

Abstract
Background
South Asian individuals experience a higher burden of chronic diseases and limited access to health care services compared with their Caucasian peers. Digital health interventions can enhance the delivery of health care, minimize health inequities, and consequently improve health status among minority ethnic groups. However, it is unclear how South Asian people view and perceive the use of digital health technologies to support their health needs.
Objective
The aim of the review is to identify South Asian individuals’ experiences and attitudes of digital health and explore the barriers and facilitators affecting their use of digital health services.
Methods
The Arksey and O’Malley methodological framework was used to guide this scoping review. Five electronic databases were examined for pertinent papers, which were augmented by searching bibliographies of the retrieved papers and gray literature. A total of 1328 potentially relevant papers were retrieved from the initial search, and the supplemental search added 7 papers to the final list of potentially included papers. Each paper on the initial inclusion list was independently reviewed, leaving 15 papers to be included in the review.
Results
Data were analyzed thematically leading to the development of two overarching themes: (1) barriers to uptake of digital health and (2) facilitators of use of digital health services. There was a general consensus that South Asian communities still struggle with inadequate access to digital health technologies. Some studies suggest multiple initiatives to improve accessibility and acceptability of digital health services within South Asian communities in order to mitigate health disparities and develop a more inclusive health care system. These include the development of multiple-language and culturally sensitive interventions and digital skill development sessions. Most studies were conducted in South Asian countries, focusing on measurable outcomes of digital health interventions. Few explored the experiences and views of South Asian community members residing in the West as a minority ethnic group, for example, British South Asians.
Conclusions
Literature mapping proposes that South Asian people frequently struggle with a health care system that may limit their access to digital health services, and sometimes fails to consider social and cultural needs. There is growing evidence that digital health interventions have the potential to facilitate supported self-management, which is part of the plans to adopt person-centered care. These interventions are particularly important for overcoming some of the challenges, for example, time constraints, safety, and gender sensitivity, associated with the delivery of health care interventions in minority ethnic groups such as South Asians in the United Kingdom, and thus to improve minority ethnic groups’ access to health care services to support individual health needs, and consequently enhance health status.
Keywords: South Asians, Asia, digital health, eHealth, mHealth, mobile health, aging, ethnicity, ethnic, culturally sensitive, cultural sensitivity, inequality, inequalities, disparity, disparities, physical activity, exercise, immigrant, scoping review, experience, attitude, barrier, facilitator, opinion, adoption, digital divide, accessibility, minority, mobile phone
Introduction
The concept of enhancing health care delivery and support through electronic means (ie, digital health) is gaining popularity worldwide [1]. Indeed, the current pandemic (COVID-19) and associated surge in health care demands necessitated a greater shift from traditional health care delivery (face-to-face) to digital health care. The term “digital health” has a wide variety of definitions in different contexts, with Oh et al [2] highlighting 51 different definitions in their systematic review. However, for the purposes of this paper, “digital health” can be generally defined as the intersection of health care with information and communication technology [3]. It can also include eHealth and mobile health (mHealth). There are various forms of digital health technologies, which include the use of electronic patient records, telemedicine for remote support and monitoring of patients, and smartphone or tablet apps to arrange medical appointments or request medication prescriptions. These methods have the potential to augment and facilitate health care delivery and meet health care targets of government departments, policy makers, and health care providers; for example, to improve patient outcomes and enhance the productivity and efficiency of the health system [4,5]. Digital health technology also has the potential to assist in providing more equitable access to health services, hence, mitigating health disparities especially for those classified as clinically vulnerable and those from minority ethnic groups, such as South Asians in the United Kingdom [6].
South Asian people account for nearly 20% of the global population. The term “South Asian” conventionally refers to individuals whose ethnic roots originate in the Indian subcontinent including India, Pakistan, and Bangladesh. In the United Kingdom, the South Asian population is the largest minority ethnic group, comprising about 3 million individuals (5.3% of the total population) [7].
The literature focusing on South Asian communities suggests that they experience poorer health, a higher burden of chronic diseases, and development of cardiovascular diseases at a younger age compared with their White peers [8,9]. A systematic review concluded that South Asian populations have higher prevalence of hypertension, cardiovascular diseases, and type 2 diabetes and are also less likely to engage in physical activities and exercise [10]. Their experience may be exacerbated by the reported ethnic disparities and inadequate access to health care services [11].
As advocates of digital health claim that it could help improve the delivery of health services and reduce health inequities among underrepresented communities, it is necessary to first explore the targeted population’s views and perceptions of using digital health technologies. This is likely to help in determining the feasibility and acceptability of digital health interventions within these communities. This paper will focus on South Asian communities as one of the largest ethnic groups worldwide.
Methods
Study Design
The Arksey and O’Malley [12] framework for scoping reviews was used to guide this review of the current literature pertaining to South Asian individuals’ experiences and perceptions of using digital to support their health needs. Scoping reviews aim to systematically assess the breadth, depth, and characteristics of the substantive literature [13]. They attempt to provide a broad overview of the current literature; hence, a formal quality appraisal of the included studies is not always a requirement [14,15]. This allows scoping reviews to include a broader range of literature compared to systematic reviews [16]. Although formal quality assessment is not always necessary, the methodological issues within the relevant included literature are discussed.
The framework by Arksey and O’Malley [12] for scoping reviews consists of 5 phases: identification of the research question, identification of the relevant papers, development of eligibility criteria for paper selection, charting the extracted data, and reporting the findings. The framework also includes an additional, but optional, sixth phase: consulting key stakeholders, as they may offer additional resources or new thoughts that have not been discussed in the literature yet. This review included only phases 1-5, and the reporting criteria are informed by the PRISMA-ScR (Preferred Reporting Items for Systematic Reviews and Meta-Analyses extension for Scoping Reviews) checklist [17].
Identifying Research Question
The review question was “What are the experiences and perceptions of South Asian adults of digital health interventions to support their health needs?”
Identifying Relevant Papers
The mnemonic population, interest, and context were used to identify search terms and keywords that were relevant to the review question [18]. Textbox 1 presents the search strategy. The ASSIA, PsycINFO, MEDLINE, Embase, and PubMed databases were searched. In addition, eHealth-related websites including EU*US eHealth Work and Digital Health & Care Scotland were searched for gray literature. To expand the scope of the review, the database search was not limited by the time of publication and included papers that were published in English.
Search strategy.
Inclusion criteria
Paper type: published and nonpublished (gray literature) papers
Language: English
Population: South Asian adults
Interest: eHealth
Context: all health care settings
Exclusion criteria
Language: non-English
Population: other Asians, other ethnicities, age<18 years
Interest: traditional delivery of health care
Paper Selection
The initial search retrieved 1328 papers. Seven additional papers were added from the bibliographies of retrieved papers and gray literature. Two of the authors independently reviewed the titles and abstracts of the papers potentially to be included, resulting in 46 eligible full-text papers. When the full-text papers were reviewed, a further 31 were excluded for reasons such as not being specifically related to eHealth interventions or the reviewer being unable to ascertain the ethnicity of participants, leaving 15 papers to be included in the review (Figure 1).
Figure 1.
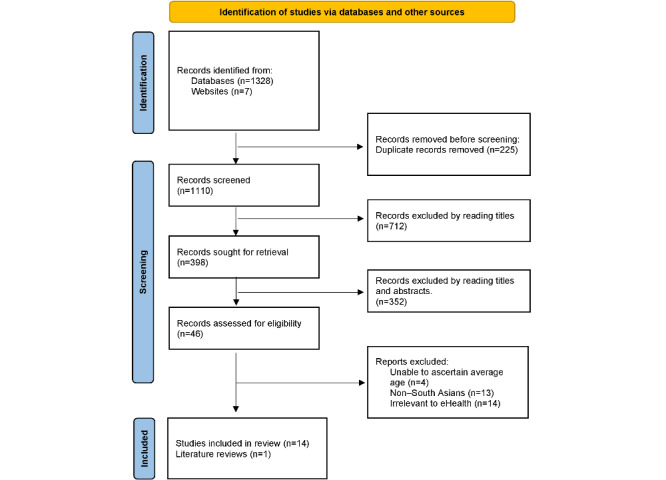
Flowchart of literature search.
Charting the Data
Relevant data were extracted from the included papers, including authors, date of publication, study sample, methods, and findings (Table 1).
Table 1.
Charting the data.
| Author (year) | Country | Study objective | Study sample | Methods | Findings |
| Anand et al (2016) [20] | Canada | What is the impact of messaging (emails and texting) focused on improving diet and physical activity (PA) in reducing risk for myocardial infarction (MI) among a South Asian community in Canada? |
|
|
|
| DeSouza et al (2014) [21] | India | To explore the acceptability of delivering health care interventions through mobile phones among users in India |
|
|
|
| Hoque et al (2017) [22] | Bangladesh | To investigate factors that influence patients to adopt and use eHealth apps in Bangladesh |
|
|
|
| Horne et al (2018) [23] | United Kingdom | To identify interventions focused on increasing PA levels among South Asian adults and identify the specific changes in the content and delivery mode of these interventions | —a |
|
|
| Hossain et al (2019) [24] | Bangladesh | To explore the factors that influence rural end users’ acceptance of eHealth in Bangladesh |
|
|
|
| Hyman et al (2022) [25] | Canada | To understand the barriers to and facilitators of digital health tool uptake experienced by South Asian community in Canada |
|
|
|
| Kumar et al (2019) [26] | India | To assess the acceptability of mobile phone support during care and treatment in patients with tuberculosis in South India |
|
|
|
| Makowsky et al (2021) [27] | Canada | To explore the increase, patterns, and predictors of the use of the internet, digital devices, and apps for health purposes in South Asian Canadians |
|
|
|
| Prinjha et al (2020) [28] | United Kingdom | To explore the perceptions and views of British South Asian patients with type 2 diabetes on mobile health texting to support medication adherence |
|
|
|
| Quaosar et al (2018) [29] | Bangladesh | To identify the factors that influence the elderly’s intention to use mHealth services |
|
|
|
| Ramachandran et al (2015) [30] | India | To assess willingness to receive health-related information through mobile phones (mHealth intervention) |
|
|
|
| Teo et al (2021) [31] | Singapore | To evaluate elderly Asians’ acceptance toward digital health services amid the pandemic (COVID-19) |
|
|
|
| Vyas et al (2013) [32] | United States | To better understand health-related behaviors within South Asian community in the United States |
|
|
|
| Yasmin et al (2020) [33] | Bangladesh | To explore the perceptions of patients with type 2 diabetes of an mHealth intervention for diabetes management |
|
|
|
| Zibrik et al (2015) [34] | Canada | To assess eHealth literacy and explore barriers to eHealth self-management | Surveys:
|
|
|
aNot available.
Results
An Overview of the Findings
The 15 papers included emanated from different parts of the globe, most from Canada (n=4) and Bangladesh (n=4), followed by India (n=3). Other countries generated 1 or 2 papers.
Different methodologies were used; quantitative designs, including randomized controlled trials and descriptive designs, were most frequently used (n=9). The methodological designs of the included papers were quantitative (n=9), qualitative (n=4), mixed method (n=1), and systematic review (n=1).
Thematic Analysis of the Findings
Overview
Thematic analysis facilitates the identification of issues that are discussed frequently in data and can be modified to be used for reviews of literature [35]. Thematic analysis of the data and discussions was performed with NVivo 12 (Lumivero, 2018). It was noticed that terms such as “eHealth,” “mHealth,” and “digital health” were used sometimes interchangeably in the reviewed papers. For clarification purpose, in this review, “digital health” is used as a generic term to refer to all health care interventions that are delivered via electronic means (Table 2).
Table 2.
eHealth term or intervention discussed by authors.
| Term | Studies |
| eHealth: portable health clinic (PHC) | Hossain et al [24] |
| mHealth: interactive calls and call center | Yasmin et al [33] |
| mHealth: voice calls and texting | DeSouza et al [21] and Ramachandran et al [30] |
| Digital health: email and texting | Anand et al [20] |
| Health apps and web-based sources | Makowsky et al [27] |
| Internet for health purposes | Vyas et al [32] |
| Photovoice | Hyman et al [25] |
| mHealth: video-based calls and in-person | Kumar et al [26] |
| mHealth: texting | Prinjha et al [28] |
| Digital health service | Teo et al [31] |
Thematic analysis of the included papers resulted in the development of 2 major themes, each encompasses a number of subsidiary categories.
Theme 1: Barriers to the Uptake of Digital Health
Several subsidiary categories form the overarching theme that discusses barriers to the uptake of the digital health.
Level of Literacy
Limited English proficiency is frequently noted as a barrier to accessing digital health services for South Asian community members, particularly older individuals. In a study of the use of digital health by senior immigrants in Canada, only 25% of the Punjabi participants reported advanced English proficiency [34]. Reading and writing fluency in the English language are assumed to be a requirement for effective use of digital health services. Moreover, in a qualitative study to explore the barriers to and facilitators of accessing a digital health intervention, “Photovoice,” most of the older South Asian Canadians had struggled to use the intervention due to their limited proficiency in English [25]. The participants also cited a problem with translation of the intervention content as it was perceived as either too academic or improperly translated. Thus, digital health interventions should avoid the use of complicated medical terminology and provide health information in a simplified (ie, everyday) language to make it more accessible for all end users.
Although provision of digital health interventions in multiple languages seems beneficial, the evidence supporting this claim is inconclusive. Prinjha et al [28] stated that the written versions of some South Asian languages may be too formal and difficult for most people to understand, and some dialects do not have a written form. Indeed, many older people from the same ethnicity reported difficulty reading or writing in any language [25]. In a cross-sectional study to explore the acceptability of using mHealth to manage tuberculosis in India, Kumar et al [26] reported that more than 20% of participants (mean age 35 years) had no formal education. Therefore, the provision of multilanguage options is not necessarily effective in enhancing the use and uptake of eHealth interventions among older South Asian people. According to Prinjha et al [28], the vast majority of British South Asians understand English, and those who speak no or little English could rely on their children or grandchildren for translation. In addition, the authors suggested the provision of health information in languages other than English might not be helpful for encouraging recently immigrated South Asians to improve their English fluency.
Technology Literacy
In terms of technology literacy, older South Asian individuals (aged 65 years or older) commonly rated their literacy as low or even none. The difficulties associated with using technology and accessing web-based health information were frequently mentioned as a barrier to improving digital health literacy within this population [25,27]. This lack of technology literacy might contribute to exacerbating the identified digital divide within the general community and leaving the South Asian group behind in terms of research and health policy. Kumar et al [26] stated that more than 40% (64 out of 151) of their study participants in India did not know how to use the camera on their phones. However, this percentage might have been lower if the study had included South Asian immigrants in one of the developed countries as they tend to have better level of education [32].
Negative Preconceptions of Digital Health
Prior to introducing a new initiative, it is always important to measure the feasibility of the specific intervention and whether it is acceptable to the target community. The uptake of many digital health interventions appears to have been hampered by sociotechnical challenges, lack of trust, mismatch between design and user needs, and other adoption hurdles specific to at-risk and clinically vulnerable groups such as immigrants and older adults [23,24]. There are also concerns about the detrimental health impacts of technology (particularly cell phones) and the perception that excessive use of technology interferes with spending time with family [34]. This is an essential aspect when developing or introducing a digital health intervention, especially for people from family-oriented cultures such as South Asians [31].
Time Constraints
Learning to use technology, especially for health reasons, was often constrained by lack of time. Many South Asian men are involved in jobs that require long working hours and struggle with work pressure [32,33] resulting in little or no time for self-care. The social expectations of women in South Asian communities in Canada also appear to play a role in them being unable to learn or use digital health tools [25]. Moreover, due to associated familial and household duties, they are less likely to undertake the recommended amount of physical activity. However, in comparison with conventional ways of self-care such as joining a physical activity group, digital health interventions might be more accessible and supportive for South Asian people to manage and improve their health status. They (digital health interventions) could be a solution for older South Asian individuals to overcome time constraints that hinder their self-management of their health conditions.
Gender Sensitivity (Roles)
The roles associated with people based on their gender seem to be a factor in the likelihood of and acceptance of digital health. Makowsky et al [27] studied the use of internet and digital devices for health purposes among Canadian South Asians, suggesting that being a woman was independently correlated with lower likelihood of health-related internet use. In these communities that are largely dominated by males, females are less likely to use digital health and, in Bangladesh, they may even need permission from their male family members to buy or use a technology device [33]. This has been partly linked with socioeconomic status and social and cultural norms in South Asian communities [22,24]. In contrast, it was suggested that female Punjabi adults in Canada, compared to males, were more knowledgeable about web-based health resources and the quality of these resources [34]. This, however, could be related to the immigration status of many of these participants, who had lived in a Western country for more than 20 years, which might have altered some of their cultural norms. This is corroborated by a study of South Asian community members in Canada, which also proposed that their culture is changing toward gender equality [25].
Unlike older South Asian men, women might be more sensitive to cultural values, for example, modesty, that may limit their freedom to maintain a healthy lifestyle. In a systematic review, Horne et al [23] suggested that interventions to increase the level of physical activity that are not culturally sensitive, for example, involve exercising in a mixed gender facility, may be unacceptable or ineffective for South Asian women. Other issues that might hamper the success of these interventions include safety and unfavorable weather [33]. Thus, digital health interventions might be a suitable alternative to traditional initiatives to increase the uptake of exercise and improve health in general within South Asian communities. These digital health interventions are likely to be safer because they do not require people to leave their own home, more acceptable because they do not involve unfavorable physical mixing with the other gender, and weather-independent.
Aging and Self-Efficacy
The lack of confidence and fear of learning among older community members in Canada were also thought to hinder the uptake of digital health services [34]. Some older people have a misconception that they cannot learn anything new since they are 60 years or older [25]. They believe that there is too much to learn and that they are unable to absorb new concepts, which sometimes demotivates them from engaging in the learning and use of digital health services. Therefore, it is important to improve their confidence and digital literacy levels to ensure their inclusion in the new system of health care, that is, digital health. Zibrik et al [34] reported that over 65% of their South Asian Canadian participants had the desire to improve their digital skills to better manage their health conditions. This indicates that training courses to enhance older peoples’ digital literacy might be in high demand and are likely to attenuate the digital divide gap and improve their health outcomes. These courses could also help to increase the awareness of digital health interventions available. However, Hyman et al [25] suggested that the cost of training courses should be considered because some older people might struggle to afford them.
Lack of Trust in Digital Health Services
The literature pertinent to the use of digital health has indicated that there is an association between trust and the use of digital health services. Hoque et al [22] surveyed 326 participants in Bangladesh and argued that trust was an important prerequisite for the use of eHealth services and that there was a positive relationship between trust and intention to use eHealth. The more the patients trust digital health interventions (eg, mHealth), the more they are willing to share their health status and medical information [29]. In congruence, Hyman et al [25] reported that some older participants in Canada had relatively low trust in digital health and often opted for conventional ways, for example, visiting a doctor rather than using digital health services to seek medical advice. Moreover, those who obtain health information from the internet often feel they need to double-check with their family doctor. This preference for conventional ways could be related to the participants’ age group (>50 years), or fear of their information being misused, or it might have a cultural basis, where physical interactions are normally preferred over web-based communication.
Communication Preferences
Despite the recent exponential increase in the use of web-based communication, face-to-face interaction seems to remain a preference for many older South Asian individuals. Prinjha et al [28] explained that older British South Asians preferred attending face-to-face groups to discuss management of their health conditions over receiving health recommendations via texting. This was also corroborated by a study of 709 South Asian people in the United States to determine their health information resources [32]. Although the majority of participants cited the internet (42.8%), followed by physicians (36.9%) as their key resources for health information, older participants were inclined to choose physicians over the internet. The study, however, was limited to participants who were fluent in English, dismissing other South Asian adults with varying levels of English proficiency. Having conducted a randomized control trial to assess the impact of a digital health intervention (emails and texting) on improving diet and physical activity, Anand et al [20] proposed that face-to-face contacts may result in better outcomes. In contrast, the majority of patients in India (98% and 60%) preferred receiving health information via mobile phones [21,30]. However, voice calls were often preferred over texting for those participants. In the latter 2 studies, preference for texting was linked with gender, age, and literacy in English. However, the recent pandemic (COVID-19) and its consequences that have forced a shift in the health care delivery mode (from traditional to digital health) might now have changed the negative perceptions of digital health among people, especially older ones.
Theme 2: Facilitators of the Use of Digital Health
To overcome some of the challenges associated with successful adoption of digital health in South Asian communities, the literature has suggested several strategies such as social support and digital skills training opportunities [25,33]. The strong cultural emphasis on family life within these communities can be used to promote the uptake of digital health services. Prinjha et al [28] discussed the significant role of family members in supporting older British South Asian individuals in using technology to arrange an appointment with their doctor or request an electronic prescription. Thus, social support from family members, particularly younger adults, in South Asian culture is likely to facilitate the acceptance and use of eHealth services. Reliance on social support, however, is not necessarily a facilitator; it can sometimes be a barrier to technology use [34]. Heavy reliance of older adults on their children or grandchildren to help them with using digital health services might be counterproductive for improving the level of digital literacy among older adults. Thus, in parallel with social support, older adults should be encouraged to self-manage their health status and maintain their independence.
To enhance digital health literacy, computer classes and hands-on workshops have been cited as mitigating the digital gap between older South Asian adults and the general community in Canada [27]. These classes are likely to enable the use of health technologies, spark older people’s curiosity, and reduce their dependence on others to manage their health needs [25]. However, the site of delivery of these workshops should be carefully considered. As Horne et al [23] suggested, the use of community facilities and familiar gathering places, for example, temples, is essential for the accessibility and acceptability of community-based interventions for older South Asian people.
In terms of improving health literacy, many older adults in India suggest the use of conventional modes of communication, for example, television, radio, or even voice calls, in order to reach individuals who are less familiar with modern technology [26]. These modes can additionally be used to increase the awareness among older adults about digital health technologies and learning opportunities to improve their digital literacy. Hyman et al [25] stated that many older South Asian Canadian members, following participation in a digital health intervention (Photovoice), which promoted learning about eHealth services and health in general, highlighted the importance of the intervention being accessible and simple. This indicates that carefully designed digital health interventions that consider accessibility, ease of use, and the social and cultural preferences of the end users can effectively support older adults to self-maintain and manage their own health.
Discussion
Principal Findings
This scoping review sought to map the existing knowledge pertaining to the experiences and views of South Asian communities on using digital health to support their health needs. The findings indicate that South Asian populations experience limited access to digital health services. South Asian people, especially older adults, encounter multiple sociotechnical challenges that constrain their access to learning about or using digital health services, including limited English language proficiency [34], low levels of technology literacy [26,27], and lack of trust in digital health [25]. Therefore, this inadequate access to digital health services, if not addressed, may widen the digital divide gap between South Asian communities and the general population and exacerbate health disparities.
A number of authors have claimed that the development of multiple-language digital health interventions could help some South Asian community members to overcome the English language barrier [25,34]. Providing a digital health intervention in the end user’s preferred language is more likely to increase its acceptability and usability. However, it should be noted that South Asian communities are heterogeneous in terms of spoken language and that some dialects have no written form. Thus, a prior discussion with the targeted population is crucial to identify the preferred languages that should be used in the digital health intervention.
In terms of sociocultural barriers, time constraints and gender roles sensitivity have been frequently cited by older South Asian individuals, including those residing in Western countries, as major barriers to the use and uptake of digital health services [27,33]. It was reported that there is often little or no time to learn or explore digital health services due to work-related pressure or familial responsibilities. Moreover, health interventions that involve the mixing of men and women in 1 avenue (eg, gymnasium) are less preferred within South Asian communities [23]. Digital health interventions, in comparison with traditional interventions, require relatively less time as they do not require relocation (eg, going from work or home to gymnasium center) or unfavorable mixing with different genders. However, access to digital health services can also be hampered by gender inequity within South Asian countries [33]. Therefore, it is necessary to measure access to digital health tools within the targeted community prior to introducing or implementing a digital health intervention, as the level of accessibility would likely impact on the intervention usability and effectiveness.
Concerns about using digital health interventions (eg, confidentiality) and preference for conventional ways of communication are positively associated. People often opt for face-to-face health visits because they are more reliable and trustworthy compared to web-based consultation for instance. Thus, a number of studies reported that older South Asian adults prefer conventional ways of communication to meet their health needs [25,28]. However, most of these studies compared physical health visits to emails or texting, which require higher ability in reading and writing. Video calls, on the other hand, such as Teams or Zoom, can be relatively easy to use regardless of the user’s level of literacy. Therefore, older adults may find video calls easier than using emails or texting services, and equally usable compared to traditional ways, to support their health needs. However, a comparative study to compare video calls to face-to-face visits for health purposes is warranted to support this assumption.
To overcome some of the barriers to the use of digital health services, a few authors have suggested social support and digital skills training sessions for older adults [27,33]. These suggestions are expected to encourage older adults to learn and use digital health services, address their trust concerns, and improve their confidence in using new modern technology for health purposes. However, the cost of these sessions should be considered as some individuals may find it unaffordable.
Despite the South Asian communities being one of the largest ethnic groups in the world, this review identified only a relatively small number of papers that discussed their experiences and perceptions of digital health. This highlights the underrepresentation of these communities in the international literature and urges further exploration of these communities in order to improve the health status of South Asian communities and potentially mitigate current health disparities. Furthermore, there were even fewer papers that focused on South Asian people who are residing permanently in the West, for example, British South Asians. Thus, there is an increasing demand to explore the experiences and attitudes of these minority communities in order to improve their health status and ensure the development of an inclusive health care system.
Limitations
This review of literature encountered some limitations. First, it was not clear that the findings of studies conducted in South Asian countries are transferable to South Asians residing in Western countries. Second, there was a risk of selection bias as the included papers were not formally assessed for quality. This risk, however, was reduced by the use of a dual independent review throughout the selection and data extraction processes. Moreover, the review focus was expanded from older (50+ years) South Asian individuals to include all South Asians due to the very limited number of papers retrieved by the initial search.
Conclusions
This paper reviewed the literature on South Asian individuals’ experiences and perceptions of digital health, highlighting the barriers and facilitators affecting their use of digital health services. It has become evident that South Asian ethnic groups are generally overlooked in the international health-related literature. It is concerning that South Asian people’s health needs are not always explicitly highlighted and addressed. Yet, many health interventions have been developed and implemented aiming to improve the health status of these communities. The basis of these interventions has largely relied on international literature, which can sometimes fail to take South Asian people’s circumstances and needs into account, risking wasting their time and resources.
Digital health interventions have the potential to facilitate supported self-management, which is part of the British National Health Service’s long-term plan to adopt person-centered care. These interventions are particularly important for overcoming some of the challenges, for example, time constraints, safety, and gender sensitivity, associated with the delivery of health care interventions in minority ethnic groups such as South Asians in the United Kingdom.
Acknowledgments
The authors would like to thank King Abdullah Medical City (Mecca) for supporting NA to conduct this review. This research was supported by Policy@ Manchester as part of the QR Strategic Priorities Fund grant monies allocation from United Kingdom Research and Innovation (UKRI), Research England and Healthy Ageing Research Group at the University of Manchester, as well as being supported by National Institute for Health Research (NIHR) Applied Research Collaboration Greater Manchester (ARC-GM).
Abbreviations
- mHealth
mobile health
- PRISMA-ScR
Preferred Reporting Items for Systematic Reviews and Meta-Analyses extension for Scoping Reviews
Full details of the included papers.
Data Availability
Full details of the included papers are submitted in Multimedia Appendix 1.
Footnotes
Conflicts of Interest: None declared.
References
- 1.Global strategy on digital health 2020-2025. World Health Organization. 2021. [2023-05-16]. https://www.who.int/docs/default-source/documents/gs4dhdaa2a9f352b0445bafbc79ca799dce4d.pdf .
- 2.Oh H, Rizo C, Enkin M, Jadad A. What is eHealth (3): a systematic review of published definitions. J Med Internet Res. 2005;7(1):e1. doi: 10.2196/jmir.7.1.e1. https://www.jmir.org/2005/1/e1/ v7e1 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Blake A, Blake R, Hulkkonen P, Huotari S, Jauhiainen M, Tolonen J, Värri A. An overview of eHealth. eHealth WORK. 2020. [2023-05-16]. http://ehealthwork.org/FC/overview1.html .
- 4.Shah SS, Gvozdanovic A, Knight M, Gagnon J. Mobile app-based remote patient monitoring in acute medical conditions: prospective feasibility study exploring digital health solutions on clinical workload during the COVID crisis. JMIR Form Res. 2021;5(1):e23190. doi: 10.2196/23190. https://formative.jmir.org/2021/1/e23190/ v5i1e23190 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Wongvibulsin S, Habeos EE, Huynh PP, Xun H, Shan R, Rodriguez KAP, Wang J, Gandapur YK, Osuji N, Shah LM, Spaulding EM, Hung G, Knowles K, Yang WE, Marvel FA, Levin E, Maron DJ, Gordon NF, Martin SS. Digital health interventions for cardiac rehabilitation: systematic literature review. J Med Internet Res. 2021;23(2):e18773. doi: 10.2196/18773. https://www.jmir.org/2021/2/e18773 .v23i2e18773 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Eysenbach G. What is e-health? J Med Internet Res. 2001;3(2):e20. doi: 10.2196/jmir.3.2.e20. https://www.jmir.org/2001/2/e20 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Population of England and Wales. Gov.UK. 2020. [2023-05-16]. https://www.ethnicity-facts-figures.service.gov.uk/uk-population-by-ethnicity/national-and-regional-populations/population-of-england-and-wales/latest .
- 8.Patel AP, Wang M, Kartoun U, Ng K, Khera AV. Quantifying and understanding the higher risk of atherosclerotic cardiovascular disease among South Asian individuals: results from the UK biobank prospective cohort study. Circulation. 2021;144(6):410–422. doi: 10.1161/CIRCULATIONAHA.120.052430. https://www.ahajournals.org/doi/10.1161/CIRCULATIONAHA.120.052430 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Cainzos-Achirica M, Fedeli U, Sattar N, Agyemang C, Jenum AK, McEvoy JW, Murphy JD, Brotons C, Elosua R, Bilal U, Kanaya AM, Kandula NR, Martinez-Amezcua P, Comin-Colet J, Pinto X. Epidemiology, risk factors, and opportunities for prevention of cardiovascular disease in individuals of South Asian ethnicity living in Europe. Atherosclerosis. 2019;286:105–113. doi: 10.1016/j.atherosclerosis.2019.05.014. https://www.atherosclerosis-journal.com/article/S0021-9150(19)30432-0/fulltext .S0021-9150(19)30432-0 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Rana A, de Souza RJ, Kandasamy S, Lear SA, Anand SS. Cardiovascular risk among South Asians living in Canada: a systematic review and meta-analysis. CMAJ Open. 2014;2(3):E183–E191. doi: 10.9778/cmajo.20130064. https://www.cmajopen.ca/content/2/3/E183 .20130064 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Razai MS, Kankam HKN, Majeed A, Esmail A, Williams DR. Mitigating ethnic disparities in covid-19 and beyond. BMJ. 2021;372:m4921. doi: 10.1136/bmj.m4921. https://www.bmj.com/content/372/bmj.m4921 . [DOI] [PubMed] [Google Scholar]
- 12.Arksey H, O'Malley L. Scoping studies: towards a methodological framework. Int J Soc Res Methodol. 2005;8(1):19–32. doi: 10.1080/1364557032000119616. https://www.tandfonline.com/doi/abs/10.1080/1364557032000119616 . [DOI] [Google Scholar]
- 13.Munn Z, Peters MDJ, Stern C, Tufanaru C, McArthur A, Aromataris E. Systematic review or scoping review? Guidance for authors when choosing between a systematic or scoping review approach. BMC Med Res Methodol. 2018;18(1):143. doi: 10.1186/s12874-018-0611-x. https://bmcmedresmethodol.biomedcentral.com/articles/10.1186/s12874-018-0611-x .10.1186/s12874-018-0611-x [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Levac D, Colquhoun H, O'Brien KK. Scoping studies: advancing the methodology. Implement Sci. 2010;5:69. doi: 10.1186/1748-5908-5-69. https://implementationscience.biomedcentral.com/articles/10.1186/1748-5908-5-69 .1748-5908-5-69 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Peterson J, Pearce PF, Ferguson LA, Langford CA. Understanding scoping reviews: definition, purpose, and process. J Am Assoc Nurse Pract. 2017;29(1):12–16. doi: 10.1002/2327-6924.12380. https://journals.lww.com/jaanp/Citation/2017/01000/Understanding_scoping_reviews__Definition,.5.aspx . [DOI] [PubMed] [Google Scholar]
- 16.Pham MT, Rajić A, Greig JD, Sargeant JM, Papadopoulos A, McEwen SA. A scoping review of scoping reviews: advancing the approach and enhancing the consistency. Res Synth Methods. 2014;5(4):371–385. doi: 10.1002/jrsm.1123. https://onlinelibrary.wiley.com/doi/10.1002/jrsm.1123 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Tricco AC, Lillie E, Zarin W, O'Brien KK, Colquhoun H, Levac D, Moher D, Peters MDJ, Horsley T, Weeks L, Hempel S, Akl EA, Chang C, McGowan J, Stewart L, Hartling L, Aldcroft A, Wilson MG, Garritty C, Lewin S, Godfrey CM, Macdonald MT, Langlois EV, Soares-Weiser K, Moriarty J, Clifford T, Tunçalp Ö, Straus SE. PRISMA extension for scoping reviews (PRISMA-ScR): checklist and explanation. Ann Intern Med. 2018;169(7):467–473. doi: 10.7326/M18-0850. https://www.acpjournals.org/doi/10.7326/M18-0850 .2700389 [DOI] [PubMed] [Google Scholar]
- 18.Stern C, Jordan Z, McArthur A. Developing the review question and inclusion criteria. Am J Nurs. 2014;114(4):53–56. doi: 10.1097/01.NAJ.0000445689.67800.86. https://journals.lww.com/ajnonline/Fulltext/2014/04000/Developing_the_Review_Question_and_Inclusion.30.aspx .00000446-201404000-00030 [DOI] [PubMed] [Google Scholar]
- 19.Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, Shamseer L, Tetzlaff JM, Akl EA, Brennan SE, Chou R, Glanville J, Grimshaw JM, Hróbjartsson A, Lalu MM, Li T, Loder EW, Mayo-Wilson E, McDonald S, McGuinness LA, Stewart LA, Thomas J, Tricco AC, Welch VA, Whiting P, Moher D. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021;372:n71. doi: 10.1136/bmj.n71. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Anand SS, Samaan Z, Middleton C, Irvine J, Desai D, Schulze KM, Sothiratnam S, Hussain F, Shah BR, Pare G, Beyene J, Lear SA, South Asian Heart Risk Assessment Investigators A digital health intervention to lower cardiovascular risk: a randomized clinical trial. JAMA Cardiol. 2016;1(5):601–606. doi: 10.1001/jamacardio.2016.1035. https://jamanetwork.com/journals/jamacardiology/fullarticle/2523462 .2523462 [DOI] [PubMed] [Google Scholar]
- 21.DeSouza SI, Rashmi MR, Vasanthi AP, Joseph SM, Rodrigues R. Mobile phones: the next step towards healthcare delivery in rural India? PLoS One. 2014;9(8):e104895. doi: 10.1371/journal.pone.0104895. https://journals.plos.org/plosone/article?id=10.1371/journal.pone.0104895 .PONE-D-14-01603 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Hoque MR, Bao Y, Sorwar G. Investigating factors influencing the adoption of e-Health in developing countries: a patient's perspective. Inform Health Soc Care. 2017;42(1):1–17. doi: 10.3109/17538157.2015.1075541. https://www.tandfonline.com/doi/abs/10.3109/17538157.2015.1075541?journalCode=imif20 . [DOI] [PubMed] [Google Scholar]
- 23.Horne M, Tierney S, Henderson S, Wearden A, Skelton DA. A systematic review of interventions to increase physical activity among South Asian adults. Public Health. 2018;162:71–81. doi: 10.1016/j.puhe.2018.05.009. https://www.sciencedirect.com/science/article/abs/pii/S0033350618301707?via%3Dihub .S0033-3506(18)30170-7 [DOI] [PubMed] [Google Scholar]
- 24.Hossain N, Yokota F, Sultana N, Ahmed A. Factors influencing rural end-users' acceptance of e-Health in developing countries: a study on portable health clinic in Bangladesh. Telemed J E Health. 2019;25(3):221–229. doi: 10.1089/tmj.2018.0039. https://www.liebertpub.com/doi/10.1089/tmj.2018.0039 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Hyman A, Stacy E, Mohsin H, Atkinson K, Stewart K, Lauscher HN, Ho K. Barriers and facilitators to accessing digital health tools faced by South Asian Canadians in Surrey, British Columbia: community-based participatory action exploration using photovoice. J Med Internet Res. 2022;24(1):e25863. doi: 10.2196/25863. https://www.jmir.org/2022/1/e25863 .v24i1e25863 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Kumar AA, De Costa A, Das A, Srinivasa GA, D'Souza G, Rodrigues R. Mobile health for tuberculosis management in South India: is video-based directly observed treatment an acceptable alternative? JMIR Mhealth Uhealth. 2019;7(4):e11687. doi: 10.2196/11687. https://mhealth.jmir.org/2019/4/e11687/ v7i4e11687 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Makowsky MJ, Jones CA, Davachi S. Prevalence and predictors of health-related internet and digital device use in a sample of South Asian adults in Edmonton, Alberta, Canada: results from a 2014 community-based survey. JMIR Public Health Surveill. 2021;7(1):e20671. doi: 10.2196/20671. https://publichealth.jmir.org/2021/1/e20671 .v7i1e20671 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Prinjha S, Ricci-Cabello I, Newhouse N, Farmer A. British South Asian patients' perspectives on the relevance and acceptability of mobile health text messaging to support medication adherence for type 2 diabetes: qualitative study. JMIR Mhealth Uhealth. 2020;8(4):e15789. doi: 10.2196/15789. https://mhealth.jmir.org/2020/4/e15789/ v8i4e15789 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Quaosar GMAA, Hoque MR, Bao Y. Investigating factors affecting elderly's intention to use m-Health services: an empirical study. Telemed J E Health. 2018;24(4):309–314. doi: 10.1089/tmj.2017.0111. https://www.liebertpub.com/doi/10.1089/tmj.2017.0111 . [DOI] [PubMed] [Google Scholar]
- 30.Ramachandran N, Srinivasan M, Thekkur P, Johnson P, Chinnakali P, Naik BN. Mobile phone usage and willingness to receive health-related information among patients attending a chronic disease clinic in rural Puducherry, India. J Diabetes Sci Technol. 2015;9(6):1350–1351. doi: 10.1177/1932296815599005. https://journals.sagepub.com/doi/10.1177/1932296815599005 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Teo CL, Chee ML, Koh KH, Tseng RMWW, Majithia S, Thakur S, Gunasekeran DV, Nusinovici S, Sabanayagam C, Wong TY, Tham Y-C, Cheng C-Y. COVID-19 awareness, knowledge and perception towards digital health in an urban multi-ethnic Asian population. Sci Rep. 2021;11(1):10795. doi: 10.1038/s41598-021-90098-6. https://www.nature.com/articles/s41598-021-90098-6 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Vyas AN, Chaudhary N, Ramiah K, Landry M. Addressing a growing community‘s health needs: project SAHNA (South Asian Health Needs Assessment) J Immigr Minor Health. 2012;15(3):577–583. doi: 10.1007/s10903-012-9655-x. https://link.springer.com/article/10.1007/s10903-012-9655-x . [DOI] [PubMed] [Google Scholar]
- 33.Yasmin F, Ali L, Banu B, Rasul FB, Sauerborn R, Souares A. Understanding patients’ experience living with diabetes type 2 and effective disease management: a qualitative study following a mobile health intervention in Bangladesh. BMC Health Serv Res. 2020;20(1):29. doi: 10.1186/s12913-019-4811-9. https://bmchealthservres.biomedcentral.com/articles/10.1186/s12913-019-4811-9 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Zibrik L, Khan S, Bangar N, Stacy E, Lauscher HN, Ho K. Patient and community centered eHealth: exploring eHealth barriers and facilitators for chronic disease self-management within British Columbia’s immigrant Chinese and Punjabi seniors. Health Policy Technol. 2015;4(4):348–356. doi: 10.1016/j.hlpt.2015.08.002. https://www.sciencedirect.com/science/article/abs/pii/S221188371500060X . [DOI] [Google Scholar]
- 35.Braun V, Clarke V. Using thematic analysis in psychology. Qual Res Psychol. 2006;3(2):77–101. doi: 10.1191/1478088706qp063oa. https://www.tandfonline.com/doi/abs/10.1191/1478088706QP063OA . [DOI] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Full details of the included papers.
Data Availability Statement
Full details of the included papers are submitted in Multimedia Appendix 1.