

Abstract
Objective:
There is a broad spectrum of dietary supplements (DS) and their accessibility worldwide. However, little is known about the prevalence of DS use among Bangladeshi adolescents. This study estimates the prevalence, correlates and common conditions related to DS use.
Design:
A cross-sectional, convenient sampling strategy was adopted using an interviewer-administered, structured questionnaire.
Setting:
Kurigram and Patuakhali districts of Bangladesh.
Participants:
702 adolescents aged 10–19 years.
Results:
The overall prevalence of DS use was 83 %. The majority of participants (93·4 %) agreed that DS were good for health, and 28·3 % reported general health and well-being as the reason for using DS. The most frequently used supplements were multivitamins (38·6 %) and Ca (37 %). DS use was more common among adolescents who had ≤5 siblings, good health status, no chronic diseases, a positive impression that DS are good for health and who had the tendency to encourage DS to others. DS use was also higher among those who received DS information from healthcare providers, professional literature, friends, family and relatives.
Conclusions:
The prevalence of DS use is relatively higher among Bangladeshi adolescents compared to Bangladeshi adults and adolescents from other countries, highlighting the inclination towards DS use. Guidelines for safe DS use for adolescents are warranted to control DS use and prevent adverse effects.
Keywords: Dietary supplements, Adolescents, Prevalence and predictors, Bangladesh
An increasing rate in the era of using dietary or nutritional supplements is seen worldwide. In addition, adolescents’ interest in taking dietary supplements (DS) is countably growing, ranging from approximately 10 % to as high as 74 %(1). There is no one particular reason behind the use of DS and a few studies found some reasons for taking supplements that include: reducing the risk of dietary deficiency; losing or gaining weight; muscle building; overall wellness to boost immunity and decrease susceptibility to diseases and as an energy source(2,3). Adolescents think they need extra nutrients from DS to compensate for their energy loss for studies and extra-academic activities(4). These supplements are neither meant to cure diseases or health conditions nor to be used as medicines(5).
Researchers reported that approximately one-third of US children and adolescents (34·0 %) take DS(6). In Japan, only 6·8 % of elementary school children were spotted as DS users, and this use was significantly associated with the highest frequency of sports participation, household income and maternal education(7). Another Korean study identified that 33·4 % of the children and adolescents in their study population took DS and concluded that DS were higher in the socio-economically stable groups with good health behaviour(8). A study conducted in Poland reported that about 29·6 % of participants used DS, where gender, residential area, BMI and health status were the predictors of DS use(9). As reported earlier, about 20·1 % of adolescents use DS in the Australian population(10). The previous literature shows that most multivitamins, vitamin D, n-3-fatty acids and minerals are the prioritised DS. On the other hand, herbs, probiotics, proteins, fish oils, soya products and botanicals are used less(6–12).
Diversity in demographic characteristics of the population appears to influence the prevalence of supplement use(9,13). A recent study revealed that the DS use was higher among women and older people in Bangladesh. Demographic and lifestyle factors such as monthly income, educational status, sedentary lifestyle and smoking status were reported to correlate with DS use(14). Another survey was conducted in 2018 to investigate the dynamics of DS use and the assessment revealed that approximately 41·3 % of undergraduate female students were DS users according to their previous year’s usage records(15). They use DS for health and well-being, as energy sources, immune boosters and memory enhancers, for weight loss or maintenance and on physician recommendations, among others(15).
The use of DS represents a field of interest because of their potential impact on disease. However, in Bangladesh, surveys on the prevalence and determinants of DS use primarily focus on adults(4,14,15), demonstrating that pregnant and non-pregnant women mainly consume Ca, Zn and Fe supplements, and male and female participants consume DS without prescriptions. At the same time, the number of studies conducted on children and adolescents is limited. Therefore, the main objective of our current study is to evaluate the prevalence of DS and their associated factors among adolescents in the selected parts of Bangladesh.
Methods
Study area and settings
A cross-sectional study was conducted in the Kurigram and Patuakhali districts of Bangladesh. The Kurigram district is located in the northern region along with the border of India and is administratively divided into nine Upazilas (sub-districts). Patuakhali district is located in the southern part of Bangladesh and is divided into eight Upazilas.
Questionnaire and data collection techniques
A structured questionnaire was prepared by critically reviewing relevant literature(7–10,13–15). The survey included socio-demographic characteristics, health-related factors, sources of information on DS, reasons for use and non-use of DS, types of DS used, frequency of DS use, adverse effects of DS use and opinions regarding DS use. Six health professionals and two-BSc qualified nutritionists were recruited for data collection. Data were collected through face-to-face interviews in the schools outside the classroom using a pretested questionnaire. Interviews were conducted only with those participants who agreed to provide the data. Data collection was under the continuous supervision of the authors.
Sampling and sample size
The study data were collected by a convenient sampling method. Participants were selected based on study purpose (10 to 19 years) with the expectation that each participant would provide unique and rich information to the study. The sample size was determined using the formula for cross-sectional study,
 , where n is the required sample size, Z is 1·96 at a 95 % CI, D is the margin of error at 5 % (SD of 0·05) and
, where n is the required sample size, Z is 1·96 at a 95 % CI, D is the margin of error at 5 % (SD of 0·05) and
 . The value of P was considered 50 % because of the unavailability of a similar study among adolescents. Therefore, a minimum sample size of 384 was obtained. There were 734 participants interviewed, of whom 32 were excluded due to missing values, yielding a final analytical sample size of 702 (360 from Patuakhali and 342 from Kurigram). This made the response rate 95·60 %.
. The value of P was considered 50 % because of the unavailability of a similar study among adolescents. Therefore, a minimum sample size of 384 was obtained. There were 734 participants interviewed, of whom 32 were excluded due to missing values, yielding a final analytical sample size of 702 (360 from Patuakhali and 342 from Kurigram). This made the response rate 95·60 %.
Dependent variable and predictors
The dependent variable DS use was categorised as ‘yes’ if the participants had used it in the past month and ‘no’ if they had not used DS in the past month. In addition, socio-demographic and socio-economic variables (age, sex, education, mother’s education, area, income, religion and number of siblings) and other related variables (self-related health status, chronic disease, physical activity, number of meals taken/day, impression about DS for health and knowledge source of DS) were considered as predictors (see Fig. 1 for details).
Fig. 1.

Frequency of dietary supplements consumption (n 583)
Statistical analysis
All the statistical analyses were done using IBM SPSS statistics (version 26.0) and R (version 3.8.1). This study used Microsoft Excel as a calculator and second analysing software. First, simple descriptive tests (Chi-square and Fisher’s exact tests) were done to observe the frequencies, percentages, means and other information regarding variables. Then multivariate logistic regression analysis was used to evaluate the association between DS use and independent variables. The logistic regression model was validated by the ‘Omnibus tests of model coefficient’ and the ‘Hosmer and Lemeshow test’ with a P-value of <0·001 (30 df, χ 2 = 239·18) and 0·116 (517 df, χ 2 = 555·61), respectively. AOR with 95 % CI and P < 0·05 were used to assess the association between dependent and independent variables. P < 0·05 were considered significant. A forest plot was used for the graphical display of the significant findings.
Results
Demographic and health-related information of the participants
Table 1 represents the socio-demographic and health-related information of 702 participants, of whom 83 % (583) were DS users and 17 % (119) were non-users. The number of female participants was 54·1 % (n 380) which was relatively higher than males. Most of the participants (81·8 %, n 574) were 15 to 19 years old. In addition, the majority of the participants were from high school (94·6 %, n 664). Almost all the participants (88·9 %, n 624) lived in rural areas. Furthermore, most of the participants (n 429, 61·1 %) had a lower family income level of <15 000 BDT (15 000 BDT = 157·90 US $). Finally, 82·2 % (n 577) of participants reported good health status and 88·7 % (n 623) of participants were free from chronic diseases.
Table 1.
Association of demographic and health-related variables with the use of dietary supplements (DS)
| Variables | Categories | Dietary supplement | χ 2 | P-value | |||||
|---|---|---|---|---|---|---|---|---|---|
| Total (n 702) | DS (-) = 119 | DS (+) = 583 | |||||||
| n | % | n | % | n | % | ||||
| Age | 10 to 14 | 128 | 18·2 | 27 | 21·1 | 101 | 78·9 | 1·91 | 0·167 |
| 15 to 19 | 574 | 81·8 | 92 | 16·0 | 482 | 84·0 | |||
| Gender | Male | 322 | 45·9 | 52 | 16·1 | 270 | 83·9 | 0·27 | 0·602 |
| Female | 380 | 54·1 | 67 | 17·6 | 313 | 82·4 | |||
| Education | High school | 664 | 94·6 | 107 | 16·1 | 557 | 83·9 | 6·11 | 0·013 |
| College | 38 | 5·4 | 12 | 31·6 | 26 | 68·4 | |||
| Mother’s education | No formal education | 25 | 3·6 | 7 | 28·0 | 18 | 72·0 | 6·80 | 0·147 |
| Primary school | 222 | 31·6 | 29 | 13·1 | 193 | 86·9 | |||
| Secondary school | 317 | 45·2 | 60 | 18·9 | 257 | 81·1 | |||
| Higher secondary school | 128 | 18·2 | 20 | 15·6 | 108 | 84·4 | |||
| Honor’s and above | 10 | 1·4 | 3 | 30·0 | 7 | 70·0 | |||
| Family income (BDT) | Low (<15 000) | 429 | 61·1 | 77 | 17·9 | 352 | 82·1 | 1·63 | 0·443 |
| Middle (15 000–30 000) | 234 | 33·3 | 34 | 14·5 | 200 | 85·5 | |||
| High (>30 000) | 39 | 5·6 | 8 | 20·5 | 31 | 79·5 | |||
| Religion | Muslim | 604 | 86·0 | 99 | 16·4 | 505 | 83·6 | 0·97 | 0·326 |
| Hindu | 98 | 14·0 | 20 | 20·4 | 78 | 79·6 | |||
| Residence | Urban | 78 | 11·1 | 11 | 14·1 | 67 | 85·9 | 0·51 | 0·477 |
| Rural | 624 | 88·9 | 108 | 17·3 | 516 | 82·7 | |||
| Number of siblings | 1 to 2 | 301 | 42·9 | 53 | 17·6 | 248 | 82·4 | 25·94 | <0·001 |
| 3 to 5 | 377 | 53·7 | 53 | 14·1 | 324 | 85·9 | |||
| More than 5 | 24 | 3·4 | 13 | 54·2 | 11 | 45·8 | |||
| Self-reported health status | Poor or fair | 20 | 2·8 | 8 | 40·0 | 12 | 60·0 | 24·63 | <0·001 |
| Good | 577 | 82·2 | 90 | 15·6 | 487 | 84·4 | |||
| Very good | 88 | 12·5 | 12 | 13·6 | 76 | 86·4 | |||
| Excellent | 17 | 2·4 | 9 | 52·9 | 8 | 47·1 | |||
| Physical ability | Low | 24 | 3·4 | 8 | 33·3 | 16 | 66·7 | 5·96 | 0·051 |
| Moderate | 638 | 90·9 | 107 | 16·8 | 531 | 83·2 | |||
| High | 40 | 5·7 | 4 | 10·0 | 36 | 90·0 | |||
| Chronic diseases | No | 623 | 88·7 | 86 | 13·8 | 537 | 86·2 | 38·96 | <0·001 |
| Yes | 79 | 11·3 | 33 | 41·8 | 46 | 58·2 | |||
| Number of meals/d | ≤3 | 413 | 58·8 | 87 | 21·1 | 326 | 78·9 | 12·06 | 0·002 |
| Four | 261 | 37·2 | 29 | 11·1 | 232 | 88·9 | |||
| ≥5 | 28 | 4·0 | 3 | 10·7 | 25 | 89·3 | |||
| DS are good for health | No | 30 | 4·3 | 16 | 53·3 | 14 | 46·7 | 137·53 | <0·001 |
| Yes | 476 | 67·8 | 27 | 5·7 | 449 | 94·3 | |||
| I do not know | 196 | 27·9 | 76 | 38·8 | 120 | 61·2 | |||
| Encourage the use of DS | Yes, I always encourage | 239 | 34·0 | 17 | 7·1 | 222 | 92·9 | 163·59 | <0·001 |
| Yes, only on doctor’s recommendation | 283 | 40·3 | 16 | 5·7 | 267 | 94·3 | |||
| Not at all | 180 | 25·6 | 86 | 47·8 | 94 | 52·2 | |||
| Knowledge sources | Healthcare provider | 155 | 22·1 | 14 | 9·0 | 141 | 91·0 | 11·06 | 0·050 |
| Internet | 99 | 14·1 | 21 | 21·2 | 78 | 78·8 | |||
| Professional literature | 41 | 5·8 | 6 | 14·6 | 35 | 85·4 | |||
| Friends, family members and relatives | 241 | 34·3 | 43 | 17·8 | 198 | 82·2 | |||
| Social media or seminar | 75 | 10·7 | 14 | 18·7 | 61 | 81·3 | |||
| Book | 91 | 13·0 | 21 | 23·1 | 70 | 76·9 | |||
Note: (15 000 BDT = 157·90 US $). DS (−) = Dietary supplement non-users, and DS (+) = Dietary supplement users.
Sources of knowledge of dietary supplements
The knowledge sources are also explained in Table 1. A major portion of the participants (34·3 %) knew about DS from their friends, family members and relatives. 22·1 % were informed by their healthcare provider. About 14·1 % and 13 % of the participants reported that they learned about DS from the internet and books, respectively.
Association of demographic and health-related variables with dietary supplement use
The interrelation of demographic and health-related variables with DS use is displayed in Table 1. Education, number of siblings, self-reported health status, chronic diseases, number of meals/d, DS are good for health and encouragement of DS use were significantly associated with DS use.
Frequency of dietary supplement use
Figure 1 illustrates that 58·5 % of participants used DS 2–5 times a week, 20·8 % used DS less than twice a week and 20·8 % used DS more than 5 times a week (n 583).
Reasons for using and not-using dietary supplements
The comprehensive rationales regarding using and non-using participants of DS are represented in Fig. 2 (n 583 for DS users and n 119 for non-users). A large number of the participants took DS to improve their general health and well-being (28·3 %). A smaller portion of the participants used DS as an energy source (18·2 %). On the other hand, several reasons came out from the survey for not using DS. A greater portion (40·3 %) mentioned that they did not know enough about the use of DS. Moreover, 29·4 % of participants believed that they did not need any DS. Of note, 21 % of the participants did not take supplements due to the fear of complications.
Fig. 2.

Reasons for using and not using dietary supplements (n 583 for DS users and n 119 for non-users)
Types of dietary supplement use
There was a mixed response to the use of supplements among participants (n 583). Figure 3 shows that the majority (38·6 %) of supplement users commonly used multivitamins. The second peak of users (37 %) took Ca as DS. Apart from those, 9·1 % of participants reported using other supplements that were not specified.
Fig. 3.

Types of dietary supplements used (n 583)
Adverse effects of dietary supplement use
The interviewers asked participants if they experienced any adverse reactions due to DS use (n 583). The results are represented in Fig. 4, where more than half (69·6 %) of users did not face any effect on using DS. In contrast, many of them revealed several adverse effects, which include rapid weight gain (11·1 %), hair loss (3·9 %), nausea, vomiting and diarrhoea (2·7 %), confusion, headaches and vertigo (2·6 %). Excluding these reactions, an observable number of other consequences were encountered by 9·9 % of participants, which were not specified.
Fig. 4.

Adverse reactions experienced from dietary supplements (n 583)
Opinions regarding dietary supplement use
The details of opinions about the use of DS are presented in Fig. 5 (n 702). More than 53·3 % of the adolescents disagreed with recommending DS for all age groups, whereas 65·5 % of the participants were neutral that DS use seemed harmless. Besides, approximately 60 % of participants showed neutral thoughts that the use of DS might prevent chronic diseases. Over 40 % of the participants were neutral about whether DS might prevent cancer. On the contrary, 30 % of participants disagreed with this opinion. Another opinion came forward from the participants that if DS were improperly used, they might be harmful to health and 41 % of participants strongly agreed with this opinion. The rest of the participants had non-specified explanations, most of which were neutral (approximately 70 %).
Fig. 5.
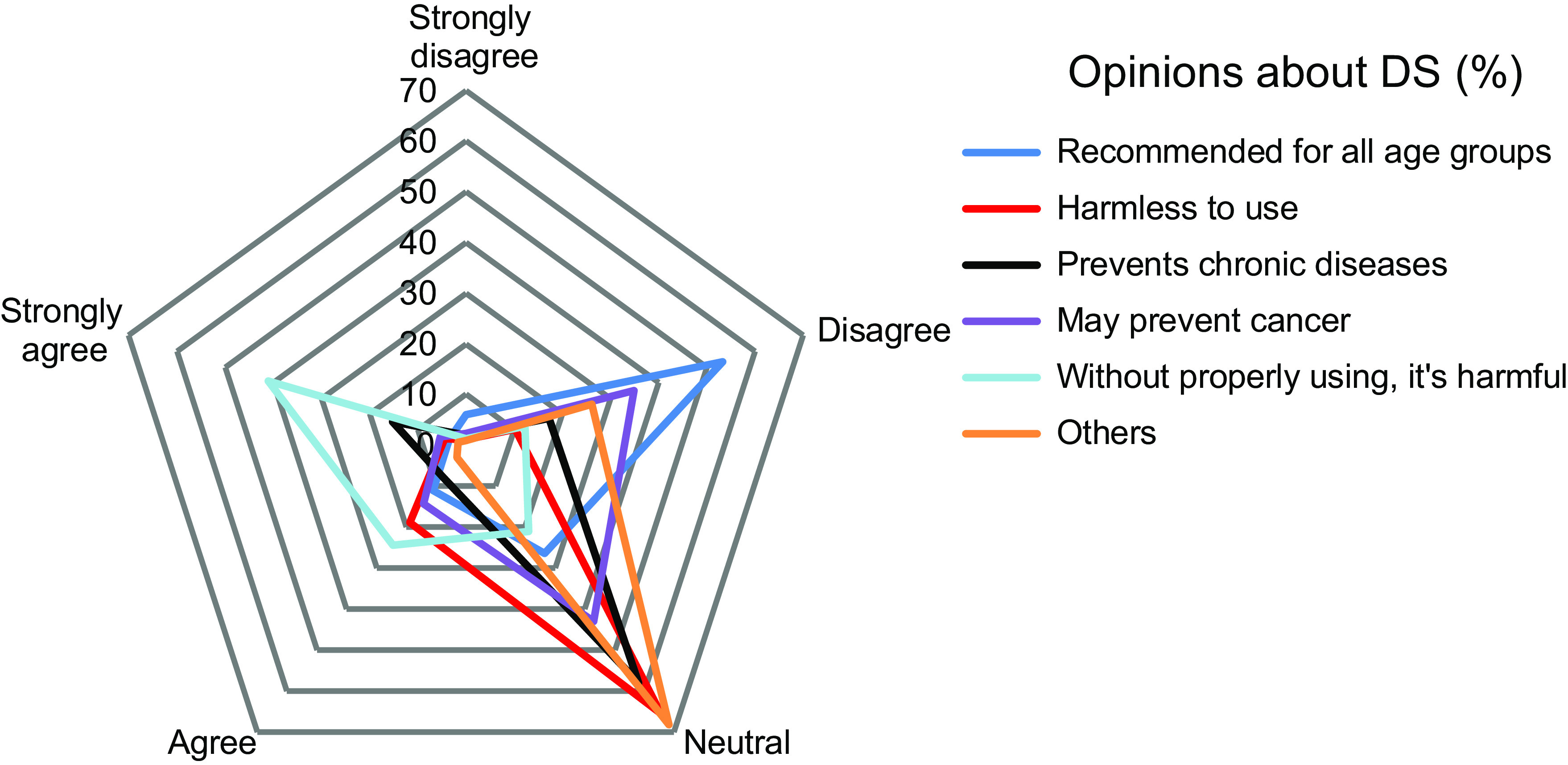
Opinions regarding the use of dietary supplements (n 702)
Predictors of dietary supplement use
Figure 6 puts on a view of predictors of DS use. DS use was associated with the number of siblings, self-reported health status, chronic disease, perceived health benefits of DS, encouragement of DS use and knowledge sources (a resource where information about DS can be found). Participants with ≤2 siblings (AOR = 5·25, 95 % CI (1·47, 18·69)) and those with 3 to 5 siblings had higher odds (AOR = 5·21, 95 % CI (1·47, 18·50)) than those with ≥5 siblings. In terms of self-reported health status, participants with good health status (AOR = 5·96, 95 % CI (1·57, 22·63)) and very good health status had higher odds (AOR = 6·29, 95 % CI (1·40, 28·18)) than those with excellent health status. Participants who did not have chronic disease had higher odds (AOR = 3·58, 95 % CI (1·82, 7·05)) than those who did. Participants who claimed DS were good for their health had higher odds (AOR = 5·27, 95 % CI (2·67, 10·40)) than those who did not know whether DS were good for their health. Participants who always encouraged others (AOR = 4·23, 95 % CI (1·93, 9·25)) and encouraged others on the doctor’s advice had higher odds (AOR = 6·77, 95 % CI (3·19, 14·37)) than those who never encouraged others. Participants whose knowledge source was healthcare providers had higher odds (AOR = 4·91, 95 % CI (1·87, 12·87)) than those whose knowledge source was the book. Moreover, participants whose knowledge source was professional literature (AOR = 6·32, 95 % CI (1·53, 26·10)), and friends, family and relatives had greater odds (AOR = 3·39, 95 % CI (1·47, 7·83)) in contrast to those who knew by the book.
Fig. 6.

Forest plot of OR and 95 % CI representing the correlation between predictors and dietary supplement use
Discussion
The current cross-sectional study was conducted to demonstrate the prevalence of DS use and the related factors among adolescents in Bangladesh. This survey was specifically carried out with male and female teenagers from 10 to 19 years of age. The demographic and health characteristics greatly influenced the prevalence of DS use among adolescents. The prevalence of DS use in Bangladeshi adolescents (83 %) seemed higher than in Bangladeshi adults (41 %), Bangladeshi undergraduate female students(14,15), Japanese adolescents (20·4 %)(16), Australian teenagers (20·1 %)(10), Canadian adolescents (42·5 %)(17) and Korean children and adolescents (34 %)(8). However, there was no data available for Bangladeshi adolescents to compare with. The higher prevalence of DS use in this study compared to Bangladeshi adults and adolescents from other countries might be due to the increased availability and wide variety of DS across the country, such as in pharmacies and drug and DS markets, as the sale of supplements is not regulated in Bangladesh(15). There is no regulation and health policy on the production and use of DS in Bangladesh compared to countries (including Canada, Australia, Japan and Korea) applying regulations to DS considerably(8,10,16,17). DS use in Bangladesh might also be influenced by commercial advertisements.
Across all participants in our study, the most commonly reported type of DS used was multivitamins, which is in line with other literature(18,19). Ca was the most supplemented mineral, similar to the results of a German study(20). The higher use of multivitamins and Ca in this study might be due to their availability in pharmacies, large discount stores and online.
The adolescents were asked about the reasons behind the use of DS. In accordance with previous studies(18,19), the main reason for using DS was to improve or maintain general health and well-being, followed by energy sources. Moreover, we found that only a few took those supplements on a physician’s recommendation, while the majority did not even realise they needed a recommendation and willingly used supplements on their own. Some participants had no particular reason as they were unsure about their use. It may indicate a lack of knowledge that leads them to misinformation and uncertainty. Thus, the results of this study contribute to a deeper understanding of the reasons for dietary supplementation by adolescents.
This current study reported several adverse effects of taking DS, although the majority of the participants reported no adverse effects, similar to other studies(15,21). However, when taken in excess, DS may have adverse effects(22,23). Interestingly, similar to a previous study, a large proportion of the participants strongly agreed that DS are harmful if not used properly(24). Surprisingly, another recent study provides results that are incompatible with the findings of our study(15), maintains that DS are safe to use and ignores the necessity for paying attention to the use of DS.
In this study, we observed that a small number of siblings was associated with a higher intake of DS, whereas the other studies found no such association(15,25). One prominent explanation is that a small number of siblings might increase personal finances and household savings, thereby enhancing the use of DS.
Similar to recent studies(7,13), an interesting finding was that DS use was more prevalent among adolescents with good and very good health status. These findings are unique and require further elucidation. In our study, adolescents suffering from chronic diseases consume fewer DS might reflect that the DS used in Bangladeshi adolescents are mainly for health promotion but not for the treatment of diseases(8,9).
In agreement with extant literature, most of the participants from the current study believed that DS are good for health and used more DS while a negligible number of the participants disagreed with the statement(15,26). Moreover, the largest portion of the participants recommended DS only on a doctor’s recommendation and used more DS. Although, all the given frequencies of the participants regarding other statements are almost similar. According to our study, knowledge sources have an impact on DS use, and it shows that gathering knowledge from healthcare professionals, family and friends and professional literature contributes to higher DS use. This could be explained by the fact that participants from the study area were influenced by their family and friends and by healthcare professionals while practicing DS.
The major limitation of this study was that it was carried out in a few districts in limited areas. Hence, our results are not generalisable. In addition, we did not examine the dosage used for the DS nor the duration of use by the participants. Information about nutritional status-related parameters was not available. Since our data were cross-sectional, no causal inferences can be drawn. Despite this point, we believe that our study will be a great resource of research information to understand the current state of DS use among adolescents and build an ideal direction in the case of future supplementary uses. Furthermore, adolescents and parents may understand the importance of the involvement of health professionals and authorities before planning to take such DS to avoid harmful effects.
Conclusions
In summary, the present findings are that 83 % of Bangladeshi adolescents use DS, a higher prevalence than what has been found in adolescents living in other countries. Many of these participants believe that DS are good for their general health based on information obtained from Friends, family members and relatives, healthcare providers and the internet, but a significant number may not recognise the potential for adverse effects. Therefore, healthcare professionals should assess whether or not their young patients use DS and ensure that they are appropriately informed about these supplements’ potential benefits and risks. In addition, further research is needed, encompassing a wide variety of DS, including a larger study population, exploring nutritional supplementations along with nutritional status, food habits and health.
Acknowledgements
Acknowledgements: We would like to thank all the participants for their enthusiastic participation. Our special thanks to all the data collectors for their time and effort. Financial support: This research received no specific grant from any funding agency, commercial or not-for-profit sectors. Authorship: N.R.: Conceptualisation, Visualisation, methodology, software, data curation, formal analysis, writing-original draft, writing-reviewing and editing, supervision. M.B.A.: Visualisation, methodology, software, data curation, formal analysis, writing-original draft, writing-reviewing and editing. M.A.: Visualisation, methodology, writing-original draft, writing-reviewing and editing. A.E.M.: Visualisation, methodology, writing-original draft, writing-reviewing and editing. E.H.: Visualisation, writing-reviewing and editing. M.N.I.: Writing-reviewing and editing. All authors read and approved the final version of the manuscript. Ethics of human subject participation: This study was conducted according to the guidelines laid down in the Declaration of Helsinki and all procedures involving research study participants were approved by the Research Ethical Committee (REC) of the Department of Biochemistry and Food Analysis, Patuakhali Science and Technology University, Bangladesh (Approval Number: BFA: 13/09/2021:04). Written informed consent was obtained from all subjects/patients.
Conflicts of interest:
There are no conflicts of interest.
References
- 1. Dorsch KD & Bell A (2005) Dietary supplement use in adolescents. Curr Opin Pediatr 17, 653–657. [DOI] [PubMed] [Google Scholar]
- 2. Ervin RB, Wright JD & Kennedy-Stephenson J (1999) Use of dietary supplements in the United States, 1988–1994. Vital Health Stat 11, 1–14. [PubMed] [Google Scholar]
- 3. Dickinson A, Blatman J, El-Dash N et al. (2014) Consumer usage and reasons for using dietary supplements: report of a series of surveys. J Am Coll Nutr 33, 176–182. [DOI] [PubMed] [Google Scholar]
- 4. Tasfia SZ, Kabir MA, Islam MR et al. (2020) Study on nutritional supplements for females in Dhaka City, Bangladesh. Bangladesh Pharm J 23, 39–43. [Google Scholar]
- 5. NIH (2020) Dietary Supplements: What You Need to Know – Consumer. National Institutes of Health. https://ods.od.nih.gov/factsheets/WYNTK-Consumer/ (accessed August 2022).
- 6. Stierman B, Mishra S, Gahche JJ et al. (2020) Dietary supplement use in children and adolescents aged ≤19 years – United States, 2017–2018. MMWR Morb Mortal Wkly Rep 69, 1557–1562. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7. Ishitsuka K, Sasaki S, Mezawa H et al. (2021) Dietary supplement use in elementary school children: a Japanese web-based survey. Environ Health Prev Med 26, 63. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8. Yoon JY, Park HA, Kang JH et al. (2012) Prevalence of dietary supplement use in Korean children and adolescents: insights from Korea national health and nutrition examination survey 2007–2009. J Korean Med Sci 27, 512–517. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9. Sicińska E, Pietruszka B, Januszko O et al. (2019) Different socio-demographic and lifestyle factors can determine the dietary supplement use in children and adolescents in central-eastern Poland. Nutrients 11, 658. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10. O’Brien SK, Malacova E, Sherriff JL et al. (2017) The prevalence and predictors of dietary supplement use in the Australian population. Nutrients 9, 1154. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11. Murphy J (2020) Top Vitamins and Supplements in 2020 | MDLinx. https://www.mdlinx.com/article/top-vitamins-and-supplements-in-2020/1x034atzR5XSk5FHhFg0Mt (accessed April 2022).
- 12. ConsumerLab. (2019) CBD and Collagen Rise in Popularity, as Probiotics and Coconut Oil Dip in Latest ConsumerLab Survey of Supplement Users. https://www.consumerlab.com/news/cbd-collagen-supplements-rise-in-popularity/02-24-2019/ (accessed April 2022).
- 13. Gardiner P, Buettner C, Davis RB et al. (2008) Factors and common conditions associated with adolescent dietary supplement use: an analysis of the national health and nutrition examination survey (NHANES). BMC Complement Altern Med 8, 9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14. Islam M, Hasan MDT, Al-Fuad MDS et al. (2018) Dietary supplements use and associated determinants among adult population in Southern Bangladesh. Am J Food Sci Nutr Res 5, 64–70. [Google Scholar]
- 15. Jahan I, Uddin ABMN, Reza ASMA et al. (2021) Tendencies and attitudes towards dietary supplements use among undergraduate female students in Bangladesh. PLoS ONE 16, e0249897. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16. Mori N, Kubota M, Hamada S et al. (2011) Prevalence and characterization of supplement use among healthy children and adolescents in an urban Japanese city. Health 3, 135–140. [Google Scholar]
- 17. Bell A, Dorsch KD, Mccreary DR et al. (2004) A look at nutritional supplement use in adolescents. J Adolesc Health 34, 508–516. [DOI] [PubMed] [Google Scholar]
- 18. Chen S, Binns CW, Maycock B et al. (2014) Prevalence of dietary supplement use in healthy pre-school Chinese children in Australia and China. Nutrients 6, 815–828. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19. Dwyer J, Nahin RL, Rogers GT et al. (2013) Prevalence and predictors of children’s dietary supplement use: the 2007 national health interview survey. Am J Clin Nutr 97, 1331–1337. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20. Sichert-Hellert W & Kersting M (2004) Vitamin and mineral supplements use in German children and adolescents between 1986 and 2003: results of the DONALD study. Ann Nutr Metab 48, 414–419. [DOI] [PubMed] [Google Scholar]
- 21. Sirico F, Miressi S, Castaldo C et al. (2018) Habits and beliefs related to food supplements: results of a survey among Italian students of different education fields and levels. PLoS ONE 13, e0191424. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22. Dwyer JT, Coates PM & Smith MJ (2018) Dietary supplements: regulatory challenges and research resources. Nutrients 10, 41. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23. Rooney MR, Harnack L, Michos ED et al. (2017) Trends in use of high-dose vitamin D supplements exceeding 1000 or 4000 international units daily, 1999–2014. JAMA 317, 2448–2450. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24. Or F, Kim Y, Simms J et al. (2019) Taking stock of dietary supplements’ harmful effects on children, adolescents, and young adults. J Adolesc Health 65, 455–461. [DOI] [PubMed] [Google Scholar]
- 25. Shaikh U, Byrd RS & Auinger P (2009) Vitamin and mineral supplement use by children and adolescents in the 1999–2004 national health and nutrition examination survey: relationship with nutrition, food security, physical activity, and health care access. Arch Pediatr Adolesc Med 163, 150–157. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26. Ishihara J, Sobue T, Yamamoto S et al. (2003) Demographics, lifestyles, health characteristics, and dietary intake among dietary supplement users in Japan. Int J Epidemiol 32, 546–553. [DOI] [PubMed] [Google Scholar]