

ABSTRACT
BACKGROUND:
Evidence of the benefits of dance for people with Parkinson disease is well established, but only recently has dance been investigated for people with multiple sclerosis (MS). The purpose of this review was to identify and evaluate the feasibility and effectiveness of dance interventions to improve functional, psychosocial, and participation outcomes in people with MS.
METHODS:
Eight databases and gray literature sources were searched from inception to March 2022. Quantitative, mixed-methods, and qualitative studies evaluating dance interventions for adults with MS were included. Included studies were critically appraised using the Mixed Methods Appraisal Tool, and results were analyzed through a parallel-results convergent synthesis.
RESULTS:
Thirteen studies were included, with a total of 174 participants. Various dance genres were investigated, and only 1 mild adverse event was reported. Four to 12 weeks of twice-weekly, 60-minute dance sessions were feasible in those with mild to moderate relapsing-remitting MS. Positive effects were identified mainly in motor outcomes, with qualitative themes indicating psychological and social benefits.
CONCLUSIONS:
A variety of dance interventions are likely feasible and potentially beneficial for people with mild to moderate relapsing-remitting MS, but studies were generally of low-moderate quality. High-quality studies are needed to determine the effectiveness of dance interventions for people with MS, including those with progressive forms of MS and higher levels of disability.
Keywords: multiple sclerosis, dance, dance therapy, dance for health, review
Multiple sclerosis (MS) is a chronic autoimmune inflammatory disease of the central nervous system characterized by neurodegeneration leading to a variety of symptoms and, often, disability.1 A growing number of disease-modifying therapies are available that can help reduce relapse rates and disability severity; however, disease-modifying therapies do not target the multifaceted symptoms of MS or the psychological, emotional, and social consequences of living with an unpredictable degenerative condition.1 Nonpharmacologic and lifestyle interventions are safe and effective for ameliorating common symptoms and improving quality of life for people with MS.1,2 Exercise training, physical activity, cognitive behavioral therapy, and mindfulness-based interventions have been shown to support physical and emotional wellness in people with MS, an identified priority among the MS community.3
Extensive research evidences the benefits of exercise for a range of physical functioning outcomes,4 but there is a low rate of adequate physical activity among people with MS.5 Although a variety of personal and contextual barriers limit their exercise participation, personalized exercise suited to the needs, abilities, goals, and interests of people with MS could help to overcome these barriers.6,7 Mindfulness-based movement practices such as tai chi and yoga have been investigated as alternative, attractive exercise forms for people with MS that may provide physical and psychosocial benefits owing to their movement and meditative components.8,9 Dance is another potentially attractive form of physical activity that generally incorporates types of exercise recommended for people with MS (eg, aerobics, balance, coordination, stretching10) into an enjoyable and emotionally, socially, and artistically enriching experience.11,12
Dance is the synchronization of movement to rhythm, most often characterized by genre, function, or context.13,14 Because dance can be delivered in a variety of forms across different settings and easily tailored to different abilities, it has been characterized as an accessible and adaptable activity.15 Dance interventions have been found to be equally and occasionally more effective than other exercise forms for improving a range of physical health outcomes, including musculoskeletal functions such as mobility and balance.16 Several psychosocial benefits have also been reported from dance interventions, including improvements in stress levels, depressive symptoms, and anxiety17 and positive psychological constructs such as well-being, coping strategies, and self-esteem.13
Research shows that dance yields a variety of physical and psychosocial benefits in populations with other chronic neurologic conditions, such as dementia and Parkinson disease (PD).18,19 Dance has been especially widely investigated in the context of rehabilitation for PD,20 with several systematic reviews demonstrating the effectiveness of dance for improving motor impairments.18,21,22 Given the benefits of dance for PD and the extensive research on the benefits of exercise for MS, there has been a growing practical and research interest in the use of dance for people with MS.23 Literature reviews have been conducted on therapeutic arts for MS24 and music-based therapeutic approaches for MS25; however, to our knowledge, there has yet to be a systematic literature review concerning only dance interventions for people with MS. Therefore, the aim of this study was to systematically review the evidence on the feasibility and effectiveness of dance for improving functional, psychosocial, and participation outcomes in people with MS.
METHODS
The method of this systematic review was developed in accordance with the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guideline.26 The review protocol was registered on the PROSPERO database.
Search Strategy
Searches were performed from inception through March 2022 in MEDLINE, the Allied and Complementary Medicine Database, the Cumulative Index to Nursing and Allied Health Literature, PsycINFO, Web of Science, Scopus, ProQuest Central Health & Medical Collection, and ProQuest Nursing & Allied Health Database. The search strategy was adapted for use in each database (TABLE S1, available online at IJMSC.org). Key terms were built around 2 domains, dance and MS. Due to the anticipated dearth of studies in this area, the database search was complemented by a gray literature search of reference lists of included studies, Conference Proceedings Citation Index, ProQuest Dissertations & Theses Database, Science Citation Index, and Google Scholar (citation searching of included studies). Experts from organizations with publicized community-based dance for MS programs were also contacted to identify evidence that may not appear in academic databases.
Inclusion and Exclusion Criteria
Articles were included if they met the following eligibility criteria: (1) included adults with a diagnosis of MS (formal or self-report), and, if included alongside other clinical populations, data on adults with MS had to be extractable; (2) evaluated an intervention defined as dance or characterized by purposefully selected, rhythmic movement sequences27; and (3) assessed any outcome related to the body function, activity, or participation domains in the World Health Organization’s International Classification of Functioning, Disability, and Health28 or psychosocial aspects such as self-efficacy, well-being, or quality of life. There were no restrictions on the study design or publication period. Gray literature (ie, evaluation reports, unpublished studies, theses) was eligible for inclusion in line with the stance of a recent systematic review on dance for health across the life span12 to allow for all available evidence on the topic to be included.29 Studies were excluded if they were reviews or opinion articles, not full texts, or not available in English or Spanish.
Eligibility Screening
All database and gray literature search results were entered into Covidence systematic review software (Version 2156; Veritas Health Innovation [available at https://www.covidence.org]),30 and duplicates were removed. Two independent reviewers (E.D. and A.W.) screened the titles and abstracts against the selection criteria and then screened full texts of the remaining articles for eligibility. Any disagreements were resolved through discussion among the reviewers or consultation with a third reviewer (L.P.).
Quality Assessment
Quality was assessed using the McGill University Mixed Methods Appraisal Tool (MMAT),31 which was selected to account for the heterogeneity of the study designs. Quality assessment was completed independently by 2 reviewers (E.D. and A.W.), and any disagreements were resolved through consensus in consultation with a third reviewer (L.P.). No studies were excluded based on the result of the quality assessment.
Data Extraction
One reviewer (E.D.) extracted the relevant data from eligible studies using a standardized data extraction table. Data extracted included study details, study design, participant information, intervention characteristics, data collection methods/outcomes, and main findings. Qualitative data such as participant quotes and author interpretations were extracted as individual data.
Data Synthesis
A parallel-results convergent synthesis was conducted: quantitative and qualitative data were analyzed and presented separately, and the integration of the results occurred in the interpretation of the findings.32 The quantitative and qualitative data were analyzed using narrative synthesis following the Economic and Social Research Council Guidance on Conducting Narrative Synthesis.33 Qualitative data were further synthesized using a thematic analysis process adapted from Thomas and Harden,34 in which results were coded line-by-line according to content and meaning, and the resulting codes were organized into descriptive themes and, subsequently, analytical themes. Due to the inclusion of quasi-experimental studies and the heterogeneity of the included quantitative study designs and outcome measures, meta-analysis was not appropriate.
RESULTS
Study Selection
Through the search of the 8 selected databases, 734 studies were identified (FIGURE). After duplicates were removed, 491 studies were screened for relevance. After title and abstract screening, 462 studies were excluded. The remaining 29 studies were retrieved and screened for eligibility; 19 were excluded . An additional 5 records were identified by contacting experts (n = 4) and by citation searching via Google Scholar (n = 1). Four reports were retrieved, and 3 full texts met the eligibility criteria. In total, 13 studies were accepted for inclusion in the review. Seven studies were conducted in the United States, and the other 6 studies were conducted in Spain, Belgium, Scotland, Canada, and Brazil.
FIGURE.
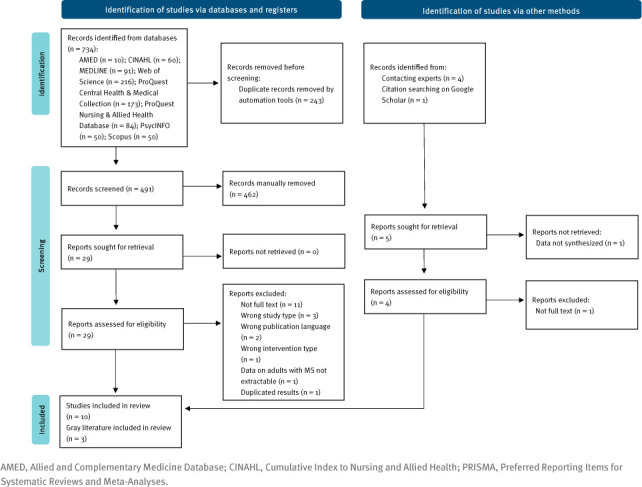
PRISMA of Search Results and Screening
Study Designs
Ten of the included studies used quantitative methods: 1 was a proof-of-concept randomized controlled trial (RCT) with 3 trial arms (ie, movement-to-music, adapted yoga, waitlist control)35; 2 quasi-experimental studies compared dance with visual arts36 or a no-dance control group37; 3 were uncontrolled, before-and-after studies38–40; 1 was a single-case experimental study41; and 3 were descriptive studies (ie, 1 program evaluation42 and 2 case reports43,44) (TABLE). Two studies used mixed methods (ie, master’s thesis45 and program evaluation46). One case study used only qualitative methods.47
TABLE.
Characteristics of Included Studies
| Author, date | Sample characteristics | Intervention characteristics | Main findings | Quality |
|---|---|---|---|---|
| Randomized controlled trial | ||||
| Young et al,35 2019 | 81 (66F/15M); mean age dance group, 49.67 ± 9.40 y; PDDS range, 0–6; mean disease duration, 13.56 ± 8.26 y |
Movement-to-music (n = 27); group, in-person; 60 m × 3/wk for 12 wk Adapted yoga CG (n = 26) Waitlist CG (n = 28) |
Mobility (TUG) and walking endurance (6MWT) improved significantly post intervention compared to waitlist controls. | *** |
| Nonrandomized studies | ||||
| Mandelbaum et al,38 2016 | 8 (5F/3M); age range, 29–63 y; 7 RRMS/1 SPMS; PDDS range, 0–3; disease duration range, 1–22 y |
Salsa dance Group, in-person; 60 m × 2/wk for 4 wk |
Mobility (TUG), balance (DGI), physical activity (GLTEQ), and gait (MSWS-12) improved significantly post intervention and/or at the 3-month follow-up, although MS symptoms worsened significantly post intervention. | *** |
| Scheidler et al,39 2018 | 8 (8F); age range, 36–65 y; all RRMS; EDSS range, 2.5–6.5 |
Targeted ballet Group, in-person; 60 m × 2/wk for 16 wk |
Ataxia (ICARS; smoothness of gait) and balance (MBT; balance in a step-to-stand task in the back direction) improved significantly post intervention. | **** |
| Ng et al,37 2020 | 13 (12F/1M); age range, 40–59 y; 12 RRMS/1 PPMS; PDDS range, 1–4 |
Ballroom dance (n = 7); group, in-person; 60 m × 2/week for 6 weeks; No-dance CG (n = 6) |
Quality of life (PROMIS-GH), cognition (PASAT), and physical function (MSFC) improved significantly post intervention, with no improvements noted in the control group. | **** |
| Van Geel et al,36 2020 | 17 (16F/1M); age range, 29–65 y; disability status, cane (n = 1), walker (n = 2), crutch (n = 1); disease duration range, 3–21 y |
Choreo-based participatory dance (n = 7); group, in-person; 90 m × 2/wk for 10 wk Mixed art CG (n = 10) |
Fatigue (MFIS), lower extremity strength (5XSTS), balance confidence (ABC), gait (MSWS-12), hand function (9HPT-dominant), cognitive performance, and leg coordination improved significantly in the dance group post intervention, with fatigue (MFIS), cognition (SDMT), and cognitive performance improving significantly post intervention in the control art group. | *** |
| Camacho et al,40 2021 | 5 (4F/1M); age range, 38–64 y; all RRMS; EDSS, mean 3.5 ± 1.5 |
Targeted ballet Group, in-person; 60 min × 2/week for 12 weeks |
Ataxia (ICARS; smoothness of gait) and balance (MBT) improved significantly post intervention. | *** |
| Quantitative descriptive studies | ||||
| Salgado and de Paula Vasconcelos,43 2010 | 1 (F); 45 y; RRMS; EDSS, 3; disease duration, 10 y |
Dance/movement therapy 1 on 1, in-person; 100 m × 2/wk for 20 wk |
Neurologic disability (EDSS; MRD; NRS) improved post intervention. |
** |
| Charlton et al,42 2010 | 11 (11F); age range, 32–70 y; disability status, ambulatory without assistance (n = 7), walker use (n = 4) |
Jazzercise Group, in-person; 45 m × 2/wk for 16 wk |
All participants reported experiencing positive changes in energy and mood, and enjoyment and motivation to continue with the dance classes, with most also reporting positive changes in confidence, strength, flexibility, balance, and coordination. | ** |
| Lachance et al,41 2021 | 7 people with reduced mobility (total) including 1 with MS (F; 60 y; walks with limp) |
Clinical dance therapy Group, in-person; 90 min × 2/wk for 12 wk |
Mobility improved significantly in the secondary measures of mobility (MDRT-behind; MBT), but not the primary mobility measure (FSST). | *** |
| Ares-Benítez et al,44 2021 | 1 (F); 49 y; RRMS; EDSS, 5; disease duration, 24 y |
Spanish dance and physiotherapy 1 on 1, in-person; 60 min × 5/wk for 3 wk |
Positive changes were reported in balance (BBS), walking endurance (6MWT), ankle strength (MMT), spasticity in the sural triceps (MAS), and spatiotemporal gait parameters post intervention. | ** |
| Mixed-methods studies | ||||
| Mason,45 2020 | 5 |
Participatory dance Group; in-person; 75 m × 1/wk for 6 wk |
No significant change was reported in self-efficacy (MSSE-10) post intervention, but participants reported experiencing improvements in self-confidence and physical well-being in the exit questionnaire. | * |
| Whiteside and Ruckert,46 2020 | 22 (21F/1M); n = 12 (AM group) and n =10 (PM group); disability status, multiple walking aids, wheelchairs (n = 2) |
Participatory dance Group; in-person; 75 m × 1/wk for 10 wk |
Fatigue (FSS) improved significantly post intervention only in the AM group, but participants reported experiencing improvements in body confidence and awareness, well-being, belonging, and quality of life in interviews. | *** |
| Qualitative study | ||||
| Baeza and Fuertes,47 2022 | 1 (F); 53 y; cane use at home and wheelchair outside; disease duration, 18 y |
Creative movement practice Solo, remote; 100 m × 1/wk for 6 wk |
Participant reported improvements in body confidence, emotional confidence, well-being, and connectedness with family members in interviews. | ** |
5XSTS, 5 Times Sit-to-Stand Test; 6MWT, 6-minute walk test; 9HPT, 9-Hole Peg Test ; ABC, Activities-Specific Balance Confidence Scale; BBS, Berg Balance Scale; CG, control group; DGI, Dynamic Gait Index; EDSS, Expanded Disability Status Scale; F, female; FSS, Fatigue Severity Scale; FSST, 4 Square Step Test; GLTEQ, Godin Leisure Time Exercise Questionnaire; ICARS International Cooperative Ataxia Rating Scale; M, male; MAS, Modified Ashworth Scale; MBT, Mini-Balance Evaluation Systems Test; MDRT, Multi-Directional Reach Test; MFIS, Modified Fatigue Impact Scale; MMT, Daniels-Worthingham manual muscle test; MRD, Minimal Record Disability; MS, multiple sclerosis; MSFC, MS Functional Composite score; MSSE, MS Self-Efficacy Scale; MSWS-12, 12-Item MS Walking Scale; NRS, Neurologic Rating Scale; PASAT, Paced Auditory Serial Addition Test; PDDS, Patient Determined Disease Steps; PPMS, primary progressive MS; PROMIS-GH, Patient-Reported Outcomes Measurement Information System-Global Health; RRMS, relapsing-remitting MS; SPMS, secondary progressive MS; TUG, Timed Up and Go Test; SDMT, Symbol Digit Modalities Test.
*P ≤ .05
Participant Characteristics
Across the 13 studies, 174 participants with MS were included, 81 in 1 study.35 All other studies had small sample sizes, with 4 studies each including only 1 person with MS.41,43,44,47 Type of MS was reported in 6 studies,37–40,43,44 with 95% of participants having relapsing-remitting MS. Across validated and subjective measures of disability status, assessments ranged from no disability to bilateral support (score, 0-6) on the Patient-Determined Disease Steps scale35 and wheelchair use,46,47 with most participants having a mild to moderate disability. Disease duration was reported in 6 studies,35,36,38,43,44,47 with durations ranging from 1 year38 to 24 years.44 Most studies had limited reporting of other sample characteristics (eg, ethnicity, educational level, socioeconomic status, previous dance experience).
Intervention Characteristics
Intervention types ranged from clinical dance therapy41,43 to nonclinical, participatory dance.45,46 Only 2 studies implemented the same intervention type, targeted ballet training.39,40 Two studies investigated partnered dance styles, salsa38 and mixed ballroom.37 Dance-based exercise was also instructed in 2 studies, Jazzercise42 and mixed genre.35 Spanish dance combined with physiotherapy,44 choreography-based dancing showcased in a public performance,36 and creative dance practice47 were investigated by 1 study each. Only 1 intervention was delivered remotely47; most interventions were delivered in a group in a community setting such as fitness facilities.35,42 Interventions ranged from 3 weeks44 to 20 weeks43; the median intervention length was 10 weeks. The average session duration was 71.9 minutes, with 6 interventions delivering hour-long sessions.35,37–40,44 Eight interventions delivered sessions twice weekly.36–43 Only 1 study reported the intensity of the intervention as light to moderate exercise intensity using ratings of perceived exertion and ambulatory heart rate.37 Other studies detailed the relative intensities and purposes of the session’s components (eg, the target fitness, motor, or cognitive domain) and durations of components.35,36,38–40,42 Some studies also described the intervention’s progression, such as incorporating new dance steps38 or progressively increasing the difficulty of dance sequences over the course of the sessions.43,46
Feasibility
When reported, dropouts from the dance intervention ranged from 037,38,40,45 to 3 participants.35,42 Reasons for discontinuing the dance intervention were personal or scheduling conflicts,35,41 transportation challenges,35,42 geographical barriers,42 and unrelated health complications.35,36,39–41 Eight studies reported adherence, with 4 reporting attendance rates greater than 90%.38–40,45 The lowest attendance rates were for the dance-based exercise interventions, mixed genre at 53.7%35 and Jazzercise at 67% to 75%.42 Adherence was not reported in the 1 study delivered remotely.47 Across the 6 studies reporting adverse events,35,37–40,42 dance was well-tolerated, with only 1 study reporting 1 adverse event related to the dance intervention studied, a mild muscle strain treated with rest and ice.35 Studies noted adaptations made to the dance sessions or environment to support adherence and tolerability, including thermoregulation of the dance studio,37,40,42 availability of trained assistants,40,46 and encouragement to rest as needed37,38 (TABLE S2).
Effects of Dance Interventions on Outcome Measures
Functional Outcomes
Balance. Eight of the 13 studies included examined balance.36–42,44 Balance improved in 6 studies after the intervention,38–42,44 including the 3 before-and-after studies that showed statistically significant improvements in the Mini-Balance Evaluation Systems Test results, with large effect sizes compared with baseline,39–41 1 of which also reported a significant change in balance in a backward step-to-stand task.39 One case report of Spanish dance physiotherapy showed a 25-point improvement in the participant’s Berg Balance Scale score after the intervention,44 and another study showed a statistically significant change in the Dynamic Gait Index at 3-month follow-up compared with baseline.38 Three studies examined balance confidence36,38,46 which significantly improved in only 1 study after the intervention in the dance group but not the control art group.36
Gait and gait parameters. Four studies assessed changes in overall walking ability using the 12-item Multiple Sclerosis Walking Scale36,38,46 and the Timed 25-Foot Walk test.36–38 Two of three studies using the scale reported significant improvements.36,38 Three studies evaluated changes in specific gait parameters39,40,44; 2 before-and-after studies showed statistically significant improvements after the intervention in the smoothness of gait,39,40 and a case report showed improvements in spatiotemporal gait parameters (ie, speed, step length, cadence) after the intervention.44
Walking endurance. Three studies assessed changes in walking endurance using the 6-Minute Walk Test.35,36,44 The case report of Spanish dance physiotherapy showed a 37.76-m increase in the participant’s 6-Minute Walk Test after the intervention,44 but only 1 study, an RCT, showed a statistically significant difference in walking endurance between the dance-based exercise group and the waitlist control group; this difference was not observed between the adapted yoga group and controls.35
Functional mobility. Three studies evaluated functional mobility using the Timed Up and Go test.35,37,38 Two studies, 1 RCT and 1 before-and-after study, showed statistically significant improvements in functional mobility.35,38
Ataxia. Two studies measured changes in ataxia, both of which were before-and-after studies of targeted ballet.39,40 The studies demonstrated statistically significant reductions in ataxia after the intervention compared with baseline in clinical and direct assessments.
Extremity function. Two studies assessed lower extremity function using the Five Times Sit-to-Stand Test35,36 (5XSTS) and upper-extremity function using the Nine-Hole Peg Test36,37; one study showed significant improvements after the intervention in the dance group in both the 5XSTS and the Nine-Hole Peg Test in the dominant hand; these improvements were not observed in the control art group.36 This was also the only study to investigate leg coordination, showing a significant increase in the dance group compared with baseline but not in the control art group.
Cognition. Two quasi-experimental studies measured changes in cognitive functioning.36,37 Both studies showed positive changes in performance of the Paced Auditory Serial Addition Test; however, only 1 study demonstrated a statistically significant improvement compared with the no-dance control group,37 with the other study demonstrating only a trend toward significance in both the dance group and the control art group.36 Significant improvements were also reported in this study in executive cognitive performance during dual tasking in both the dance and control art groups after the intervention, but a significant improvement in the Symbol Digit Modalities Test was reported only in the control art group.36
Overall physical functioning and MS symptoms. Three studies evaluated changes in overall physical functioning.37,38,43 One study showed a statistically significant improvement in MS Functional Composite scores after the intervention compared with the control group,37 and a case report demonstrated improvements in 3 clinical assessments of neurologic disability, including a 1-point decrease in the Expanded Disability Status Scale score.43 The only study monitoring changes in MS symptoms, using the MS Symptoms Checklist, showed a statistically significant worsening of MS symptoms after the 4-week intervention, which was not replicated at the 3-month follow-up.38
Other physical functioning outcomes. Two studies assessed overall strength, 1 noting a self-reported overall improvement in strength after the intervention42 and the other citing an improvement in ankle strength only.44 One case report assessed spasticity using the Modified Ashworth Scale, which decreased in both sural triceps after the intervention.44 No significant change was reported in the only study assessing sensory function.36
Psychosocial and Participation Outcomes
Fatigue. Four of the 13 included studies assessed fatigue35–37,46; only 1 study examined fatigue as the primary outcome.36 This study demonstrated statistically significant improvements in the Modified Fatigue Impact Scale after the intervention in both the dance and control art groups compared with baseline but no significant changes in performance motor fatigability or cognitive fatigability.36 One before-and-after study showed a significant improvement in the Fatigue Severity Scale score after the intervention in the morning dance group but not in the evening dance group.46 The other 2 studies demonstrated positive trends toward significance not observed in their waitlist35,37 or active control groups.35
Quality of life. Two studies assessed quality of life.36,37 One study reported a significant change in the Patient-Reported Outcomes Measurement Information System–Global Health score in the dance intervention group compared with controls,37 and the other showed a positive statistical trend after the intervention in the 29-item Multiple Sclerosis Impact Scale score in the dance group not observed in the control art group.36
Self-efficacy, pain, and mental health. Three studies assessed self-efficacy,37,38,45 and changes in pain,35 depression,37 and dimensions of mental health and well-being42 were each measured by 1 study. No significant changes were reported after the interventions in validated assessments, but 78% to 100% of participants in 1 study reported experiencing positive changes in confidence, energy, and mood.42
Physical activity. One study examined physical activity, reporting statistically significant improvements in total leisure activity ratings (time and metabolic equivalents) after the intervention compared with baseline.38
Thematic Synthesis of Qualitative Findings on the Effects of Dance Interventions
Three studies included qualitative analyses, 2 mixed-methods studies45,46 and 1 qualitative study.47 Qualitative methods used included interviews,46,47 participant observations,46 and an open-ended questionnaire.45 Four themes concerning perceived effects were identified across the included qualitative data: body awareness and physical confidence, psychological well-being, sense of belonging, and social relationships (TABLE S3).
Theme 1: Body Awareness and Physical Confidence
Participants experienced an improved sense of body awareness and physical confidence during the dance sessions46,47 and when completing daily activities.45,46 They explained that dancing helped them become more “in tune” with their bodies and better understand how to cope with movement limitations and motor fatigue.45–47 Some in-person dance program participants reported that dance helped them when navigating physical challenges in their daily lives.
Theme 2: Psychological Well-being
In-person or remote dance sessions resulted in positive emotions and improved mental states among participants. Afterward, they said they were “feeling good”46,47 and “feeling better, more energetic.”45 The studies associated these positive emotional changes with the enjoyable and expressive nature of the sessions. Some participants said that the sense of well-being and achievement after the sessions outweighed or lessened their fatigue.45–47 Sustained improvements in self-esteem were also reported across the studies.45–47 For in-person participants, these self-esteem improvements were attributed to the encouraging dance class environment and sense of achievement felt after mastering dance skills.45,46
Theme 3: Sense of Belonging
Participants reported feeling an increased sense of belonging as a result of taking part in remote or in-person dance sessions.45–47 Feelings of belonging emerged from feeling safe and comfortable practicing movements at home47 or feeling accepted, understood, and included in the dance class environment.45,46 Dancing in a group in-person setting provided the additional benefit of connecting with like-minded individuals.46
Theme 4: Social Relationships
Dance also provided the opportunity for participants to create or enhance interpersonal relationships.45–47 Remote dancing provided a meaningful way for the case study participant to connect creatively with her family members,47 and the in-person dance classes facilitated the development of new social relationships with other participants.45,46
Quality Assessment
Because presenting solely an overall score is discouraged by the MMAT, an overall score is provided alongside a summary of justification for each criterion in the MMAT.31 Two studies were moderate-high quality (80% of the quality criteria met),37,39 6 were moderate quality (60% of the quality criteria met),35,36,38,40,41,46 and 5 were low quality (≤40% of the quality criteria met)42–45,47 (Table 1). The case reports, case study, master’s thesis, and program evaluations were generally of lower quality than the quantitative studies due to uncertainty or problems regarding the sampling strategy,41–46 problems with mixed-methods data integration45 or qualitative data presentation and coherence,47 and limitations in the outcome measures42 or statistical analysis used43,44 (TABLE S4). The only RCT was limited by incomplete outcome measures and low adherence rates.35 Although of moderate to moderate-high quality, quantitative, nonrandomized studies were limited by biased participant sampling,36,37 and quantitative, uncontrolled studies were further limited by inadequate reporting on adherence and any unplanned or cointerventions.38–40
DISCUSSION
The aim of the present study was to systematically review the evidence regarding the feasibility and effectiveness of dance interventions for people with MS. Evidence included a range of study designs and gray literature to allow for a comprehensive evaluation of a complex intervention in an area where current research is limited and RCTs may not always be appropriate or sufficient.32 Findings are positive regarding the feasibility of a wide range of dance interventions for people with MS; however, evidence of effectiveness is weak due to the large heterogeneity of the intervention and study designs, the low power of the quantitative studies, and the low-moderate methodological quality of most of the included studies. Consequently, conclusions must be drawn with caution.
Across the 6 studies reporting adverse events that included 70% of the participants, only 1 study reported 1 mild adverse event related to the dance intervention,35 indicating that dance is likely safe and tolerable for people with MS. This finding is comparable with other reviews showing that dance is safe and tolerable for people with other progressive neurologic conditions, such as PD.15,18 When reported, the levels of adherence for most included studies were greater than 90%, with the lowest adherence rates for the dance-based exercise programs.35,42 This discrepancy suggests that genre-specific or participatory dance programs may encourage higher levels of adherence than exercise programs that incorporate dance movements and music. Some participants also continued or expressed a desire to continue with the community-based programs after the intervention period,36–38,46 indicating that dance programs could promote sustained physical activity behavior in people with MS. Most participants had mild to moderate relapsing-remitting MS, but other participants were wheelchair users, suggesting that, when appropriately adapted, dance could provide an accessible physical activity option across a range of disability severities.
The quantitative studies all reported some improvements in multiple functional outcome measures. Generally, 50% or more of studies assessing a certain outcome measure reported improvements. Significant gains were predominantly reported in physical and functional outcomes, with fewer studies assessing changes in other domains (eg, sensory and cognitive function). The mobility-targeted dance interventions generally reported greater gains in functional outcomes than more holistic dance interventions. Some mobility changes in the 12-item Multiple Sclerosis Walking Scale,36,38 6-Minute Walk Test,36 Berg Balance Scale,44 and Mini-Balance Evaluation Systems Test39,40 exceeded the minimal clinically important difference. Although all of these studies were underpowered and most were uncontrolled, they demonstrated positive effects across self-report and performance assessments of mobility, with 2 studies investigating mobility-targeted ballet showing larger effect sizes than those reported in other gait, balance, and functional training interventions using similar balance measures.48 Clinically meaningful improvements were also reported in lower extremity function (5XSTS)36 and neurologic disability (Expanded Disability Status Scale).43
Improvements in cognition (Paced Auditory Serial Addition Test) were reported in 2 studies,36,37 but these improvements were significant only when compared with a waitlist control group.37 The only clinically meaningful improvement in cognition (via the Symbol Digit Modalities Test) was reported in a study’s control art group, not in the dance group.36 Accordingly, it is unclear whether dance is as effective as other leisure or physical activities in improving certain outcomes, such as cognition. One study reported a significant worsening of MS symptoms as assessed by the MS Symptoms Checklist after 4 weeks of dance but not at the 3-month follow-up.38 This finding indicates that certain dance interventions could be detrimental to MS symptoms, albeit the MS Symptoms Checklist does not assess changes in common MS symptoms (eg, mobility challenges) as rigorously as symptom-specific measures for which some positive, significant results were reported after the dance interventions across the studies.
Qualitative data suggest that dance has the potential to support activities of daily living, but these results primarily showed perceived improvements in the psychosocial and participation domains. Responses from a questionnaire-based study indicated that participants experienced psychological changes in energy, mood, and self-confidence more strongly than physical changes in balance, strength, and coordination.42 Improvements in fatigue were reported across the quantitative and qualitative data; however, it is uncertain whether the significant changes in fatigue reported in 2 of the 4 quantitative studies assessing fatigue are due to the dance intervention specifically.36,46 Although the quantitative results do not clearly indicate a benefit of dance to fatigue, likely due to the studies being underpowered to detect significant change, qualitative findings suggest that participants experienced improved energy mood states after dance sessions.45,46 The varying participant experiences reiterate the complexity of fatigue as a multidimensional outcome and the challenge of differentiating MS-specific fatigue, physical activity-induced fatigue, and energy-related mood states.49,50 These findings also align with the literature on dance for people with cancer in showing some significant effects on disease-related fatigue alongside positive changes in emotional functioning.51,52
Although functional outcomes were generally the focus of quantitative studies, qualitative studies focused more on psychosocial outcomes. Quality of life improved significantly after the intervention in only 1 of 2 quantitative studies assessing this outcome,37 but qualitative data indicate that dance may improve aspects of psychosocial functioning by boosting psychological well-being, promoting belonging, and enhancing social relationships.45–47 Positive affect and social integration can act as a buffer to distress and improve outcomes such as quality of life53,54; however, positive psychological assessments were not used in quantitative studies, with only 1 study assessing changes in depression.37
Quantitative results showed no effects of dance on self-efficacy,37,38,45 but qualitative findings suggest that dance could enhance the 4 sources of self-efficacy characterized by Bandura55 in allowing participants to experience self-accomplishment (1 - mastery), see peers succeed (2 - vicarious experiences), receive positive feedback (3 - verbal persuasion), and experience improved well-being (4 - physiological and affective states).45 One study using the Multiple Sclerosis Self-Efficacy Scale explained that the lack of an effect could be attributed to a “ceiling effect” owing to sampling bias for people with already adequate self-efficacy of their MS symptoms, function, and exercise participation.37 It is also possible that MS-specific self-efficacy was not affected by dance but that dance could affect general or coping self-efficacy.
Although a wide range of dance interventions generally resulted in multiple perceived improvements, given the heterogeneity of the included intervention designs, no conclusions could be drawn on the optimal design of dance for MS interventions. The most common intervention frequency and duration (ie, twice-weekly 60-minute sessions for 4–12 weeks) was feasible and sufficient to see some significant changes in the outcomes studied. This finding aligns with current evidence-based guidelines that moderate-intensity exercise performed twice weekly may result in health benefits for people with MS,56 but there is insufficient evidence to determine what types of dance included in this review are of moderate intensity, with only 1 study characterizing ballroom dance as light to moderate exercise intensity.37 Interpretation is especially limited because characteristics other than dance genre (eg, music tempo) may influence intervention intensity, similar to cycling at different speeds. Most studies detailed the progression and specificity of intervention components, but the wide heterogeneity limited consideration of the influence of specific factors such as partnering, socialization, class structure, and dance genre on intervention feasibility and effectiveness. Only 1 intervention was delivered remotely, providing inadequate information to determine the feasibility and effectiveness of remote dance interventions.
Limitations of the Evidence and Review
This review’s findings are limited by the generally low-moderate quality of the studies and the heterogeneity of methodological designs, intervention types, sampling, and outcomes across the studies. The conclusions that can be drawn are limited as only 1 exploratory RCT was included, approximately one-third of the studies were case studies or reports, and all of the quasi-experimental studies were underpowered pilot studies. Certain study designs, particularly the uncontrolled studies and the single-case experimental study, were challenging to assess against the MMAT criteria, potentially affecting the accuracy of the quality assessment. Because only 2 studies used active control groups, yoga or art,35,36 and only 1 study considered the long-term effects of dance,38 there is insufficient evidence to compare the effects of dance to other interventions or to understand whether any effects may be sustained after the intervention. The representativeness of the samples was unclear given that only 2 participants with progressive MS types were included,37,38 participants were often biased toward people with mild to moderate MS,35,37,38,40,43 and there was mixed reporting on other demographic characteristics. Although most participants had mild to moderate MS, some of the sample populations included participants with a wide range of MS severity, meaning that the intervention and outcome measures may have been more appropriate for some participants than for others. Certain outcome measures (eg, Berg Balance Scale,37,38 Dynamic Gait Index,37 Multiple Sclerosis Self-Efficacy Scale37,45) were subject to ceiling effects in some studies, and some measures could have been subject to pre-, postfamiliarization. Owing to the limited number of studies reporting the same outcome measure, it was not possible to perform a meta-analysis, an important step for future studies. During the qualitative synthesis, although reflexivity was practiced, a priori assumptions may have influenced the grouping and coding process. Lastly, the review was restricted to studies written in English and Spanish.
Future Research
High-quality RCTs using consistent outcome measures are needed to determine the effectiveness of dance in improving functional, psychosocial, and participation outcomes in people with MS compared with more established forms of adjunct therapy. Different methodological designs should be used to investigate the sustained impact of dance for MS, the optimal dance session component intensities and class structure, and the influence of specific factors of dance sessions, such as music tempo, socialization, and dance genre. Future studies should consider targeting individuals with progressive MS forms and more severe disability statuses and incorporating positive psychosocial outcomes such as social support and self-efficacy, which are applicable to people experiencing a range of disability severities. Remote dance instruction should also be further investigated as a physical activity option for people with MS that minimizes environmental barriers. Further qualitative and mixed-methods research is significant to provide a more comprehensive understanding of the impact of dance on people with MS in examining how and why dance might support people with MS and in what contexts.
CONCLUSION
Recognizing the limited evidence base on dance for people with MS, this review, the first on dance for MS, took a broad approach, including a range of study designs and grey literature. The findings provide promising preliminary evidence that a variety of dance interventions are feasible and may improve aspects of physical and psychosocial functioning for people living with mild to moderate relapsing-remitting MS; however, the heterogeneity among the reviewed studies, primarily centered on methodological rigor, intervention type, and outcomes assessed, limited the conclusions that can be drawn regarding effectiveness. Further high-quality, fully powered RCTs are needed to determine the effectiveness of dance interventions for people with MS.
PRACTICE POINTS
Structured dance is likely a safe and feasible physical activity for people with mild to moderate relapsing-remitting multiple sclerosis.
Dance may improve functional and psychosocial outcomes in people with mild to moderate relapsing-remitting multiple sclerosis.
Supplementary Material
Funding Statement
FUNDING/SUPPORT: Ms Davis is funded by a scholarship from the Thouron Award. Ms Webster is funded by the Multiple Sclerosis (MS) Society, UK (grant 115).
Footnotes
FINANCIAL DISCLOSURES: The authors declare no conflicts of interest.
PRIOR PRESENTATION: A part of this review was presented as a poster at the Annual Conference of the International Association for Dance Medicine and Science; October 28-31, 2022; Limerick, Ireland.
REFERENCES
- 1.Thompson AJ, Baranzini SE, Geurts J, Hemmer B, Ciccarelli O. Multiple sclerosis. Lancet . 2018;391(10130):1622–1636. doi: 10.1016/S0140-6736(18)30481-1. [DOI] [PubMed] [Google Scholar]
- 2.Jakimovski D, Guan Y, Ramanathan M, Weinstock-Guttman B, Zivadinov R. Lifestyle-based modifiable risk factors in multiple sclerosis: review of experimental and clinical findings. Neurodegener Dis Manag . 2019;9(3):149–172. doi: 10.2217/nmt-2018-0046. [DOI] [PubMed] [Google Scholar]
- 3.Dunn M, Bhargava P, Kalb R. Your patients with multiple sclerosis have set wellness as a high priority-and the National Multiple Sclerosis Society is responding. US Neurol . 2015;11(2):80–86. doi: 10.17925/USN.2015.11.02.80. [DOI] [Google Scholar]
- 4.Motl RW, Sandroff BM, Kwakkel G et al. Exercise in patients with multiple sclerosis. Lancet Neurol . 2017;16(10):848–856. doi: 10.1016/S1474-4422(17)30281-8. [DOI] [PubMed] [Google Scholar]
- 5.Kinnett-Hopkins D, Adamson B, Rougeau K, Motl RW. People with MS are less physically active than healthy controls but as active as those with other chronic diseases: an updated meta-analysis. Mult Scler Relat Disord . 2017;13:38–43. doi: 10.1016/j.msard.2017.01.016. [DOI] [PubMed] [Google Scholar]
- 6.Asano M, Duquette P, Andersen R, Lapierre Y, Mayo NE. Exercise barriers and preferences among women and men with multiple sclerosis. Disabil Rehabil . 2013;35(5):353–361. doi: 10.3109/09638288.2012.742574. [DOI] [PubMed] [Google Scholar]
- 7.Moffat F, Paul L. Barriers and solutions to participation in exercise for moderately disabled people with multiple sclerosis not currently exercising: a consensus development study using nominal group technique. Disabil Rehabil . 2019;41(23):2775–2783. doi: 10.1080/09638288.2018.1479456. [DOI] [PubMed] [Google Scholar]
- 8.Burschka JM, Keune PM, Oy UH, Oschmann P, Kuhn P. Mindfulness-based interventions in multiple sclerosis: beneficial effects of Tai Chi on balance, coordination, fatigue and depression. BMC Neurol . 2014;14:165. doi: 10.1186/s12883-014-0165-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Shohani M, Kazemi F, Rahmati S, Azami M. The effect of yoga on the quality of life and fatigue in patients with multiple sclerosis: a systematic review and meta-analysis of randomized clinical trials. Complement Ther Clin Pract . 2020;39:101087. doi: 10.1016/j.ctcp.2020.101087. [DOI] [PubMed] [Google Scholar]
- 10.Halabchi F, Alizadeh Z, Sahraian MA, Abolhasani M. Exercise prescription for patients with multiple sclerosis; potential benefits and practical recommendations. BMC Neurol . 2017;17:185. doi: 10.1186/s12883-017-0960-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Dhami P, Moreno S, DeSouza JF. New framework for rehabilitation – fusion of cognitive and physical rehabilitation: the hope for dancing. Front Psychol . 2015;5:1478. doi: 10.3389/fpsyg.2014.01478. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Chappell K, Redding E, Crickmay U, Stancliffe R, Jobbins V, Smith S. The aesthetic, artistic and creative contributions of dance for health and wellbeing across the lifecourse: a systematic review. Int J Qual Stud Health Wellbeing . 2021;16(1):1950891. doi: 10.1080/17482631.2021.1950891. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Murcia C, Kreutz G, Clift S, Bongard S. Shall we dance? an exploration of the perceived benefits of dancing on well-being. Arts Health . 2010;2:149–163. doi: 10.1080/17533010903488582. [DOI] [Google Scholar]
- 14.Fortin S. Tomorrow’s dance and health partnership: the need for a holistic view. Res Dance Educ . 2018;19(2):152–166. doi: 10.1080/14647893.2018.1463360. [DOI] [Google Scholar]
- 15.Emmanouilidis S, Hackney ME, Slade SC, Heng H, Jazayeri D, Morris ME. Dance is an accessible physical activity for people with Parkinson’s disease. Parkinsons Dis . 2021;2021:e7516504. doi: 10.1155/2021/7516504. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Fong Yan A, Cobley S, Chan C et al. The effectiveness of dance interventions on physical health outcomes compared to other forms of physical activity: a systematic review and meta-analysis. Sports Med . 2018;48(4):933–951. doi: 10.1007/s40279-017-0853-5. [DOI] [PubMed] [Google Scholar]
- 17.Salihu D, Kwan RYC, Wong EML. The effect of dancing interventions on depression symptoms, anxiety, and stress in adults without musculoskeletal disorders: an integrative review and meta-analysis. Complement Ther Clin Pract . 2021;45:101467. doi: 10.1016/j.ctcp.2021.101467. [DOI] [PubMed] [Google Scholar]
- 18.Shanahan J, Morris ME, Bhriain ON, Saunders J, Clifford AM. Dance for people with Parkinson disease: what is the evidence telling us. Arch Phys Med Rehabil . 2015;96(1):141–153. doi: 10.1016/j.apmr.2014.08.017. [DOI] [PubMed] [Google Scholar]
- 19.Guzmán-García A, Hughes JC, James IA, Rochester L. Dancing as a psychosocial intervention in care homes: a systematic review of the literature. Int J Geriatr Psychiatry . 2013;28(9):914–924. doi: 10.1002/gps.3913. [DOI] [PubMed] [Google Scholar]
- 20.Bruyneel AV. Effects of dance activities on patients with chronic pathologies: scoping review. Heliyon . 2019;5(7):e02104. doi: 10.1016/j.heliyon.2019.e02104. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Carapellotti AM, Stevenson R, Doumas M. The efficacy of dance for improving motor impairments, non-motor symptoms, and quality of life in Parkinson’s disease: a systematic review and meta-analysis. PLoS One . 2020;15(8):e0236820. doi: 10.1371/journal.pone.0236820. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Ismail SR, Lee SWH, Merom D et al. Evidence of disease severity, cognitive and physical outcomes of dance interventions for persons with Parkinson’s Disease: a systematic review and meta-analysis. BMC Geriatr . 2021;21(1):503. doi: 10.1186/s12877-021-02446-w. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Sonke J, Langley J, Whiteside B et al. Movement for multiple sclerosis: a multi-site partnership for practice and research. Arts Health . 2021;13(2):204–212. doi: 10.1080/17533015.2020.1852435. [DOI] [PubMed] [Google Scholar]
- 24.Gallagher LM, Bethoux F. Therapeutic use of the arts for patients with multiple sclerosis. US Neurol . 2017;13(2):82–89. https://doi.org/10.17925/USN.2017.13.02.82 . [Google Scholar]
- 25.Lopes J, Keppers II. Music-based therapy in rehabilitation of people with multiple sclerosis: a systematic review of clinical trials. Arq Neuropsiquiatr . 2021;79(6):527–535. doi: 10.1590/0004-282X-ANP-2020-0374. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Page MJ, McKenzie JE, Bossuyt PM et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ . 2021;372:n71. doi: 10.1136/bmj.n71. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Kreutz G, Murcia CQ. Dance and health: exploring interactions and implications. In: MacDonald R, Kreutz G, Mitchell L, editors. Music Health & Wellbeing . Oxford University Press; 2012. pp. 125–135. [DOI] [Google Scholar]
- 28.International Classification of Functioning, Disability and Health (ICF) World Health Organization. 2001. Accessed May 12, 2022. https://apps.who.int/iris/handle/10665/42407.
- 29.Paez A. Gray literature: an important resource in systematic reviews. J Evid Based Med . 2017;10(3):233–240. doi: 10.1111/jebm.12266. [DOI] [PubMed] [Google Scholar]
- 30. Covidence Systematic Review Software . Version 2156. [Google Scholar]
- 31.Hong QN, Fàbregues S, Bartlett G et al. The Mixed Methods Appraisal Tool (MMAT) version 2018 for information professionals and researchers. Educ Inf . 2018;34(4):285–291. doi: 10.3233/EFI-180221. [DOI] [Google Scholar]
- 32.Hong QN, Pluye P, Bujold M, Wassef M. Convergent and sequential synthesis designs: implications for conducting and reporting systematic reviews of qualitative and quantitative evidence. Syst Rev . 2017;6(1):61. doi: 10.1186/s13643-017-0454-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Popay J, Roberts H, Sowden A, et al. Guidance on the Conduct of Narrative Synthesis in Systematic Reviews . Lancaster University; 2006. [Google Scholar]
- 34.Thomas J, Harden A. Methods for the thematic synthesis of qualitative research in systematic reviews. BMC Med Res Methodol . 2008;8:45. doi: 10.1186/1471-2288-8-45. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Young HJ, Mehta TS, Herman C, Wang F, Rimmer JH. The effects of M2M and adapted yoga on physical and psychosocial outcomes in people with multiple sclerosis. Arch Phys Med Rehabil . 2019;100(3):391–400. doi: 10.1016/j.apmr.2018.06.032. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Van Geel F, Van Asch P, Veldkamp R, Feys P. Effects of a 10-week multimodal dance and art intervention program leading to a public performance in persons with multiple sclerosis: a controlled pilot-trial. Mult Scler Relat Disord . 2020;44:102256. doi: 10.1016/j.msard.2020.102256. [DOI] [PubMed] [Google Scholar]
- 37.Ng A, Bunyan S, Suh J et al. Ballroom dance for persons with multiple sclerosis: a pilot feasibility study. Disabil Rehabil . 2020;42(8):1115–1121. doi: 10.1080/09638288.2018.1516817. [DOI] [PubMed] [Google Scholar]
- 38.Mandelbaum R, Triche EW, Fasoli SE, Lo AC. A pilot study: examining the effects and tolerability of structured dance intervention for individuals with multiple sclerosis. Disabil Rehabil . 2016;38(3):218–222. doi: 10.3109/09638288.2015.1035457. [DOI] [PubMed] [Google Scholar]
- 39.Scheidler AM, Kinnett-Hopkins D, Learmonth YC, Motl R, López-Ortiz C. Targeted ballet program mitigates ataxia and improves balance in females with mild-to-moderate multiple sclerosis. PLoS One . 2018;13(10):e0205382. doi: 10.1371/journal.pone.0205382. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Camacho PB, Sutton BP, López-Ortiz C. Brain connectivity and motor improvements after ballet intervention in multiple sclerosis: pilot. medRxiv . 2021 doi: 10.1101/2021.03.10.21252757. 2021.03.10.21252757. [DOI] [Google Scholar]
- 41.Lachance B, Fortin S, Bier N, Swaine B. Exploring the impact of a clinical dance therapy program on the mobility of adults with a neurological condition using a single-case experimental design. Arts Health . 2021;13(3):278–295. doi: 10.1080/17533015.2020.1802606. [DOI] [PubMed] [Google Scholar]
- 42.Charlton M, Gabriel K, Munsinger T, Schmaderer L, Healey K. Program evaluation results of a structured group exercise program in individuals with multiple sclerosis. Int J MS Care . 2010;12(2):92–96. doi: 10.7224/1537-2073-12.2.92. [DOI] [Google Scholar]
- 43.Salgado R, de Paula Vasconcelos LA. The use of dance in the rehabilitation of a patient with multiple sclerosis. Am J Dance Ther . 2010;32(1):53–63. doi: 10.1007/s10465-010-9087-x. [DOI] [Google Scholar]
- 44.Ares-Benítez I, Luque-Moreno C, Alonso-Enríquez L et al. Physical therapy and Spanish dance in the reeducation of gait disturbances in multiple sclerosis: a case report. Rev Cient Soc Enferm Neurol (English ed) . 2021;54:46–50. doi: 10.1016/j.sedeng.2020.03.002. [DOI] [Google Scholar]
- 45.Mason K. Exploring the Impact of Dance on SelfEfficacy for People with MS A Feasibility Study. 2020 Master’s thesis. University of Florida; [Google Scholar]
- 46.Whiteside B, Ruckert C. Elevate: exploring the impact of a dance for multiple sclerosis programme. Scottish Ballet. June 2020. https://www.scottishballet.co.uk/actions/supercoolTools/downloadFile?id=56616.
- 47.Baeza MA, Fuertes AP. Expresión corporal, danza y esclerosis múltiple: beneficios emocionales en una intervención durante la contingencia de la COVID-19. Retos nuevas tendencias en educación física deporte y recreación . 2022;(45):34–42. doi: 10.47197/challenges.v45i0.91470. [DOI] [Google Scholar]
- 48.Gunn H, Markevics S, Haas B, Marsden J, Freeman J. Systematic review: the effectiveness of interventions to reduce falls and improve balance in adults with multiple sclerosis. Arch Phys Med Rehabil . 2015;96(10):1898–1912. doi: 10.1016/j.apmr.2015.05.018. [DOI] [PubMed] [Google Scholar]
- 49.Loy BD, Cameron MH, O’Connor PJ. Perceived fatigue and energy are independent unipolar states: supporting evidence. Med Hypotheses . 2018;113:46–51. doi: 10.1016/j.mehy.2018.02.014. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 50.Dittner AJ, Wessely SC, Brown RG. The assessment of fatigue: a practical guide for clinicians and researchers. J Psychosom Res . 2004;56(2):157–170. doi: 10.1016/S00223999(03)00371-4. [DOI] [PubMed] [Google Scholar]
- 51.Karkou V, Dudley-Swarbrick I, Starkey J et al. Dancing with health: quality of life and physical improvements from an EU collaborative dance programme with women following breast cancer treatment. Front Psychol . 2021;12:635578. doi: 10.3389/fpsyg.2021.635578. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 52.Sturm I, Baak J, Storek B, Traore A, Thuss-Patience P. Effect of dance on cancer-related fatigue and quality of life. Support Care Cancer . 2014;22(8):2241–2249. doi: 10.1007/s00520-014-2181-8. [DOI] [PubMed] [Google Scholar]
- 53.Latinsky-Ortiz EM, Strober LB. Keeping it together: the role of social integration on health and psychological well-being among individuals with multiple sclerosis. Health Soc Care Community . 2022;30(6):e4074–e4085. doi: 10.1111/hsc.13800. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 54.Murray K, Melchiorre G, Dobbin A, Welch KA. Positive mental training in patients with multiple sclerosis experiencing psychological distress: a preliminary randomised controlled trial. medRxiv . 2021 doi: 10.1101/2021.07.15.21260604. 2021.07.15.21260604. [DOI] [Google Scholar]
- 55.Bandura A. Self-efficacy: toward a unifying theory of behavioral change. Psychol Rev . 1977;84(2):191–215. doi: 10.1037//0033-295x.84.2.191. [DOI] [PubMed] [Google Scholar]
- 56.Latimer-Cheung AE, Martin Ginis KA, Hicks AL et al. Development of evidence-informed physical activity guidelines for adults with multiple sclerosis. Arch Phys Med Rehabil . 2013;94(9):1829–1836.e7. doi: 10.1016/j.apmr.2013.05.015. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.