

Abstract
The post-September 11 era has prompted unprecedented attention to medical preparations for national special security events (NSSE), requiring extraordinary planning and coordination among federal, state, and local agencies. For an NSSE, the US Secret Service (USSS) serves as the lead agency for all security operations and coordinates with relevant partners to provide for the safety and welfare of participants. For the 2004 Democratic National Convention (DNC), designated an NSSE, the USSS tasked the Boston Emergency Medical Services (BEMS) of the Boston Public Health Commission with the design and implementation of health services related to the Convention. In this article, we describe the planning and development of BEMS’ robust 2004 DNC Medical Consequence Management Plan, addressing the following activities: public health surveillance, on-site medical care, surge capacity in the event of a mass casualty incident, and management of federal response assets. Lessons learned from enhanced medical planning for the 2004 DNC may serve as an effective model for future mass gathering events.
Keywords: mass gathering, emergency medical services, public convention
In 1998 President Bill Clinton issued Presidential Decision Directive-62 (PDD-62) Protection against Unconventional Threats to the Homeland and Americans Overseas, which designates certain events of national interest as national special security events (NSSEs).1 NSSE designation criteria include size of event, anticipated attendance by dignitaries, and any cultural, historical, or political significance that increases its potential as a terrorist target.2 PDD-62 provisions for NSSEs include placing security measures otherwise used by local agencies under explicit federal control, with the US Secret Service (USSS) serving as the lead agency for both planning and implementation of operations,1,2 and making available federal support, including prepositioned response assets.2 Since 1998, there have been 24 NSSEs, including presidential inaugurations, major sporting events, and several international meetings.3,4
The 2004 Democratic National Convention (DNC), held in Boston from July 26 to 29, represented the first political convention after September 11, 2001. Given the high-profile nature of this event, the Department of Homeland Security (DHS) designated it an NSSE in May 2003. Upon NSSE designation, the USSS coordinated federal, state, and local agencies through an executive steering committee and multiple subcommittees to provide critical support for the event (Table 1).5,6 Before September 11, the executive steering committee, typically composed of leaders from public safety agencies, did not include representation from the local medical community. However, in an unprecedented strategy, the USSS approved the request of the Mayor of Boston for Boston Emergency Medical Services (BEMS), a department of the Boston Public Health Commission (BPHC), to join the executive steering committee and serve as the lead planning agency and principal provider for all DNC-related health and medical services (personal communication, US Secret Service Special Agent Steven Ricciardi, Boston field office, January 29, 2007).1,2
TABLE 1.
Executive Steering Committee Membership and Subcommittees
| Executive Steering Committee Membership | Subcommittees |
|---|---|
| Boston Emergency Medical Services Civil disobedience/prisoner processing* Boston Police Department Federal Bureau of Investigation Federal Bureau of Investigation Federal Emergency Management Agency Fleet Center Management Massachusetts Executive Office of Public Safety Massachusetts State Police US Attorney General Office US Coast Guard US Secret Service |
Airspace security Boston Fire Department Consequence management* Credentialing* Crisis management* Critical infrastructure Dignitary/VIP protection* Explosive ordnance disposal/K-9* Fire/life safety/hazmat* Intelligence/counterterrorism Interagency communication* Legal Public affairs Tactical/countersurveillance Training* Transportation/traffic* Venues* |
Indicates Boston Emergency Medical Services representation on subcommittee.
This article summarizes and analyzes the planning, results, and long-term preparedness outcomes for the City of Boston related to this NSSE. We use the traditional public health core functions of assessment, policy development, and assurance as a framework for presentation and analysis.7
One way to assess public health systems capabilities is to directly observe response to real public health emergencies (eg, anthrax, severe acute respiratory syndrome, Hurricane Katrina) or other events (eg, foodborne disease outbreaks, seasonal influenza epidemics). A simple approach involving limited cost that embeds learning and assessment in routine practice is “look-back,” a retrospective analysis of past responses to public health events that have the potential to threaten the health of a community and that require organizational efforts that go beyond routine public health activities.8 In this article, we use the look-back approach on the organizational efforts and emergency medical consequence management plan developed by the City of Boston for the DNC. Data were gathered by a series of interviews with 2 of the major leaders of this planning effort (K.H.B., R.A.S.) and representatives of the USSS, BPHC, Boston Medical Center (BMC), and the American Red Cross (ARC), and a review by 2 independent reviewers (K.A.K., E.S.) of government documents and notes produced as part of planning and execution. Subsequently, using the approach developed in other similar assessments, all of the information was categorized within the traditional framework of the 3 core public health functions: assessment, assurance, and policy development.
ASSESSMENT
Surveillance
After September 11, BPHC augmented their volume-based surveillance system, which automatically records the daily number of patient visits to Boston’s acute care facilities and select community health centers.9 In collaboration with BEMS and local hospitals, BPHC implemented an active syndromic surveillance system, which collected a wider range of data (chief complaint, discharge diagnosis, and a limited set of demographic information) on patient visits. The chief complaint data, sorted into categories of symptoms occurring together, are then measured against historic thresholds to identify patterns indicating a possible outbreak of disease.9
In addition, BPHC instituted several new sources of surveillance information during the DNC, including daily data collected from EMS transports, Poison Control Center calls, death certificates, and monitoring of medical services provided at the Convention venue, area hotels, and the Suffolk County House of Corrections (SCHOC).
Environmental Health
A complement of 5 US Food and Drug Administration and 10 Boston Inspectional Services Department inspectors conducted food safety inspections at the Convention venue from July 23 through July 29. The syndromic surveillance and food safety systems linked together to detect early outbreaks of foodborne illness.
Chemical, biological, and radiological agents monitoring was conducted on a 24-hour basis between July 23 and July 29 throughout the Convention venue and its surrounding areas. Boston’s BioWatch plan was implemented throughout the city under normal citywide protocols. Detection equipment was supplied and monitored by the Massachusetts National Guard Civil Support Team, USSS, and Department of Energy in conjunction with the Boston Fire Department (BFD), Boston Police Department (BPD), BPHC, and Massachusetts State Police (MSP). More than 800 personal radiation detectors were distributed to public safety and BEMS officers. If needed, response to chemical, biological, and radiological incidents was to be implemented by 5 joint hazardous assessment teams (JHATs), each composed of a representative from the USSS, Federal Bureau of Investigation, BFD, and BPD.
POLICY DEVELOPMENT
Planning for Response to Public Health Emergencies
BEMS is uniquely both a public safety and public health service agency, effectively bridging Boston’s health care and first responder systems. As such, BEMS led coordination with Boston’s wider medical community to prepare for the DNC. As part of new explicit NSSE emergency medical consequence planning, BEMS formed a medical advisory group, composed of 39 organizations, including federal, state, and local public health and public safety agencies, and area hospitals, community health centers, and private sector partners, under the auspices of the USSS Consequence Management Subcommittee (Table 2).
TABLE 2.
Medical Advisory Group Members
| Hospitals | Boston Medical Center | Children’s Hospital |
| Emerson Hospital | Massachusetts General Hospital | |
| New England Medical Center | ||
| Emergency Medical Services | American Medical Response | Armstrong Ambulance |
| Boston Emergency Medical Services | Cataldo Ambulance | |
| Commonwealth Ambulance | EASCare Ambulance | |
| Fallon Ambulance | General Ambulance | |
| Professional Ambulance | ||
| Federal partners | 1st Civil Support Team Army National Guard | Agency for Toxic Substance and Disease Registry |
| Centers for Disease Control and Prevention | Federal Emergency Management Agency | |
| National Disaster Medical System | Northern Joint Regional Medical Plans and Operations | |
| US Coast Guard | US Department of Health and Human Services | |
| US Public Health Service | US Secret Service | |
| Department of Veterans Affairs | ||
| State partners | Massachusetts Department of Public Health | Massachusetts Emergency Management Agency |
| Massachusetts Office of Emergency Medical Services | Massachusetts State Police | |
| Local partners | American Red Cross | Boston Emergency Management Agency |
| Boston Police Department | Boston Public Health Commission | |
| Boston Fire Department | Massachusetts Bay Transportation Authority | |
| Metropolitan Medical Response System | Suffolk County House of Corrections | |
| Conference of Boston Teaching Hospitals | Massachusetts Ambulance Association | |
| Council and umbrella organizations | Massachusetts League of Community Health Centers | |
| Metropolitan Boston Emergency Medical Services Council |
The medical group, meeting monthly from December 2003 to April 2004 and twice monthly thereafter until the DNC, developed an extensive framework for provision of health services and mass casualty incident (MCI) medical management. In addition to public health surveillance, the medical consequence management plan (MCMP), adopted by all partner organizations, addressed direct care at the convention and its surrounding areas, as well as security and traffic control, hospital readiness, and pharmaceutical support.
Conceptualization and Implementation of Zones of Operation
Mass gatherings can challenge any community’s medical system. The attendance of more than 35,000 dignitaries, delegates, media, and staff at the DNC necessitated a logistic framework that would coordinate efficient medical response onsite, as well as at a large number of DNC-related functions throughout the city. In addition, mass demonstrations were expected, with the potential for associated injuries incurred by both participants and responding public safety officials. Meanwhile, the day-to-day medical needs of Boston residents outside the DNC had to be addressed.
To meet these demands, the MCMP delineated 5 zones of operations, both topographical and functional in nature, to address all aspects of DNC medical planning. The hard and soft zones (zones 1 and 2) represented onsite medical care at the Convention venue, the Fleet Center (later renamed TD Banknorth Garden), a 19,600-seat indoor sports arena, and its immediate surroundings (Fig. 1). Zone 3 encompassed medical resources for non–Fleet Center events, and zone 4 represented coverage for both participants and law enforcement related to demonstrations. Zone 5 took into account the medical needs for Boston residents outside the DNC. A zone commander (a deputy superintendent paramedic with BEMS) oversaw each zone and participated in daily briefings to update and adjust planning throughout the Convention. A detailed description of the activities performed in each zone is reported below.
FIGURE 1.
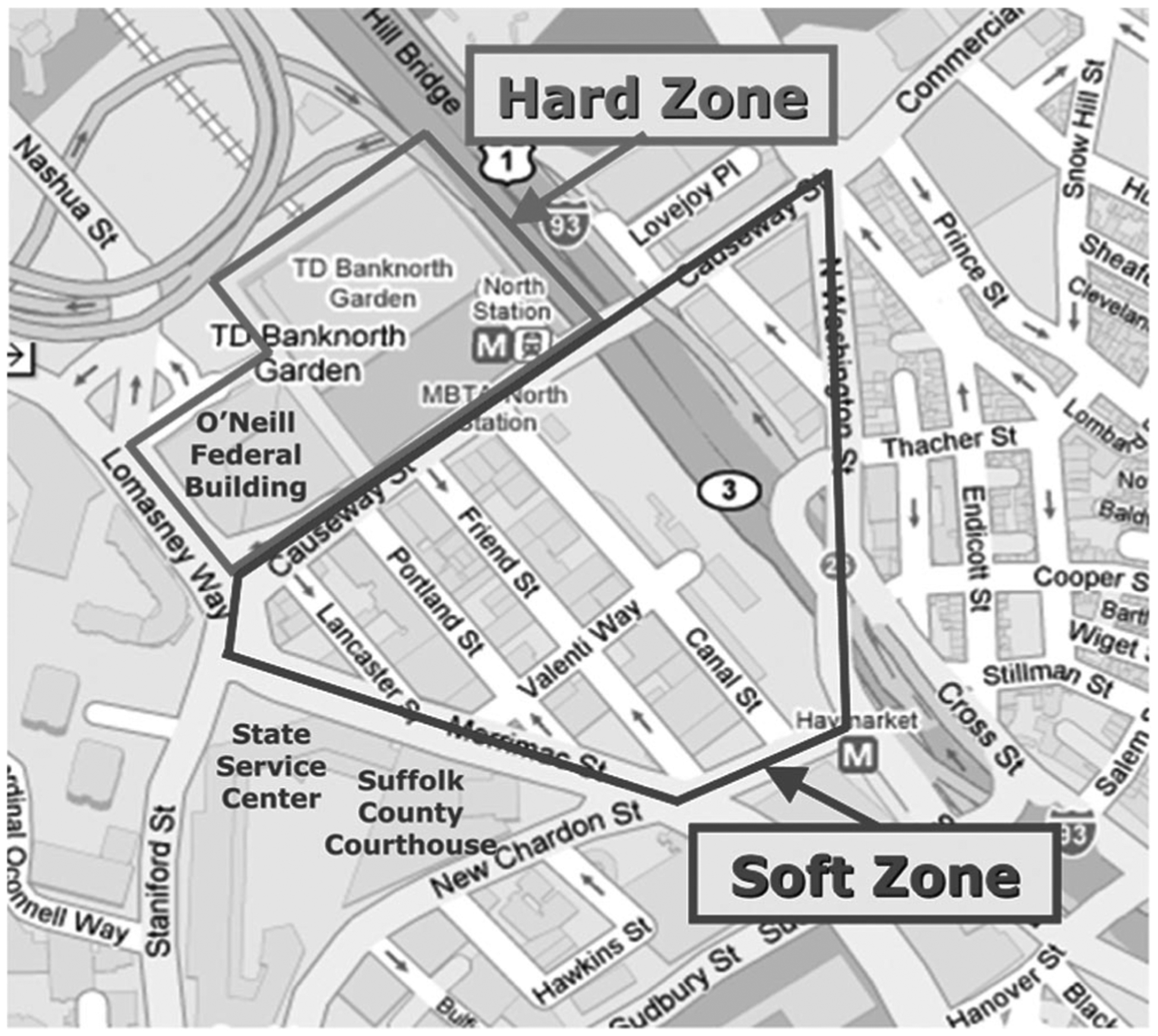
The MCMP delineated 5 zones of operations (both topographical and functional) to address all aspects of DNC medical planning. The hard and soft zones represented on-site medical care at the Convention venue.
Zones 1 and 2: Hard and Soft Zones
To provide flexible and efficient care in a crowded venue, BEMS assigned 6 mobile response teams (and an equal number of backup teams), each comprised of an emergency medical technician (EMT) and a paramedic, to respond to calls to the Convention floors. Teams were strategically stationed on various levels at 4 points of the venue. Peripheral “spotters” (security personnel) would contact teams for medical intervention. Teams were equipped with a wheel cot, basic life support first-responder supplies, a Mark I Nerve Agent Antidote Kit (Meridian Medical Technologies, Columbia, MD), and epinephrine auto-injector pens to treat individuals potentially experiencing allergic reactions following a planned balloon drop the last night of the Convention. Teams assessed and treated patients onsite and transported them to a BEMS-operated medical station within the Fleet Center, or if necessary, to a hospital via an ambulance located outside the security fence, to avoid time-consuming security clearance protocols.
An additional 2 teams (mobilized with all-terrain vehicles), each comprising 2 paramedics, provided exterior first response within the hard zone. By staffing these teams with paramedics, it was possible to provide a higher level of care and greater flexibility in a larger coverage area than would be possible if only EMTs were used. Two ambulances were prepositioned inside the hard zone to transport patients in critical condition (exterior mobile response teams were to staff these ambulances).
In addition, BEMS established a medical station. Staffed with a security guard, 2 paramedics, 2 EMTs, and 2 emergency physicians, the station was operational 24 hours per day from July 23 to July 30. Located on the Convention floor, the station measured 12 × 15 ft and was outfitted with 3 examination tables. Mainly intended as a treat-and-release site, it was equipped to treat limited pediatric and obstetrics conditions as well as advanced trauma and airway issues if potentially life-threatening delays in ambulance transport arose. The station was also supplied with 4 U pRBCs of type O blood and a large inventory of pharmaceuticals to provide care at the level of an urgent care clinic. Supplies were provided through the ARC and BEMS.
At each end of the soft zone, planners established 2 multipurpose areas for personnel and equipment staging as well as for evacuee gathering in the event of an MCI at the Convention. Each staging area was staffed with a BEMS liaison, a mobile response team, and a 35-person disaster medical assistance team (DMAT), available to provide surge capacity in coordination with BEMS. Two mobile response teams (paramedics) and 7 BEMS paramedics on bicycles also patrolled the soft zone and provided emergency medical care. Each staging area featured 3 ambulances available for deployment to support all of the zones (zone commanders submitted daily incident action plans requesting deployment of ambulances). In addition, 3 mass decontamination units were positioned throughout the soft zone.
Zone 3: Venues and Events
During the week-long Convention, more than 1000 events took place in and around Boston. BEMS divided a third DMAT into 6 “go-teams” consisting of 1 physician, 1 nurse, 2 additional medical staff, and 1 logistics specialist or communications officer to provide coverage for these events. Four ambulances also were assigned to special events (go-teams and special event ambulances were also available to support zones 4 and 5). Medical services were provided depending on levels of attendance, the nature of the event, and available staffing.
BEMS also provided medical support to any dignitary detail requested by the USSS, including the presidential and vice presidential nominees, who both received an ambulance escort. In addition, a municipal housing or school police officer, equipped with a radio to relay medical requests directly to BEMS, was assigned to buses transporting delegates.
Zone 4: Law Enforcement Support
To ensure the safety of both demonstrators and any emergency personnel responding to a possible civil disturbance, the medical group coordinated with the BPD and SCHOC. Twelve EMTs were assigned to a total of 6 public order platoons, deployed in and around a designated demonstration area. In addition, BEMS coordinated bike units with the BPD to stay abreast of mobile demonstrations. BEMS members were equipped with Morgan lens flushes, oxygen, automated external defibrillators, portable eyewash stations to treat individuals for pepper spray irritation, and Mark I kits.
Mindful that the 2000 Republican National Convention (RNC) resulted in more than 300 arrests,9 the SCHOC’s preparations included onsite mass decontamination unit, triage and clinical assessment (including eye examination) performed by Suffolk County Sheriffs Department paramedics, and referral capability to nearby BMC, which increased the capacity of its emergency department to triage an additional 150 patients per day. Specifically, BMC enhanced surge capacity by establishing separate reception areas to treat injured officers, fast track areas for eye washing and prisoner processing, and the deployment of occupational health personnel assigned to perform eye examinations and treat lacerations and fractures.
Zone 5: Citywide Response
Anticipating an increase in call volume from DNC-related activities (Boston’s population swelled by approximately 6% during the week of the Convention), the medical group wanted to ensure continuity of services to Boston’s residents. Therefore, BEMS collaborated with mutual aid partners to augment citywide coverage. Six private companies contributed 20 ambulances to the city, increasing the total number available during the DNC to 60. All of the contributing mutual aid partners were issued handheld radios to facilitate communication over citywide channels. BEMS units and mutual aid partners shared and responded to emergency calls according to the level of priority, with BEMS answering priority 1 calls.
BEMS also negotiated agreements whereby 200 nonmunicipal ambulances would be available within 30 minutes of an MCI. To increase response capacity, BEMS funded minigrants for essential equipment (ie, portable ventilators and suction machines, pulse oximeters, defibrillators, and hooded escape masks) to all mutual aid partners.
Traffic Control
The location of the Fleet Center, in downtown Boston amid several major freeways, posed a significant challenge for Convention security. To isolate the area, the USSS closed Interstate 93, the primary artery leading traffic into Boston, as well as several surrounding roads, bridges, and tunnels. To obviate concerns that traffic disruptions would prevent access to city hospitals, the medical group worked with the MSP to permit ambulance access to secure roads.
Specifically, ambulances requested access to closed roads through Centralized Medical Emergency Direction (CMED), which manages the regional communications system for emergency medical services and hospitals in Boston. CMED subsequently relayed requests to the multiagency command center (MACC), the primary site for interagency communication during the DNC. BEMS liaisons stationed at the MACC verified information received by C-MED against previously submitted rosters and then relayed the request for access to MSP MACC liaisons to arrange clearance through roadblocks. At the access ramp, MSP patrols checked photo identification and searched vehicles. As part of planning, officials from BEMS, MSP, and the Massachusetts Office of Emergency Medical Services cosigned a letter of explanation and issued hard copies of the plan to all of the emergency medical services, police, and fire departments in Maine, Rhode Island, New Hampshire, and Massachusetts. In addition, BEMS made more than 25 presentations to both local and out-of-area hospitals, EMS regional meetings, and council organizations explaining the plan and answering questions.
Hospital Readiness
An integral component of the MCMP involved increasing the ability of hospitals to respond to an MCI through added surge capacity. As part of the medical group, the Conference of Boston Teaching Hospitals (COBTH-an umbrella organization of Boston’s teaching and research hospitals), facilitated coordination among Boston’s acute care facilities, each of which developed a DNC mass casualty plan. COBTH members also agreed to maintain collectively a minimum of 500 free beds, reschedule the majority of elective surgeries and outpatient services, and suspend ambulance diversion during the DNC.
In addition, COBTH expanded staffing availability by suspending vacation time during the DNC. To help health care personnel living in outlying areas, city officials arranged overnight accommodations at Boston hotels and an earlier subway start time of 4:30 AM. In addition to BMC, hospitals within the vicinity of the Convention had emergency operations centers open 24 hours per day. In the weeks leading up to the Convention, all of the major Boston hospitals established mass decontamination units.
During the Convention, C-MED requested bed and staffing counts twice daily from all of the hospitals, community health centers, and rehabilitation facilities in Boston, and communicated this information to the Massachusetts Department of Public Health. In addition, C-MED conducted a once-daily statewide bed count. A daily conference call occurred during the Convention for DNC medical planning partners, including hospitals. A special e-mail address was established to gather issues to be discussed during the call.
Stockpiling Antidotes
To effectively treat victims of a potential mass exposure to nerve agents, the medical group took steps to ensure large quantities of antidotes were immediately available in Boston. Through a Massachusetts State Homeland Security Grant, the medical group provided each Massachusetts hospital with multiple doses of doxycycline, Mark I kits, cyanide antidote kits, and atropine. The state also positioned 250,000 doses of potassium iodide throughout metropolitan Boston. BEMS also equipped all of the ambulances with 60 Mark I kits, and stored 22,400 potassium iodide doses at BEMS headquarters.
Despite this planning, an emergency involving mass casualties was expected to tax local resources and require federal augmentation. Under the provisions of PDD-62, federal authorities can supplement local assets, with a precise package tailored for each NSSE. Therefore, BEMS developed a formal request, endorsed by the Boston Emergency Management Agency and USSS, for pharmaceutical support from the Federal Emergency Management Agency as well as the Department of Health and Human Services (DHHS) through the Strategic National Stockpile (SNS) and the National Disaster Medical System (DMATs were also part of this requested support).
The supplies received were 5 special events packages (configured with ventilators and nerve agent antidotes), 500 cyanide kits, 2000 Mark I kits, and 2 emergency response packs (1 for trauma victims, 1 for chemical exposure victims) per the request specifications of the BEMS medical director. Materials were staged at various facilities, including the hard and soft zones, and hospitals in and around Boston to ensure an efficient and timely response to an MCI.
Concerned that an MCI would likely strain available blood resources, particularly in the summer months when supplies historically decline due to a lack of school drives, the medical group also took preventive steps. The ARC, in collaboration with the medical group, hosted a special blood drive and public awareness campaign 30 days before the Convention, including a series of print, television, and radio advertisements featuring the chief of BEMS. The ARC also provided daily updates on inventory status to the medical group during the DNC.
Assurance
Steps were taken to increase the awareness of hospital staff to patient decontamination and isolation procedures, as well as identification and treatment of chemical, biological, and radiological agents. In coordination with the DelValle Institute for Emergency Preparedness (a section of BEMS and BPHC), COBTH organized specialized trainings for health care professionals (EMTs, paramedics, physicians, nurses, security, and environmental response team members). More than 600 workers were trained on incident command structure, hazardous material detection, decontamination and isolation procedures, smallpox vaccination, and respirator fit testing.
Pre-event Communication to the Public
The City of Boston also conducted outreach to prepare residents for heightened security during the DNC, including establishing a DNC helpline and Web site to answer questions and address concerns about transportation, road closures, and city services. BEMS participated in daily intelligence briefings and press conferences with both the BPD and the MSP to ensure consistency of messages to the public.
SHORT-TERM OUTCOMES
Utilization Rates and Case Mix
Of 35,000 Convention attendees, a total of 405 patients were examined between July 23 and July 29, resulting in a medical usage rate of 11.6 medical encounters per 1000 visitors. Mobile response teams recorded approximately 200 medical interactions within the hard and soft zones. These patients were either evaluated onsite and released for minor to moderate injuries and illnesses (cuts/abrasions, dehydration, syncope) or transported directly to area hospitals (bypassing the medical station). Despite the crowd, mobile response teams reached all patients in less than 5 minutes.
Of the 205 patients who directly accessed the medical station, 90% had minor complaints such as headache, blisters, or mild abdominal pain. Chief complaints of significance included severe abdominal pain, chest pain, and extremity injury and laceration.
Of note, the most commonly seen moderate illness, both at the medical station and by the mobile response teams, was dehydration, attributable to limited access to water. In part this was seen because to minimize debris, convention planners had prohibited water bottles and cups on the Convention floor. Also, security dictated no one was permitted reentry due to overcrowding, thus discouraging participants who wanted to leave and purchase water. Although staff processed patients in a timely manner, the limited number of examination tables and stretchers frequently reached capacity due to a discrete number of heat-related patients (who needed a recovery time ranging from 15 minutes to 1 hour). Of note, weather conditions were optimal throughout the DNC, with the daytime temperature averaging in the mid-70s. Such conditions may have limited the number of cases of heat-related illness which could have occurred during this summer event.
No mass casualty event occurred during the course of the Convention. Also, at the medical station, no critically ill patient was treated during the course of the Convention, as the site was mainly intended for treat-and-release or stabilization, followed by rapid transport to nearby hospitals for more seriously ill patients. Sixteen patients were transferred to hospitals (via units outside the hard zone perimeter) with diagnoses including chest pain, severe hypertension, severe foot skin laceration, rule-out fracture, and gastroenteritis. Although staff at the medical station knew of approximately 100 preidentified delegates affected by chronic conditions at a severe stage (eg, asthma, cancer, diabetes) and were pre pared to treat them if necessary, they were less prepared for the large numbers of children and infants that were unexpectedly in attendance. Nevertheless, only a few pediatric patients were brought to the medical station.
Civil disturbances, substantially less than anticipated, resulted in 6 arrests, and none required medical attention. BEMS units, deployed 27 times in support of law enforcement, treated 67 police officers for minor/moderate conditions (cuts/abrasions, dehydration, and heat-related illness). Three public safety officers were transported to BMC for hypertension, chest pain, and asthma, respectively.
Traffic Control and Response to Emergency Calls
Regarding traffic control, 162 ambulances were cleared through closed roads without any breaches in security. Communication with mobile response teams proceeded smoothly, although on several occasions multiple calls were made concerning the same patient, and a multiteam response was occasionally made for a single victim.
Although mutual aid partners normally respond to less than 1% of emergency calls, they answered approximately 25% of the call volume during the week of the Convention. Overall, response time improved during the DNC. The average citywide response time for priority 1 calls from July 1 to 24 was 6 minutes, 1 second, which decreased to 5 minutes, 7 seconds the week of the Convention. The combined average citywide response time for priority 2 and 3 calls during July 1 through 24 was 8 minutes, 1 second, which decreased to 7 minutes, 6 seconds the week of the Convention.
Supplies
Blood supplies, for which regional capacity increased by 111% following the ARC campaign, were deemed sufficient for the DNC. However, inventory issues, onerous storage requirements, and delayed responses created challenges regarding coordination of SNS and National Disaster Medical System materials. For example, 13 of the 20 drugs requested by BEMS were not included in the SNS. Furthermore, DHHS would not position pharmaceuticals in nongovernment facilities or hospitals without a previous SNS agreement, which precluded institutions, including the Fleet Center, from receiving medications. After much discussion, BEMS loaned the Fleet Center and several acute-care facilities containers of nerve agent and cyanide antidotes from their own organization’s supplies for the week.
Other supply coordination issues required direct communication between the city and federal leaders at the highest levels. For example, the Federal Emergency Management Agency first expressed concern that budgetary constraints would limit availability of federal resources to support Boston during the DNC. Subsequently, in June 2004 the Mayor of Boston sent a letter to the DHS Secretary requesting support, which was immediately granted. BEMS also received extra supplies in addition to what had been requested. Shortly before the Convention, DHHS delivered 1000 ventilators, as well as an additional number of special events packages and cyanide antidotes.
LONG-TERM OUTCOMES
National Collaborations
Since the 2004 DNC, the MCMP has been recognized repeatedly by the USSS as a model for future NSSE events. Furthermore, BEMS and the medical group received the rarely granted USSS Directors Award of Excellence. BEMS has widely disseminated the MCMP, responding to more than 100 requests for copies by local, state, and federal agencies across the United States, including high-level officials at the DHS, DHHS, and Department of Defense. In addition, at the recommendation of the USSS, BEMS is providing ongoing assistance for the medical planning and preparation efforts for the 2008 DNC and RNC in Denver and Minneapolis, respectively.
Regional and Local Partnerships
The unique opportunity for collaboration around the 2004 DNC has also led to subsequent long-term benefits for the City of Boston. The medical group experience of interagency coordination and mutual support has since extended to application in dozens of large events in the city. An outgrowth of the DNC preparations is a permanent Boston-based JHAT, comprising representatives of BEMS, the National Guard, BFD, BPD, and the Coast Guard, to provide medical security for city mass gathering events such as the Boston Marathon, the 2004 and 2007 World Series, and Boston’s Fourth of July and New Year’s Eve celebrations. The plans developed for the DNC regarding ambulance transport and secure roads have also since been successfully used for other major events hosted by the city. Finally, in a collaboration that may be unique in the country, following the DNC, a BEMS paramedic was assigned to the Boston Regional Intelligence Center to ensure constant coordination between the health care and intelligence communities.
The DNC also helped BEMS to exercise and evaluate their operational readiness for a large-scale emergency by deploying basic medical services in coordination with state and federal responders, including DMATs. BEMS continues working in conjunction with the USSS, providing medical coverage for visiting dignitaries.
Training
The DNC experience also reinforced the need for continued training. Since 2004 the DelValle Institute for Emergency Preparedness, in collaboration with BEMS, BFD, BPD, and COBTH, offers annual refresher MCI training for hospital, police and special operations, and EMS personnel. Such training has reached more than 10,000 professionals in the state. In addition, such trainings complemented ongoing efforts supported by the Metropolitan Medical Response System and other initiatives.
DISCUSSION
To our knowledge, this article is the first to describe dedicated emergency medical considerations for NSSEs. Although the NSSE designation was established only in 1998, it has gained special significance since September 11. Mass gatherings have many medical challenges that vary according to key characteristics such as their duration, crowd density and mood, whether they are held predominantly outdoors or indoors, whether the crowd is predominantly seated or mobile, and weather conditions.10 In addition to these characteristics, an NSSE requires communication and cooperation among a multitude of local, state, and federal agencies under the overall leadership of the USSS. Before September 11 there was little explicit attention paid to dimensions of possible medical consequences of terrorism and mass casualties related to NSSEs. Hence, jurisdictions hosting such events were essentially left on their own to address these issues. In previous NSSE events and political conventions, medical coverage was generally coordinated by local fire departments (typically a city’s primary EMS provider) and a selection of medical partners, such as local hospitals. No formalized planning, communication, or command structure between the security and medical communities previously existed.1,2,7,8,10,12–14
In contrast, for the 2004 Boston DNC, medical issues received the highest priority through a new organizational structure. The USSS appointed a local agency, BEMS, to the executive steering committee and designated BEMS as the lead medical consequence agency. This new command structure, which capitalized on BEMS’ preexisting relationships with members of the local public health and health care communities, created a heightened medical focus for the executive steering committee. Moreover, BEMS formally established a medical advisory group, comprising a broad array of partners, including federal, state, and local security, public safety, EMS, hospitals, and public health agencies. Through a joint mobilization of resources, this group created a comprehensive MCMP that addressed mass gathering medical care issues, including surveillance, zones of operation, traffic control, hospital readiness, and stockpiling of antidotes.
Planning in 2004 incorporated an unprecedented level of preparations for MCI medical management, including the establishment of off-site staging areas, the integration of federal response assets such as DMATs and SNS materials, collaboration with mutual aid partners, and the augmentation of surveillance and hospital activities. The depth of these preparations—expecting a worst-case scenario—reflected the sensitivities involved in the first NSSE after September 11.
The Boston DNC NSSE experience yielded an array of positive short-term and long-term outcomes. Regarding the former, the level of services available met the burden of injury and illness, medical supplies (including blood) were sufficient to meet the need at the Convention, traffic control was achieved, few arrests were made, and response times for emergency care were maintained, if not improved, in the city throughout the time of the DNC. Medical utilization rates of 11.6/1000 visitors were consistent with prior published studies on medical care at political conventions. The literature notes reported medical utilization rates at political conventions ranging from lows of 1.46 and 3.53/1000 attendees (at the 1996 DNC in Chicago and 2000 RNC in Philadelphia, where documentation was not completed for patients with minor complaints) to highs of 12.7 and 21.23/1000 attendees (at the 1984 DNC and RNC 1984 in San Francisco and Dallas, respectively).10,12–14 The types of medical complaints (headaches, extremity injuries and lacerations, syncope, chest pain, and abdominal pain) were likewise typical of prior reports and may be reflective of the age demographics of the attendees as well as the crowded nature of the venues.10,12–14
Just as important were long-term outcomes. Since 2004 the legacy of the planning and coordination has led to critical national collaborations. The USSS has prioritized emergency medical consequence management of future NSSEs, using the Boston experience as 1 model. BEMS advisors are now providing onsite technical assistance for the 2008 DNC and RNC. Furthermore, sustained long-term collaborations have led to the formation of an official JHAT that has helped coordinate care around dozens of mass gatherings in Boston since the summer of 2004.
Future NSSEs can improve on the Boston experience with added attention to issues such as space (enlargement of the medical station), broader distribution of fixed medical assets on the floor (addition of multiple first aid stations within the Convention venue), prevention of dehydration (focusing efforts on the provision of free water on the Convention floor), improvement of efficiency of communication (eg, having medical mobile teams receive emergency calls based on a dispatch from a single command post, rather than separate sources of information), and staffing (providing more personnel to provide short, flexible shifts).
Planning and implementation of medical management around the 2004 Boston DNC led to a new model for NSSE planning, upheld care both for host city residents and for Convention attendees, and generated insights that are being applied to other mass gathering events. Future research must explore the establishment of uniform standards of medical care provision at mass gatherings and NSSEs, including the identification of adequate staffing levels and performance standards, as well as metrics for data gathering.11 Dedication to lessons learned and improving research and evaluation of such efforts for the future can inform public health in the post-September 11 era.
Acknowledgments
The Center for Public Health Preparedness at the Harvard School of Public Health is supported in part by grant number U90/CCU124242-03 from the Centers for Disease Control and Prevention (CDC).
The authors are grateful to Anita Barry, MD, Josh Frances, MPH, Maureen McMahon, MS, RN, Donna Morrissey, and Special Agent Steve Ricciardi for sharing valuable insights and experience during the preparation of this article.
Footnotes
Authors’ Disclosures
The authors report no conflicts of interest.
REFERENCES
- 1.US Secret Service. National Special Security Events. http://www.secretservice.gov/nsse.shtml. Accessed October 3, 2007.
- 2.Department of Homeland Security. DHS Designates President Ford Memorial Service as National Special Security Event. December 28, 2006. http://www.dhs.gov/xnews/releases/pr_1167323576041.shtm. Accessed February 14, 2008.
- 3.Department of Homeland Security. Designation of the President’s State of the Union Address as a National Special Security Event. January 28, 2008. http://www.dhs.gov/xnews/releases/pr_1201541187429.shtm. Accessed February 14, 2008.
- 4.Department of Homeland Security. Fact Sheet: National Special Security Events Memorial Service for President Reagan. June 6, 2004. http://www.dhs.gov/xnews/releases/press_release_0428.shtm. Accessed February 14, 2008.
- 5.Medical Consequence Management Plan: 2004 Democratic National Convention. Command Staff version. Boston: Boston Emergency Medical Services; July 23, 2004. [Google Scholar]
- 6.Department of Homeland Security. Fact Sheet: The Department of Homeland Security Partners With State and Locals to Protect Democratic National Convention. July 14, 2004. http://www.dhs.gov/xnews/releases/press_release_0463.shtm. Accessed February 14, 2008.
- 7.Meehan P, Toomey KE, Drinnon J, Cunningham S, Anderson N, Baker E. Public health response for the 1996 Olympic games. JAMA. 1998; 279:1469–1473. [DOI] [PubMed] [Google Scholar]
- 8.Nelson C, Lurie N, Wasserman J. Assessing public health emergency preparedness: concepts, tools, and challenges. Annu Rev Public Health. 2007;28:1–18. [DOI] [PubMed] [Google Scholar]
- 9.McKenna VB, Gunn JE, Auerbach J, et al. Local collaborations: development and implementation of Boston’s bioterrorism surveillance system. J Public Health Manag Pract. 2003;9:384–393. [DOI] [PubMed] [Google Scholar]
- 10.Mechem CC, Hare S. Hvisdas R, et al. Emergency medical planning for the 2000 Republican National Convention. Prehospital Emergency Care. 2001;5:344–352. [DOI] [PubMed] [Google Scholar]
- 11.Arbon P Mass-gathering medicine: a review of the evidence and future directions for research. Prehosp Disaster Med. 2007;22:131–135. [DOI] [PubMed] [Google Scholar]
- 12.Binder LS, Willoughby PJ, Matkaitis L. Development of a unique decentralized rapid-response capability and contingency mass-casualty field hospital for the 1996 Democratic National Convention. Prehosp Emerg Care. 1997;1:238–245. [DOI] [PubMed] [Google Scholar]
- 13.Reissman S EMS at the Democratic National Convention. J Emerg Med. 1993;18:58–59. [PubMed] [Google Scholar]
- 14.Thal ER, Riggs LM Jr. Community planning for medical support of a national political Convention. J Trauma. 1988;28:799–803. [DOI] [PubMed] [Google Scholar]