

Abstract
Background
Studies on disease burden in Taiwan are lacking. We aimed to quantify the burden of cardiovascular disease (CVD) attributable to high body mass index (BMI) in Taiwan.
Methods
Using a comparative risk assessment approach from the Global Burden of Disease study, we estimated the population attributable fraction (PAF), attributable CVD burden, and disability-adjusted life years (DALYs) according to sex, age, and area of residence in Taiwan. The BMI distribution for the population was obtained from the National Health Interview Survey in 2013. CVD was defined as an ischemic heart disease or stroke.
Results
The attributable PAF for CVD from high BMI was 18.0% (19.6% in men and 15.6% in women), and it was highest (42.7%) in those aged 25-30 years. Adults aged 60-65 years had the highest absolute DALYs (11,546). The average relative age-standardized attributable burden was 314 DALYs per 100,000 person-years, and it was highest in those aged 75-80 years (1,407 DALYs per 100,000 person-years). Those living in Taitung County had the highest PAF of 21.9% and the highest age-standardized attributable burden (412 DALYs).
Conclusions
In Taiwan, an 18% reduction in CVDs could be achieved if obesity/overweight was prevented. Prevention was most effective in early adulthood. The absolute CVD burden from obesity/overweight was highest in middle-aged men, and the relative burden was highest in older adults. Resource allocation in targeted populations and specific areas to eliminate CVD and health inequities is urgently required.
Keywords: Attributable disease burden, Cardiovascular disease, Comparative risk assessment, High body mass index, Population attributable fraction
Abbreviations
BMI, Body mass index
CRA, Comparative risk assessment
CVD, Cardiovascular disease
DALY, Disability-adjusted life years
GBD, Global Burden of Disease
IHD, Ischemic heart disease
NHIRD, National Health Insurance Research Database
NHIS, National Health Interview Survey
PAF, Population attributable fraction
pys, Person-years
RR, Relative risk
SD, Standard deviation
UI, Uncertainty interval
YLD, Years lived with disability
YLL, Years of life lost
BACKGROUND
Obesity and overweight have reached epidemic levels worldwide and contribute to substantial cardiovascular disease (CVD) and other health risks.1 CVDs include ischemic heart disease (IHD), stroke, and other heart diseases,2 and IHD and ischemic stroke account for approximately 50% and 17.7% of CVD deaths, respectively.3 CVD deaths increased from 1990 to 2019 and remain the leading cause of mortality worldwide.3 Among CVD risk factors, obesity plays a role in the direct structural and functional adaptations of the cardiovascular system, and it acts as an indirect mediator of other co-existing risk factors.4 Globally, CVD burden attributable to obesity/overweight or high body mass index (BMI) has been increasing over the past three decades.5 Compared to China, Japan, Singapore, and South Korea, Taiwan has the highest age-standardized disability-adjusted life years (DALYs) attributable to high BMI compared to other CVD risk factors.5 Reasons for the high BMI attributed to more CVD burden than other risk factors in Taiwan merit further exploration. The prevalence of high BMI is known to vary with sex, age, income, and education.6 Publications on detailed demographics and geographic differences in BMI in Taiwan are lacking. To compare these differences, we used comparative quantified estimation to illustrate the CVD burden attributed to a high BMI in Taiwan.
The Global Burden of Disease (GBD) Study, conducted by the Institute of Health Metrics and Evaluation, provides a systematic, scientific effort to periodically quantify the comparative magnitude of health loss.7 The GBD study includes estimates from 154 countries, 87 risk factors, 286 causes of death, and 3,228 sequelae.7 DALYs is a summary measurement to sum the years of life lost (YLLs) and years lived with disability (YLDs), which represent premature death and disability from a certain health condition.8 To measure a certain risk factor, we assessed the population attributable fraction (PAF) and attributable burden. PAF was defined as the proportional reduction in mortality or morbidity that would occur if past population exposure to a risk factor was reduced to a counterfactual condition. The attributable burden was defined as the disease burden that would occur if exposure had been shifted to an alternative exposure.
In the GBD geographical framework, the estimates for 204 countries were hierarchically grouped into 21 regions, seven super-regions, and globally. In Bayesian modeling of the GBD framework, a higher geographical hierarchy of "region-level" data were prior assumptions and would be the posterior best estimates if the lower "country-level" data were lacking. In the GBD framework, Taiwan, China, and South Korea were categorized in East Asia rather than in the high-income Asia Pacific due to political concerns.7 Thus, incorrect conclusions9 due to inappropriate region-level prior assumptions occurred. However, a large amount of country-level data from periodic population-based health surveys and universal health insurance is readily available.10 Thus, to reflect the health outcomes in Taiwan, this study aimed to quantify the PAF and attributable CVD burden due to high BMI using the GBD framework. We also aimed to compare disease burden between different sex, age, and geographic area groups to identify the most susceptible populations for resource allocation and policy making.
METHODS
Using the comparative risk assessment (CRA) approach from the GBD study,11 we quantified the PAF and CVD disease burden related to high BMI. PAF was a function of the prevalence of exposure (high BMI) and relative risk (RR) for the association between high BMI and CVD. We used National Health Interview Survey (NHIS) data to estimate the prevalence, and used the RR derived from GBD study in 2015.12 The prevalence of high BMI among adults aged ≥ 20 years in Taiwan was obtained from the NHIS in 2013. Details of these surveys have been published elsewhere.13 The study was conducted in accordance with the Declaration of Helsinki and was approved under exempt review procedures by the Institutional Review Board of National Taiwan University Hospital (approval number: 201808105RINC). The need for informed consent statements and consent to participate was waived. To estimate the entire population, the BMI distribution and number of participants were weighted by the sampling rate of each geographic area. High BMI was defined as BMI ≥ 24 kg/m2 according to the Bureau of Health Promotion, Department of Health, Taiwan.14 The composite outcome, CVD, was defined as IHD or ischemic stroke. The RR associated with a change in five units of BMI in five-year age groups for IHD and ischemic stroke was derived from the GBD study in 201512 (shown in Supplementary Table 1). We set the theoretical minimum risk exposure BMI distribution at 21 ± 1 kg/ m2 according to previous literature reviews.15
The burden of CVD was assessed according to the number of deaths, YLL, YLD, and DALYs in the GBD modeling strategies as published elsewhere.8 YLLs were obtained by subtracting the reference life expectancy from the age at CVD death. YLDs were calculated from the point prevalence of CVD, severity of each disease, and corresponding disability weight. In Taiwan, using the burden of disease center, the total disease burden was estimated annually through the Vital Registration and National Health Insurance Research Database (NHIRD) from 2000 to 2015. The cause-specific mortality rates in five-year age groups and GBD life table from the GBD study in 2017 were used to calculate the YLLs. The point prevalence of CVD was defined according to International Classification of Diseases-9 codes 410-414 for IHD, and 433-435 or 437 for ischemic stroke. Prevalent stroke survivors were defined as those with two sequelae: acute and chronic stroke. Acute stroke included first-ever stroke within 30 days, while repeated events were defined as chronic stroke. We estimated the point prevalence (July 1 was assigned as the index date) by sex and the five-year age group. Due to data limitations, the prevalent IHD survivors were not further categorized. The severity of IHD was not assessed. We directly used the severity distribution of ischemic stroke from the GBD study. Disability weights ranged between 0 and 1, where 0 denoted no disability (symptom, limitation, or loss of health), and 1 denoted a life value equal to death. Supplementary Table 2 presents the disability weights of each stroke sequela adopted from the GBD study in 2017.16 To consider comorbidities, a microsimulation method that assumed independent probabilities of comorbid diseases was used.17 The total disability weight of the people who had both IHD and stroke would be less than the sum of each disability weight.
We presented the absolute attributable disease burden from a high BMI to reveal the current condition, calculated by multiplying the PAF of high BMI by the total number of disease burdens. Since little geographical data were misclassified through the administrative process in 2013 and 2014 in the NHIRD, we multiplied the PAF in 2013 by the total disease burden estimated in 2015. We also presented the relative disease burden for every 100,000 person-years (pys) to facilitate comparisons. We calculated the relative attributable age-standardized disease burden per 100,000 pys using the standard population reported in the 2017 GBD study.
The confidence interval through 1,000 samplings of the entire population was not available. We reported point estimates and 95% uncertainty intervals (UIs). UIs were calculated from 1,000 draw-level estimates for each RR, and 95% UIs were defined by the 2.5th and 97.5th percentiles of the ordered 1,000 estimates. We analyzed the overall and disease burden, every five-year age group, sex, and geographic area-specific PAF. We also reported both the absolute and relative attributable burdens. To evaluate time trends, we performed further analyses using the prevalence of high BMI from the NHIS in 2009 and 2005 to calculate the PAF and the disease burden of the corresponding year to calculate the attributable burden. The Guidelines for Accurate and Transparent Health Estimates Reporting checklist of information that should be included in reports of global health estimates is shown in Supplementary Table 3.
RESULTS
The key findings of the study are shown in the Central Illustration. The distributions of sex, age, and geographic area-specific BMI are shown in Supplementary Table 4. A total of 23,158.90 weighted participants in the NHIS, with an average of 32.59 weighted participants to represent the entire population in 20 specific areas according to the sampling rate, were presented. The overall mean BMI standard deviation (SD) was 22.89 (2.55) kg/m2 in 2013 in Taiwan. A weighted 11770.68 men and 11388.22 women had mean (SD) BMIs of 23.56 (2.36) kg/m2 and 22.19 (2.12) kg/m2, respectively. The average BMI gradually increased with age before 60 years and was highest at 24.54 to 24.60 kg/m2 in those aged 55-70 years. The mean BMI was highest in Taitung County, Hualien County, and Keelung City at 23.87, 23.23, and 23.23 kg/m2, respectively. The top three high BMI populations in Taiwan were men aged 35-40 years who lived in Taitung County, men aged 25-30 years who lived in Taitung County, and women aged 75-80 years who lived in Hualien County, at 28.34, 27.77, and 26.92 kg/m2, respectively. Supplementary Table 1 shows the RRs associated with a change in five units of BMI in five-year age groups for IHD and ischemic stroke. The RR for ischemic stroke was highest in the 20-30 age group and decreased with age. Those under 70 years of age had a higher RR for IHD than ischemic stroke, and those aged > 70 years had a higher RR of ischemic stroke than IHD.
Central Illustration.

The PAF and CVD burden in Taiwan.
Table 1 shows that the overall attributable PAF for CVD from high BMI was 18.0% (95% UI 13.5, 21.9). The PAF for IHD from high BMI was higher (19.7%) compared to that of ischemia stroke (15.4%). The PAF for CVD in men with high BMI was higher (19.6%) compared to that in women (15.6%). The absolute attributable CVD burden from a high BMI was 73,745 DALYs, including 39,481 YLLs and 34,265 YLDs. The relative age-standardized attributable burden was 314 DALYs per 100,000 pys, including 168 YLLs and 146 YLDs. The age-standardized attributable IHD burden due to high BMI was higher compared to that due to ischemic stroke (135 vs. 73 DALYs per 100,000 pys). Both CVD and IHD had higher YLLs than YLDs, and stroke had higher YLDs than YLLs.
Table 1. Population attributable fractions and age-standardized cardiovascular disease burdens attributable to high body mass index.
| Disease | Sex | PAF (%) | Numbers | Age-standardized attributable burdens (per 100,000 person years) | ||||||
| Deaths | YLLs | YLDs | DALYs | Deaths | YLLs | YLDs | DALYs | |||
| Cardiovascular disease | Both | 18.0 [13.5, 21.9] | 2338 [1660, 2963] | 39481 [29987, 47910] | 34265 [25556, 42049] | 73745 [55543, 89959] | 10 [7, 13] | 168 [128, 204] | 146 [109, 179] | 314 [236, 383] |
| Women | 15.6 [11.4, 19.6] | 837 [553, 1103] | 11600 [8387, 14564] | 14331 [10449, 17902] | 25931 [18836, 32466] | 7 [5, 9] | 98 [71, 124] | 122 [89, 152] | 220 [160, 276] | |
| Men | 19.6 [15.0, 23.5] | 1501 [1107, 1860] | 27880 [21600, 33346] | 19934 [15107, 24148] | 47814 [36707, 57493] | 13 [9, 16] | 238 [184, 285] | 170 [129, 206] | 408 [313, 491] | |
| Ischemic heart disease | Both | 19.7 [15.1, 23.8] | 2108 [1517, 2652] | 34086 [26147, 41129] | 13725 [10541, 16509] | 47811 [36688, 57638] | 6 [4, 7] | 96 [73, 116] | 39 [29, 47] | 135 [102, 163] |
| Women | 17.1 [12.7, 21.1] | 747 [504, 974] | 9698 [7136, 12063] | 5589 [4248, 6802] | 15287 [11384, 18866] | 4 [3, 5] | 52 [38, 64] | 30 [22, 37] | 82 [60, 101] | |
| Men | 21.3 [16.6, 25.4] | 1361 [1013, 1678] | 24388 [19011, 29065] | 8136 [6293, 9707] | 32524 [25304, 38772] | 8 [6, 10] | 142 [109, 171] | 48 [36, 57] | 190 [145, 228] | |
| Ischemic stroke | Both | 15.4 [11.2, 19.2] | 230 [143, 311] | 5395 [3840, 6781] | 20539 [15015, 25541] | 25934 [18855, 32322] | 1 [0, 1] | 15 [11, 19] | 58 [42, 72] | 73 [53, 91] |
| Women | 14.0 [9.8, 17.8] | 90 [49, 129] | 1902 [1251, 2501] | 8742[6201, 11099] | 10644 [7452, 13600] | 0 [0, 1] | 10 [7, 14] | 47 [33, 59] | 57 [40, 73] | |
| Men | 16.6 [12.4, 20.4] | 140 [94, 183] | 3493 [2589, 4280] | 11798[8814, 14441] | 15290 [11403, 18721] | 1 [1, 1] | 21 [15, 25] | 69 [51, 85] | 90 [66, 110] |
Presented with point estimates with 95% uncertainty intervals.
DALY, disability adjusted life years; PAF, population attributable fractions; YLD, years of life lost; YLL, years lived with disability.
Figure 1 shows that both men and women had a single peak PAF in early adulthood. Men aged 25-30 years with high BMI even had a peak PAF of 51.5%, compared to 30.9% in women in the same age group. Men had a rapid decrease in PAF with age, whereas women had a relatively stable PAF before 70 years of age. The PAF of both sexes crossed at 60-65 years of age. Figure 2 shows that men aged 60-65 years and women aged 75-80 years had the highest absolute attributable CVD burdens of 7,695 and 4,151 DALYs, respectively. Figure 2 shows that both men and women aged 75-80 years had the highest relative attributable age-standardized CVD burdens of 1,508 and 1,327 DALYs per 100,000 pys, respectively. The detailed numbers are shown in Supplementary Table 5. The number of YLDs was higher compared to the number of YLLs before 30 years of age, and the number of YLLs exceeded the number of YLDs in those aged 30-60 years.
Figure 1.

The population attributable fractions attributable to high body mass index for cardiovascular disease.
Figure 2.

The cardiovascular disease burdens attributable to high body mass index in the different age groups. DALY, disability-adjusted life year. The scale of the bar chart is on the left axis and the scale of the line chart is on the right axis.
Figure 3 shows the PAF for CVD due to high BMI in different geographical areas in Taiwan. The average PAF was approximately 17-18% in most areas. However, it was particularly high at 21.9% in Taitung County, followed by New Taipei City (19.8%) and Taoyuan City (19.6%). Figure 4 shows the age-standardized attributable CVD burden due to high BMI in different geographical areas. The population with high BMI who lived in Taitung County had an almost two-fold relative attributable CVD burden compared to the other areas (412 DALYs vs. 200-250 DALYs per 100,000 pys), and it was much higher than the second highest area, Pingtung County at 261 DALYs per 100,000 pys. Detailed numbers are shown in Supplementary Table 6.
Figure 3.
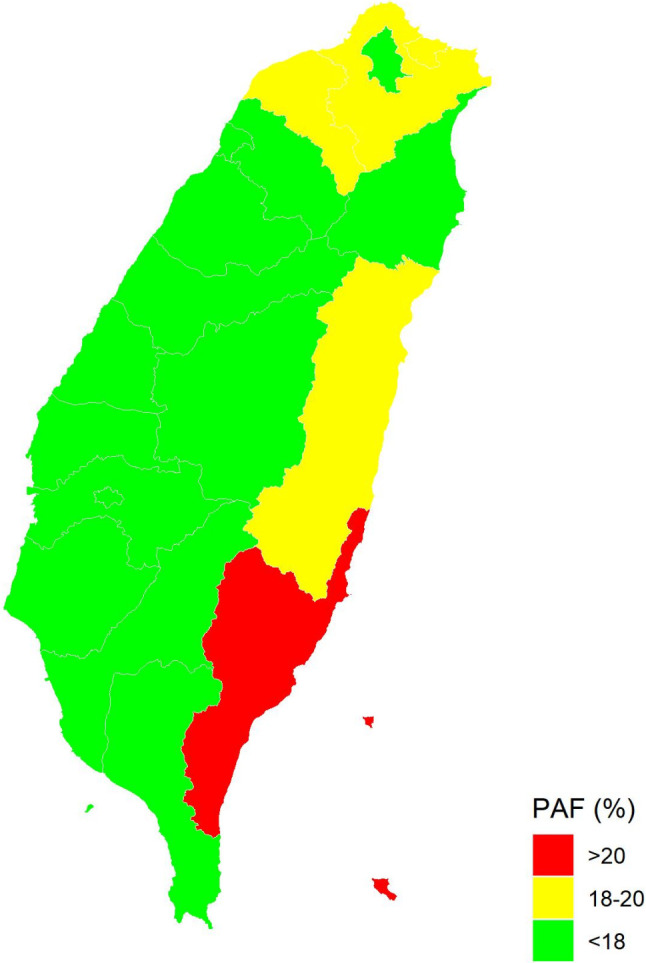
The population attributable fractions due to high body mass index in the different geographic areas in Taiwan. PAF, population attributable fractions. The red areas are Taitung County, and the yellow areas are New Taipei City, Taoyuan City, and Hualien County.
Figure 4.
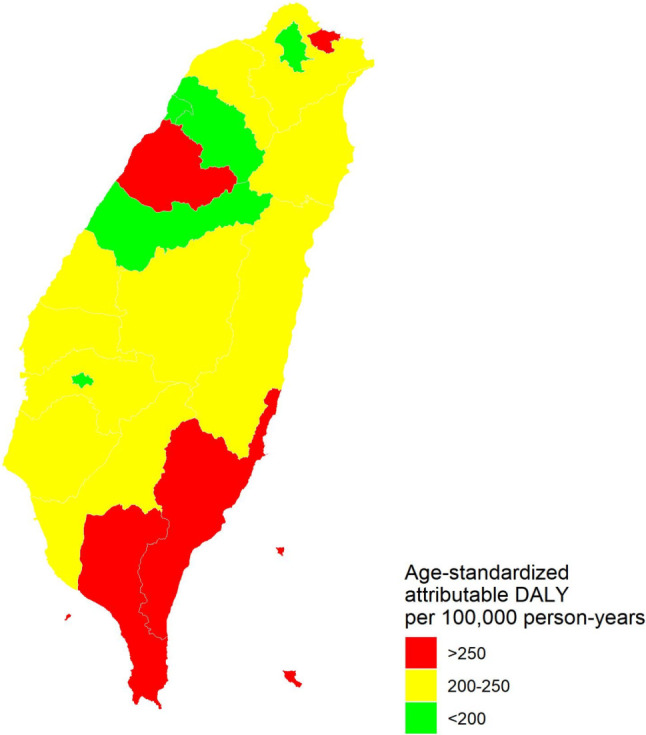
The age-standardized attributable disability adjusted life year due to high body mass index in Taiwan. DALY, disability adjusted life year. The red areas are Taitung County, Pingtung County, and Miaoli County, and the green areas are Taipei City, Hsinchu City, Taichung City, and Chiayi City.
The PAF of CVD due to high BMI was stable in 2005, 2009, and 2013 at 18.4%, 18.0%, and 18.0%, respectively. Similarly, men had a higher PAF of CVD due to high BMI compared to women, and the PAF of IHD due to high BMI was higher compared to that of ischemic stroke. The absolute attributable CVD burden due to high BMI increased by 54,021, 60,173, and 73,745 DALYs in 2005, 2009, and 2013, respectively. The relative age-standardized attributable CVD burden due to high BMI also increased at 237, 260, and 314 DALYs per 100,000 pys in 2005, 2009, and 2013, respectively. Detailed numbers are shown in Supplementary Table 7.
DISCUSSION
Our results showed that an 18.0% reduction in CVD mortality and morbidity could be achieved if high BMI was reduced to a counterfactual condition. High BMI played a greater role in IHD compared to ischemic stroke, and men with high BMI were associated with a higher CVD burden compared to women. Young adults aged 25-30 years had the highest PAF for CVD based on a high BMI. Our results highlight the importance of early obesity/overweight prevention in young men, which would result in a reduction in future IHD. The middle-aged population contributed the most to CVD-related absolute premature deaths and disability attributed to obesity/ overweight. Older adults had the highest relative CVD disease burden. We also found disproportionally high PAFs and attributable CVD burden from high BMI in certain areas in Taiwan.
Globally, the PAFs attributed to IHD and ischemic stroke from high BMI were 16-17% and 9-10%, respectively in 2010, which increased to 22.7% and 17.7% in 2017, respectively.18,19 Our study revealed a relatively stable trend in PAF and a similar increasing trend in CVD burden from 2005 to 2013. Adults aged 30-35 and 30-40 years had the highest PAF for IHD and stroke from a high BMI, respectively.19 We observed a similar PAF peak in early adulthood, which confirmed that early obesity/ overweight prevention should be emphasized. Generally, both sexes had similar PAF globally. The PAF attributed to IHD from high BMI was 16% in men and 17% in women, and that from ischemic stroke was 10% in men and 9% in women.19 Regionally, our estimates are more compatible with those of the high-income Asian Pacific area with regards to sex differences, in that men had a higher PAF of CVD compared to women with high BMI, and the PAFs of IHD from high BMI and stroke were 14.9/10.8% and 18.1/14.9% in men/women, respectively. In contrast, in East Asia, the PAF of IHD has been reported to be similar in both sexes at 15.6%, with an even higher PAF of stroke in women (20.0%) than in men (18.7%).19,20 Additionally, the mean BMI in Taiwan is closer to that in Asia Pacific than in East Asia.21 Furthermore, the ratio of observed to expected age-standardized rates of DALYs of stroke was lower than one, which is similar to that in Japan, Singapore, and South Korea. However, it is different to China, where the ratio has been reported to be higher than one.22 We provide evidence that better re-classification in geographical hierarchy in the GBD framework is needed.
The mechanisms of obesity and CVD are well known.23 However, reasons for the crossover of attributable DALY rate in both sexes aged 70-80 years are not completely understood.19 However, it may be associated with the higher prevalence of obesity in older women, and the physiological effect of a decrease in estrogen with age.6,24 Globally, the prevalence of obesity is inversely associated with household income and educational level.25 In Taiwan, Taitung County has the fewest residents, highest proportion of indigenous people, and highest prevalence of obesity.26 Ethnic differences in indigenous populations have been reported to be related to metabolic syndrome.27 Uneven distribution density of medical services28 and relatively low socioeconomic status have been shown to contribute to the highest standardized mortality, lowest disability-free life expectancy at birth, and highest CVD burden attributed to obesity/overweight in Taitung.26
We provide prospective evidence that authoritative interventions are required to tackle obesity prevention and treatment along with health inequalities. Identifying those at risk from obesity/overweight and encouraging individuals to take responsibility for their own health is important.
To the best of our knowledge, this is the first study to use the framework of the GBD study to analyze data from Taiwan. As a strength, our study used representative population-based primary data from Taiwan and ascertained the outcomes using the official National Death Registry and NHIRD, which covers 99.9% of the Taiwanese population.30 However, this study also has some limitations. First, current data on the prevalence of high BMI were not available due to the limitations of our database. We performed further analyses in 2005 and 2009 to ensure the robustness of our results in 2013. Second, the CRA framework of the GBD did not involve underweight adults. However, the risk factors and outcomes of underweight children and adults were not of interest in this study. Finally, CVD in our study was defined as IHD or ischemic stroke, which is more valid in the NHIRD database and accounted for 70% of total CVD burden. Further exploration of other risk factors and outcomes is warranted.
CONCLUSIONS
In conclusion, an approximate 18% reduction in CVD-related premature deaths and disabilities could be achieved if obesity/overweight are successfully prevented in Taiwan. The absolute health burden of obesity/overweight was highest in middle-aged men, and the relative burden was highest in older adults. Taiwan has a disproportionally high CVD burden from obesity/overweight in specific areas. To reduce CVD, awareness of health inequities and adequate resource allocation is urgently required.
DECLARATION OF CONFLICT OF INTEREST
All the authors declare no conflict of interest.
SUPPLEMENTARY MATERIALS
Supplementary Table 1. Relative risks used by age for ischemic heart disease and ischemic stroke for high body mass index in adults for both sex and for both morbidity and mortality.
| Risk – Outcome | Category/units | 20-24 years | 25-29 years | 30-34 years | 35-39 years | 40-44 years | 45-49 years | 50-54 years | 55-59 years | 60-64 years | 65-69 years | 70-74 years | 75-79 years | 80-84 years | 85+ years |
| Ischemic heart disease | 5 kg/m2 | 2.274 (1.259 to 3.683) | 2.274 (1.259 to 3.683) | 2.018 (1.3 to 3.099) | 1.724 (1.533 to 1.93) | 1.599 (1.418 to 1.784) | 1.567 (1.458 to 1.68) | 1.52 (1.417 to 1.631) | 1.466 (1.372 to 1.557) | 1.414 (1.325 to 1.504) | 1.364 (1.287 to 1.448) | 1.319 (1.242 to 1.4) | 1.274 (1.187 to 1.365) | 1.17 (1.091 to 1.252) | 1.17 (1.091 to 1.252) |
| Ischemic stroke | 5 kg/m2 | 2.472 (1.4 to 3.975) | 2.472 (1.4 to 3.975) | 2.235 (1.457 to 3.329) | 1.979 (1.699 to 2.313) | 1.826 (1.6 to 2.075) | 1.733 (1.581 to 1.898) | 1.635 (1.479 to 1.795) | 1.543 (1.441 to 1.653) | 1.455 (1.345 to 1.566) | 1.38 (1.31 to 1.458) | 1.304 (1.234 to 1.376) | 1.228 (1.16 to 1.304) | 1.068 (0.992 to 1.143) | 1.068 (0.992 to 1.143) |
Reference from: "Global Burden of Disease Study 2019 Data Resources." from http://ghdx.healthdata.org/gbd-2019.
Supplementary Table 2. The disability weight and lay description of stroke in our study.
| Health state | Lay description | Disability weight |
| Stroke: long-term consequences, mild | The patient has some difficulty in moving around and some weakness in one hand, but is able to walk without help. | 0.019 (0.010-0.032) |
| Stroke: long-term consequences, moderate | The patient has some difficulty in moving around, and in using the hands for lifting and holding things, dressing and grooming. | 0.070 (0.046-0.099) |
| Stroke: long-term consequences, moderate plus cognition problems | The patient has some difficulty in moving around, in using the hands for lifting and holding things, dressing and grooming, and in speaking. The person is often forgetful and confused. | 0.316 (0.206-0.437) |
| Stroke: long-term consequences, severe | The patient is confined to bed or a wheelchair, has difficulty speaking and depends on others for feeding, toileting and dressing. | 0.552 (0.377-0.707) |
| Stroke: long-term consequences, severe plus cognition problems | The patient is confined to bed or a wheelchair, depends on others for feeding, toileting and dressing, and has difficulty speaking, thinking clearly and remembering things. | 0.588 (0.411-0.744) |
Reference from: 2017 GBD study.1
Supplementary Table 3. GATHER checklist of information that should be included in reports of global health estimates.
| # | Checklist item | Section/paragraph/interpretation |
| Objectives and funding | ||
| 1 | Define the indicators, populations, and time periods for which estimates were made. | Methods/1st paragraph |
| 2 | List the funding sources for the work. | Abstract. Funding supports from Taiwan Ministry of Education (grant number: 107L891601-107L891607, 108L891601-108L891607, 109L891601-109L891607) |
| Data Inputs | ||
| For all data inputs from multiple sources that are synthesized as part of the study: | ||
| 3 | Describe how the data were identified and how the data were accessed. | Methods/1st and 2nd paragraph |
| 4 | Specify the inclusion and exclusion criteria. Identify all ad-hoc exclusions. | Methods/4th paragraph |
| 5 | Provide information on all included data sources and their main characteristics. For each data source used, report reference information or contact name/institution, population represented, data collection method, year(s) of data collection, sex and age range, diagnostic criteria or measurement method, and sample size, as relevant. | Methods/supplement |
| 6 | Identify and describe any categories of input data that have potentially important biases (e.g., based on characteristics listed in item 5). | Methods |
| For data inputs that contribute to the analysis but were not synthesized as part of the study: | ||
| 7 | Describe and give sources for any other data inputs. | All data inputs were mentioned as above. |
| For all data inputs: | ||
| 8 | Provide all data inputs in a file format from which data can be efficiently extracted (e.g., a spreadsheet as opposed to a PDF), including all relevant meta-data listed in item 5. For any data inputs that cannot be shared due to ethical or legal reasons, such as third-party ownership, provide a contact name or the name of the institution that retains the right to the data. | Acknowledgments. The datasets generated and/or analyzed during the current study are not publicly available due to the terms of consent to which the participants agreed but data are however available from the authors upon reasonable request and with permission of the Health Promotion Administration at the Ministry of Health and Welfare in Taiwan. |
| Data analysis | ||
| 9 | Provide a conceptual overview of the data analysis method. A diagram may be helpful. | Flow diagrams of the overall methodological processes were available online (http://ghdx.healthdata.org/gbd-2019/code) |
| 10 | Provide a detailed description of all steps of the analysis, including mathematical formulae. This description should cover, as relevant, data cleaning, data pre-processing, data adjustments and weighting of data sources, and mathematical or statistical model(s). | Methods/1st and 4th paragraph |
| 11 | Describe how candidate models were evaluated and how the final model(s) were selected. | Methods/1st and 2nd paragraph |
| 12 | Provide the results of an evaluation of model performance, if done, as well as the results of any relevant sensitivity analysis. | Methods/4th paragraph |
| 13 | Describe methods for calculating uncertainty of the estimates. State which sources of uncertainty were, and were not, accounted for in the uncertainty analysis. | Methods/4th paragraph |
| 14 | State how analytic or statistical source code used to generate estimates can be accessed. | Supplement |
| Results and discussion | ||
| 15 | Provide published estimates in a file format from which data can be efficiently extracted. | Results and supplement |
| 16 | Report a quantitative measure of the uncertainty of the estimates (e.g. uncertainty intervals). | Results and supplement |
| 17 | Interpret results in light of existing evidence. If updating a previous set of estimates, describe the reasons for changes in estimates. | Discussion, paragraphs 1-3 |
| 18 | Discuss limitations of the estimates. Include a discussion of any modelling assumptions or data limitations that affect interpretation of the estimates. | Discussion, paragraph 4 |
Supplementary Table 4. The distribution of sex-, age- and geographic area-specific body mass index.
| City | Sex | n | 20-25 | n | 25-30 | n | 30-35 | n | 35-40 | n | 40-45 | n | 45-50 | n | 50-55 | n | 55-60 | n | 60-65 | n | 65-70 | n | 70-75 | n | 75-80 | n | ≥ 80 |
| Changhua County | Men | 34 | 22 (3) | 40 | 24 (4) | 46 | 25 (4) | 38 | 26 (4) | 36 | 26 (6) | 35 | 25 (4) | 38 | 26 (3) | 34 | 25 (3) | 27 | 24 (3) | 16 | 25 (3) | 15 | 22 (3) | 11 | 24 (3) | 6 | 23 (2) |
| Women | 32 | 20 (3) | 36 | 22 (5) | 40 | 24 (5) | 36 | 24 (4) | 35 | 24 (4) | 36 | 23 (3) | 38 | 25 (3) | 36 | 24 (3) | 25 | 24 (4) | 14 | 26 (2) | 16 | 25 (4) | 11 | 26 (4) | 13 | 23 (5) | |
| Chiayi City | Men | 26 | 25 (4) | 28 | 24 (3) | 30 | 25 (3) | 28 | 25 (5) | 29 | 24 (3) | 31 | 25 (4) | 31 | 26 (3) | 27 | 26 (3) | 22 | 25 (3) | 13 | 25 (4) | 11 | 23 (4) | 9 | 24 (3) | 11 | 22 (2) |
| Women | 22 | 20 (2) | 28 | 21 (4) | 31 | 20 (3) | 32 | 22 (4) | 35 | 24 (4) | 39 | 23 (3) | 30 | 23 (3) | 28 | 24 (3) | 22 | 23 (3) | 14 | 24 (3) | 14 | 25 (4) | 11 | 25 (5) | 11 | 23 (3) | |
| Chiayi County | Men | 32 | 23 (4) | 34 | 25 (6) | 34 | 23 (3) | 40 | 26 (4) | 42 | 25 (4) | 46 | 24 (3) | 44 | 25 (3) | 36 | 26 (3) | 30 | 23 (4) | 18 | 25 (2) | 19 | 24 (3) | 15 | 26 (4) | 14 | 23 (4) |
| Women | 31 | 22 (3) | 27 | 21 (3) | 42 | 22 (4) | 36 | 23 (4) | 34 | 23 (3) | 32 | 23 (3) | 37 | 25 (6) | 34 | 25 (5) | 28 | 26 (3) | 14 | 26 (3) | 17 | 23 (3) | 12 | 23 (4) | 10 | 21 (3) | |
| Hsinchu City | Men | 31 | 25 (4) | 35 | 24 (4) | 44 | 25 (4) | 43 | 26 (3) | 38 | 25 (4) | 37 | 25 (3) | 32 | 24 (4) | 25 | 25 (3) | 18 | 25 (3) | 11 | 23 (3) | 9 | 24 (3) | 6 | 23 (4) | 12 | 24 (2) |
| Women | 31 | 21 (3) | 31 | 22 (4) | 44 | 21 (3) | 44 | 22 (4) | 42 | 23 (4) | 33 | 23 (3) | 31 | 24 (3) | 28 | 23 (3) | 21 | 23 (4) | 13 | 26 (5) | 11 | 24 (4) | 9 | 24 (2) | 10 | 25 (4) | |
| Hsinchu County | Men | 34 | 23 (4) | 35 | 25 (5) | 41 | 24 (3) | 45 | 26 (4) | 40 | 26 (4) | 40 | 24 (4) | 36 | 25 (3) | 29 | 24 (3) | 21 | 25 (3) | 14 | 25 (3) | 15 | 25 (2) | 12 | 23 (3) | 14 | 22 (4) |
| Women | 30 | 20 (3) | 24 | 21 (4) | 48 | 24 (5) | 46 | 22 (3) | 39 | 24 (3) | 35 | 23 (3) | 30 | 23 (3) | 26 | 24 (3) | 24 | 24 (4) | 14 | 24 (4) | 14 | 24 (3) | 11 | 23 (3) | 13 | 26 (5) | |
| Hualien County | Men | 28 | 24 (5) | 23 | 26 (5) | 34 | 26 (3) | 35 | 26 (5) | 35 | 25 (4) | 38 | 24 (3) | 36 | 25 (4) | 30 | 26 (3) | 26 | 25 (4) | 16 | 25 (3) | 12 | 24 (2) | 7 | 23 (3) | 17 | 23 (4) |
| Women | 28 | 22 (3) | 30 | 22 (4) | 34 | 24 (5) | 30 | 23 (5) | 34 | 24 (7) | 31 | 24 (4) | 35 | 24 (4) | 32 | 24 (4) | 25 | 26 (3) | 16 | 24 (4) | 16 | 24 (4) | 10 | 27 (5) | 12 | 24 (4) | |
| Kaohsiung City | Men | 84 | 24 (5) | 76 | 25 (5) | 103 | 26 (4) | 91 | 26 (5) | 91 | 25 (3) | 96 | 25 (4) | 89 | 25 (3) | 83 | 25 (3) | 66 | 24 (3) | 42 | 23 (3) | 27 | 25 (3) | 20 | 23 (3) | 24 | 24 (3) |
| Women | 77 | 21 (3) | 80 | 23 (4) | 92 | 22 (4) | 94 | 22 (3) | 89 | 23 (4) | 92 | 24 (4) | 95 | 24 (3) | 84 | 24 (4) | 71 | 25 (3) | 38 | 25 (3) | 37 | 23 (3) | 20 | 25 (4) | 19 | 23 (4) | |
| Keelung City | Men | 27 | 23 (5) | 30 | 24 (4) | 28 | 24 (3) | 26 | 26 (6) | 33 | 24 (3) | 34 | 25 (3) | 32 | 25 (4) | 30 | 26 (4) | 19 | 25 (3) | 11 | 23 (3) | 11 | 26 (3) | 6 | 24 (2) | 9 | 25 (4) |
| Women | 25 | 22 (3) | 24 | 21 (4) | 29 | 23 (4) | 26 | 23 (3) | 30 | 24 (4) | 34 | 24 (4) | 34 | 24 (3) | 29 | 24 (3) | 24 | 24 (4) | 14 | 24 (3) | 9 | 26 (5) | 9 | 23 (4) | 11 | 24 (3) | |
| Miaoli County | Men | 30 | 24 (4) | 35 | 23 (4) | 36 | 25 (4) | 33 | 24 (4) | 35 | 24 (4) | 31 | 26 (5) | 37 | 26 (3) | 30 | 25 (3) | 22 | 24 (3) | 15 | 25 (3) | 15 | 23 (3) | 12 | 24 (3) | 17 | 23 (3) |
| Women | 30 | 21 (4) | 34 | 22 (3) | 38 | 22 (3) | 32 | 23 (3) | 30 | 23 (3) | 34 | 23 (4) | 32 | 23 (4) | 29 | 22 (3) | 22 | 25 (3) | 14 | 26 (4) | 16 | 26 (3) | 14 | 23 (3) | 19 | 23 (4) | |
| Nantou County | Men | 36 | 23 (4) | 35 | 23 (3) | 38 | 24 (4) | 37 | 25 (3) | 36 | 25 (3) | 39 | 25 (4) | 40 | 24 (4) | 38 | 25 (3) | 28 | 24 (3) | 16 | 25 (4) | 18 | 24 (3) | 13 | 22 (2) | 13 | 24 (3) |
| Women | 29 | 21 (4) | 34 | 20 (2) | 37 | 23 (4) | 32 | 22 (3) | 35 | 23 (3) | 38 | 24 (4) | 39 | 24 (3) | 35 | 24 (4) | 29 | 25 (4) | 17 | 24 (3) | 18 | 25 (4) | 12 | 26 (3) | 18 | 24 (4) | |
| New Taipei City | Men | 61 | 23 (4) | 66 | 26 (5) | 66 | 25 (4) | 58 | 25 (3) | 57 | 26 (4) | 60 | 25 (4) | 53 | 25 (4) | 53 | 25 (4) | 39 | 24 (4) | 18 | 23 (3) | 14 | 23 (3) | 5 | 25 (3) | 13 | 23 (3) |
| Women | 49 | 21 (3) | 56 | 21 (4) | 70 | 22 (4) | 65 | 22 (3) | 56 | 23 (4) | 60 | 22 (4) | 57 | 24 (4) | 46 | 24 (3) | 36 | 25 (4) | 17 | 24 (3) | 15 | 26 (3) | 13 | 26 (3) | 13 | 24 (5) | |
| Penghu County | Men | 29 | 24 (4) | 27 | 23 (4) | 25 | 24 (3) | 28 | 25 (3) | 24 | 24 (3) | 29 | 25 (4) | 28 | 25 (3) | 23 | 24 (4) | 21 | 26 (4) | 12 | 25 (4) | 11 | 24 (3) | 9 | 23 (3) | 12 | 23 (3) |
| Women | 29 | 21 (4) | 22 | 22 (3) | 28 | 23 (3) | 26 | 22 (4) | 25 | 22 (4) | 23 | 23 (3) | 26 | 23 (4) | 19 | 24 (4) | 18 | 24 (3) | 12 | 25 (3) | 9 | 25 (3) | 9 | 25 (3) | 12 | 22 (4) | |
| Pingtung County | Men | 34 | 23 (3) | 32 | 25 (4) | 36 | 25 (4) | 37 | 25 (3) | 39 | 26 (5) | 40 | 25 (4) | 36 | 25 (3) | 37 | 25 (3) | 25 | 25 (3) | 19 | 24 (3) | 17 | 23 (2) | 13 | 23 (3) | 13 | 23 (3) |
| Women | 35 | 21 (4) | 34 | 23 (5) | 35 | 22 (4) | 28 | 23 (4) | 38 | 23 (4) | 37 | 23 (3) | 40 | 25 (3) | 35 | 25 (4) | 29 | 24 (3) | 18 | 25 (4) | 15 | 23 (4) | 13 | 23 (5) | 13 | 23 (4) | |
| Taichung City | Men | 85 | 23 (4) | 86 | 24 (4) | 109 | 25 (4) | 86 | 26 (4) | 91 | 24 (4) | 85 | 25 (4) | 88 | 25 (3) | 69 | 25 (3) | 54 | 24 (4) | 24 | 24 (3) | 24 | 24 (3) | 17 | 25 (3) | 19 | 22 (2) |
| Women | 87 | 21 (4) | 89 | 22 (5) | 103 | 22 (4) | 90 | 22 (4) | 94 | 23 (4) | 91 | 23 (4) | 82 | 24 (3) | 74 | 24 (4) | 57 | 25 (4) | 28 | 25 (4) | 29 | 24 (4) | 18 | 23 (2) | 12 | 24 (3) | |
| Tainan City | Men | 77 | 24 (4) | 77 | 25 (5) | 99 | 25 (4) | 84 | 26 (4) | 71 | 25 (3) | 85 | 25 (3) | 88 | 25 (4) | 75 | 25 (3) | 56 | 24 (3) | 28 | 24 (3) | 31 | 24 (3) | 23 | 23 (3) | 22 | 24 (3) |
| Women | 72 | 21 (4) | 82 | 22 (4) | 88 | 23 (5) | 87 | 22 (4) | 78 | 23 (4) | 84 | 23 (3) | 85 | 24 (4) | 74 | 24 (3) | 57 | 25 (4) | 30 | 25 (6) | 26 | 25 (4) | 24 | 24 (3) | 20 | 22 (3) | |
| Taipei City | Men | 48 | 23 (3) | 61 | 23 (3) | 62 | 25 (4) | 56 | 25 (3) | 52 | 25 (4) | 54 | 26 (5) | 52 | 26 (3) | 49 | 26 (4) | 37 | 25 (3) | 21 | 24 (4) | 17 | 24 (3) | 15 | 23 (3) | 23 | 22 (3) |
| Women | 51 | 20 (2) | 58 | 21 (4) | 75 | 22 (3) | 58 | 22 (4) | 58 | 22 (4) | 54 | 22 (3) | 55 | 23 (3) | 53 | 23 (4) | 43 | 24 (3) | 26 | 25 (4) | 24 | 24 (5) | 12 | 25 (4) | 25 | 24 (4) | |
| Taitung County | Men | 25 | 26 (6) | 18 | 28 (5) | 29 | 26 (5) | 30 | 28 (4) | 32 | 26 (5) | 34 | 26 (3) | 36 | 25 (3) | 31 | 26 (4) | 20 | 26 (4) | 14 | 25 (3) | 12 | 24 (3) | 7 | 22 (2) | 11 | 22 (3) |
| Women | 18 | 21 (3) | 26 | 23 (4) | 25 | 22 (4) | 28 | 24 (5) | 30 | 25 (5) | 25 | 24 (3) | 31 | 25 (3) | 26 | 26 (4) | 19 | 25 (4) | 14 | 24 (5) | 17 | 25 (4) | 6 | 24 (6) | 9 | 25 (2) | |
| Taoyuan City | Men | 51 | 23 (3) | 52 | 24 (5) | 67 | 25 (4) | 53 | 26 (4) | 56 | 25 (3) | 52 | 25 (4) | 47 | 25 (3) | 37 | 24 (3) | 28 | 26 (4) | 15 | 26 (3) | 9 | 25 (3) | 8 | 24 (3) | 13 | 24 (4) |
| Women | 43 | 21 (4) | 42 | 22 (5) | 54 | 22 (3) | 52 | 23 (4) | 49 | 23 (3) | 48 | 24 (3) | 45 | 23 (3) | 40 | 25 (4) | 27 | 25 (4) | 16 | 25 (2) | 18 | 25 (3) | 7 | 25 (2) | 7 | 22 (3) | |
| Yilan County | Men | 27 | 23 (4) | 29 | 25 (5) | 30 | 26 (5) | 31 | 26 (4) | 33 | 26 (3) | 39 | 26 (4) | 34 | 25 (2) | 33 | 26 (3) | 24 | 25 (3) | 13 | 25 (3) | 18 | 25 (3) | 9 | 24 (4) | 9 | 22 (3) |
| Women | 26 | 20 (2) | 28 | 21 (4) | 31 | 22 (4) | 31 | 22 (3) | 32 | 23 (5) | 33 | 23 (3) | 34 | 23 (3) | 30 | 23 (3) | 22 | 26 (3) | 10 | 26 (5) | 12 | 25 (5) | 11 | 23 (3) | 10 | 23 (3) | |
| Yunlin County | Men | 33 | 23 (3) | 30 | 24 (4) | 33 | 24 (4) | 33 | 26 (3) | 35 | 25 (4) | 40 | 24 (3) | 36 | 25 (3) | 26 | 24 (3) | 26 | 25 (3) | 17 | 24 (3) | 18 | 24 (3) | 11 | 25 (4) | 14 | 23 (4) |
| Women | 22 | 21 (5) | 27 | 23 (4) | 32 | 22 (5) | 28 | 21 (3) | 28 | 22 (3) | 28 | 23 (3) | 27 | 25 (4) | 30 | 25 (3) | 24 | 24 (3) | 18 | 25 (3) | 19 | 25 (4) | 16 | 24 (4) | 17 | 23 (5) |
The body mass index was presented by mean (standard deviation) in kg/m2. The results were weighted by the sampling rate of the geographic areas.
Supplementary Table 5. The population attributable fractions and age-specific cardiovascular disease burdens attributable to high body mass index.
| Sex | Age | PAF (%) | Numbers | Age-specific attributable burdens (per 100,000 person-years) | ||||||
| Deaths | YLLs | YLDs | DALYs | Deaths | YLLs | YLDs | DALYs | |||
| Both | 20-25 | 30.1 [0.1, 47.8] | 1 [0, 2] | 69 [0, 111] | 105 [0, 166] | 174 [0, 276] | 0 [0, 0] | 4 [0, 7] | 7 [0, 10] | 11 [0, 17] |
| 25-30 | 42.7 [0.3, 64.0] | 4 [0, 7] | 227 [1, 337] | 253 [2, 382] | 480 [3, 719] | 0 [0, 0] | 14 [0, 21] | 16 [0, 24] | 30 [0, 45] | |
| 30-35 | 39.8 [2.5, 60.2] | 12 [0, 18] | 543 [15, 827] | 482 [51, 723] | 1026 [66, 1551] | 1 [0, 1] | 29 [1, 44] | 25 [3, 38] | 54 [3, 82] | |
| 35-40 | 39.2 [31.2, 46.0] | 38 [30, 44] | 1565 [1249, 1831] | 849 [669, 1000] | 2414 [1918, 2831] | 2 [1, 2] | 77 [62, 90] | 42 [33, 49] | 119 [95, 140] | |
| 40-45 | 33.5 [26.1, 39.9] | 63 [49, 75] | 2355 [1831, 2808] | 1234 [962, 1466] | 3589 [2793, 4274] | 4 [3, 4] | 132 [103, 158] | 69 [54, 82] | 202 [157, 240] | |
| 45-50 | 32.4 [27.6, 36.8] | 109 [93, 123] | 3583 [3053, 4060] | 2075 [1755, 2362] | 5658 [4808, 6422] | 6 [5, 7] | 195 [166, 221] | 113 [95, 128] | 308 [261, 349] | |
| 50-55 | 29.0 [24.1, 33.5] | 149 [124, 170] | 4291 [3593, 4923] | 3274 [2694, 3791] | 7565 [6288, 8713] | 8 [7, 9] | 229 [192, 263] | 175 [144, 203] | 404 [336, 466] | |
| 55-60 | 27.4 [23.2, 31.3] | 214 [181, 245] | 5349 [4530, 6118] | 4715 [4003, 5376] | 10065 [8533, 11494] | 12 [10, 14] | 308 [261, 352] | 271 [230, 309] | 579 [491, 662] | |
| 60-65 | 23.7 [19.4, 27.6] | 268 [222, 310] | 5728 [4740, 6634] | 5818 [4728, 6811] | 11546 [9469, 13446] | 18 [15, 20] | 377 [312, 437] | 383 [311, 448] | 760 [623, 885] | |
| 65-70 | 20.3 [16.6, 23.8] | 219 [177, 258] | 4043 [3267, 4754] | 4826 [3957, 5627] | 8870 [7224, 10380] | 22 [18, 26] | 414 [334, 487] | 494 [405, 576] | 908 [739, 1062] | |
| 70-75 | 17.2 [13.5, 20.6] | 254 [200, 305] | 3714 [2924, 4457] | 4411 [3473, 5288] | 8125 [6397, 9745] | 38 [30, 45] | 551 [433, 661] | 654 [515, 784] | 1205 [948, 1445] | |
| 75-80 | 14.3 [10.1, 18.2] | 349 [244, 446] | 4028 [2821, 5145] | 3857 [2742, 4897] | 7885 [5564, 10042] | 62 [43, 79] | 719 [503, 918] | 688 [489, 874] | 1407 [993, 1791] | |
| 80-85 | 5.6 [2.2, 8.8] | 222 [114, 323] | 1857 [916, 2752] | 1140 [267, 1991] | 2997 [1182, 4743] | 58 [30, 84] | 482 [238, 714] | 296 [69, 517] | 778 [307, 1231] | |
| ≥ 85 | 5.5 [2.1, 8.8] | 438 [226, 638] | 2128 [1047, 3154] | 1225 [252, 2170] | 3353 [1298, 5324] | 128 [66, 187] | 624 [307, 925] | 359 [74, 636] | 983 [381, 1561] | |
| Women | 20-25 | 17.8 [0.1, 30.1] | 0 [0, 0] | 16 [0, 27] | 30 [0, 50] | 46 [0, 77] | 0 [0, 0] | 2 [0, 3] | 4 [0, 7] | 6 [0, 10] |
| 25-30 | 30.9[0.2, 50.0] | 1 [0, 2] | 59 [0, 95] | 88 [1, 142] | 147 [1, 238] | 0 [0, 0] | 8 [0, 12] | 11 [0, 19] | 19 [0, 31] | |
| 30-35 | 26.3 [2.6, 41.4] | 1 [0, 2] | 68 [7, 107] | 139 [14, 220] | 207 [21, 326] | 0 [0, 0] | 7 [1, 11] | 15 [1, 23] | 22 [2, 34] | |
| 35-40 | 23.7 [18.2, 28.7] | 3 [3, 4] | 161 [124, 193] | 202 [154, 245] | 362 [278, 438] | 0 [0, 0] | 16 [12, 19] | 20 [15, 24] | 35 [27, 43] | |
| 40-45 | 23.6 [18.0, 28.6] | 7 [5, 9] | 310 [236, 377] | 314 [240, 379] | 624 [476, 756] | 1 [1, 1] | 34 [26, 42] | 35 [27, 42] | 69 [53, 84] | |
| 45-50 | 22.1 [18.5, 25.5] | 10 [8, 12] | 378 [318, 434] | 507 [423, 583] | 885 [741, 1018] | 1 [1, 1] | 41 [34, 47] | 55 [46, 63] | 96 [80, 110] | |
| 50-55 | 24.3 [20.0, 28.2] | 23 [19, 27] | 751 [623, 870] | 992 [811, 1157] | 1743 [1435, 2027] | 2 [2, 3] | 79 [66, 92] | 105 [86, 122] | 184 [152, 214] | |
| 55-60 | 24.3 [20.5, 27.9] | 34 [28, 39] | 949 [799, 1090] | 1596 [1348, 1825] | 2545 [2147, 2915] | 4 [3, 4] | 107 [90, 123] | 180 [152, 206] | 287 [242, 329] | |
| 60-65 | 24.2 [19.9, 28.2] | 62 [51, 72] | 1499 [1240, 1737] | 2351 [1917, 2755] | 3850 [3157, 4492] | 8 [7, 9] | 191 [158, 222] | 300 [245, 352] | 492 [403, 573] | |
| 65-70 | 22.9 [18.7, 26.8] | 79 [64, 92] | 1598 [1297, 1876] | 2336 [1918, 2720] | 3934 [3215, 4596] | 15 [13, 18] | 313 [254, 368] | 458 [376, 533] | 771 [630, 901] | |
| 70-75 | 19.0 [15.0, 22.8] | 98 [78, 118] | 1589 [1253, 1907] | 2303 [1817, 2758] | 3892 [3070, 4665] | 27 [21, 33] | 440 [347, 528] | 637 [503, 763] | 1077 [849, 1291] | |
| 75-80 | 15.5 [11.0, 19.8] | 163 [114, 208] | 2014 [1412, 2572] | 2137 [1520, 2713] | 4151 [2932, 5285] | 52 [36, 66] | 644 [451, 822] | 683 [486, 867] | 1327 [937, 1689] | |
| 80-85 | 6.1 [2.3, 9.6] | 111 [57, 163] | 1003 [488, 1491] | 651 [152, 1137] | 1654 [639, 2628] | 52 [27, 76] | 469 [228, 697] | 304 [71, 531] | 773 [299, 1228] | |
| ≥ 85 | 6.1 [2.3, 9.7] | 244 [126, 356] | 1206 [590, 1789] | 685 [135, 1217] | 1891 [725, 3006] | 136 [70, 199] | 674 [330, 1000] | 383 [75, 680] | 1057 [405, 1680] | |
| Men | 20-25 | 39.9 [0.0, 61.9] | 1 [0, 2] | 53 [0, 84] | 75 [0, 115] | 128 [0, 199] | 0 [0, 0] | 6 [0, 10] | 9 [0, 14] | 15 [0, 24] |
| 25-30 | 51.5 [0.4, 74.4] | 3 [0, 5] | 169 [1, 242] | 164 [1, 239] | 333 [2, 481] | 0 [0, 1] | 21 [0, 30] | 20 [0, 29] | 41 [0, 59] | |
| 30-35 | 45.8 [2.5, 68.6] | 11 [0, 16] | 475 [8, 721] | 343 [37, 504] | 818 [45, 1224] | 1 [0, 2] | 50 [1, 76] | 36 [4, 53] | 86 [5, 129] | |
| 35-40 | 44.3 [35.4, 51.7] | 34 [27, 40] | 1404 [1125, 1637] | 647 [515, 755] | 2051 [1640, 2393] | 3 [3, 4] | 140 [112, 163] | 64 [51, 75] | 204 [163, 238] | |
| 40-45 | 36.7 [28.7, 43.6] | 56 [43, 66] | 2045 [1595, 2431] | 920 [722, 1086] | 2965 [2317, 3518] | 6 [5, 8] | 233 [182, 277] | 105 [82, 124] | 338 [264, 401] | |
| 45-50 | 35.5 [30.2, 40.2] | 99 [84, 112] | 3205 [2735, 3626] | 1569 [1333, 1779] | 4774 [4067, 5405] | 11 [9, 12] | 351 [300, 397] | 172 [146, 195] | 523 [445, 592] | |
| 50-55 | 30.9 [25.7, 35.5] | 126 [105, 144] | 3540 [2970, 4052] | 2282 [1883, 2634] | 5822 [4853, 6687] | 14 [11, 16] | 382 [321, 438] | 246 [203, 284] | 629 [524, 722] | |
| 55-60 | 28.6 [24.3, 32.6] | 180 [153, 206] | 4400 [3731, 5028] | 3120 [2655, 3551] | 7520 [6386, 8579] | 21 [18, 24] | 517 [438, 590] | 366 [312, 417] | 883 [750, 1007] | |
| 60-65 | 23.5 [19.2, 27.3] | 205 [170, 238] | 4229 [3501, 4898] | 3467 [2811, 4056] | 7696 [6312, 8954] | 28 [23, 32] | 574 [475, 665] | 471 [382, 551] | 1045 [857, 1216] | |
| 65-70 | 18.6 [15.1, 21.9] | 141 [113, 166] | 2445 [1969, 2877] | 2491 [2039, 2906] | 4936 [4009, 5784] | 30 [24, 36] | 524 [422, 616] | 534 [437, 623] | 1057 [859, 1239] | |
| 70-75 | 15.7 [12.4, 18.9] | 155 [122, 186] | 2125 [1671, 2550] | 2108 [1656, 2530] | 4233 [3327, 5080] | 50 [39, 60] | 679 [534, 814] | 673 [529, 808] | 1352 [1063, 1622] | |
| 75-80 | 13.2 [9.3, 16.8]0 | 186 [130, 238] | 2014 [1409, 2573] | 1720 [1222, 2184] | 3734 [2632, 4757] | 75 [52, 96] | 813 [569, 1039] | 694 [494, 882] | 1508 [1063, 1921] | |
| 80-85 | 5.1 [2.0, 8.0] | 110 [58, 160] | 854 [428, 1261] | 489 [115, 854]0 | 1343 [543, 2115] | 64 [34, 94] | 498 [250, 736] | 285 [67, 498] | 784 [317, 1234] | |
| ≥ 85 | 5.0 [1.9, 7.9] | 194 [100, 283] | 922 [457, 1365] | 540 [117, 953]0 | 1462 [573, 2319] | 119 [62, 174] | 568 [282, 842] | 333 [72, 588] | 901 [354, 1429] |
Presented with point estimates with 95% uncertainty interval.
BMI, body mass index; CVD, Cardiovascular disease; DALY, Disability Adjusted Life Year; PAF, Population Attributable Fractions; YLD, Years of Life Lost; YLL, Years Lives with Disability
Supplementary Table 6. Population attributable fractions and age-standardized cardiovascular disease burdens attributable to high body mass index in different geographic areas in Taiwan.
| City | PAF (%) | Numbers | Age-standardized attributable burdens (per 100,000 person-years) | ||||||
| Deaths | YLLs | YLDs | DALYs | Deaths | YLLs | YLDs | DALYs | ||
| Yilan County | 17.4 [13.1, 21.1] | 52 [38, 66] | 887 [673, 1075] | 815 [615, 997] | 1702 [1288, 2072] | 7 [5, 9] | 125 [94, 150] | 112 [85, 137] | 237 [178, 287] |
| Hsinchu County | 16.5 [12.2, 20.4] | 45 [30, 58] | 646 [486, 792] | 742 [538, 925] | 1388 [1024, 1717] | 6 [4, 7] | 85 [65, 104] | 101 [74, 126] | 186 [138, 230] |
| Miaoli County | 16.5 [12.5, 20.1] | 64 [46, 81] | 1059 [824, 1280] | 1180 [877, 1452] | 2239 [1701, 2732] | 7 [5, 8] | 121 [95, 145] | 136 [102, 167] | 257 [197, 312] |
| Changhua County | 17.5 [12.9, 21.5] | 119 [82, 153] | 1947 [1439, 2385] | 1919 [1405, 2374] | 3866 [2845, 4759] | 6 [4, 7] | 101 [74, 123] | 99 [72, 122] | 200 [147, 245] |
| Nantou County | 16.7 [12.4, 20.7] | 59 [41, 76] | 886 [671, 1084] | 1033 [753, 1283] | 1919 [1424, 2367] | 6 [5, 8] | 103 [79, 125] | 121 [88, 150] | 224 [167, 275] |
| Yunlin County | 17.3 [12.8, 21.4] | 95 [65, 123] | 1488 [1117, 1821] | 1358 [991, 1689] | 2845 [2108, 3510] | 7 [5, 9] | 127 [97, 154] | 113 [83, 140] | 240 [180, 294] |
| Chiayi County | 16.3 [12.4, 19.9] | 66 [47, 84] | 1117 [850, 1358] | 954 [724, 1163] | 2071 [1574, 2520] | 7 [5, 8] | 124 [94, 150] | 105 [80, 128] | 229 [174, 278] |
| Pingtung County | 17.6 [13.4, 21.4] | 104 [75, 130] | 1921 [1458, 2324] | 1645 [1248, 2000] | 3566 [2706, 4323] | 7 [5, 9] | 143 [107, 173] | 119 [89, 144] | 261 [196, 318] |
| Taitung County | 21.9 [16.8, 26.3] | 47 [34, 58] | 930 [719, 1110] | 497 [376, 602] | 1427 [1095, 1712] | 13 [9, 16] | 273 [209, 325] | 139 [104, 168] | 412 [313, 493] |
| Hualien County | 18.9[14.1, 23.1] | 39 [28, 50] | 616 [459, 753] | 629 [471, 771] | 1245 [930, 1524] | 7 [5, 9] | 115 [84, 140] | 117 [87, 143] | 231 [171, 284] |
| Penghu County | 17.0 [13.0, 20.6] | 13 [9, 16] | 216 [168, 259] | 148 [111, 182] | 364 [280, 441] | 7 [5, 9] | 132 [104, 156] | 92 [70, 112] | 223 [174, 268] |
| Keelung City | 19.3 [14.8, 23.5] | 62 [44, 78] | 945 [735, 1141] | 625 [466, 769] | 1570 [1201, 1910] | 10 [7, 13] | 154 [120, 186] | 104 [76, 129] | 258 [196, 315] |
| Hsinchu City | 16.8 [12.5, 20.8] | 31 [21, 40] | 483 [367, 591] | 499 [364, 622] | 982 [731, 1213] | 5 [4, 7] | 82 [63, 101] | 87 [63, 109] | 170 [126, 210] |
| Chiayi City | 16.8 [12.8, 20.3] | 22 [16, 27] | 366 [282, 442] | 378 [287, 460] | 744 [569, 902] | 5 [4, 6] | 87 [67, 106] | 94 [70, 114] | 181 [137, 220] |
| Taipei City | 16.9 [12.7, 20.7] | 283 [197, 365] | 4371 [3323, 5333] | 3513 [2593, 4350] | 7884 [5916, 9682] | 6 [4, 8] | 97 [74, 118] | 78 [58, 97] | 176 [132, 215] |
| Kaohsiung City | 18.0 [13.6, 21.9] | 281 [203, 354] | 4965 [3789, 6004] | 4091 [3064, 5011] | 9056 [6853, 11015] | 7 [5, 9] | 117 [87, 142] | 95 [69, 117] | 212 [157, 259] |
| New Taipei City | 19.8 [14.9, 24.1] | 440 [313, 558] | 7420 [5618, 9010] | 5304 [3960, 6499] | 12723 [9578, 15510] | 8 [6, 11] | 131 [96, 161] | 92 [67, 115] | 223 [163, 276] |
| Taichung City | 17.5 [13.2, 21.3] | 185 [134, 230] | 3366 [2542, 4080] | 3430 [2585, 4185] | 6795 [5127, 8265] | 5 [4, 7] | 91 [67, 112] | 93 [69, 114] | 184 [136, 225] |
| Tainan City | 17.3 [13.0, 21.1] | 168 [120, 212] | 3024 [2290, 3668] | 2857 [2141, 3488] | 5882 [4431, 7157] | 6 [4, 7] | 105 [79, 127] | 98 [72, 119] | 202 [151, 247] |
| Taoyuan City | 19.6 [14.9, 23.7] | 163 [118, 204] | 2829 [2177, 3401] | 2647 [1985, 3227] | 5476 [4161, 6628] | 6 [4, 8] | 103 [78, 125] | 98 [72, 120] | 201 [150, 244] |
Presented with point estimates with 95% uncertainty interval.
BMI, body mass index; CVD, cardiovascular disease; DALY, disability adjusted life year; PAF, population attributable fractions; YLD, years of life lost; YLL, years lives with disability.
Supplementary Table 7. The population attributable fractions and age-standardized cardiovascular disease burdens rate attributable to high body mass index in 2005, 2009 and 2013.
| Sex | PAF (%) | Numbers | Age-standardized attributable burdens (person years per 100,000) | |||||||
| Deaths | YLLs | YLDs | DALYs | Deaths | YLLs | YLDs | DALYs | |||
| 2013 | ||||||||||
| Cardiovascular disease | Both | 18.0 [13.5, 21.9] | 2338 [1660, 2963] | 39481 [29987, 47910] | 34265 [25556, 42049] | 73745 [55543, 89959] | 10 [7, 13] | 168 [128, 204] | 146 [109, 179] | 314 [236, 383] |
| Women | 15.6 [11.4, 19.6] | 837 [553, 1103] | 11600 [8387, 14564] | 14331 [10449, 17902] | 25931 [18836, 32466] | 7 [5, 9] | 98 [71, 124] | 122 [89, 152] | 220 [160, 276] | |
| Men | 19.6 [15.0, 23.5] | 1501 [1107, 1860] | 27880 [21600, 33346] | 19934 [15107, 24148] | 47814 [36707, 57493] | 13 [9, 16] | 238 [184, 285] | 170 [129, 206] | 408 [313, 491] | |
| Ischemic heart disease | Both | 19.7 [15.1, 23.8] | 2108 [1517, 2652] | 34086 [26147, 41129] | 13725 [10541, 16509] | 47811 [36688, 57638] | 6 [4, 7] | 96 [73, 116] | 39 [29, 47] | 135 [102, 163] |
| Ischemic stroke | Both | 15.4 [11.2, 19.2] | 230 [143, 311] | 5395 [3840, 6781] | 20539 [15015, 25541] | 25934 [18855, 32322] | 1 [0, 1] | 15 [11, 19] | 58 [42, 72] | 73 [53, 91] |
| 2009 | ||||||||||
| Cardiovascular disease | Both | 18.0 [13.5, 22.0] | 1924 [1376, 2423] | 33795 [25349, 41130] | 26379 [19775, 32315] | 60173 [45124, 73445] | 8 [6, 10] | 146 [110, 178] | 114 [86, 140] | 260 [195, 318] |
| Women | 16.3 [12.0, 20.2] | 683 [463, 888] | 10214 [7500, 12701] | 11777 [8744, 14566] | 21990 [16245, 27267] | 6 [4, 8] | 89 [65, 111] | 103 [76, 127] | 192 [141, 237] | |
| Men | 19.2 [14.5, 23.2] | 1241 [913, 1536] | 23581 [17848, 28429] | 14602 [11031, 17750] | 38183 [28879, 46178] | 11 [8, 13] | 203 [153, 244] | 125 [95, 153] | 328 [248, 397] | |
| Ischemic heart disease | Both | 19.5 [14.8, 23.6] | 1762 [1270, 2210] | 29628 [22351, 35932] | 9995 [7683, 12009] | 39623 [30034, 47941] | 6 [4, 8] | 98 [73, 120] | 33 [25, 40] | 131 [99, 160] |
| Ischemic stroke | Both | 15.6 [11.5, 19.4] | 162 [107, 214] | 4166 [2998, 5198] | 16384 [12092, 20307] | 20551 [15090, 25504] | 1 [0, 1] | 14 [10, 17] | 55 [40, 69] | 69 [50, 86] |
| 2005 | ||||||||||
| Cardiovascular disease | Both | 18.4 [13.8, 22.5] | 1990 [1422, 2508] | 35230 [26105, 43026] | 18791 [14264, 22878] | 54021 [40369, 65904] | 9 [6, 11] | 155 [115, 189] | 83 [63, 100] | 237 [177, 289] |
| Women | 16.7 [12.5, 20.5] | 679 [468, 878] | 10625 [7894, 13140] | 8622 [6562, 10535] | 19247 [14456, 23675] | 6 [4, 8] | 95 [70, 117] | 77 [59, 94] | 172 [129, 211] | |
| Men | 19.6 [14.6, 23.7] | 1310 [954, 1630] | 24605 [18211, 29886] | 10168 [7701, 12342] | 34774 [25913, 42229] | 11 [8, 14] | 213 [158, 258] | 88 [67, 107] | 301 [224, 365] | |
| Ischemic heart disease | Both | 19.4 [14.5, 23.6] | 1525 [1098, 1913] | 26429 [19595, 32254] | 6823 [5278, 8191] | 33252 [24873, 40446] | 6 [4, 8] | 98 [72, 120] | 25 [20, 31] | 123 [91, 151] |
| Ischemic stroke | Both | 17.0 [12.7, 20.9] | 465 [324, 595] | 8802 [6510, 10772] | 11967 [8986, 14686] | 20769 [15495, 25458] | 2 [1, 2] | 33 [24, 40] | 45 [34, 56] | 78 [58, 96] |
Presented with point estimates with 95% uncertainty interval. PAF, population attributable fraction.
1 Salomon JA, Vos T, Hogan DR, et al. Common values in assessing health outcomes from disease and injury: disability weights measurement study for the Global Burden of Disease Study 2010. Lancet 2012;380:2129-43.
REFERENCES
- 1.Lavie CJ, Laddu D, Arena R, et al. Healthy weight and obesity prevention: JACC health promotion series. J Am Coll Cardiol. 2018;72:1506–1531. doi: 10.1016/j.jacc.2018.08.1037. [DOI] [PubMed] [Google Scholar]
- 2.Cardiovascular diseases. World Health Organization; 2021. [Google Scholar]
- 3.Roth GA, Mensah GA, Fuster V. The global burden of cardiovascular diseases and risks: a compass for global action. J Am Coll Cardiol. 2020;76:2980–2981. doi: 10.1016/j.jacc.2020.11.021. [DOI] [PubMed] [Google Scholar]
- 4.Koliaki C, Liatis S, Kokkinos A. Obesity and cardiovascular disease: revisiting an old relationship. Metabolism. 2019;92:98–107. doi: 10.1016/j.metabol.2018.10.011. [DOI] [PubMed] [Google Scholar]
- 5.Wu YC, Lo WC, Lu TH, et al. Mortality, morbidity, and risk factors in Taiwan, 1990-2017: findings from the Global Burden of Disease Study 2017. J Formos Med Assoc. 2021;120:1340–1349. doi: 10.1016/j.jfma.2020.11.014. [DOI] [PubMed] [Google Scholar]
- 6.Collaborators GBDO, Afshin A, Forouzanfar MH, et al. Health effects of overweight and obesity in 195 countries over 25 years. N Engl J Med. 2017;377:13–27. doi: 10.1056/NEJMoa1614362. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Diseases GBD; Injuries C. Global burden of 369 diseases and injuries in 204 countries and territories, 1990-2019: a systematic analysis for the Global Burden of Disease Study 2019. Lancet. 2020;396:1204–1222. doi: 10.1016/S0140-6736(20)30925-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Diseases GBD; Injuries I; Prevalence C. Global, regional, and national incidence, prevalence, and years lived with disability for 354 diseases and injuries for 195 countries and territories, 1990-2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet. 2018;392:1789–1858. doi: 10.1016/S0140-6736(18)32279-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Forouzanfar MH, Alexander L, Anderson HR, et al. Global, regional, and national comparative risk assessment of 79 behavioural, environmental and occupational, and metabolic risks or clusters of risks in 188 countries, 1990-2013: a systematic analysis for the Global Burden of Disease Study 2013. Lancet. 2015;386:2287–2323. doi: 10.1016/S0140-6736(15)00128-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Yeh TL, Hsu HY, Tsai MC, et al. Association between metabolically healthy obesity/overweight and cardiovascular disease risk: a representative cohort study in Taiwan. PLoS One. 2021;16:e0246378. doi: 10.1371/journal.pone.0246378. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Murray CJ, Lopez AD. On the comparable quantification of health risks: lessons from the Global Burden of Disease Study. Epidemiology. 1999;10:594–605. [PubMed] [Google Scholar]
- 12.Gadde KM, Vetter ML, Iqbal N, et al. Efficacy and safety of autoinjected exenatide once-weekly suspension versus sitagliptin or placebo with metformin in patients with type 2 diabetes: The DURATION-NEO-2 randomized clinical study. Diabetes Obes Metab. 2017;19:979–988. doi: 10.1111/dom.12908. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Lai YJ, Hu HY, Lee YL, et al. Association between obesity and risk of chronic kidney disease: a nationwide Cohort study in Taiwan. Nutr Metab Cardiovasc Dis. 2017;27:1008–1014. doi: 10.1016/j.numecd.2017.08.006. [DOI] [PubMed] [Google Scholar]
- 14.Health Promotion Administration Ministry of Health and Welfare, Community Health Division. Check your body weight everyday. Health promotion administration ministry of health and welfare. Health Promotion Administration Ministry of Health and Welfare, Community Health Division; 2018. [Google Scholar]
- 15.Lo WC, Ku CC, Chiou ST, et al. Adult mortality of diseases and injuries attributable to selected metabolic, lifestyle, environmental, and infectious risk factors in Taiwan: a comparative risk assessment. Popul Health Metr. 2017;15:17. doi: 10.1186/s12963-017-0134-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Salomon JA, Vos T, Hogan DR, et al. Common values in assessing health outcomes from disease and injury: disability weights measurement study for the Global Burden of Disease Study 2010. Lancet. 2012;380:2129–2143. doi: 10.1016/S0140-6736(12)61680-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Vos T, Flaxman AD, Naghavi M, et al. Years lived with disability (YLDs) for 1160 sequelae of 289 diseases and injuries 1990–2010: a systematic analysis for the Global Burden of Disease Study 2010. The Lancet. 2013;380:2163–2196. doi: 10.1016/S0140-6736(12)61729-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Global Burden of Metabolic Risk Factors for Chronic Diseases Collaboration. Cardiovascular disease, chronic kidney disease, and diabetes mortality burden of cardiometabolic risk factors from 1980 to 2010: a comparative risk assessment. Lancet Diabetes Endocrinol. 2014;2:634–647. doi: 10.1016/S2213-8587(14)70102-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Dai H, Alsalhe TA, Chalghaf N, et al. The global burden of disease attributable to high body mass index in 195 countries and territories, 1990-2017: an analysis of the Global Burden of Disease Study. PLoS Med. 2020;17:e1003198. doi: 10.1371/journal.pmed.1003198. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Felisbino-Mendes MS, Cousin E, Malta DC, et al. The burden of non-communicable diseases attributable to high BMI in Brazil, 1990-2017: findings from the Global Burden of Disease Study. Popul Health Metr. 2020;18:18. doi: 10.1186/s12963-020-00219-y. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.NCD Risk Factor Collaboration. Heterogeneous contributions of change in population distribution of body mass index to change in obesity and underweight. Elife. 2021;10:e60060. doi: 10.7554/eLife.60060. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Wu YC, Lo WC, Lu TH, et al. Mortality, morbidity, and risk factors in Taiwan, 1990-2017: findings from the Global Burden of Disease Study 2017. J Formos Med Assoc. 2020 doi: 10.1016/j.jfma.2020.11.014. [DOI] [PubMed] [Google Scholar]
- 23.Fletcher GF, Landolfo C, Niebauer J, et al. Promoting physical activity and exercise: JACC health promotion series. J Am Coll Cardiol. 2018;72:1622–1639. doi: 10.1016/j.jacc.2018.08.2141. [DOI] [PubMed] [Google Scholar]
- 24.Grady D, Wenger NK, Herrington D, et al. Postmenopausal hormone therapy increases risk for venous thromboembolic disease. The Heart and Estrogen/progestin Replacement Study. Ann Intern Med. 2000;132:689–696. doi: 10.7326/0003-4819-132-9-200005020-00002. [DOI] [PubMed] [Google Scholar]
- 25.Zukiewicz-Sobczak W, Wroblewska P, Zwolinski J, et al. Obesity and poverty paradox in developed countries. Ann Agric Environ Med. 2014;21:590–594. doi: 10.5604/12321966.1120608. [DOI] [PubMed] [Google Scholar]
- 26.Health Promotion Administration Ministry of Health and Welfare. Statistics fo health promotion. https://www.hpa.gov.tw/Pages/Detail.aspx?nodeid=268&pid=14315. Health Promotion Administration, Ministery of Health and Welfare; 2013. [Google Scholar]
- 27.Lin CY, Hung HJ, Chung CJ, et al. Ethnic disparity in metabolic syndrome and related obesity and health behavior: a community study in Taiwan. Diabetol Metab Syndr. 2021;13:134. doi: 10.1186/s13098-021-00751-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Hong YC. Exploring the relationship between medical resources and health status: an empirical study of crude and accidental death rates in 23 counties in Taiwan. Taiwan J Public Health. 2010;29:347–359. [Google Scholar]
- 29.Brownell KD, Kersh R, Ludwig DS, et al. Personal responsibility and obesity: a constructive approach to a controversial issue. Health Aff (Millwood) 2010;29:379–387. doi: 10.1377/hlthaff.2009.0739. [DOI] [PubMed] [Google Scholar]
- 30.Ho Chan WS. Taiwan’s healthcare report 2010. EPMA J. 2010;1:563–585. doi: 10.1007/s13167-010-0056-8. [DOI] [PMC free article] [PubMed] [Google Scholar]