

Abstract
Background
Testicular sperm extraction (TESE) is an essential therapeutic tool for the management of male infertility. However, it is an invasive procedure with a success rate up to 50%. To date, no model based on clinical and laboratory parameters is sufficiently powerful to accurately predict the success of sperm retrieval in TESE.
Objective
The aim of this study is to compare a wide range of predictive models under similar conditions for TESE outcomes in patients with nonobstructive azoospermia (NOA) to identify the correct mathematical approach to apply, most appropriate study size, and relevance of the input biomarkers.
Methods
We analyzed 201 patients who underwent TESE at Tenon Hospital (Assistance Publique-Hôpitaux de Paris, Sorbonne University, Paris), distributed in a retrospective training cohort of 175 patients (January 2012 to April 2021) and a prospective testing cohort (May 2021 to December 2021) of 26 patients. Preoperative data (according to the French standard exploration of male infertility, 16 variables) including urogenital history, hormonal data, genetic data, and TESE outcomes (representing the target variable) were collected. A TESE was considered positive if we obtained sufficient spermatozoa for intracytoplasmic sperm injection. After preprocessing the raw data, 8 machine learning (ML) models were trained and optimized on the retrospective training cohort data set: The hyperparameter tuning was performed by random search. Finally, the prospective testing cohort data set was used for the model evaluation. The metrics used to evaluate and compare the models were the following: sensitivity, specificity, area under the receiver operating characteristic curve (AUC-ROC), and accuracy. The importance of each variable in the model was assessed using the permutation feature importance technique, and the optimal number of patients to include in the study was assessed using the learning curve.
Results
The ensemble models, based on decision trees, showed the best performance, especially the random forest model, which yielded the following results: AUC=0.90, sensitivity=100%, and specificity=69.2%. Furthermore, a study size of 120 patients seemed sufficient to properly exploit the preoperative data in the modeling process, since increasing the number of patients beyond 120 during model training did not bring any performance improvement. Furthermore, inhibin B and a history of varicoceles exhibited the highest predictive capacity.
Conclusions
An ML algorithm based on an appropriate approach can predict successful sperm retrieval in men with NOA undergoing TESE, with promising performance. However, although this study is consistent with the first step of this process, a subsequent formal prospective multicentric validation study should be undertaken before any clinical applications. As future work, we consider the use of recent and clinically relevant data sets (including seminal plasma biomarkers, especially noncoding RNAs, as markers of residual spermatogenesis in NOA patients) to improve our results even more.
Keywords: machine learning, azoospermia, prediction model, biomedical informatics, model, predict, sperm, men's health, infertility, infertile
Introduction
In the context of azoospermia, testicular sperm extraction (TESE) can be proposed to obtain mature germ cells (ie, spermatozoa) for in vitro fertilization with intracytoplasmic sperm injection (ICSI) [1-3]. Several surgical techniques are available for this, including conventional surgical TESE (cTESE) and microsurgical TESE (microTESE), the latter of which requires the use of an operating microscope to visualize the seminiferous tubules that are most likely to contain complete spermatogenesis [4]. However, both of these are invasive procedures and are, thus far, not exempt from complications such as hematoma, infection, vascular damage, and testosterone deficiency [4]. Thus, TESE must be proposed after a couple’s complete infertility checkup and information session as well as following a multidisciplinary discussion. Finally, spermatozoa can be retrieved from testicular tissue in only about 50% of cases [5,6].
Some teams have aimed to identify the most predictive factors of a positive TESE, first using univariate models, followed by multivariate models and, finally, artificial intelligence, including machine learning (ML) models [7]. We conducted a scoping review on the prediction of TESE success, extended to relevant citations on PubMed (MeSH terms: TESE; prediction; non-obstructive azoospermia; machine learning; sperm). A combination of search terms and Boolean operators (such as OR, AND) were used as appropriate to broaden the search and retrieve all relevant papers.
Among the clinical and hormonal variables in a preoperative assessment, age, BMI, total testosterone, and prolactin levels seem insufficiently predictive of the presence of spermatozoa in testicular tissue [8-13], while small testicular volume [14-17]; high follicle-stimulating hormone (FSH) [18]; and low inhibin B, reflecting impaired testicular function, are generally accompanied by a lower probability of successful TESE [19-22]. In addition, abnormal karyotype and microdeletion in the azoospermia factor (AZF) region are found in 6% to 18% of patients with azoospermia [23-26]. Except for complete AZFa and AZFb mutations, which are systematically associated with an absence of complete spermatogenesis, genetic results are insufficient predictors of TESE outcomes [26]. Finally, a history of cryptorchidism and smoking status have shown inconsistent results [27-29]. Consequently, separately, none of these predictors has so far shown satisfactory, sufficient, and reproducible predictive performance to guide practitioners regarding the probability of TESE success and the evaluation of the benefit-risk balance [7,14,30-33]. In addition, this surgery involves a substantial cost for some patients.
ML techniques allow for predictions based on the integration of a large amount of data due to an increase in computing power. We previously reported the relevance of mathematical modeling and ML approaches [34,35]. Concerning TESE, different models were developed with conventional clinical and biological data from the preoperative checkup. Mostly, the models developed were logistic regression (LR) or artificial neural network (ANN) models. For instance, Tsujimura et al [36] developed an LR using 100 patients and an area under the curve (AUC) of 0.83. Notwithstanding the use of a larger cohort of more than 1000 patients, the LR model from Cissen et al [37] achieved an AUC of only 0.65. Furthermore, the ANN model that Ramasamy et al [38] used yielded even poorer performance, with an AUC of 0.59. Finally, Zeadna et al [39] developed a more complex ensemble model based on decision trees (XGBoost [XGB]), which exhibited a sensitivity of over 90% but a very low specificity (51%).
Nevertheless, these studies applied different approaches and used various sample sizes, making it difficult to compare them and establish the correct mathematical methodology.
As it is challenging to determine which mathematical approach and, thus, which type of ML model will be the most appropriate and effective, an extensive search of the most common models is essential to avoid model selection bias. Similarly, the number of patients needed to obtain a successful model is mostly empirical and depends on the problem and type of data made available.
Therefore, the aim of this study was to develop, evaluate, and compare a wide range of predictive models under similar conditions for TESE outcomes in patients with nonobstructive azoospermia (NOA) to identify the correct mathematical approach to apply thereto, as well as the most appropriate study size. To our knowledge, our study is the first intermethodology comparative study in this field, as well as the first to assess the requisite sample size.
Methods
Description of the Patients
Data from 201 patients who underwent TESE (cTESE or microTESE) between January 2012 and December 2021 at Tenon Hospital (Assistance Publique-Hôpitaux de Paris, Sorbonne University, Paris) were collected. All included patients presented with NOA, which is defined as the absence of spermatozoa in the semen in at least two collections at least three months apart (2010 World Health Organization criteria for semen analysis) [40]. Patients with NOA following radiotherapy or with hypogonadotropic hypogonadism were excluded from the study.
Surgical Procedure
The surgical procedure was systematically performed under general anesthesia. After the scrototomy and opening of the tunica vaginalis, the albuginea was incised. The testicular pulp was then expressed and dissected (cTESE: 136/201, 67.7%). In some cases, the dissection of testicular tissue was done under a surgical microscope to better locate the seminiferous tubules that most likely contain sperm (microTESE: 65/201, 32.3%). Fragments could be taken bilaterally (from both testicles) or unilaterally at the upper, middle, and lower pole of each testicle, sparing the rete testis area. One sample was systematically collected to send it for anatomopathology. Once collected, the testicular fragments were transported in a culture medium (Ferticult Hepes) to the laboratory. The testicular fragments were then prepared using mechanical methods and observed under optical microscopy for the spermatozoon search [40].
Study Overview
In the first step, preoperative data including urogenital history, hormonal data, genetic data, and TESE outcomes (representing the target variable) were collected from patients’ medical records, including management software and paper records (patients in the retrospective training cohort: 175/201, 87.1%; patients in the prospective testing cohort: 26/201, 12.9%). This data collection was driven by the potentially relevant predictors identified from the literature and expert recommendations regarding evaluation of male infertility [6,41,42]. In the second step, raw data were preprocessed (eg, imputation of missing values, encoding [eg, turning qualitative variable into numbers], and scaling [eg, transforming quantitative variable when they were on a different scale]) to transform them into a format suitable for the ML models. Once these data were preprocessed, 8 ML and deep learning (DL) models were trained and selected using the retrospective training cohort data in the third step. Finally, in the 4th and last step, data from the prospective training cohort were used to evaluate the models (temporal validation) and allow for comparison using the prospective test set from patients the models had never seen. The results from the test set give a good indication of how the model should perform in the real world (Figure 1).
Figure 1.
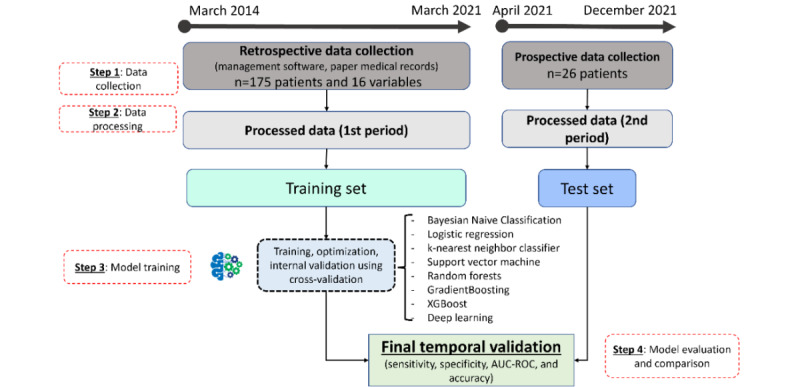
Summary workflow from data collection to final model evaluation. AUC-ROC: area under the receiver operating characteristic curve.
Data Set
Description of the Variables
The input data corresponded with the French standard exploration of male infertility and the TESE preoperative assessment [6]. Among the 16 included variables, 7 were quantitative, and 9 were qualitative or categorical. The variables were age, BMI, tobacco consumption, hormonal assessment (FSH, luteinizing hormone [LH], testosterone, inhibin B, and prolactin), genetic exploration (karyotype and search for Y-chromosome microdeletion), and urogenital history (cryptorchidism, infection, trauma, gonadotoxic therapy, urogenital surgery, and varicoceles), for a total of 16 variables.
Description of the Target
The outcome was the presence (y=1) or absence (y=0) of spermatozoa after examination of the surgical specimens. A TESE was considered positive when we obtained enough spermatozoa for the ICSI procedure.
Statistical Analysis
Prior to the modeling process, exploratory analysis of the data was conducted to quantify missing data and analyze the variables’ distributions. Correlations and mean comparisons were also performed. Regarding the statistics, the qualitative variables are reported as percentages, and the quantitative variables are reported as medians (IQRs). We used the Mann-Whitney test for quantitative variables (among the quantitative variables, none was normally distributed [Shapiro-Wilk]) and χ2 for qualitative variables. For correlations, the Pearson coefficient was used. A P value of <.05 was considered significant.
Preprocessing and Modeling
Our main objective was to train a classification model to classify a new patient as presenting with either an “absence of sperm” or “presence of sperm” during TESE based on the patient’s variables. After processing the raw data (eg, handling missing data, management of categorical or qualitative variables, standardization), many different models (n=8) were trained, optimized, and evaluated. ML models (Bayesian naive classification, LR, k-nearest neighbor classifier, support vector machine [SVM], random forest [RF], gradient-boosted tree [GBT], and XGB) and DL models using several neural network architectures were also tested. The optimization and fine-tuning of the hyperparameters were performed using a cross-validation random search technique on each split of the training set: Each hyperparameter was sampled from a distribution of possible parameter values. The highest performing hyperparameter combination was used for each model [43].
The Validation and Evaluation Procedure
The data set (patient cohort) was distributed into a training set for training, during which hyperparameters were set and models were selected (internal validation, repeated 5-fold cross-validation [10 iterations]), and a separate test set, during which a final evaluation of patients that the models had never seen (external validation) was conducted. The external validation consisted of testing the models’ ability to classify or correctly predict the patients of the test cohort. Both sets came from the same institution, but the patients’ data were collected at separate periods. In a monocentric study, splitting by time and developing a model using data from one period and evaluating its performance using the data from the other period (temporal validation) is a stronger approach, as indicated by the “Transparent reporting of a multivariable prediction model for individual prognosis or diagnosis” (TRIPOD) Statement [44].
The following several classification metrics were used to evaluate the models and compare them objectively: sensitivity, specificity, area under the receiver operating characteristic curve (AUC-ROC), and accuracy. Moreover, as a binary classification task, the thresholds for both ML and deep learning models were maintained at 50%. For example, a TESE was classified as positive when the probability of success was greater than 50% and negative when the probability was less than 50%. Finally, the following 2 additional factors were considered when evaluating the models: importance of each variable in the model and optimal number of patients to include in the study. The importance of each variable in the models was determined using the permutation technique: Permutation feature importance (PFE) consists of comparing the performances of the model with and without the variable under evaluation [45]. PFE generates an ordered list of variables along with their importance values. Interpreting the output of this algorithm is straightforward: Variables ranked higher have more impact on the model predictions. Identifying relevant variables is also useful for the model’s explainability. For the optimal number of patients, we used the learning curve, which is a graphical representation of the relationship between the model’s performance (measured on the vertical axis) and the number of patients used for training (measured on the horizontal axis). A learning curve allows for visually evaluating the evolution of the model’s performance as new patients are included. The shape of this learning curve (plateau or rising slope) provides information on the number of patients needed to obtain good performance and discern whether it is necessary to include new patients.
Computer Tools
The whole project was realized exclusively with the Python 3.8 programming language and several libraries: NumPy 1.20.3 and Pandas 1.2.4 for data table management and matrix calculation, SciPy 1.7.0 and Pingouin 0.3.12 for statistics, and Sklearn 0.24.2 and TensorFlow 2.5.0 for modeling [46-50]. The code to build and train the model is openly available on github [51].
Ethical Considerations
The local ethics committee “Comité d’Éthique de la Recherche, Sorbonne Université” (CER@SU) approved this study under protocol number CER-2021-041, and this study had no external source of funding.
Results
Exploratory Data Analysis
The clinical characteristics of the patients included in the study are shown in Table 1. All the variables from the preoperative assessment were included, with missing data in the training cohort ranging from 5.7% (10/175) to 57.7% (101/175) for varicocele and prolactin, respectively. No missing data were reported in the test cohort. Within the training set (n=175), enough spermatozoa for the ICSI procedure were found in the testicular tissue of 104 (59.4%) patients (positive TESE), while the TESE was negative in the 71 (40.6%) remaining patients. Within the test set, the distribution between the classes was equal. The following 3 variables were significantly different between the 2 groups: FSH, LH, and inhibin B levels (Table 1). In addition, in the training set, several quantitative variables were significantly correlated: FSH and inhibin B (r=−0.637; P<.001), LH and inhibin B (r=−0.454; P<.001), LH and testosterone (r=−0.194; P=.03), age and LH (r=−0.186; P=.04), FSH and total testosterone (r=−0.176; P=.04), age and inhibin B (r=0.222; P=.04), and FSH and LH (r=0.852; P<.001).
Table 1.
Baseline characteristics of patients in the training and test sets.
| Variable | Presence of spermatozoa (n=104) | Absence of spermatozoa (n=71) | P value | |||||||
| Training set (n=175) | ||||||||||
|
|
Clinical | |||||||||
|
|
|
Agea (years), median (IQR) | 38.11 (9.56) | 36.89 (5.40) | .16 | |||||
|
|
|
BMIb (kg/m2), median (IQR) | 25.41 (4.99) | 25.11 (3.65) | .87 | |||||
|
|
|
Smokingc (yes), n (%) | 27d (28.7) | 19e (30.2) | .99 | |||||
|
|
Hormonal | |||||||||
|
|
|
FSHf,g (UI/L), median (IQR) | 9.90 (14.10) | 23.50 (23.03) | <.001 | |||||
|
|
|
LHh,i (UI/L), median (IQR) | 6.37 (5.49) | 11.90 (12.80) | <.001 | |||||
|
|
|
Testosteronei (ng/mL), median (IQR) | 4.50 (2.76) | 4.00 (3.05) | .28 | |||||
|
|
|
Inhibin Bj (pg/mL), median (IQR) | 60.00 (94.00) | 14.00 (28.25) | <.001 | |||||
|
|
|
Prolactink (ng/mL), median (IQR) | 12.00 (5.58) | 11.85 (8.08) | .94 | |||||
|
|
Genetics | |||||||||
|
|
|
Normal karyotypel, n (%) | 9m (10.3) | 6n (9.4) | >.99 | |||||
|
|
|
Y microdeletiono, n (%) | 2p (2.1) | 3n (4.7) | .61 | |||||
|
|
Medical history | |||||||||
|
|
|
Cryptorchidismq, n (%) | 20r (20.4) | 11s (16.4) | .66 | |||||
|
|
|
Infectiont, n (%) | 11u (11.3) | 3v (4.6) | .23 | |||||
|
|
|
Traumaw, n (%) | 2u (2.1) | 1x (1.5) | >.99 | |||||
|
|
|
Gonadotoxic therapyw, n (%) | 8r (8.2) | 7v (10.8) | .77 | |||||
|
|
|
Urogenital surgeryt, n (%) | 11u (11.3) | 6v (9.2) | .87 | |||||
|
|
|
Varicoceleq, n (%) | 14y (14.1) | 15x (22.7) | .23 | |||||
| Test set (n=26) | ||||||||||
|
|
Clinical | |||||||||
|
|
|
Age (years), median (IQR) | 40.83 (6.50) | 36.62 (4.75) | .09 | |||||
|
|
BMI (kg/m2), median (IQR) | 25.95 (3.72) | 29.12 (6.42) | .25 | ||||||
|
|
Smoking (yes), n (%) | 3z (23.1) | 5z (38.5) | >.99 | ||||||
|
|
Hormonal | |||||||||
|
|
|
FSH (UI/L), median (IQR) | 8.59 (5.58) | 25.78 (9.76) | <.001 | |||||
|
|
LH (UI/L), median (IQR) | 6.67 (3.69) | 10.88 (4.42) | .02 | ||||||
|
|
Testosterone (ng/mL), median (IQR) | 4.30 (3.37) | 4.45 (2.85) | .45 | ||||||
|
|
Inhibin B (pg/mL), median (IQR) | 109.00 (92.10) | 20.00 (18.00) | <.001 | ||||||
|
|
Prolactin (ng/mL), median (IQR) | 10.00 (3.38) | 8.00 (3.60) | .98 | ||||||
|
|
Genetics | |||||||||
|
|
|
Normal karyotype, n (%) | 1z (7.7) | 1z (7.7) | .99 | |||||
|
|
|
Y microdeletion, n (%) | 1z (7.7) | 0z (0) | .99 | |||||
|
|
Medical history | |||||||||
|
|
|
Cryptorchidism, n (%) | 3z (23.1) | 1z (7.7) | .59 | |||||
|
|
|
Infection, n (%) | 0z (0) | 1z (7.7) | .98 | |||||
|
|
|
Trauma, n (%) | 0z (0) | 0z (0) | .99 | |||||
|
|
|
Gonadotoxic therapy, n (%) | 0z (0) | 0z (0) | .99 | |||||
|
|
|
Urogenital surgery, n (%) | 0z (0) | 0z (0) | .99 | |||||
|
|
|
Varicocele, n (%) | 2z (15.4) | 1z (7.7) | .97 | |||||
a25 (14.3%) missing values.
b43 (25.7%) missing values.
c18 (10.3%) missing values.
dN=94.
eN=63.
fFSH: follicle-stimulating hormone.
g17 (9.7%) missing values.
hLH: luteinizing hormone.
i37 (21.1%) missing values.
j74 (42.3%) missing values.
k101 (57.7%) missing values.
l14 (8%) missing values.
mN=87.
nN=64.
o15 (8.6%) missing values.
pN=96.
q10 (5.7%) missing values.
rN=98.
sN=67.
t13 (7.4%) missing values.
uN=97.
vN=65.
w12 (6.9%) missing values.
xN=66.
yN=99.
zN=13.
The Valuation Procedure and Cohort Splitting
Both cohorts (training and test sets) were from the same institution, and patients were managed in a similar manner. A retrospective cohort of 175 patients was first used for model building. Following this first step of the study, a prospective collection of data of patients undergoing TESE in the institution was conducted. This second temporal test cohort, consisting of prospectively collected data from May 2021 to December 2021, served to independently evaluate the performance of the models. Moreover, the prospective data collection allowed the inclusion of only “complete” patients’ TESE preoperative assessments, resulting in no missing values for this temporal test cohort. The distribution between classes of 1/0 (positive/negative) was 104/71 in the training set and 13/13 in the test set. Further, the characteristics (variables) of the patients were not significantly different between the 2 cohorts (training and test).
Performance of the Tested Models
Table 2 reports the internal and external validation results for the different models: The ensemble models based on decision trees (RF and GBT) showed the best performance. Additionally, the DL models were less efficient than the more classical ML models, especially in the test cohort. The highest performing hyperparameter combination for each model is reported in Table S1 in Multimedia Appendix 1.
Table 2.
Internal and external performances of the 8 different trained models.
| Model | Internal validation (cross validation), mean (SD) | External temporal validation | |||||||
|
|
AUC-ROCa | Accuracy (%) | Sensitivity (%) | Specificity (%) | AUC-ROC | Accuracy (%) | Sensitivity (%) | Specificity (%) | |
| LRb | 0.670 (0.097) | 66.4 (7.1) | 76.3 (10.1) | 53.7 (9) | 0.85 | 69.2 | 76.9 | 61.5 | |
| BNCc | 0.624 (0.092) | 62.1 (7.5) | 66.3 (11.5) | 55.9 (11.3) | 0.83 | 69.2 | 69.2 | 69.2 | |
| RFd | 0.780 (0.084) | 74.7 (7.3) | 85.2 (7.1) | 61 (11.5) | 0.90 | 84.6 | 100.0 | 69.2 | |
| GBTe | 0.765 (0.092) | 73.5 (6.9) | 82.2 (7.8) | 62.4 (10.8) | 0.82 | 76.9 | 92.3 | 61.5 | |
| XGBf | 0.760 (0.087) | 72.2 (7.1) | 80.2 (7.8) | 62.1 (9.9) | 0.82 | 80.8 | 92.3 | 69.2 | |
| SVMg | 0.723 (0.094) | 67.6 (8.3) | 81.8 (9.8) | 49.1 (13.6) | 0.72 | 61.5 | 84.6 | 38.5 | |
| KNNh | 0.669 (0.089) | 63.8 (6.1) | 76.2 (9) | 48.3 (11.1) | 0.76 | 69.2 | 84.6 | 53.8 | |
| ANNi (64x32) | 0.690 (0.085) | 66.7 (7) | 77 (8.6) | 55.4 (10.9) | 0.65 | 65.0 | 54.0 | 77.0 | |
aAUC-ROC: area under the receiver operating characteristic curve.
bLR: logistic regression.
cBNC: Bayesian naive classification.
dRF: random forest.
eGBT: gradient-boosted tree.
fXGB: XGBoost.
gSVM: support vector machine.
hKNN: k-nearest neighbor.
iANN: artificial neural network.
Top Model, Biomarker Ranking, and Sample Size Requirements
The most efficient model was the RF model. The RF model showed the best performance in the test cohort, with an AUC of 0.90, a sensitivity of 100%, and a specificity of 69.2%. Notably, the performances in the test cohort were better each time than during cross-validation in the training cohort. The RF model is an ensemble model (ie, it combines several models). For the RF model, the most discriminating variable (mean 26.6%, SD 2.5%) was serum inhibin B concentration (Figure 2). In addition, serum prolactin concentration (mean 3.1%, SD 1.1%), patient age (mean 3.2%, SD 0.8%), and the presence of a history of varicoceles (whatever the grade; mean, 2.3%, SD 0.4%) also seemed to be important in discriminating between the 2 groups.
Figure 2.
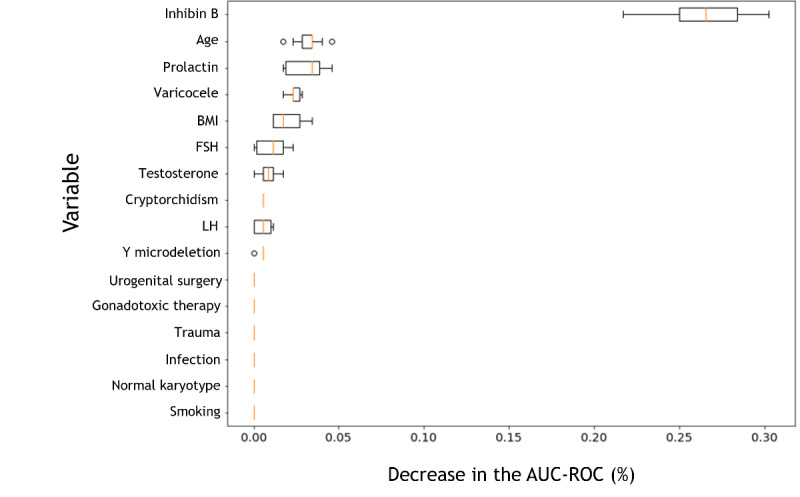
The importance of each variable in the random forest (RF) model using permutation feature importance (PFE), which generates an ordered list of variables along with their importance values: Variables with higher ranks have more impact on the model predictions. AUC-ROC: area under the receiver operating characteristic curve; FSH: follicle-stimulating hormone; LH: luteinizing hormone.
Despite a lower reliability of the analysis, given the weaker performance of the 6 other models tested, the importance of the variables was also determined for 6 models (see Table S2 in Multimedia Appendix 2). These outputs were not available for neural networks (due to their black box appearance). Briefly, as shown in Table S2 in Multimedia Appendix 2, for the 2 decision tree models (XGB and GBT), which are similar to the RF model, the discriminant variables were comparable to those observed for the RF model (including serum inhibin and prolactin concentrations). In contrast, for linear models (such as SVM and LR), additional variables such as FSH concentration, smoking, and the presence of genetic abnormalities (Y microdeletion and abnormal karyotype) appeared to be also stratifying. However, the interpretation of the ranking results of these latter models should be interpreted with caution, insofar as such variable combinations did not produce efficient models.
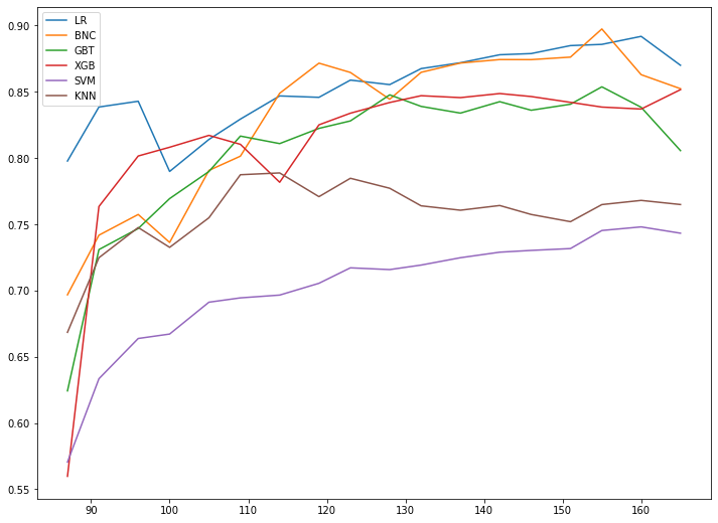
The performance of the RF model increased to a plateau at around 120 patients (Figure 3). Beyond this number of patients used to train the model, increasing the number of patients did not bring any performance gain. Indeed, beyond this threshold, the inclusion of additional patients did not allow for any increase in performance. These findings are similar for the other models evaluated: indeed, the learning curves also reached a plateau after 120 patients, showing the limitation of their performance despite the increase in the amount of data (see Multimedia Appendix 3). However, these results should be interpreted carefully, considering the poor relevance and performance of these models.
Figure 3.
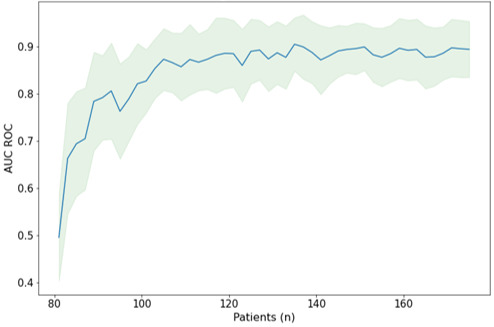
Learning curve for the random forest model, showing the graphical representation of the relationship between model performance (area under the receiver operating characteristic curve [AUC ROC]) and the number of patients used for training.
Discussion
Overview
We aimed to develop and evaluate predictive models of TESE outcomes in patients with NOA using ML methods and integrating retrospective data from the preoperative assessment. To our knowledge, this study was the first to compare several methodologies under the same conditions with the aim of determining the correct mathematical approach to apply and the most appropriate study size. TESE is an essential therapeutic tool for the management of male infertility and is often the “last hope” before gamete donation for these patients, but it is an invasive procedure. Consequently, it is essential to have a decision tool that could help the surgeon to decide whether this invasive procedure is the best option for the patient.
Best Mathematical Approach to Apply and Best Sample Size to Use
Heterogeneity in the methodology and sample sizes in previous studies was the main obstacle to determining the correct mathematical approach to apply and the proper number of patients to include. In our study, the application of various approaches to the same cohort of patients allowed for an unbiased comparison. Regarding the different models investigated, the best results were provided by decision tree–based ensemble models, especially the RF model. Zeadna et al [39], who used the GBT and XGB models, which are close to the RF model, also found interesting results. Linear models such as LR or Bayesian models performed less well and produced results close to those of Tsujimura et al [36] and Cissen et al [37]. Despite more recent developments in artificial intelligence and more sophisticated technology, the neural network–based DL models yielded poor results that were below those of more traditional or classical methods. This could have been because data from the preoperative assessment used as input were inappropriate or because neural networks are classically used to process less structured, complex, and larger sized data such as sound signals or images (computer vision) or text (natural language processing). Overall, nonlinear methods such as decision trees and related methods (particularly the RF model) seem to be the most appropriate approach to predict TESE success. Beyond the raw performance of the models, the main strength of this study was its comparison of many models under identical conditions: similar patients and a similar sampling strategy. On the other hand, 120 patients seemed to be enough to properly exploit the preoperative data during the modeling process.
The Relevance of Input Biomarkers
The most relevant variables in the previous models described in the literature were somewhat heterogeneous; for example, hormonal parameters (eg, LH, FSH) were powerful in the LR used by Cissen et al [37], while semen volume and ethnicity surprisingly appeared to be significant in the GBT used by Zeadna et al [39]. PFE measures the predictive value of a feature by evaluating how the prediction error increases when a variable is not available. PFE is a global explanation method that provides insights into an ML model’s behavior. It estimates and ranks feature importance based on the impact each variable has on the trained ML model’s predictions. In our study, and using the RF model, the most discriminating variable was the serum inhibin B level. Inhibin B is a hormone produced by Sertoli cells and is directly correlated with spermatogenesis. This hormone is a relevant variable in patients with and without spermatozoa [52]. Moreover, albeit with no significant difference between the groups, prolactin did indeed negatively impact sperm production [53], and therefore, its contribution to the discriminative power of the model seems meaningful. Unfortunately, due to missing data, we could not demonstrate the discriminative contribution of prolactin levels. Finally, the presence of a history of varicoceles, which is characterized by the dilation of a vein in the spermatic cord and is frequently found in infertile men, also seemed to be important in discriminating patients with positive TESEs from those with negative TESEs. Despite the good performance of the RF, the true classification power of conventional preoperative assessment can be challenged to explain the results of TESE. Moreover, the preoperative data were chosen for their accessibility and availability for incorporation into the patient’s therapeutic management. The selection of these data brings up other more general discussion points. For example, the available preoperative data may not have been sufficient to characterize the phenomenon that makes a TESE positive or not. Consequently, other variables or innovative biomarkers, such as genetic, proteomic, lifestyle, and environmental data, could be considered for further investigation. In the future, the integration of new biomarkers could allow for the construction of more efficient models [54]. These include serum 17-hydroxyprogesterone concentration, which appears to be an interesting marker of intratesticular testosterone [55]. More specifically, biomarkers in seminal plasma may be of interest. Thus, the integration of seminal inhibin B and seminal antiMüllerian hormone into an LR model could allow for the better prediction of the outcome of TESE [56]. Moreover, small noncoding RNA are increasingly being studied, and their variation in seminal plasma could encourage new diagnostic perspectives. For instance, Fang et al [57] observed different miRNA profiles in the seminal plasma of men with positive or negative TESEs. Likewise, Xie et al [58] were interested in the predictive characteristics of extracellular vesicle long noncoding RNA in seminal plasma. Finally, Ji et al [59] recently highlighted the value of circRNA for the same purpose.
Limitations and Routine Usage of the Predictive Model
Two limitations of the study are worth mentioning: its monocentric design and the use of 2 surgical procedures, namely cTESE and microTESE. Despite the monocentric design, the work was carried out in 2 periods: first, model building with retrospective data from patients undergoing TESE until June 2021. This modeling process highlighted the challenge of collecting retrospective data and promoted the initiation of a prospective collection of patients managed from that date onwards. Following several months of data collection (until December 2021), a prospective testing cohort was therefore used to objectively evaluate the performance of the models. One perspective for the future should be to keep going in this way, including new patients over time and incorporating them into the model, in order to refine the performance of the models through time. The target could also have been a limitation, as its results were variable. Indeed, the target may depend on the surgeon, surgical technique used, site of the biopsy, and presence of focal spermatogenesis that may vary according to the tissue heterogeneity of the testis [60]. This heterogeneous distribution of seminiferous tubules, making the result dependent on the skill and experience of the surgeon, can eventually lead to errors in patient labeling, which can be detrimental to building ML models. Furthermore, the development of the microTESE technique, with its seminiferous tube visualization step, may certainly reduce this variability and make the biopsy results more reproducible.
Despite these limitations, the RF model showed excellent performance and seemed to be the most appropriate modeling approach. Additionally, 120 patients seemed adequate as a study population to train and validate this model. A diagnostic tool with perfect performance would be difficult to obtain, so a model with an AUC of nearly than 90% and an excellent sensitivity would probably be suitable as an additional tool for the management of men presenting with azoospermia. It would, therefore, be necessary to confirm these results and improve the performance of the model in a prospective multicenter design study, for sufficient robustness.
Conclusions
ML models can provide the basis for an enhanced decision support system tool in the context of azoospermia, as they give additional and more relevant information than each variable taken separately. Nevertheless, many innovative AI models were tested, but none can determine TESE results with absolute certainty. However, we report promising results with decision tree–based ensemble models, and these require multicentric validation prior to any clinical use. It would, therefore, be interesting to improve the model, and several ways for improvement should be considered. Indefinitely increasing the number of participants and testing other DL models do not seem to be the most effective solutions. Integrating additional innovative biomarkers into the models may be necessary to improve the model’s performance. For example, biomarkers in seminal plasma may be of interest, as well as small noncoding RNA, which are increasingly being studied and whose variation in seminal plasma could encourage new diagnostic perspectives.
Abbreviations
- ANN
artificial neural network
- AUC
area under the curve
- AZF
azoospermia factor
- cTESE
conventional surgical testicular sperm extraction
- DL
deep learning
- FSH
follicle-stimulating hormone
- GBT
gradient-boosted tree
- ICSI
intracytoplasmic sperm injection
- LH
luteinizing hormone
- LR
logistic regression
- microTESE
microsurgical testicular sperm extraction
- ML
machine learning
- NOA
nonobstructive azoospermia
- PFE
permutation feature importance
- RF
random forest
- ROC
receiver operating characteristic
- SVM
support vector machine
- TESE
testicular sperm extraction
- TRIPOD
Transparent reporting of a multivariable prediction model for individual prognosis or diagnosis
Most performing hyperparameter combination for each model.
The importance of each variable in the LR, BNC, RF, GBT, XGB, SVM, and KNN models model using permutation feature importance (PFE).
Learning curve for the logistic regression (LR), Bayesian naive classification (BNC), gradient-boosted tree (GBT), XGBoost (XGB), support vector machine (SVM), and k-nearest neighbor (KNN) models: graphical representation of the relationship between model performance (measured on the vertical axis (mean area under the curve [AUC]) and the number of patients used for training (on the horizontal axis).
{kind=link}
Data Availability
The data sets generated during and/or analyzed during the current study are available from the corresponding author upon reasonable request.
Footnotes
Authors' Contributions: GB performed the statistical analysis, drafted the manuscript, participated in the study conception and design, and interpreted the data. NS participated in study conception and design, interpretation of the data, and drafting the manuscript. RHH participated in acquisition of data, interpretation of data, and drafting the manuscript. FD, IB, VF, MP, KK, LS, EM-D, DR-D, and RL participated in acquisition of data, patient care, and critical revision of the manuscript for intellectual content. AL supervised the study, participated in study conception and design, and contributed to critical revision of the manuscript for intellectual content. CD supervised the study, participated in study conception and design, interpretation of the data, and drafting the manuscript.
Conflicts of Interest: None declared.
References
- 1.Ramasamy R, Schlegel PN. Microdissection testicular sperm extraction: effect of prior biopsy on success of sperm retrieval. J Urol. 2007 Apr;177(4):1447–9. doi: 10.1016/j.juro.2006.11.039.S0022-5347(06)03073-4 [DOI] [PubMed] [Google Scholar]
- 2.Robin G, Boitrelle F, Leroy X, Peers M, Marcelli F, Rigot J, Mitchell V. [Assessment of azoospermia and histological evaluation of spermatogenesis] Ann Pathol. 2010 Jun;30(3):182–95. doi: 10.1016/j.annpat.2010.03.015.S0242-6498(10)00082-9 [DOI] [PubMed] [Google Scholar]
- 3.Su LM, Palermo GD, Goldstein M, Veeck LL, Rosenwaks Z, Schlegel PN. Testicular sperm extraction with intracytoplasmic sperm injection for nonobstructive azoospermia: testicular histology can predict success of sperm retrieval. J Urol. 1999 Jan;161(1):112–6.S0022-5347(01)62079-2 [PubMed] [Google Scholar]
- 4.Bernie AM, Mata DA, Ramasamy R, Schlegel PN. Comparison of microdissection testicular sperm extraction, conventional testicular sperm extraction, and testicular sperm aspiration for nonobstructive azoospermia: a systematic review and meta-analysis. Fertil Steril. 2015 Nov;104(5):1099–103.e1. doi: 10.1016/j.fertnstert.2015.07.1136. https://linkinghub.elsevier.com/retrieve/pii/S0015-0282(15)01647-7 .S0015-0282(15)01647-7 [DOI] [PubMed] [Google Scholar]
- 5.Abdel Raheem A, Garaffa G, Rushwan N, De Luca F, Zacharakis E, Abdel Raheem T, Freeman A, Serhal P, Harper JC, Ralph D. Testicular histopathology as a predictor of a positive sperm retrieval in men with non-obstructive azoospermia. BJU Int. 2013 Mar;111(3):492–9. doi: 10.1111/j.1464-410X.2012.11203.x. [DOI] [PubMed] [Google Scholar]
- 6.Huyghe E, Boitrelle F, Methorst C, Mieusset R, Ray PF, Akakpo W, Koscinski I, Chalas C, Rives N, Plotton I, Robin G, El Osta R, Hennebicq S, Eustache F, Marcelli F, Lejeune H. [AFU and SALF recommendations for the evaluation of male infertility] Prog Urol. 2021 Mar;31(3):131–144. doi: 10.1016/j.purol.2020.09.011.S1166-7087(20)30587-X [DOI] [PubMed] [Google Scholar]
- 7.Qi L, Liu YP, Zhang NN, Su YC. Predictors of testicular sperm retrieval in patients with non-obstructive azoospermia: a review. J Int Med Res. 2021 Apr;49(4):3000605211002703. doi: 10.1177/03000605211002703. https://journals.sagepub.com/doi/10.1177/03000605211002703?url_ver=Z39.88-2003&rfr_id=ori:rid:crossref.org&rfr_dat=cr_pub0pubmed . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Gnessi L, Scarselli F, Minasi MG, Mariani S, Lubrano C, Basciani S, Greco PF, Watanabe M, Franco G, Farcomeni A, Greco E. Testicular histopathology, semen analysis and FSH, predictive value of sperm retrieval: supportive counseling in case of reoperation after testicular sperm extraction (TESE) BMC Urol. 2018 Jul 04;18(1):63. doi: 10.1186/s12894-018-0379-7. https://bmcurol.biomedcentral.com/articles/10.1186/s12894-018-0379-7 .10.1186/s12894-018-0379-7 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Bernie AM, Ramasamy R, Schlegel PN. Predictive factors of successful microdissection testicular sperm extraction. Basic Clin Androl. 2013;23:5. doi: 10.1186/2051-4190-23-5. https://bacandrology.biomedcentral.com/articles/10.1186/2051-4190-23-5 .4 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Althakafi SA, Mustafa OM, Seyam RM, Al-Hathal N, Kattan S. Serum testosterone levels and other determinants of sperm retrieval in microdissection testicular sperm extraction. Transl Androl Urol. 2017 Apr;6(2):282–287. doi: 10.21037/tau.2017.02.04. https://europepmc.org/abstract/MED/28540237 .tau-06-02-282 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Ramasamy R, Bryson C, Reifsnyder JE, Neri Q, Palermo GD, Schlegel PN. Overweight men with nonobstructive azoospermia have worse pregnancy outcomes after microdissection testicular sperm extraction. Fertil Steril. 2013 Mar;99(2):372–6. doi: 10.1016/j.fertnstert.2012.10.025.S0015-0282(12)02337-0 [DOI] [PubMed] [Google Scholar]
- 12.Mehmood S, Aldaweesh S, Junejo NN, Altaweel WM, Kattan SA, Alhathal N. Microdissection testicular sperm extraction: Overall results and impact of preoperative testosterone level on sperm retrieval rate in patients with nonobstructive azoospermia. Urol Ann. 2019;11(3):287–293. doi: 10.4103/UA.UA_36_18. http://www.urologyannals.com/article.asp?issn=0974-7796;year=2019;volume=11;issue=3;spage=287;epage=293;aulast=Mehmood .UA-11-287 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Tsujimura A, Matsumiya K, Miyagawa Y, Takao T, Fujita K, Koga M, Takeyama M, Fujioka H, Okuyama A. Prediction of successful outcome of microdissection testicular sperm extraction in men with idiopathic nonobstructive azoospermia. J Urol. 2004 Nov;172(5 Pt 1):1944–7. doi: 10.1097/01.ju.0000142885.20116.60.S0022-5347(05)60900-7 [DOI] [PubMed] [Google Scholar]
- 14.Corona G, Minhas S, Giwercman A, Bettocchi C, Dinkelman-Smit M, Dohle G, Fusco F, Kadioglou A, Kliesch S, Kopa Z, Krausz C, Pelliccione F, Pizzocaro A, Rassweiler J, Verze P, Vignozzi L, Weidner W, Maggi M, Sofikitis N. Sperm recovery and ICSI outcomes in men with non-obstructive azoospermia: a systematic review and meta-analysis. Hum Reprod Update. 2019 Nov 05;25(6):733–757. doi: 10.1093/humupd/dmz028.5609422 [DOI] [PubMed] [Google Scholar]
- 15.Bryson CF, Ramasamy R, Sheehan M, Palermo GD, Rosenwaks Z, Schlegel PN. Severe testicular atrophy does not affect the success of microdissection testicular sperm extraction. J Urol. 2014 Jan;191(1):175–8. doi: 10.1016/j.juro.2013.07.065. https://europepmc.org/abstract/MED/23911635 .S0022-5347(13)05030-1 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Kizilkan Y, Toksoz S, Turunc T, Ozkardes H. Parameters predicting sperm retrieval rates during microscopic testicular sperm extraction in nonobstructive azoospermia. Andrologia. 2019 Dec;51(11):e13441. doi: 10.1111/and.13441. [DOI] [PubMed] [Google Scholar]
- 17.Devroey P, Liu J, Nagy Z, Goossens A, Tournaye H, Camus M, Van Steirteghem A, Silber S. Pregnancies after testicular sperm extraction and intracytoplasmic sperm injection in non-obstructive azoospermia. Hum Reprod. 1995 Jun;10(6):1457–60. doi: 10.1093/humrep/10.6.1457. [DOI] [PubMed] [Google Scholar]
- 18.Salehi P, Derakhshan-Horeh M, Nadeali Z, Hosseinzadeh M, Sadeghi E, Izadpanahi MH, Salehi M. Factors influencing sperm retrieval following testicular sperm extraction in nonobstructive azoospermia patients. Clin Exp Reprod Med. 2017 Mar;44(1):22–27. doi: 10.5653/cerm.2017.44.1.22. https://europepmc.org/abstract/MED/28428940 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Anniballo R, Ubaldi F, Cobellis L, Sorrentino M, Rienzi L, Greco E, Tesarik J. Criteria predicting the absence of spermatozoa in the Sertoli cell-only syndrome can be used to improve success rates of sperm retrieval. Hum Reprod. 2000 Nov;15(11):2269–77. doi: 10.1093/humrep/15.11.2269. [DOI] [PubMed] [Google Scholar]
- 20.Vernaeve V, Tournaye H, Schiettecatte J, Verheyen G, Van Steirteghem A, Devroey P. Serum inhibin B cannot predict testicular sperm retrieval in patients with non-obstructive azoospermia. Hum Reprod. 2002 Apr;17(4):971–6. doi: 10.1093/humrep/17.4.971. [DOI] [PubMed] [Google Scholar]
- 21.Zitzmann M, Nordhoff V, von Schönfeld V, Nordsiek-Mengede A, Kliesch S, Schüring AN, Luetjens CM, Kamischke A, Cooper T, Simoni M, Nieschlag E. Elevated follicle-stimulating hormone levels and the chances for azoospermic men to become fathers after retrieval of elongated spermatids from cryopreserved testicular tissue. Fertil Steril. 2006 Aug;86(2):339–47. doi: 10.1016/j.fertnstert.2005.12.058. https://linkinghub.elsevier.com/retrieve/pii/S0015-0282(06)00651-0 .S0015-0282(06)00651-0 [DOI] [PubMed] [Google Scholar]
- 22.Mitchell V, Robin G, Boitrelle F, Massart P, Marchetti C, Marcelli F, Rigot J. Correlation between testicular sperm extraction outcomes and clinical, endocrine and testicular histology parameters in 120 azoospermic men with normal serum FSH levels. Int J Androl. 2011 Aug;34(4):299–305. doi: 10.1111/j.1365-2605.2010.01094.x.IJA1094 [DOI] [PubMed] [Google Scholar]
- 23.Hopps CV, Mielnik A, Goldstein M, Palermo GD, Rosenwaks Z, Schlegel PN. Detection of sperm in men with Y chromosome microdeletions of the AZFa, AZFb and AZFc regions. Hum Reprod. 2003 Aug;18(8):1660–5. doi: 10.1093/humrep/deg348. [DOI] [PubMed] [Google Scholar]
- 24.Simoni M, Tüttelmann Frank, Gromoll J, Nieschlag E. Clinical consequences of microdeletions of the Y chromosome: the extended Münster experience. Reprod Biomed Online. 2008 Mar;16(2):289–303. doi: 10.1016/s1472-6483(10)60588-3.S1472-6483(10)60588-3 [DOI] [PubMed] [Google Scholar]
- 25.Tüttelmann F, Ruckert C, Röpke A. Disorders of spermatogenesis: Perspectives for novel genetic diagnostics after 20 years of unchanged routine. Med Genet. 2018;30(1):12–20. doi: 10.1007/s11825-018-0181-7. https://europepmc.org/abstract/MED/29527098 .181 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Foresta C, Moro E, Ferlin A. Y chromosome microdeletions and alterations of spermatogenesis. Endocr Rev. 2001 Apr;22(2):226–39. doi: 10.1210/edrv.22.2.0425. [DOI] [PubMed] [Google Scholar]
- 27.Raman JD, Schlegel PN. Testicular sperm extraction with intracytoplasmic sperm injection is successful for the treatment of nonobstructive azoospermia associated with cryptorchidism. J Urol. 2003 Oct;170(4 Pt 1):1287–90. doi: 10.1097/01.ju.0000080707.75753.ec.S0022-5347(05)63147-3 [DOI] [PubMed] [Google Scholar]
- 28.Pavan-Jukic D, Stubljar D, Jukic T, Starc A. Predictive factors for sperm retrieval from males with azoospermia who are eligible for testicular sperm extraction (TESE) Syst Biol Reprod Med. 2020 Mar;66(1):70–75. doi: 10.1080/19396368.2019.1680764. [DOI] [PubMed] [Google Scholar]
- 29.Barbotin A, Dauvergne A, Dumont A, Ramdane N, Mitchell V, Rigot J, Boitrelle F, Robin G. Bilateral versus unilateral cryptorchidism in nonobstructive azoospermia: Testicular sperm extraction outcomes. Asian J Androl. 2019;21(5):445–451. doi: 10.4103/aja.aja_2_19. http://www.ajandrology.com/article.asp?issn=1008-682X;year=2019;volume=21;issue=5;spage=445;epage=451;aulast=Barbotin .254313 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Ramasamy R, Lin K, Gosden LV, Rosenwaks Z, Palermo GD, Schlegel PN. Reprint of: High serum FSH levels in men with nonobstructive azoospermia does not affect success of microdissection testicular sperm extraction. Fertil Steril. 2019 Oct;112(4 Suppl1):e67–e70. doi: 10.1016/j.fertnstert.2019.08.075. https://linkinghub.elsevier.com/retrieve/pii/S0015-0282(19)32282-4 .S0015-0282(19)32282-4 [DOI] [PubMed] [Google Scholar]
- 31.Li H, Chen L, Yang J, Li M, Chen R, Lan R, Wang S, Liu J, Wang T. Predictive value of FSH, testicular volume, and histopathological findings for the sperm retrieval rate of microdissection TESE in nonobstructive azoospermia: a meta-analysis. Asian J Androl. 2018;20(1):30–36. doi: 10.4103/aja.aja_5_17. http://www.ajandrology.com/article.asp?issn=1008-682X;year=2018;volume=20;issue=1;spage=30;epage=36;aulast=Li .202902 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Tunc L, Kirac M, Gurocak S, Yucel A, Kupeli B, Alkibay T, Bozkirli I. Can serum Inhibin B and FSH levels, testicular histology and volume predict the outcome of testicular sperm extraction in patients with non-obstructive azoospermia? Int Urol Nephrol. 2006;38(3-4):629–35. doi: 10.1007/s11255-006-0095-1. [DOI] [PubMed] [Google Scholar]
- 33.Kavoussi PK, West BT, Chen S, Hunn C, Gilkey MS, Machen GL, Kavoussi KM, Esqueda A, Wininger JD, Kavoussi SK. A comprehensive assessment of predictors of fertility outcomes in men with non-obstructive azoospermia undergoing microdissection testicular sperm extraction. Reprod Biol Endocrinol. 2020 Aug 26;18(1):90. doi: 10.1186/s12958-020-00646-4. https://rbej.biomedcentral.com/articles/10.1186/s12958-020-00646-4 .10.1186/s12958-020-00646-4 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Bachelot G, Lévy R, Bachelot A, Faure C, Czernichow S, Dupont C, Lamazière A, Alifert Collaborative Group Proof of concept and development of a couple-based machine learning model to stratify infertile patients with idiopathic infertility. Sci Rep. 2021 Dec 14;11(1):24003. doi: 10.1038/s41598-021-03165-3. doi: 10.1038/s41598-021-03165-3.10.1038/s41598-021-03165-3 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Agnani H, Bachelot G, Eguether T, Ribault B, Fiet J, Le Bouc Y, Netchine I, Houang M, Lamazière A. A proof of concept of a machine learning algorithm to predict late-onset 21-hydroxylase deficiency in children with premature pubic hair. J Steroid Biochem Mol Biol. 2022 Jun;220:106085. doi: 10.1016/j.jsbmb.2022.106085. https://linkinghub.elsevier.com/retrieve/pii/S0960-0760(22)00036-X .S0960-0760(22)00036-X [DOI] [PubMed] [Google Scholar]
- 36.Tsujimura A, Miyagawa Y, Takao T, Fujita K, Komori K, Matsuoka Y, Takada S, Koga M, Takeyama M, Fujioka H, Matsumiya K, Okuyama A. Impact of age, follicle stimulating hormone and Johnsen's score on successful sperm retrieval by microdissection testicular sperm extraction. Reprod Med Biol. 2005 Mar;4(1):53–57. doi: 10.1111/j.1447-0578.2005.00082.x. https://europepmc.org/abstract/MED/32351316 .RMB082 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Cissen M, Meijerink AM, D'Hauwers KW, Meissner A, van der Weide N, Mochtar MH, de Melker AA, Ramos L, Repping S, Braat DDM, Fleischer K, van Wely M. Prediction model for obtaining spermatozoa with testicular sperm extraction in men with non-obstructive azoospermia. Hum Reprod. 2016 Sep;31(9):1934–41. doi: 10.1093/humrep/dew147.dew147 [DOI] [PubMed] [Google Scholar]
- 38.Ramasamy R, Padilla WO, Osterberg EC, Srivastava A, Reifsnyder JE, Niederberger C, Schlegel PN. A comparison of models for predicting sperm retrieval before microdissection testicular sperm extraction in men with nonobstructive azoospermia. J Urol. 2013 Mar;189(2):638–42. doi: 10.1016/j.juro.2012.09.038.S0022-5347(12)04850-1 [DOI] [PubMed] [Google Scholar]
- 39.Zeadna A, Khateeb N, Rokach L, Lior Y, Har-Vardi I, Harlev A, Huleihel M, Lunenfeld E, Levitas E. Prediction of sperm extraction in non-obstructive azoospermia patients: a machine-learning perspective. Hum Reprod. 2020 Jul 01;35(7):1505–1514. doi: 10.1093/humrep/deaa109.5857532 [DOI] [PubMed] [Google Scholar]
- 40.WHO laboratory manual for the examination and processing of human semen, 5th ed. World Health Organization. 2010. [2023-05-31]. https://apps.who.int/iris/handle/10665/44261 .
- 41.Schlegel PN, Sigman M, Collura B, De Jonge CJ, Eisenberg ML, Lamb DJ, Mulhall JP, Niederberger C, Sandlow JI, Sokol RZ, Spandorfer SD, Tanrikut C, Treadwell JR, Oristaglio JT, Zini A. Diagnosis and treatment of infertility in men: AUA/ASRM Guideline Part I. Journal of Urology. 2021 Jan;205(1):36–43. doi: 10.1097/ju.0000000000001521. [DOI] [PubMed] [Google Scholar]
- 42.Minhas S, Bettocchi C, Boeri L, Capogrosso P, Carvalho J, Cilesiz NC, Cocci A, Corona G, Dimitropoulos K, Gül M, Hatzichristodoulou G, Jones TH, Kadioglu A, Martínez Salamanca JI, Milenkovic U, Modgil V, Russo GI, Serefoglu EC, Tharakan T, Verze P, Salonia A, EAU Working Group on Male Sexual and Reproductive Health European Association of Urology Guidelines on Male Sexual and Reproductive Health: 2021 update on male infertility. Eur Urol. 2021 Nov;80(5):603–620. doi: 10.1016/j.eururo.2021.08.014.S0302-2838(21)01982-5 [DOI] [PubMed] [Google Scholar]
- 43.Bergstra J, Bengio Y. Random search for hyper-parameter optimization. Journal of Machine Learning Research. 2012;13:281–305. https://www.jmlr.org/papers/volume13/bergstra12a/bergstra12a.pdf . [Google Scholar]
- 44.Collins GS, Reitsma JB, Altman DG, Moons K. Transparent reporting of a multivariable prediction model for individual prognosis or diagnosis (TRIPOD): the TRIPOD Statement. BMC Med. 2015 Jan 06;13(1):1. doi: 10.1186/s12916-014-0241-z. https://bmcmedicine.biomedcentral.com/articles/10.1186/s12916-014-0241-z .s12916-014-0241-z [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.Fisher A, Rudin C, Dominici F. All models are wrong, but many are useful: learning a variable's importance by studying an entire class of prediction models simultaneously. Journal of Machine Learning Research. 2019;20(177):1–81. https://www.jmlr.org/papers/volume20/18-760/18-760.pdf . [PMC free article] [PubMed] [Google Scholar]
- 46.Pedregosa F, Varoquaux G, Gramfort A, Michel V, Thirion B, Grisel O. Scikit-learn: Machine Learning in Python. Journal of Machine Learning Research. 2011;12:2825–2830. https://www.jmlr.org/papers/volume12/pedregosa11a/pedregosa11a.pdf . [Google Scholar]
- 47.Vallat R. Pingouin: statistics in Python. The Journal of Open Source Software. 2018 Nov;3(31):1026. doi: 10.21105/joss.01026. https://joss.theoj.org/papers/10.21105/joss.01026 . [DOI] [Google Scholar]
- 48.TensorFlow. Zenodo. 2022. May 23, [2023-05-29]. https://zenodo.org/record/6574269 .
- 49.Reback J, Mendel JB, McKinney W, Van DBJ, Augspurger T, Roeschke M, Hawkins S, Cloud P, Young GF, Sinhrks. Hoefler P, Klein A, Terji P, Tratner J, She C, Ayd W, Naveh S, Garcia M, Shadrach R, Schendel J, Hayden A, Saxton D, Gorelli M, Fangchen L, Zeitlin M, Jancauskas V, McMaster A, Wörtwein T, Battiston P. pandas-dev/pandas: Pandas 1.4.2. Zenodo. 2022. Apr 02, [2023-05-29]. https://zenodo.org/record/6408044 .
- 50.Harris CR, Millman KJ, van der Walt SJ, Gommers R, Virtanen P, Cournapeau D, Wieser E, Taylor J, Berg S, Smith NJ, Kern R, Picus M, Hoyer S, van Kerkwijk MH, Brett M, Haldane A, Del Río JF, Wiebe M, Peterson P, Gérard-Marchant P, Sheppard K, Reddy T, Weckesser W, Abbasi H, Gohlke C, Oliphant TE. Array programming with NumPy. Nature. 2020 Sep 16;585(7825):357–362. doi: 10.1038/s41586-020-2649-2. https://europepmc.org/abstract/MED/32939066 .10.1038/s41586-020-2649-2 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 51.guillaumebachelot / ML_TESE. GitHub. [2023-03-23]. https://github.com/guillaumebachelot/ML_TESE .
- 52.Wong WJ, Khan YS. Histology, Sertoli Cell. Treasure Island, FL: StatPearls Publishing; 2022. [PubMed] [Google Scholar]
- 53.Dabbous Z, Atkin SL. Hyperprolactinaemia in male infertility: Clinical case scenarios. Arab J Urol. 2018 Mar;16(1):44–52. doi: 10.1016/j.aju.2017.10.002.S2090-598X(17)30108-0 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 54.Tharakan T, Luo R, Jayasena CN, Minhas S. Non-obstructive azoospermia: current and future perspectives. Fac Rev. 2021;10:7. doi: 10.12703/r/10-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 55.Lima TFN, Patel P, Blachman-Braun R, Madhusoodanan V, Ramasamy R. Serum 17-hydroxyprogesterone is a potential biomarker for evaluating intratesticular testosterone. J Urol. 2020 Sep;204(3):551–556. doi: 10.1097/JU.0000000000001016. [DOI] [PubMed] [Google Scholar]
- 56.Duvilla E, Lejeune H, Trombert-Paviot B, Gentil-Perret A, Tostain J, Levy R. Significance of inhibin B and anti-Müllerian hormone in seminal plasma: a preliminary study. Fertil Steril. 2008 Mar;89(2):444–8. doi: 10.1016/j.fertnstert.2007.03.032.S0015-0282(07)00638-3 [DOI] [PubMed] [Google Scholar]
- 57.Fang N, Cao C, Wen Y, Wang X, Yuan S, Huang X. MicroRNA profile comparison of testicular tissues derived from successful and unsuccessful microdissection testicular sperm extraction retrieval in non-obstructive azoospermia patients. Reprod. Fertil. Dev. 2019;31(4):671. doi: 10.1071/rd17423. [DOI] [PubMed] [Google Scholar]
- 58.Xie Y, Yao J, Zhang X, Chen J, Gao Y, Zhang C, Chen H, Wang Z, Zhao Z, Chen W, Lv L, Li Y, Gao F, Xie M, Zhang J, Zhao L, Wang Z, Liang X, Sun X, Zou X, Deng C, Liu G. A panel of extracellular vesicle long noncoding RNAs in seminal plasma for predicting testicular spermatozoa in nonobstructive azoospermia patients. Hum Reprod. 2020 Nov 01;35(11):2413–2427. doi: 10.1093/humrep/deaa184.5903905 [DOI] [PubMed] [Google Scholar]
- 59.Ji C, Wang Y, Wei X, Zhang X, Cong R, Yao L, Qin C, Song N. Potential of testis-derived circular RNAs in seminal plasma to predict the outcome of microdissection testicular sperm extraction in patients with idiopathic non-obstructive azoospermia. Hum Reprod. 2021 Sep 18;36(10):2649–2660. doi: 10.1093/humrep/deab196.6363632 [DOI] [PubMed] [Google Scholar]
- 60.Pozza C, Kanakis G, Carlomagno F, Lemma A, Pofi R, Tenuta M, Minnetti M, Tarsitano MG, Sesti F, Paoli D, Anzuini A, Lenzi A, Isidori AM, Gianfrilli D. Testicular ultrasound score: A new proposal for a scoring system to predict testicular function. Andrology. 2020 Sep 02;8(5):1051–1063. doi: 10.1111/andr.12822. https://europepmc.org/abstract/MED/32445591 . [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Most performing hyperparameter combination for each model.
The importance of each variable in the LR, BNC, RF, GBT, XGB, SVM, and KNN models model using permutation feature importance (PFE).
Learning curve for the logistic regression (LR), Bayesian naive classification (BNC), gradient-boosted tree (GBT), XGBoost (XGB), support vector machine (SVM), and k-nearest neighbor (KNN) models: graphical representation of the relationship between model performance (measured on the vertical axis (mean area under the curve [AUC]) and the number of patients used for training (on the horizontal axis).
Data Availability Statement
The data sets generated during and/or analyzed during the current study are available from the corresponding author upon reasonable request.