

Abstract
Aim and objective
This study aimed to investigate and compare compressive strength and flexural strength of self-cured Cention N with dual-cured Cention N.
Materials and methods
Cention N is mixed according to the proportions, as mentioned by the manufacturer. Dual cured samples are cured using a diode that emits blue light. Cylindrical plexiglass split mold of dimension 6 mm height, and 4 mm diameter used to fabricate samples for compressive strength. Compressive strength tested using Instron universal testing machine. Rectangular plexiglass split mold of dimension 25 mm length, 2 mm height, and 2 mm width were used to fabricate samples for flexural strength. Flexural strength tested using Instron universal testing machine. To compare the mean values independent t-test was used and the significance of the study was measured by calculating a p-value.
Result
There is no statistically significant difference between compressive strength and flexural strength of self-cured Cention N with dual-cured Cention N.
Conclusion
The type of polymerization does not affect flexural strength and compressive strength of Cention N.
Clinical Significance
Self-curing polymerization alone is sufficient for Cention N to achieve adequate compressive strength and flexural strength. So it can be inserted as a single layer on a prepared cavity and to fasten curing additional light curing can be used.
How to cite this article
Fousiya Ks, Balagopal VR, Suresh KJ, et al. Comparative Evaluation of Compressive Strength and Flexural Strength of Self-cured Cention N with Dual-cured Cention N: An In Vitro Study. Int J Clin Pediatr Dent 2022;15(2):210-214.
Keywords: Cention N, Compressive strength, Dual-cure resin-based composite, Dual-curing, Flexural Strength, Polymerization, Self-curing
Introduction
Over the past years, aesthetic dentistry has shown substantial progress to improve many restorative materials. Direct restorative materials are those materials that can be laid directly in the prepared tooth cavity with one appointment. Various direct restorative materials are available for a dental practitioner, from silver amalgam to bulk-fill composites. Presently, the significant concerns regarding the performance of these materials point out their ability to bear the stress, durability, integrity of marginal sealing, and aesthetics.1
The first dental composites were (1950) made of self-cure polymethyl methacrylate (PMMA) and quartz particles incorporated for additional strengthening. Dr Rafael Bowen changed the monomethacrylate (MMA) with dimethacrylate monomers, mainly bisphenol A glycidyl methacrylate (Bis-GMA), due to weak abrasion resistance and high polymerization shrinkage.2 Earlier composites were self-cure systems and contained two pastes with short working time and increased porosity due to air traps during mixing.2
Light-curing dental restorative materials are specified in a patent issued in 1970 and imported to the market a few years later.3 By incorporating an ultraviolet (UV) photoinitiator, created a single-paste system, and it cured by irradiation with UV curing light.2,3 These materials give users sufficient working time to apply them in the cavity, as the polymerization reaction can start on demand.3 Health problems over personnel vulnerability to UV radiation and narrow curing depth increased searching for an alternative light-curing system.2
Composite resins cured with visible light containing alpha diketones as photoinitiators have developed.3 Camphorquinone or 1-phenyl-1,2-propanedione (PPD) and dibenzoyl (BZ) are freely available alpha diketones that absorb light in the visible spectrum.3
The addition of camphorquinone (CQ) and an amine accelerator created a more elevated curing depth when exposed to visible light. The extent of curing was dependent on the composite's formulation.2 Different monomer systems were introduced to replace Bis-GMA.2
Vienna University of Technology and Ivoclar Vivadent developed photoinitiatorIvocerin, which has significantly improved curing depth without affecting the optical properties of composite resin, such as translucency and shade.3
According to the literature, inadequate polymerization seen in the deeper aspects of the bulk placement composite restoration was due to the incapability of the light to pierce these regions. Recent developments in composite resins have resulted in increased depth of cure between 4 and 5 mm for some materials. This improvement in the depth of cure may be due to increased photoinitiator coverage or a supplemental photoinitiator type and higher material translucency.4
Another way to overcome this limited curing depth and some of the problems associated with light-curing is to combine visible light curing and chemical curing components in the same resin material (dual-cured resins).5 Dual cure materials are proposed for any situation that does not allow adequate light penetration to produce proper monomer conversion and exclude the need for incremental placement.4
Cention N is tooth-colored resin-based direct restorative material. It is a subgroup of the composite material. This novel material uses an alkaline filler (alkasite) to release acid-neutralizing ions. It is marketed as powder and liquid and hand-mixed before use (Fig. 1).6 It is self-curing with optional additional light-curing (dual-cure resin-based composite).7 Optional light curing can carry out with blue light using standard polymerization lights (400-500 nm). The curing depth is theoretically unlimited since Cention N is a self-curing material. It can be used as a one-step placement material and applied fast and convenient.6
Fig. 1.

Cention N alkasite resin-based material
Any restoration needs to resist intraoral forces during function. Flexural strength estimates a material's capacity to resist fracture, and compressive strength estimates a material's capacity to resist compression. All mechanical properties measure a material's capacity to resist fracture or deformation under an applied force or pressure.
In this situation, a usually elevated question was whether the self-curing polymerization reaction is adequate in the absence of light or in the case of reduced light transmittance. Therefore this study evaluated the effect of additional light-curing on compressive strength and flexural strength of Cention N. The null hypothesis tested whether the curing mode (self or dual) does not affect compressive strength, and the curing mode (self or dual) does not affect flexural strength of Cention N.
Materials and Methods
Manipulation of Material
Manipulation of materials was done according to the manufacturer's instructions. Cention N (Ivoclar Vivadent, LOT X 54164) is marketed as powder and liquid (Table 1). The two components of the material were mixed by one scoop of powder with one drop of liquid. Dual-cure Samples were cured using a LED light-curing unit Bluephase N (Ivoclar Vivadent), and exposure time of the 20s as per the protocol provided by the manufacturer.
Table 1.
Material, manufacturer, batch number, and composition used in this study
| Material(manufacturer) | Composition | Filler load | Batch number(lot number) | |
|---|---|---|---|---|
| Cention N (Ivoclar vivadent) |
Monomer Urethane dimethacrylate (UDMA) Tricyclodecan-dimethanol dimethacrylate (DCP) Aromatic aliphatic-UDMA Polyethylene glycol 400 dimethacrylate (PEG-400 DMA) |
Filler Barium aluminum silicate glass Ytterbium trifluoride. Isofiller Calcium barium aluminum fluorosilicate glass Calcium fluorosilicate glass |
57.6% by volume /78.4% by weight inorganic filler |
X54164 |
Compressive Strength Test
Sample Preparation for Compressive Strength
Both self-cured and dual-cured Cention N were used for this test. A total of 20 specimens were prepared in two groups (Fig. 2). Cylindrical plexiglass split mold of dimension 6 mm height and 4 mm diameter of used to fabricate samples (Fig. 2). The material is mixed according to the proportions, as mentioned by the manufacturer. Dual cured samples were cured using a diode that emits blue light. Samples were stored in distilled water at room temperature for 24 hours before evaluation.
Fig. 2.
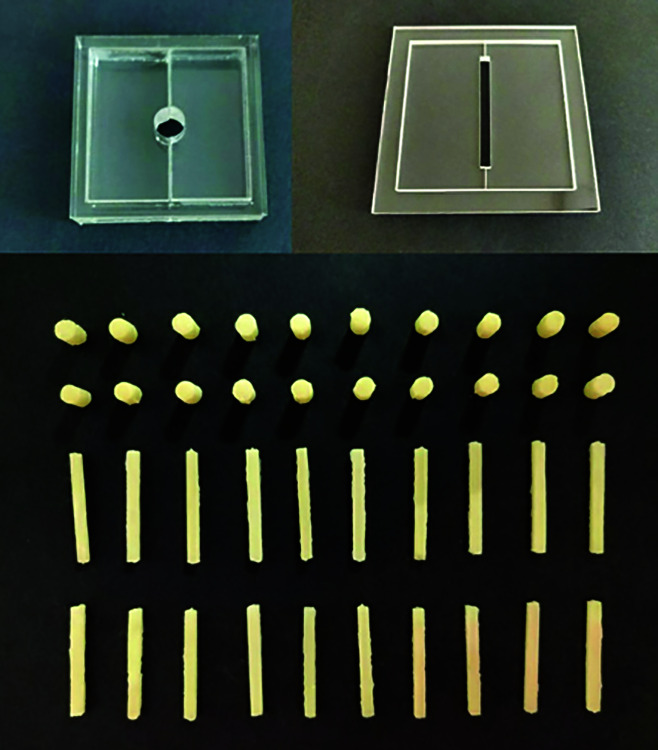
Mold and samples for compressive strength and flexural strength
Sample Evaluation for Compressive Strength
The samples were tested for compressive strength using an Instron Universal testing machine (Fig. 3) and connected to a load measuring cell. This load measuring cell continuously recorded the load applied to the samples at a crosshead speed of 0.75 ± 0.25 mm min-1 until the samples fracture.
Fig. 3.

Instron universal testing machine
Flexural Strength Test
Sample Preparation for Flexural Strength
Both self-cured and dual-cured Cention N were used for this test. A total of 20 specimens were prepared in 2 groups (Fig. 2). Rectangular plexiglass split mold of dimension 25 mm length, 2 mm height and 2 mm width used to fabricate samples (Fig. 2). The material is mixed according to the proportions, as mentioned by the manufacturer. Dual cured samples were cured using a diode that emits blue light. Samples were stored in distilled water at room temperature for 24 hours before evaluation.
Sample Evaluation for Flexural Strength
These fabricated samples were then placed on a 3-point bending test device and connected to a Universal Testing Machine (Fig. 3). The load applied to the samples was continuously recorded at a crosshead speed of 0.75 ± 0.25 mm min-1 until the samples fracture.
Statistical Analysis
The software version used for the statistical analysis was SPSS (statistical package for social sciences). An independent t-test was used to compare the mean values. The significance of the study was measured by calculating a p-value. If the p-value < 0.05, there is a significant difference between materials.
Results
Compressive Strength Test Result
Compressive strength of self-cured and dual-cured Cention N recorded. Each material's mean value and standard deviation were calculated (Table 2). A comparison of the mean strength value among the samples showed a mean compressive strength value of 151.40 MPa for self-cured Cention N and 157 MPa for dual-cured Cention N (Fig. 4). A comparison of the mean compressive strength value shows no statistically significant difference with a p-value (p = 0.448).
Table 2.
t-test of compressive strength and flexural strength
| Test | Material | Number | Mean | SD | Min | Max | SE | p-value |
|---|---|---|---|---|---|---|---|---|
| Compressive strength | Self-cured | 10 | 151.40 | 13.721 | 128 | 169 | 4.339 | 0.448 |
| Dual-cured | 10 | 157.00 | 17.839 | 136 | 182 | 5.641 | ||
| Flexural strength | Self-cured | 10 | 101.70 | 9.615 | 90.2 | 114.2 | 3.041 | 0.161 |
| Dual-cured | 10 | 107.40 | 8.972 | 90.4 | 118.9 | 2.837 |
Fig. 4.
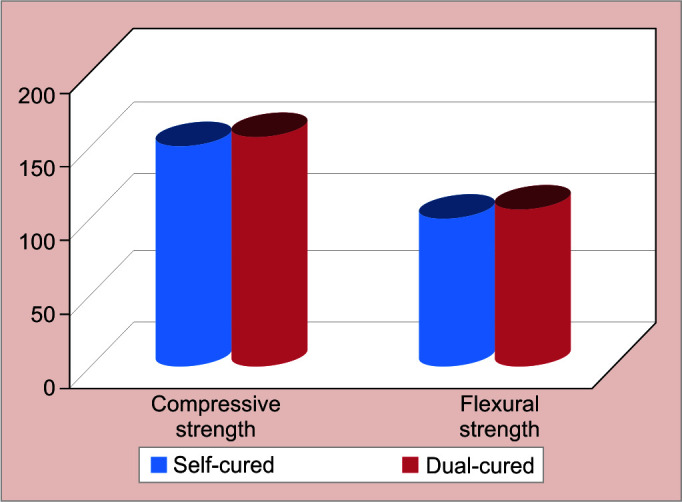
Mean values of compressive strength (MPa) and flexural strength (MPa)
Flexural Strength Test Result
Flexural strength of self-cured and dual-cured Cention N recorded. Each material's mean value and standard deviation were calculated (Table 2). Comparing the mean flexural strength values among the samples showed a mean flexural strength value of 101.7 MPa for self-cured Cention N and 107.4 MPa for dual-cured Cention N (Fig. 4). No significant changes in the measured flexural strength were identified for both self-and dual-cured groups (p = 0.161).
Discussion
In the past, less number of studies were conducted that evaluated and compared the properties of self-cured and light-cured Cention N. As per the knowledge of the authors, and no past reviews assessed the compressive strength and flexural strength of self-cured Cention N and dual-cured Cention N. This research provides a new field of knowledge that can prove to be beneficial for future studies.
The present study evaluated the effect of the curing mode on the compressive strength and the flexural strength of a novel dual-cure Resin Based Composite (RBC) with alkaline fillers used for direct filling purposes (Cention N). Cention N is accessible as powder and liquid that needs mixing before use. After mixing, the self-curing processes will initiate. After all, it may be advantageous to utilize the additional light cure function for ease in finishing and speed up the restoration.
Previous studies have shown that several factors affect the mechanical properties of the composites, such as composition, mixing method, degree of conversion, microstructure, and interaction of various other factors.8
Many factors may influence the curing of resin cement, such as the shade and translucency of cement, increment thickness, light-curing duration, distance between the light-curing tip and the curing surface, a light unit system used, cavity location, size of the cavity, filler composition, monomer composition, polymerization initiator concentration, and substrate through light passed during curing.9,10
Dual-cure resin cement behavior results from activators and the composition of the material.11
In general, polymerization of resin-based composites (RBC) initiates with free radicals because of either energy or chemical activation. An adequate amount of polymerized resin is needed for successful RBC restoration. It can achieve by having a proper amount of carbon-carbon double bonds transformed into single bonds leading to an appropriate degree of convergence.9,12
Cention N contains copper salt, peroxide, and thiocarbamide as initiator systems for the self-curing process. The liquid of Cention N contains hydroperoxide, and in the powder, the filler is coated with the other initiator components. The copper salt act as an accelerator during the curing reaction. This self-cure polymerization can only occur when the powder and liquid are mixed. self-cure polymerization involves the radical formation and redox catalysis with Cu-ions.6
Cention N contains Ivocerin (benzoyl germanium-based initiator) and an acyl phosphine oxide as a photoinitiator. Additional light-curing and polymerization take place via free radical polymerization. Photons from the curing light absorbed by the initiator Ivocerin produce free radicals and react with the monomer to create a polymer network.6 The light can only penetrate up to 4 mm thickness adequately, therefore in cavities deeper than 4 mm, the self-curing polymerization and setting time of 4 minutes must be expected.6 According to Moszner N et al. (2007), benzoyl germanium derivatives have higher photo-curing activity than ethyl 4-(N, N-dimethylamino) benzoate (EMBO) and camphorquinone (CQ).13
Studies that have compared the properties of the dual-cure resin-based composites (RBCs) have shown that the procedure of light irradiation and its effect primarily depends on the material type, providing little impact to high impact on the final properties of the material.14 According to Fonseca RG et al., the reason for this behavior variation of the dual-curing resin cement is more related to the formulation of cement.15
Most photopolymerizable dental composite resin materials are a mixture of monomers. It includes 2-hydroxyethyl methacrylate (HEMA), Bis-GMA, Bis-EMA, urethane dimethacrylate (UDMA), and tri ethylene glycol dimethacrylate (TEGDMA).16,17
Sideridou et al. 2002 found that in the polymerization of UDMA, the structure formed is more acceptable than the other monomers.18 Dickens et al. analyzed the photopolymerization of Bis-GMA and UDMA and found that UDMA was more functional than the Bis-GMA.19 Studies on the influence of monomer composition on the mechanical properties of resin composites have found that flexural strength increases when UDMA substitutes Bis-GMA or TEGDMA.20,21 Cention N does not contain Bis-GMA, TEGDMA, or HEMA, which is usually present in most resin composites. UDMA is the monomer matrix's leading component and contains aromatic and aliphatic UDMA, DCP, PEG- 400 DMA (Table 1).
Fillers impart restorative materials with adequate strength. It helps to withstand occlusal forces and attain good clinical durability.21 The inorganic fillers of Cention N contain ytterbium trifluoride, barium aluminum silicate glass, Isofiller, calcium fluorosilicate (alkaline) glass, and calcium barium aluminum fluorosilicate glass (Table 1).6
Nicoleta Ilie evaluated the influence of further light-curing on the degree of conversion (DC), polymerization kinetics, and mechanical properties of Cention N. Study found that light-curing initially hastens the polymerization kinetics and does not affect the final properties.7
The present study revealed that the curing mechanism has little effect on the flexural strength and compressive strength of the Cention N. However, it may be beneficial to use the optional light-curing function to speed up the restorative process.
Conclusion
Based on the current in-vitro study findings, there is no significant difference between compressive strength and flexural strength of self-cured Cention N with dual-cured Cention N. Also, the type of polymerization has no significant effect on the compressive strength and flexural strength of Cention N.
Clinical Significance
Self-curing polymerization alone is sufficient for Cention N to achieve adequate compressive strength and flexural strength. So it can be placed as a single layer on a prepared cavity, and light-curing can accelerate curing. As a result, this material has clinical advantages in handling, curing efficiency, and time-saving.
Acknowledgments
We appreciate the staff at the mechanical engineering department, Amrita School of Engineering, Ettimadai, Coimbatore, for their assistance in analyzing samples.
Footnotes
Source of support: Nil
Conflict of interest: None
References
- 1.Mann JS, Sharma S, Maurya S., et al. Cention N: A review. Int J Curr Res. 2018;10(5):69111–69112. [Google Scholar]
- 2.Bayne SC, Ferracane JL, Marshall GW, et al. The evolution of dental materials over the past century: silver and gold to tooth color and beyond. J Dent Res. 2019;98(3):257–265. doi: 10.1177/0022034518822808. [DOI] [PubMed] [Google Scholar]
- 3.Moszner N. State of the : Photopolymerization in dentistry. IvoclarVivadent Report. Liechtenstein: IvoclarVivadent AG. 2013:19. [Google Scholar]
- 4.Vandewalker JP, Casey JA, Lincoln TA, et al. Properties of dual-cure, bulk-fill composite resin restorative materials. Gen Dent. 2016;64(2):68–73. 26943093 [PubMed] [Google Scholar]
- 5.Anusavice KJ, Shen C, Rawls HR., editors. Phillips’ science of dental materials. Elsevier Health Sciences; 2012.
- 6.Todd JC. Ivoclar-Vivadent Press; Schaan, Liechtenstein.: 2016. Scientific Documentation: Cention N. pp. 1–58. [Google Scholar]
- 7.Ilie N. Comparative effect of self-or dual-curing on polymerization kinetics and mechanical properties in a novel, dental-resin-based composite with alkaline filler. Running resin-composites with alkaline fillers. Materials (Basel) 2018;11(1):108. doi: 10.3390/ma11010108. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.AlQahtani MQ, AlShaafi MM, Price RB. Effects of single-peak vs poly wave light-emitting diode curing lights on the polymerization of resin cement. J Adhes Dent. 2013;15(6):547–551. doi: 10.3290/j.jad.a29634. [DOI] [PubMed] [Google Scholar]
- 9.AlShaafi MM. Factors affecting polymerization of resin-based composites: a literature review. Saudi Dent J. 2017;29(2):48–58. doi: 10.1016/j.sdentj.2017.01.002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Ozturk B, Cobanoglu N, Cetin AR, et al. Conversion degrees of resin composites using different light sources. Eur J Dent. 2013;7(1):102–109. 23407765 PMC3571517 [PMC free article] [PubMed] [Google Scholar]
- 11.Peutzfeldt A. Dual-cure resin cement: in vitro wear and effect of quantity of remaining double bonds, filler volume, and light curing. Acta Odontol Scand. 1995;53(1):29–34. doi: 10.3109/00016359509005941. [DOI] [PubMed] [Google Scholar]
- 12.Rueggeberg FA. From vulcanite to vinyl, a history of resins in restorative dentistry. J Prosthet Dent. 2002;87(4):364–379. doi: 10.1067/mpr.2002.123400. [DOI] [PubMed] [Google Scholar]
- 13.Moszner N, Fischer UK, Ganster B, et al. Benzoyl germanium derivatives as novel visible light photoinitiators for dental materials. Dent Mater. 2008;24(7):901–907. doi: 10.1016/j.dental.2007.11.004. [DOI] [PubMed] [Google Scholar]
- 14.Ilie N, Simon A. Effect of curing mode on the micro-mechanical properties of dual-cured self-adhesive resin cements. Clin Oral Investig. 2012;16(2):505–512. doi: 10.1007/s00784-011-0527-x. [DOI] [PubMed] [Google Scholar]
- 15.Fonseca RG, Cruz CA, Adabo GL. The influence of chemical activation on the hardness of dual-curing resin cements. Braz Oral Res. 2004;18(3):228–232. doi: 10.1590/s1806-83242004000300009. [DOI] [PubMed] [Google Scholar]
- 16.Tanimoto Y, Hayakawa T, Nemoto K. Analysis of photopolymerization behaviour of UDMA/TEGDMA resin mixture and its composite by differential scanning calorimetry. J Biomed Mater Res B Appl Biomater. 2005;72(2):310–315. doi: 10.1002/jbm.b.30151. [DOI] [PubMed] [Google Scholar]
- 17.Moszner N, Fischer UK, Angermann J, et al. A partially aromatic urethane dimethacrylate as a new substitute for Bis-GMA in restorative composites. Dent Mater. 2008;24(5):694–699. doi: 10.1016/j.dental.2007.07.001. [DOI] [PubMed] [Google Scholar]
- 18.Sideridou I, Tserki V, Papanastasiou G. Effect of chemical structure on degree of conversion in light-cured dimethacrylate-based dental resins. Biomaterials. 2002;23(8):1819–1829. doi: 10.1016/s0142-9612(01)00308-8. [DOI] [PubMed] [Google Scholar]
- 19.Dickens SH, Stansbury JW, Choi KM, et al. Photopolymerization kinetics of methacrylate dental resins. Macromolecules. 2003;36(16):6043–6053. doi: 10.1021/ma021675k. [DOI] [Google Scholar]
- 20.Monteiro GQ, Montes MA. Evaluation of linear polymerization shrinkage, flexural strength and modulus of elasticity of dental composites. Mater Res. 2010;13(1):51–55. doi: 10.1590/s1516-14392010000100012. [DOI] [Google Scholar]
- 21.Chole D. In Vitro Comparision of Flexural Strength of Cention-N, Bulk-Fill Composites, Light-Cure Nanocomposites And Resin-Modified Glass Ionomer Cement. IOSR-JDMS. 2018;17(10):79–82. doi: 10.9790/0853-1710087982. [DOI] [Google Scholar]