339.23/6/394 [DOI] [PubMed] [Google Scholar]
- 96.Ssewanyana D, Mwangala PN, van Baar A, Newton CR, Abubakar A. Health Risk Behaviour among Adolescents Living with HIV in Sub-Saharan Africa: A Systematic Review and Meta-Analysis. Biomed Res Int. 2018;2018:7375831. doi: 10.1155/2018/7375831. doi: 10.1155/2018/7375831. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 97.Jewkes R, Nduna M, Levin J, Jama N, Dunkle K, Puren A, Duvvury N. Impact of stepping stones on incidence of HIV and HSV-2 and sexual behaviour in rural South Africa: cluster randomised controlled trial. BMJ. 2008 Aug 07;337:a506. doi: 10.1136/bmj.a506. https://europepmc.org/abstract/MED/18687720 .337/aug07_1/a506 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 98.Carney T, Browne FA, Myers B, Kline TL, Howard B, Wechsberg WM. Adolescent female school dropouts who use drugs and engage in risky sex: effects of a brief pilot intervention in Cape Town, South Africa. AIDS Care. 2019 Jan;31(1):77–84. doi: 10.1080/09540121.2018.1500008. https://europepmc.org/abstract/MED/30021470 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 99.Carney T, Johnson K, Carrico A, Myers B. Acceptability and feasibility of a brief substance use intervention for adolescents in Cape Town, South Africa: A pilot study. Int J Psychol. 2020 Dec;55(6):1016–1025. doi: 10.1002/ijop.12668. [DOI] [PubMed] [Google Scholar]
- 100.Jemmott JB, Jemmott LS, O'Leary A, Ngwane Z, Icard L, Bellamy S, Jones S, Landis JR, Heeren GA, Tyler JC, Makiwane MB. Cognitive-behavioural health-promotion intervention increases fruit and vegetable consumption and physical activity among South African adolescents: a cluster-randomised controlled trial. Psychol Health. 2011 Feb;26(2):167–85. doi: 10.1080/08870446.2011.531573. https://europepmc.org/abstract/MED/21318928 .933411620 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 101.Motamedi M, Caldwell L, Wegner L, Smith E, Jones D. Girls Just Want to Know Where to Have Fun: Preventing Substance Use Initiation in an Under-Resourced Community in South Africa Through HealthWise. Prev Sci. 2016 Aug;17(6):700–9. doi: 10.1007/s11121-016-0654-3. https://europepmc.org/abstract/MED/27129478 .10.1007/s11121-016-0654-3 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 102.Resnicow K, Reddy SP, James S, Gabebodeen Omardien R, Kambaran NS, Langner HG, Vaughan RD, Cross D, Hamilton G, Nichols T. Comparison of two school-based smoking prevention programs among South African high school students: results of a randomized trial. Ann Behav Med. 2008 Dec;36(3):231–43. doi: 10.1007/s12160-008-9072-5. [DOI] [PubMed] [Google Scholar]
- 103.Smith EA, Palen L, Caldwell LL, Flisher AJ, Graham JW, Mathews C, Wegner L, Vergnani T. Substance use and sexual risk prevention in Cape Town, South Africa: an evaluation of the HealthWise program. Prev Sci. 2008 Dec;9(4):311–21. doi: 10.1007/s11121-008-0103-z. [DOI] [PubMed] [Google Scholar]
- 104.Tibbits MK, Smith EA, Caldwell LL, Flisher AJ. Impact of HealthWise South Africa on polydrug use and high-risk sexual behavior. Health Educ Res. 2011 Aug;26(4):653–63. doi: 10.1093/her/cyr024. https://europepmc.org/abstract/MED/21511818 .cyr024 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 105.Bermudez LG, Jennings L, Ssewamala FM, Nabunya P, Mellins C, McKay M. Equity in adherence to antiretroviral therapy among economically vulnerable adolescents living with HIV in Uganda. AIDS Care. 2016 Mar;28 Suppl 2(sup2):83–91. doi: 10.1080/09540121.2016.1176681. https://europepmc.org/abstract/MED/27392003 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 106.Han CK, Ssewamala FM, Wang JSH. Family economic empowerment and mental health among AIDS-affected children living in AIDS-impacted communities: evidence from a randomised evaluation in southwestern Uganda. J Epidemiol Community Health. 2013 Mar;67(3):225–30. doi: 10.1136/jech-2012-201601. https://europepmc.org/abstract/MED/23410851 .jech-2012-201601 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 107.Jennings L, Ssewamala FM, Nabunya P. Effect of savings-led economic empowerment on HIV preventive practices among orphaned adolescents in rural Uganda: results from the Suubi-Maka randomized experiment. AIDS Care. 2016;28(3):273–82. doi: 10.1080/09540121.2015.1109585. https://europepmc.org/abstract/MED/26548549 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 108.Ssewamala FM, Han CH, Neilands TB, Ismayilova L, Sperber E. Effect of economic assets on sexual risk-taking intentions among orphaned adolescents in Uganda. Am J Public Health. 2010 Mar;100(3):483–8. doi: 10.2105/AJPH.2008.158840. https://europepmc.org/abstract/MED/20075323 .AJPH.2008.158840 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 109.Bronfenbrenner U. Ecological models of human development. In: Gauvain M, Cole M, editors. Readings on the development of children, 2nd Ed. New York: Freeman; 1993. pp. 37–43. [Google Scholar]
- 110.Earnshaw VA, Chaudoir SR. From conceptualizing to measuring HIV stigma: a review of HIV stigma mechanism measures. AIDS Behav. 2009 Dec;13(6):1160–77. doi: 10.1007/s10461-009-9593-3. https://europepmc.org/abstract/MED/19636699 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 111.Ssewamala FM, Sperber E, Zimmerman JM, Karimli L. The potential of asset‐based development strategies for poverty alleviation in Sub‐Saharan Africa. Int J Soc Welfare. 2010;19(4):433–443. doi: 10.1111/j.1468-2397.2010.00738.x. [DOI] [Google Scholar]
- 112.Sherraden M. Assets and the poor: A new American welfare policy. New York: ME Sharpe; 1991. [Google Scholar]
- 113.Zimmerman GM, Farrell C. Parents, Peers, Perceived Risk of Harm, and the Neighborhood: Contextualizing Key Influences on Adolescent Substance Use. J Youth Adolesc. 2017 Jan;46(1):228–247. doi: 10.1007/s10964-016-0475-5.10.1007/s10964-016-0475-5 [DOI] [PubMed] [Google Scholar]
- 114.Elkington KS, Bauermeister JA, Zimmerman MA. Do parents and peers matter? A prospective socio-ecological examination of substance use and sexual risk among African American youth. J Adolesc. 2011 Oct;34(5):1035–47. doi: 10.1016/j.adolescence.2010.11.004. https://europepmc.org/abstract/MED/21159374 .S0140-1971(10)00165-X [DOI] [PMC free article] [PubMed] [Google Scholar]
- 115.Jacobs W, Amuta-Jimenez AO, Olusanya OA, Bristow AF, Adeloye D, Barry AE. Socio-Ecological Factors of Adolescent Substance Use in Nigeria: A Systematic Review of Literature. J Health Care Poor Underserved. 2020;31(4):1765–1784. doi: 10.1353/hpu.2020.0131. http://hdl.handle.net/20.500.11820/af691cd5-2119-4762-9c37-70abd66eaf1e .S1548686920400221 [DOI] [PubMed] [Google Scholar]
- 116.Scribner R, Theall KP, Simonsen N, Robinson W. HIV risk and the alcohol environment: advancing an ecological epidemiology for HIV/AIDS. Alcohol Res Health. 2010;33(3):179–83. https://europepmc.org/abstract/MED/23584059 . [PMC free article] [PubMed] [Google Scholar]
- 117.Ssewanyana D, Mwangala PN, Marsh V, Jao I, van Baar A, Newton CR, Abubakar A. Socio-ecological determinants of alcohol, tobacco, and drug use behavior of adolescents in Kilifi County at the Kenyan coast. J Health Psychol. 2020 Oct;25(12):1940–1953. doi: 10.1177/1359105318782594. https://europepmc.org/abstract/MED/29944006 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 118.Dohrenwend BP, Levav I, Shrout PE, Schwartz S, Naveh G, Link BG, Skodol AE, Stueve A. Socioeconomic status and psychiatric disorders: the causation-selection issue. Science. 1992 Feb 21;255(5047):946–52. doi: 10.1126/science.1546291. [DOI] [PubMed] [Google Scholar]
- 119.Jones L, Sumnall H. Understanding the relationship between poverty and alcohol misuse. Liverpool: Liverpool John Moores University; 2016. pp. 9–17. [Google Scholar]
- 120.Wagman JA, Nabukalu D, Miller AP, Wawer MJ, Ssekubugu R, Nakowooya H, Nantume B, Park E, Hahn JA, Serwadda DM, Sewankambo NK, Nalugoda F, Kigozi G. Prevalence and correlates of men's and women's alcohol use in agrarian, trading and fishing communities in Rakai, Uganda. PLoS One. 2020;15(10):e0240796. doi: 10.1371/journal.pone.0240796. https://dx.plos.org/10.1371/journal.pone.0240796 .PONE-D-20-07764 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 121.Naamara W, Muhwezi WW. Factors Associated With Alcohol Dependence Among Adult Male Clients in Butabika Hospital, Uganda. J Soc Work Pract Addict. 2014 Jul 03;14(3):322–326. doi: 10.1080/1533256X.2014.936251. https://europepmc.org/abstract/MED/25264430 .936251 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 122.Jones SE, Underwood JM, Pampati S, Le VD, DeGue S, Demissie Z, Adkins SH, Barrios LC. School-Level Poverty and Persistent Feelings of Sadness or Hopelessness, Suicidality, and Experiences with Violence Victimization among Public High School Students. J Health Care Poor Underserved. 2020;31(3):1248–1263. doi: 10.1353/hpu.2020.0092.S1548686920300164 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 123.Reiss F. Socioeconomic inequalities and mental health problems in children and adolescents: a systematic review. Soc Sci Med. 2013 Aug;90:24–31. doi: 10.1016/j.socscimed.2013.04.026.S0277-9536(13)00260-8 [DOI] [PubMed] [Google Scholar]
- 124.Sherraden M. Stakeholding: notes on a theory of welfare based on assets. Soc Serv Rev. 1990;64(4):580–601. doi: 10.1086/603797. [DOI] [Google Scholar]
- 125.Cavazos-Rehg P, Byansi W, Xu C, Nabunya P, Sensoy Bahar Ozge, Borodovsky J, Kasson E, Anako N, Mellins C, Damulira C, Neilands T, Ssewamala FM. The Impact of a Family-Based Economic Intervention on the Mental Health of HIV-Infected Adolescents in Uganda: Results From Suubi + Adherence. J Adolesc Health. 2021 Apr;68(4):742–749. doi: 10.1016/j.jadohealth.2020.07.022. https://europepmc.org/abstract/MED/32980245 .S1054-139X(20)30420-1 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 126.Uganda AIDS Commission, Ministry of Health, and UNAIDS, HIV and AIDS Uganda country progress report 2016-2017. [2023-05-22]. https://www.unaids.org/sites/default/files/country/documents/UGA_2017_countryreport.pdf .
- 127.Chang LW, Grabowski MK, Ssekubugu R, Nalugoda F, Kigozi G, Nantume B, Lessler J, Moore SM, Quinn TC, Reynolds SJ, Gray RH, Serwadda D, Wawer MJ. Heterogeneity of the HIV epidemic in agrarian, trading, and fishing communities in Rakai, Uganda: an observational epidemiological study. Lancet HIV. 2016 Aug;3(8):e388–e396. doi: 10.1016/S2352-3018(16)30034-0. https://europepmc.org/abstract/MED/27470029 .S2352-3018(16)30034-0 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 128.Tumwesigye NM, Atuyambe L, Wanyenze RK, Kibira SP, Li Q, Wabwire-Mangen F, Wagner G. Alcohol consumption and risky sexual behaviour in the fishing communities: evidence from two fish landing sites on Lake Victoria in Uganda. BMC Public Health. 2012 Dec 11;12:1069. doi: 10.1186/1471-2458-12-1069. https://bmcpublichealth.biomedcentral.com/articles/10.1186/1471-2458-12-1069 .1471-2458-12-1069 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 129.Ssewamala FM, Sensoy Bahar Ozge, Nabunya P, Thames AD, Neilands TB, Damulira C, Mukasa B, Brathwaite R, Mellins C, Santelli J, Brown D, Guo S, Namatovu P, Kiyingi J, Namuwonge F, McKay MM. Suubi+Adherence-Round 2: A study protocol to examine the longitudinal HIV treatment adherence among youth living with HIV transitioning into young adulthood in Southern Uganda. BMC Public Health. 2021 Jan 21;21(1):179. doi: 10.1186/s12889-021-10202-3. https://bmcpublichealth.biomedcentral.com/articles/10.1186/s12889-021-10202-3 .10.1186/s12889-021-10202-3 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 130.Nabunya P, Ssewamala FM, Bahar OS, Michalopoulos LTM, Mugisha J, Neilands TB, Trani JF, McKay MM. Suubi4Stigma study protocol: a pilot cluster randomized controlled trial to address HIV-associated stigma among adolescents living with HIV in Uganda. Pilot Feasibility Stud. 2022 Apr 29;8(1):95. doi: 10.1186/s40814-022-01055-7. https://pilotfeasibilitystudies.biomedcentral.com/articles/10.1186/s40814-022-01055-7 .10.1186/s40814-022-01055-7 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 131.Ssewamala FM, Byansi W, Bahar OS, Nabunya P, Neilands TB, Mellins C, McKay M, Namuwonge F, Mukasa M, Makumbi FE, Nakigozi G. Suubi+Adherence study protocol: A family economic empowerment intervention addressing HIV treatment adherence for perinatally infected adolescents. Contemp Clin Trials Commun. 2019 Dec;16:100463. doi: 10.1016/j.conctc.2019.100463. https://linkinghub.elsevier.com/retrieve/pii/S2451-8654(19)30225-X .S2451-8654(19)30225-X [DOI] [PMC free article] [PubMed] [Google Scholar]
- 132.Jalali MS, Botticelli M, Hwang RC, Koh HK, McHugh RK. The opioid crisis: a contextual, social-ecological framework. Health Res Policy Syst. 2020 Aug 06;18(1):87. doi: 10.1186/s12961-020-00596-8. https://health-policy-systems.biomedcentral.com/articles/10.1186/s12961-020-00596-8 .10.1186/s12961-020-00596-8 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 133.Coates J, Swindale A, Bilinsky P. Household Food Insecurity Access Scale (HFIAS) for measurement of food access: indicator guide: version 3. 2007. [2023-05-22]. https://www.fantaproject.org/monitoring-and-evaluation/household-food-insecurity-access-scale-hfias .
- 134.Radloff LS. The CES-D scale: a self-report depression scale for research in the general population. Appl Psychol Meas. 2016;1(3):385–401. doi: 10.1177/014662167700100306. [DOI] [Google Scholar]
- 135.Beck AT, Steer RA, Pompili M. BHS, Beck hopelessness scale: manual. San Antonio, TX: Psychological corporation; 1988. [Google Scholar]
- 136.Coelho GL, Vilar R, Hanel PH, Monteiro RP, Ribeiro MG, Gouveia VV. Optimism scale: evidence of psychometric validity in two countries and correlations with personality. Pers Individ Differ. 2018;134:245–251. doi: 10.1016/j.paid.2018.06.030. https://www.sciencedirect.com/science/article/abs/pii/S0191886918303623 . [DOI] [Google Scholar]
- 137.Cohen S, Kamarck T, Mermelstein R. Perceived stress scale (PSS) J Health Soc Beh. 1983;24:285. doi: 10.1037/t02889-000. https://www.jstor.org/stable/2136404 . [DOI] [PubMed] [Google Scholar]
- 138.Landmark T, Romundstad P, Dale O, Borchgrevink PC, Kaasa S. Estimating the prevalence of chronic pain: validation of recall against longitudinal reporting (the HUNT pain study) Pain. 2012 Jul;153(7):1368–1373. doi: 10.1016/j.pain.2012.02.004.00006396-201207000-00010 [DOI] [PubMed] [Google Scholar]
- 139.National Institute on Drug Abuse (NIDA) National Institute on Drug Abuse (NIDA), NIDA-Modified Alcohol Smoking and Substance Involvement Screening Test (NM-ASSIST) National Institute on Drug Abuse (NIDA); [2023-05-22]. https://www.samhsa.gov/resource/ebp/nida-modified-assist-nm-assist-clinicians-screening-tool-drug-use-general-medical . [Google Scholar]
- 140.Russell DW. UCLA Loneliness Scale (Version 3): reliability, validity, and factor structure. J Pers Assess. 1996 Feb;66(1):20–40. doi: 10.1207/s15327752jpa6601_2. [DOI] [PubMed] [Google Scholar]
- 141.Stark L, Seff I, Hoover A, Gordon R, Ligiero D, Massetti G. Sex and age effects in past-year experiences of violence amongst adolescents in five countries. PLoS One. 2019;14(7):e0219073. doi: 10.1371/journal.pone.0219073. https://dx.plos.org/10.1371/journal.pone.0219073 .PONE-D-19-00495 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 142.Chiang LF, Kress H, Sumner SA, Gleckel J, Kawemama P, Gordon RN. Violence Against Children Surveys (VACS): towards a global surveillance system. Inj Prev. 2016 Apr;22 Suppl 1(Suppl 1):i17–22. doi: 10.1136/injuryprev-2015-041820. https://europepmc.org/abstract/MED/27044493 .injuryprev-2015-041820 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 143.Zimet GD, Dahlem MW, Zimet SG, Farley GK. The multidimensional scale of perceived social support. J Pers Assess. 1990;52(1):30–41. doi: 10.1080/00223891.1990.9674095. [DOI] [PubMed] [Google Scholar]
- 144.Moos RH. Family environment scale manual: Development, applications, research. Palo Alto: Consulting Psychologists Press; 1994. [Google Scholar]
- 145.Skinner HA, Steinhauer PD, Santa-Barbara J. The family assessment measure. Can J Community Ment Health. 2009;2(2):91–103. doi: 10.7870/cjcmh-1983-0018. https://www.cjcmh.com/doi/pdf/10.7870/cjcmh-1983-0018 . [DOI] [Google Scholar]
- 146.Murphy A, Steele M, Dube SR, Bate J, Bonuck K, Meissner P, Goldman H, Steele H. Adverse Childhood Experiences (ACEs) questionnaire and Adult Attachment Interview (AAI): implications for parent child relationships. Child Abuse Negl. 2014 Feb;38(2):224–33. doi: 10.1016/j.chiabu.2013.09.004.S0145-2134(13)00256-1 [DOI] [PubMed] [Google Scholar]
- 147.Shato T, Nabunya P, Byansi W, Nwaozuru U, Okumu M, Mutumba M, Brathwaite R, Damulira C, Namuwonge F, Bahar OS, Neilands TB, Ssewamala FM. Family Economic Empowerment, Family Social Support, and Sexual Risk-Taking Behaviors Among Adolescents Living With HIV in Uganda: The Suubi+Adherence Study. J Adolesc Health. 2021 Sep;69(3):406–413. doi: 10.1016/j.jadohealth.2021.02.005. https://europepmc.org/abstract/MED/33812750 .S1054-139X(21)00090-2 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 148.Berger BE, Ferrans CE, Lashley FR. Measuring stigma in people with HIV: psychometric assessment of the HIV stigma scale. Res Nurs Health. 2001 Dec;24(6):518–29. doi: 10.1002/nur.10011.10.1002/nur.10011 [DOI] [PubMed] [Google Scholar]
- 149.Wilson IB, Lee Y, Michaud J, Fowler FJ, Rogers WH. Validation of a New Three-Item Self-Report Measure for Medication Adherence. AIDS Behav. 2016 Nov;20(11):2700–2708. doi: 10.1007/s10461-016-1406-x. https://europepmc.org/abstract/MED/27098408 .10.1007/s10461-016-1406-x [DOI] [PMC free article] [PubMed] [Google Scholar]
- 150.PATH, Life Planning Skills: A Curriculum for Young People in Africa Uganda Version Facilitator's Manual. 2003. [2023-05-22]. https://www.path.org/resources/life-planning-skills-a-curriculum-for-young-people-in-africa-uganda-version/
- 151.Han CK, Ssewamala FM, Wang JSH. Family economic empowerment and mental health among AIDS-affected children living in AIDS-impacted communities: evidence from a randomised evaluation in southwestern Uganda. J Epidemiol Community Health. 2013 Mar;67(3):225–30. doi: 10.1136/jech-2012-201601. https://europepmc.org/abstract/MED/23410851 .jech-2012-201601 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 152.Ssewamala FM, Ismayilova L, McKay M, Sperber E, Bannon W, Alicea S. Gender and the effects of an economic empowerment program on attitudes toward sexual risk-taking among AIDS-orphaned adolescent youth in Uganda. J Adolesc Health. 2010 Apr;46(4):372–8. doi: 10.1016/j.jadohealth.2009.08.010. https://europepmc.org/abstract/MED/20307827 .S1054-139X(09)00339-5 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 153.Ssewamala FM, Han CK, Neilands TB. Asset ownership and health and mental health functioning among AIDS-orphaned adolescents: findings from a randomized clinical trial in rural Uganda. Soc Sci Med. 2009 Jul;69(2):191–8. doi: 10.1016/j.socscimed.2009.05.019. https://europepmc.org/abstract/MED/19520472 .S0277-9536(09)00305-0 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 154.QSR International QSR International, NVIVO 12. 2018, QSR International. 2018. [2023-05-22]. https://www.businesswire.com/news/home/20180321005288/en/QSR-International-Launches-NVivo-12-Qualitative-Data-Analysis-Software .
- 155.Lincoln YS, Guba EG. In: Naturalistic Inquiry. Guba EG, editor. Newbury Park, CA: Sage Publications; 1985. [Google Scholar]
- 156.Strauss A, Corbin J. Basics of Qualitative Research: Techniques and Procedures for Developing Grounded Theory. Thousand Oaks, CA: Sage; 1998. [Google Scholar]
- 157.Charmaz K. Grounded theory: objectivist and constructivist methods. In: Denzin NK, Lincoln YS, editors. Handbook of Qualitative Research. Thousand Oaks: Sage Publications; 2000. [Google Scholar]
- 158.Boyatzis RE. Transforming qualitative information: Thematic analysis and code development. Thousand Oaks, California: Sage Publications; 1998. [Google Scholar]
- 159.Padgett DK. Qualitative methods in social work research. Thousand Oaks, California: Sage publications; 2016. [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Summary statement for grant reviewed by Center for Scientific Review Special Emphasis Panel Member Conflict: HIV/AIDS Related Behavioral Research.
Data Availability Statement
Data sharing is not applicable to this study as no data sets were generated or analyzed during this study. However, the data sets generated during this study will be available in the National Institute of Mental Health Data Archive.