

Abstract
Background
Goal setting aids health-related behavior changes; however, the influence of different types of goals on weight loss remains unclear.
Objective
We aimed to investigate the association of 3 aspects of goal setting with weight and program dropout over a 24-week period.
Methods
This study was a prospective longitudinal analysis of participants in a 12-week digital behavioral weight loss program. Weight and engagement data for eligible participants (N=36,794) were extracted from the database. Eligible participants were adults in the United Kingdom who had enrolled in the program, had a BMI ≥25 kg/m2, and a weight reading recorded at baseline. Three aspects of goal setting were self-reported at enrollment: weight loss motivation (appearance, health, fitness, or self-efficacy), overall goal preference (low, medium, or high), and percentage weight loss goal (<5%, 5%-10%, or >10%). Weight was measured at 4, 12, and 24 weeks. Mixed models for repeated measures were used to explore the association between goals and weight across the 24-week period. To measure sustained weight change, the primary outcome was weight at 24 weeks. We explored dropout rates over the 24-week period by goal and whether engagement mediated the association between goals and weight loss.
Results
Of the 36,794 participants (mean 46.7, SD 11.1 years; 33,902/36,794, 92.14% female) included in the cohort, 13.09% (n=4818) reported weight at 24 weeks. Most participants set goals of 5%-10% weight loss (23,629/36,794, 64.22%), but setting goals for >10% was associated with greater weight loss (mean difference 5.21 kg, 95% CI 5.01-5.41; P<.001). There was no difference between goals of 5%-10% and <5% (mean difference 0.59 kg, 95% CI 0.00-1.18; P=.05). Appearance was the most prevalent motivational factor (14,736/36,794, 40.05%), but health and fitness were associated with greater weight losses (mean difference health vs appearance 1.40 kg, 95% CI 1.15-1.65; P<.001 and mean difference fitness vs appearance 0.38 kg, 95% CI 0.05-0.70; P=.03). Goal preference had no association with weight. Engagement was an independent predictor of weight loss but not a mediator of the effect of goal setting. At 24 weeks, those who set goals of >10% were less likely to drop out compared with 5%-10% goals (odds ratio [OR] 0.40, 95% CI 0.38-0.42; P<.001); those who liked to set overall high goals were more likely to drop out compared with medium goals (OR 1.20, 95% CI 1.11-1.29; P<.001); and those motivated by fitness or health were less likely to drop out compared with appearance (OR 0.92, 95% CI 0.85-0.995; P=.04 and OR 0.84, 95% CI 0.78-0.89; P<.001, respectively).
Conclusions
Setting higher weight loss goals and being motivated by health or fitness were associated with greater weight loss and lower likelihood of dropout. Randomized trials for setting these types of goals are required to confirm causality.
Keywords: obesity, overweight, weight loss, goals, motivation, mobile app, mobile health, mHealth, behavior change, mobile phone
Introduction
Background
Goal setting is an important motivational factor underlying changes in health behavior [1]. Goal setting theory is based on the principle that conscious goals direct attention and action, and that conscious behavior is regulated by an individual’s goals [2,3]. Setting a weight loss goal has been shown to lead to greater weight loss than not setting a goal [4], prescribing a higher physical activity goal has been shown to lead to greater weight loss [5], and interventions that incorporate both goal setting and self-monitoring have been found to be more effective at promoting health behaviors than interventions without these techniques [6].
The study of goal setting in the context of weight loss is particularly relevant, given the disparity between what physicians and patients who are overweight and obese consider a realistic goal. A 5%-10% reduction in weight is widely accepted as clinically meaningful because of associated improvements in cardiometabolic risk factors and is recommended by current guidelines as a weight loss target for people who are overweight or obese [7-9]. However, overweight and obese individuals regularly set weight loss goals 3 to 4 times (22%-34% weight reduction) greater than what is recommended [10-13].
There is some uncertainty regarding the best strategy for incorporating goals into behavioral programs for weight loss. On the basis of the findings from the broader goal setting literature, when goals are too ambitious, individuals experience impaired performance, which often leads to abandonment of the goal [14,15]. In the context of obesity research, retrospective studies have found that setting larger weight loss goals may result in poor weight loss maintenance [16,17]. Similarly, setting larger weight loss goals was associated with higher rates of attrition from therapy and smaller reductions in BMI after 12 months of treatment for obesity [12,18,19]. Meanwhile, other studies found either no relationship or a modest positive relationship between setting larger weight loss goals and achieved weight losses [11,20-23] and no relationship between failure to meet weight loss goals and attrition [22,24]. Previous studies of weight loss goals had small sample sizes and it is possible that the importance of goal setting differs across different behavioral programs.
It may also be important to consider how the perceived magnitude of an individual’s goal relates to weight outcomes. Failure to meet weight loss goals that are perceived as realistic may have a greater impact on long-term success than failure to meet ambitious goals, which individuals may recognize are less attainable. However, studies have reported mixed results in terms of outcomes. Women who are overweight and obese have been reported to lose more weight when their pretreatment weight loss expectations are high [25]. Similarly, participants who were instructed to set realistic lower goals lost less weight than those instructed to set unrealistic higher goals, which were 1.5 times higher [26]. No association was found between goal weights and outcomes, but dream weights (which participants perceived as less likely to achieve than goal weights) were associated with greater weight loss at 18 months [11]. Conversely, the observation that dream BMI, but not acceptable or expected BMI, was negatively associated with BMI change at 1 year shows that goals that are perceived as high may have a negative impact on the weight loss achieved [18]. However, this observation may be driven by the greater attrition rate among participants with higher weight loss expectations [18].
Motivation is a key psychosocial factor that influences weight loss success [27,28]. Frequently reported motivational factors for losing weight include improving physical appearance and health [18,24,29,30] and wanting to feel better about oneself [30,31]. Intrinsic motivations, such as an interest in exercise, predict long-term weight maintenance [32], whereas extrinsic motivations, such as appearance, have been associated with smaller weight losses [27,29,33]. Behavioral weight loss programs typically focus on increasing an individual’s level of motivation; however, there is little evidence on how the type of the initial motivation affects subsequent weight change. A better understanding of the initial motivations for considering weight loss programs is important as a lack of participant motivation is commonly used as an explanation for intervention failure or poor intervention outcomes [34]. Examining a participant’s initial reasons for weight loss could help to predict intervention outcomes.
Objectives
The primary aim of this study was to investigate the association of 3 different aspects of goal setting (weight loss motivation, overall goal preference, and percentage weight loss goal) with weight change over a 24-week period. The secondary aims were to investigate whether engagement mediated the association between goals and weight loss and to explore the association between goals and participant dropout.
Methods
Study Design and Participants
This prospective longitudinal study used data collected by Second Nature. Second Nature provides a digitally delivered behavioral program that aims to support people to increase their physical activity and create sustainable healthy eating behaviors.
Data for eligible participants were retrieved from the Second Nature database in March 2022. The researchers who conducted the analysis received a deidentified data set. All participants were adults in the United Kingdom, aged ≥18 years, and had a BMI ≥25 kg/m2 at program entry. To be eligible for inclusion in the analysis, participants must have paid to participate in the 12-week behavioral program seeking support for weight loss, recorded a baseline weight reading, and completed the bespoke health questionnaire during the enrollment process. All participants consented to the use of their anonymized data for medical research purposes by accepting the privacy policy as part of the sign-up process (Multimedia Appendix 1).
Program Description
The 12-week behavioral change program consisted of mentoring from a health coach (registered dietitian or nutritionist), peer group support, educational articles, and activity tracking technology. The program was accessed via a smartphone or a web-based app (Figure 1). Before the start of the program, each participant received an instructional handbook and recipe book and they could optionally pay extra to receive wireless weighing scales.
Figure 1.
Example Second Nature program content.
The behavioral component of the intervention has been informed by behavioral frameworks aiming to promote successful behavior change, including those outlined in the behavior change wheel [35]. A number of behavior change techniques were used within the various functions of the app and incorporated into the health coaching support, including self-monitoring (behavior and outcome), goal setting (behavior and outcome), feedback (behavior and outcome), social support (practical), and instruction on how to perform the behavior [36].
Participants were allocated a health coach who delivered personalized support via an SMS text messaging service within the app. The messaging support was provided both privately and within a group chat of up to 14 other participants to provide social accountability and motivation. Educational information, delivered through plain text and videos, could be accessed by participants through the app. The educational information covered topics focused on healthy eating, physical activity, stress management, and sleep. Participants were able to record and view their weight and step readings within the app. These could also be viewed by the health coach who encouraged participants to engage with the app and monitor their progress against their goals. The frequency of recording weight readings varied among the participants and was informed by individual choices. Health coaches were notified when participants had low engagement (defined as <10 interactions with the app in the previous week) to contact them and encourage participation.
Data Collection
At baseline, each participant answered a series of questions in a bespoke health questionnaire, including their goals for the program. Participants also self-reported their sex, height, age, presence of type 2 diabetes or prediabetes, and home postcode (which was used to calculate socioeconomic deprivation using the Index of Multiple Deprivation [IMD] [37]).
Weight data were either automatically collected using the Bluetooth weighing scales provided at the start of the program or could be manually input into the app. Having a weight reading at baseline was part of the criteria for inclusion in the analysis so the data set included complete weight data at baseline. However, for validation purposes, baseline weight readings were only retrieved from the database if they ranged between 40 kg and 200 kg. Weight data were collected at 3 further follow-up time points: 4 weeks, 12 weeks, and 24 weeks. A single weight reading was extracted for each time point by searching within a specified period (3-5 weeks for 4 weeks, 10-14 weeks for 12 weeks, and 20-28 weeks for 24 weeks) and the reading closest to the midpoint of each period was extracted. A validation algorithm, which took into account the previous reading and time since this reading was registered, was used for readings at each collection time point to only accept readings within an expected range. These validation processes were put in place to exclude anomalous readings and ensure that consistent and objective readings were extracted for analysis.
Engagement data captured participants’ interaction with the 3 main components of the smartphone app: learn, track, and support. Learn interactions were defined as the total number of articles read. Track interactions were defined as the number of times a participant viewed or had a recorded weight or steps reading. Support interactions were defined as the number of messages sent or received in either a private or group chat. Engagement was measured as the cumulative total number of interactions with these 3 components of the app at 3 time points: 0-4 weeks, 0-12 weeks, and 0-24 weeks. The exact cutoff time point for each period was defined based on the date of the extracted single weight reading.
Measures
Exposures
The following three aspects of goal setting were self-reported in the bespoke health questionnaire, which was completed as part of the enrollment process and before commencement of the program: (1) weight loss motivation—participants selected their primary reason for weight loss, categorized as appearance, health, fitness, or self-efficacy; (2) goal preference—participants selected whether they normally like to set low, medium, or high goals; and (3) percentage weight loss goal—percentage of initial body weight that participants were aiming to lose, categorized as <5%, 5%-10%, or >10%. The questionnaire was completed independently with no additional instructions.
Mediators
Total engagement, defined as the cumulative number of interactions, was considered as a mediating variable.
Outcomes
To measure sustained weight change, the primary outcome was weight at 24 weeks. The secondary outcome was dropout, defined as program cancelation up to and including each of the time points (4, 12, and 24 weeks).
Statistical Analysis
A prespecified analysis plan was published on the Open Science Framework [38]. Descriptive statistics were used to examine baseline characteristics of the study population, and 2-tailed t tests or chi-squared tests were used to compare differences in characteristics. A cross-tabulation analysis was used to explore the relationship between the different aspects of goal setting. We also explored the association between baseline characteristics and each aspect of goal setting.
Three independent mixed models for repeated measures were used to explore the association between the 3 aspects of goal setting and the dependent outcome variable, weight, over a 24-week period. A between-subjects factor of goal, a within-subjects factor of week, and the interaction between week and goal were included as fixed effects. Participant was included as a random effect to account for the repeated weight measures on the same participant at 4, 12, and 24 weeks. Further models adjusted for prespecified covariates (sex, age, IMD decile, and type 2 diabetes or prediabetes) as fixed effects. Diabetes was included as a covariate in addition to demographic characteristics as it is a weight-related condition that often affects weight loss and can also influence motivation to complete and submit weight readings in weight loss programs [39].
In a mixed effects model, missing data can be accommodated through maximum likelihood estimation, which allows for the inclusion of all available data from participants. For this analysis, a sequential testing approach was used, as follows:
Model 1—random effect: participant ID, fixed effects: goal and week
Model 2—random effect: participant ID, fixed effect: goal and week, interaction term: goal × week
Model 3—random effect: participant ID, fixed effect: goal and week, interaction term: goal × week, adjusted for sex (male or female), age (years, continuous), IMD decile (factor), and type 2 diabetes or prediabetes (yes or no)
The random effects term in the mixed effects model indirectly took into account differences in baseline weight. Model fit was compared using the R2 statistic and a P value was calculated using a likelihood ratio. The final model, adjusting for all covariates (model 3), produced the best fitting model; therefore, this is the only model presented hereafter.
A multivariable logistic regression was used to explore the association between goals and the likelihood of dropout of the program at each time point. All models were adjusted for sex, age, IMD decile, type 2 diabetes or prediabetes, and baseline weight.
Sensitivity Analyses
A sensitivity analysis was conducted by repeating the analysis of the primary outcome using completers only (ie, participants with complete data at all time points) to confirm the validity of the findings and to illustrate the pattern of weight change in the same individuals over time. As there were 8403 missing IMD values and 3054 missing goal preference values, a sensitivity analysis using the missing indicator method was also conducted.
Mediation Analysis
Mediation analysis explored whether total engagement mediated the association between goals and weight [40]. Step 1 of the mediation analysis was the primary analysis. Step 2 of the mediation analysis was a mixed effects model on the same sample, testing whether there was a significant association between goals and engagement while adjusting for all covariates. For step 3, the mixed effects model of step 1 was repeated with additional adjustment for engagement as a predictor. An engagement variable was considered as a mediator if engagement significantly predicted weight and the effect of goals was attenuated with adjustment for the engagement variable. The indirect effect and proportion of total effect mediated were calculated.
All analyses were conducted using R (version 4.1.3; R Foundation for Statistical Computing) with the Integrated Development Environment R Studio. All reported P values are for 2-sided tests, with effects considered statistically significant at P<.05.
Ethical Considerations
This study was reviewed by the University of Oxford Medical Sciences Interdivisional Research Ethics Committee (reference R84327/RE001). As the study only involved the use of previously collected, anonymized, and non–National Health Service data that cannot be traced back to identifiable individuals, it was confirmed as exempt from ethical review.
Results
Baseline Characteristics
The mean age of the total sample was 46.7 (SD 11.1) years and mean baseline BMI was 34 (SD 6.46) kg/m2, and 92.14% (33,902/36,794) of the participants were female (Table 1).
Table 1.
Baseline characteristics of total sample, participants with complete weight data (n=3193), and participants with incomplete weight data.
|
|
Total (N=36,794) | Complete data (n=3193) | Incomplete data (n=33,601) | P valuea | |||||
| Age (years), mean (SD) | 46.7 (11.1) | 48.7 (10.5) | 46.5 (11.1) | <.001 | |||||
| Sex, n (%) | .16 | ||||||||
|
|
Male | 2892 (7.86) | 272 (8.52) | 2620 (7.79) |
|
||||
|
|
Female | 33,902 (92.14) | 2921 (91.48) | 30,981 (92.2) |
|
||||
| BMI (kg/m2), mean (SD) | 34.0 (6.46) | 33.5 (6.39) | 34.1 (6.46) | <.001 | |||||
| IMDb decile, n (%) | .07 | ||||||||
|
|
1-3 | 4379 (11.9) | 357 (11.18) | 4022 (11.97) |
|
||||
|
|
4-7 | 12,091 (32.86) | 1054 (33.01) | 11,037 (32.85) |
|
||||
|
|
8-10 | 11,921 (32.39) | 1103 (34.54) | 10,818 (32.19) |
|
||||
|
|
Missing | 8403 (22.84) | 679 (21.27) | 7724 (22.99) |
|
||||
aP values were calculated using 2-tailed t tests for continuous variables or chi-squared tests for categorical variables to compare differences between participants with complete weight data and participants with incomplete weight data. Complete data were defined as having weight readings recorded at all time points (ie, at 4, 12, and 24 weeks).
bIMD: Index of Multiple Deprivation.
Most participants were motivated to lose weight for appearance reasons (14,736/36,794, 40.05%), said they preferred to set medium goals (21,963/36,794, 59.69%), and set a weight loss goal of 5%-10% of the initial body weight (23,629/36,794, 64.22%; Tables S1-S3 in Multimedia Appendix 2). More participants (641/2370, 27.05%) who said they preferred low goals set a percentage weight loss goal of <5%. There was no clear relationship between the other aspects of goal setting.
Older participants tended to be motivated by health and fitness, male participants tended to be motivated less by appearance and self-efficacy than female participants, and those who had a higher baseline BMI were motivated more by health reasons (Table S4 in Multimedia Appendix 2). Those motivated by fitness set the lowest percentage weight loss goals, and those motivated by health set the highest percentage weight loss goals. The distribution of IMD deciles was different between the motivation groups; in general, more people from higher IMD deciles selected appearance as their reason for weight loss and more people from lower IMD deciles selected fitness or self-efficacy. Participants who preferred to set higher goals were younger, a greater proportion were male, had higher baseline BMI (compared with those who preferred to set lower goals), and set higher percentage weight loss goals (Table S5 in Multimedia Appendix 2). Participants who set higher percentage weight loss goals were younger, had a greater proportion who were male, and had a higher baseline BMI (Table S6 in Multimedia Appendix 2).
Retention and Data Completeness
Among those who remained in the program, weight data were incomplete. Of the 36,794 participants in the cohort, 42% (n=15,455) had weight data available at 4 weeks, 20.73% (n=7627) at 12 weeks, and 13.09% (n=4818) at 24 weeks, whereas 8.68% (n=3193) had weight readings recorded at all time points. Examination of the participants with complete weight data at all time points, compared with participants with at least one missing weight reading, found no difference between sex or IMD decile (Table 1). Although statistically significant differences were observed for age and baseline BMI (both P<.001), these differences were not clinically meaningful.
Cumulative dropout rates of the program at 4, 12, and 24 weeks were 13.9%, 41.4%, and 62%, respectively. Figure 2 shows the dropout rates from 0 to 24 weeks. There was some dropout in the first 2 weeks of the program, followed by a steady rate of dropout week-on-week until the end of the program at 12 weeks. There was a large amount of dropout at the end of the 12-week program, and then up to 24 weeks dropout occurred on a monthly basis.
Figure 2.
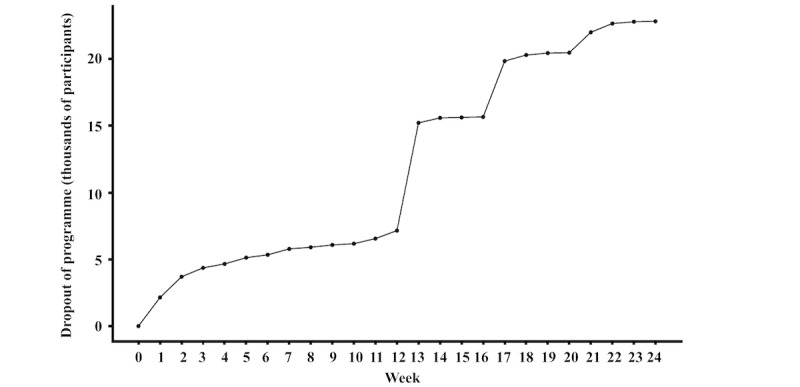
Percentage dropout of program over 24 weeks. The total number of included participants at week 0 was 36,794.
Association Between Goal Setting and Weight Change Over a 24-Week Period
In the whole cohort, the mean unadjusted weight change at 4, 12, and 24 weeks was −4.16 (SD 2.94) kg, −5.93 (SD 4.31) kg, and −6.40 (SD 5.97) kg, respectively.
At baseline, those motivated for fitness, health, and self-efficacy reasons weighed 6.1 kg, 14.8 kg, and 10.1 kg more than those motivated by appearance, respectively. At 24 weeks, compared with appearance, those motivated for health reasons lost 1.40 kg more (95% CI 1.15-1.65; P<.001), and those motivated for fitness reasons lost 0.38 kg more than appearance (95% CI 0.05-0.70; P=.03; Figure 3A and Table S7 in Multimedia Appendix 2). A sensitivity analysis using completers only also found that those motivated by health lost more weight at all time points, but there was no difference between appearance and fitness (Figure 3B and Table S7 in Multimedia Appendix 2).
Figure 3.
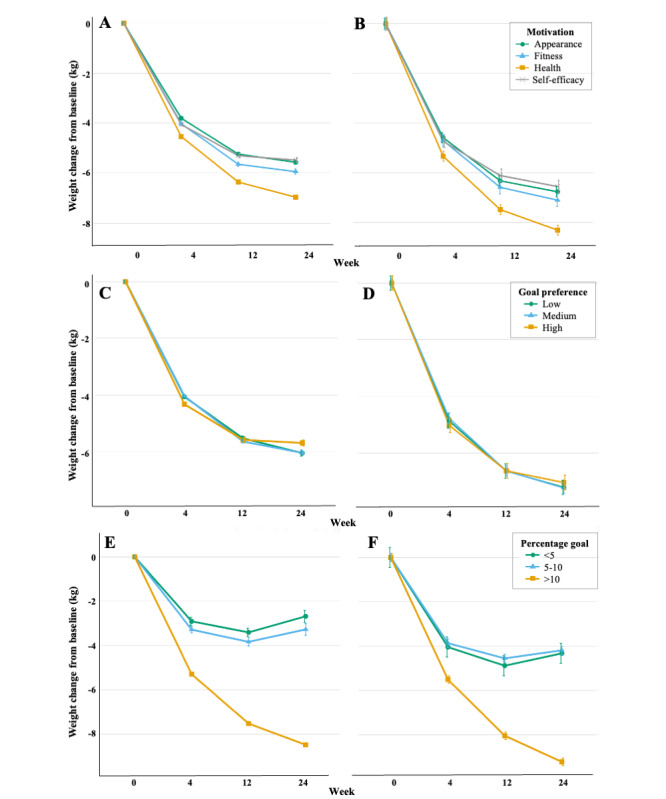
Mean adjusted weight change by (A) weight loss motivation using all available data (n=28,391), (B) weight loss motivation for completers (n=2514), (C) goal preference using all available data (n=26,158), (D) goal preference for completers (n=2194), (E) percentage weight loss goal using all available data (n=28,391), and (F) percentage weight loss goal for completers (n=2514). Weight change (kg) at 4, 12, and 24 weeks were calculated from mixed effects models, adjusted for age, sex, Index of Multiple Deprivation, and type 2 or prediabetes. Values represent mean (SE).
Those who preferred low goals weighed 3.60 kg (95% CI 2.98-4.22; P<.001) more at baseline than those who preferred medium goals. There was no difference between medium and high goals. Compared with those who preferred medium goals, high goal preference was associated with greater weight loss at 4 weeks, but lesser weight loss at 24 weeks. At 24 weeks, those who preferred high goals lost 0.34 kg less (95% CI 0.05-0.64; P=.02) than those who preferred medium goals (Figure 3C and Table S8 in Multimedia Appendix 2). A sensitivity analysis using completers only did not replicate these results and found that there was no difference between the different goal preferences at 4, 12, or 24 weeks (Figure 3D and Table S8 in Multimedia Appendix 2).
At baseline, those who set goals of <5% weighed 7.99 kg less (95% CI 7.09-8.90; P<.001) and those who set goals of >10% weighed 0.99 kg less (95% CI 0.51-1.47; P<.001), compared with goals of 5%-10%. Those who set goals of >10% lost significantly more weight at all time points compared with those who set goals of 5%-10%. At 24 weeks, those who set goals of >10% lost 5.21 kg more (95% CI 5.01-5.41; P<.001) compared with those who set goals of 5%-10% (Figure 3E and Table S9 in Multimedia Appendix 2). Furthermore, those who set goals of >10% continued to lose weight after the program ended up until 24 weeks, whereas those who set goals of <10% regained some of the weight lost after the program ended. A sensitivity analysis using completers only found a similar pattern of weight change over 24 weeks for each percentage category (Figure 3F and Table S9 in Multimedia Appendix 2).
Further sensitivity analyses using the missing indicator method (Tables S10-S12 in Multimedia Appendix 2) also showed similar results for each aspect of goal setting.
Association Between Goal Setting and Weight Change as Mediated by Engagement
Tracking was the most frequent form of engagement at every time point, but all types of engagement declined over time (Multimedia Appendix 3).
There was no evidence that engagement mediated the difference in weight loss between the motivation categories (Table S13 in Multimedia Appendix 2) or the percentage weight loss goal categories (Table S14 in Multimedia Appendix 2).
Association Between Goal Setting and Dropout of Program
There was a lower likelihood of dropout for those motivated by health compared with those motivated by appearance at all time points (Table 2). At 24 weeks, those motivated by fitness reasons were less likely to drop out compared with appearance. There was a lower likelihood of dropout for those who preferred medium goals compared with those who preferred high or low goals at 4 and 12 weeks. There was also a lower likelihood of dropout for those who preferred medium goals at 24 weeks compared with those who preferred high goals. Finally, those who set lower percentage weight loss goals were more likely to drop out at 4, 12, and 24 weeks.
Table 2.
Association between goals and likelihood of dropout of program at 4, 12, and 24 weeksa.
| Variables | Dropout at 4 weeks | Dropout at 12 weeks | Dropout at 24 weeks | ||||
|
|
ORb (95% CI) | P value | OR (95% CI) | P value | OR (95% CI) | P value | |
| Motivation (ref: appearance) | |||||||
|
|
Fitness | 0.94 (0.85-1.03) | .18 | 0.93 (0.86-1.00) | .054 | 0.92 (0.85-0.995) | .04 |
|
|
Health | 0.90 (0.83-0.98) | .01 | 0.88 (0.83-0.94) | <.001 | 0.84 (0.78-0.89) | <.001 |
|
|
Self-efficacy | 1.09 (1-1.18) | .04 | 1.04 (0.97-1.11) | .29 | 1.05 (0.98-1.14) | .17 |
| Goal preference (ref: medium) | |||||||
|
|
Low | 1.20 (1.10-1.30) | <.001 | 1.17 (1.09-1.25) | <.001 | 1.07 (1-1.16) | .06 |
|
|
High | 1.13 (1.04-1.22) | .002 | 1.17 (1.09-1.24) | <.001 | 1.20 (1.11-1.29) | <.001 |
| Percentage weight loss goal (ref: 5%-10%) | |||||||
|
|
<5% | 2.71 (2.45-3.01) | <.001 | 1.60 (1.44-1.77) | <.001 | 1.32 (1.17-1.5) | <.001 |
|
|
>10% | 0.40 (0.37-0.44) | <.001 | 0.46 (0.44-0.49) | <.001 | 0.40 (0.38-0.42) | <.001 |
aModels were adjusted for sex, age, Index of Multiple Deprivation decile, type 2 diabetes, or prediabetes.
bOR: odds ratio.
Discussion
Principal Findings
The program led to clinically meaningful weight loss of 6.40 kg (equivalent to 6.8%) at 24 weeks among the participants who continued to weigh themselves. Differences in demographic characteristics or goal setting were small. Health and fitness motivations were associated with greater weight losses and lower likelihood of dropout compared with appearance at 24 weeks. Setting weight loss goals of >10% was associated with an average 5.21 kg greater weight loss than setting the more common 5%-10% goal, and an average 60% lower odds of dropout at 24 weeks. There was no clear association between goal preference and weight loss.
Comparison With Prior Work
In other studies on weight loss motivating factors, the primary factor was to improve health, whereas appearance had a low prevalence [12,29]. These differences could be because of the recruitment strategy and resultant selection bias; patients recruited from medical centers in a research setting may be more likely to give health as their reason for weight loss, compared with this analysis of data in a community setting where participants were self-funding program attendance. However, consistent with previous research, we found that health motivation was associated with greater weight loss than appearance [29,33]. This could be explained by self-determination theory and goal contents [41]. Goal contents are distinguished by the extent to which they fulfill basic psychological needs. Intrinsic goals (eg, to improve health) are more closely related to the fulfillment of psychological needs, whereas extrinsic goals (eg, to improve appearance) are not essential to well-being and personal development. Research has shown that extrinsic goals provide motivation in the short term, whereas intrinsic goals are more beneficial for long-term results [42]. Although health or fitness motivators cannot be easily categorized as intrinsic or extrinsic, the results of this study suggest that the underlying motivational reason may be more important than increasing overall motivation. Weight loss motivation may differ according to demographic characteristics and may explain previously observed differences in outcomes [30,43].
The finding that participants who set larger weight loss goals lost more weight at 24 weeks challenges current UK clinical guidelines that encourage a weight loss goal of 5%-10% [7]. In fact, this study supports previous findings demonstrating that setting a higher weight loss goal is associated with greater weight loss at 12 months than lesser weight loss goals [23], and a systematic review that reports goal difficulty as one of the main factors that makes goal setting effective [44]. This study also found that participants who set goals of >10% continued to lose weight after the program ended, whereas those who set goals of <10% regained some weight for up to 24 weeks. For some people, setting a larger weight loss goal may be more motivating, and it has been suggested that higher goals are more self-relevant and provide a sense of direction and purpose [45]. Higher goals have also been associated with greater effort in the weight loss attempt [21], as predicted by goal setting theory, which suggests that goals have an energizing function, causing greater effort directed toward more challenging goals [2]. These findings suggest that recommendations on setting realistic weight loss goals should be reconsidered.
Goal preference had no clear association with weight loss. As the primary outcome was weight, we were only able to consider participants who submitted weight readings. It is possible that those who stopped weighing themselves or dropped out were unsuccessful in their weight loss attempts. This temporal sequence of events has been shown previously, whereby users tend to gain weight and reduce their weight loss efforts before ceasing weight tracking [46]. Thus, the lack of association with goal preference could be driven by differences in attrition, as those who liked to set high goals were 1.2 times more likely to drop out by 24 weeks (P<.001). The association between higher weight loss expectations and greater attrition has also been shown previously [18]. It is possible that when goals are perceived as too ambitious, individuals experience impaired performance, which discourages a person’s belief in their ability to control their weight, leading to abandonment of weight management behaviors [14,15,47]. Alternatively, the bespoke health questionnaire, completed as part of the enrollment process, may not have accurately measured goal preference, particularly as this is a subjective measure, as shown by a lack of correlation between the goal preference and percentage weight loss goal variables.
Overall, the mediation analysis found that participants who engaged more with program components tended to lose more weight, as reported previously [48-50], but this was independent of the type of goal set. Therefore, engagement can be considered an independent predictor of weight loss but not a mediator of the association between goals and weight. Maintaining engagement and retaining participants over time are key to the success of digital weight loss interventions. The modification of goal setting via pretreatment recommendations may be a means to maintain engagement, which is worth further exploration.
Strengths and Limitations
To date, no study in a community setting has explored the association between goals and weight loss on this scale in detail, with 3 different aspects of goal setting reported. The use of this data set allows for greater confidence than other studies in terms of the robustness and generalizability of the findings. The strengths of this study include the large sample size, the preregistration of the analysis plan, and prospective design. Although the population sample was predominantly female, this is broadly representative of enrollment in most private weight management services [51,52].
The limitations of this study largely reflect the challenges associated with analyses of a population in an uncontrolled, community setting. The observational nature means that causal relationships cannot be determined, and randomized controlled trials are required to confirm these results. There was a large proportion of missing weight readings as participants were not actively encouraged to weigh themselves or engage with the program after the initial program ended at 12 weeks. Many participants canceled their subscription after completing the main 12-week program, as shown in Figure 2, which is reflected in the availability of weight data at 24 weeks. Similar proportions of missing weight data have been reported previously for self-funded participants enrolled in the same program [39]. We aimed to mitigate the issue of missing weight readings by using mixed models for repeated measures, allowing use of all available data with weight readings assumed missing at random. The sensitivity analyses did not lead to different conclusions. However, participants who continue to register weight readings are likely to be more motivated, and to have lost weight, resulting in self-selection bias. Although the exposure groups did not significantly differ by demographic characteristics, we cannot rule out the possibility that they may have differed by other factors that were not measured here, such as ethnicity. Further research is needed to extrapolate these findings to more demographically diverse populations, particularly male participants and those from more socioeconomically deprived backgrounds. The sample only included participants who were paying to participate in the program, meaning that this population was likely to be more self-motivated to lose weight. Payment for participation may have influenced participants’ commitment, engagement, and their initial motivation for starting the program. As such, the generalizability of these findings to nonpaying populations remains unknown.
Implications and Further Research
Current guidelines recommend weight loss of 5%-10%, but encouraging individuals to set larger goals may lead to improved weight loss outcomes and better retention in weight loss programs. Future randomized controlled trials testing the effect of pretreatment counseling to set larger weight loss goals on program success are warranted. Investigating whether there is an upper limit for the association between higher weight loss goals and achieved weight losses would also be relevant for future research.
Although further research cannot realistically change participants’ primary motivation for weight loss, 2 randomized controlled trials have shown that weight loss interventions tailored to specific types of weight loss motivation achieve greater weight loss compared with controls [53,54]. Motivating factors for weight loss may be used to predict who is most likely to be successful and who may need more support, particularly as a lack of participant motivation is commonly used to explain poor intervention outcomes [34]. Without more complete weight data, it was not possible to establish the long-term outcomes of all the participants in this cohort. Further research is needed to determine ways to maintain engagement, as retaining participants over time is likely critical for the optimal effectiveness of digital weight loss programs.
Conclusions
Setting larger weight loss goals and being motivated for health or fitness reasons were associated with greater weight loss and a lower likelihood of dropout. Randomized trials testing the effects of setting these types of goals are required to confirm causality.
Acknowledgments
The authors would like to thank Second Nature for providing the data for this study. The authors would also like to thank Richard Stevens and Paul Bateman for their guidance on statistical analysis and interpretation. This work, and GMW’s time on this project, is funded by the Medical Research Council (MRC; grant MR/R015708/1). DAK, JS, and SAJ were funded by the National Institute for Health Research (NIHR) Oxford Biomedical Research Centre (grant IS-BRC-1215–20008). The views expressed are those of the authors and not necessarily those of the MRC or the NIHR. As this study used previously collected, fully anonymized data, it was exempt from ethics approval.
Abbreviations
- IMD
Index of Multiple Deprivation
- OR
odds ratio
Second Nature privacy policy.
Cross-tabulation analyses, baseline characteristics by goal aspect, full results of mixed effects models, and mediation analyses by engagement.
Mean engagement with program components.
Data Availability
The participants of this study did not provide written consent for their data to be shared publicly; thus, supporting data are not available.
Footnotes
Authors' Contributions: GMW performed the analysis, interpreted the data, and wrote the manuscript. MW performed data extraction and cleaning. DAK, JS, and SAJ supervised the overall design and activities of the analysis and supervised the drafting and editing of the manuscript. All authors were involved in the conceptualization and design of the study. All authors have read, edited, and approved the final manuscript before publication.
Conflicts of Interest: MW is an employee of Second Nature. Second Nature is the industrial partner on GMW’s Medical Research Council Industrial Collaborative Awards in Science and Engineering studentship. DAK and SAJ report being investigators in 2 investigator-led publicly funded (National Institute for Health Research) trials where the weight loss intervention was donated by Nestle Health Science and Oviva to the University of Oxford outside the submitted work. SAJ and JS report being investigators in a trial where Second Nature is delivering the weight loss intervention. JS was involved with a Nestle Health Sciences advisory board and was an invited speaker at a Nestle Health Sciences webinar, for which a personal honorarium was received. None of these associations led to payments to these authors personally.
References
- 1.Siegert RJ, Levack WMM, editors. Rehabilitation Goal Setting: Theory, Practice and Evidence. Boca Raton: Taylor & Francis Group; 2015. [Google Scholar]
- 2.Locke EA, Latham GP. Building a practically useful theory of goal setting and task motivation. A 35-year odyssey. Am Psychol. 2002 Sep;57(9):705–17. doi: 10.1037//0003-066x.57.9.705. [DOI] [PubMed] [Google Scholar]
- 3.Locke EA, Latham GP. A Theory of Goal Setting & Task Performance. Hoboken, NJ, USA: Prentice-Hall Inc; 1991. Apr, [Google Scholar]
- 4.Barrett KV, Savage PD, Ades PA. Effects of behavioral weight loss and weight loss goal setting in cardiac rehabilitation. J Cardiopulm Rehabil Prev. 2020 Nov;40(6):383–7. doi: 10.1097/HCR.0000000000000510. https://europepmc.org/abstract/MED/32694455 .01273116-202011000-00007 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Jeffery RW, Wing RR, Sherwood NE, Tate DF. Physical activity and weight loss: does prescribing higher physical activity goals improve outcome? Am J Clin Nutr. 2003 Oct;78(4):684–9. doi: 10.1093/ajcn/78.4.684. [DOI] [PubMed] [Google Scholar]
- 6.Michie S, Abraham C, Whittington C, McAteer J, Gupta S. Effective techniques in healthy eating and physical activity interventions: a meta-regression. Health Psychol. 2009 Nov;28(6):690–701. doi: 10.1037/a0016136.2009-20990-006 [DOI] [PubMed] [Google Scholar]
- 7.Centre for Public Health Excellence at NICE. National Collaborating Centre for Primary Care Obesity: the prevention, identification, assessment and management of overweight and obesity in adults and children. NICE Clinical Guidelines. 2006. Dec, [2022-08-01]. https://www.ncbi.nlm.nih.gov/books/NBK63696/ [PubMed]
- 8.Jensen MD, Ryan DH, Apovian CM, Ard JD, Comuzzie AG, Donato KA, Hu FB, Hubbard VS, Jakicic JM, Kushner RF, Loria CM, Millen BE, Nonas CA, Pi-Sunyer FX, Stevens J, Stevens VJ, Wadden TA, Wolfe BM, Yanovski SZ, Jordan HS, Kendall KA, Lux LJ, Mentor-Marcel R, Morgan LC, Trisolini MG, Wnek J, Anderson JL, Halperin JL, Albert NM, Bozkurt B, Brindis RG, Curtis LH, DeMets D, Hochman JS, Kovacs RJ, Ohman EM, Pressler SJ, Sellke FW, Shen WK, Smith Jr SC, Tomaselli GF, American College of Cardiology/American Heart Association Task Force on Practice Guidelines. Obesity Society 2013 AHA/ACC/TOS guideline for the management of overweight and obesity in adults: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines and The Obesity Society. Circulation. 2014 Jun 24;129(25 Suppl 2):S102–38. doi: 10.1161/01.cir.0000437739.71477.ee. https://www.ahajournals.org/doi/abs/10.1161/01.cir.0000437739.71477.ee?url_ver=Z39.88-2003&rfr_id=ori:rid:crossref.org&rfr_dat=cr_pub0pubmed .01.cir.0000437739.71477.ee [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Lavie CJ, McAuley PA, Church TS, Milani RV, Blair SN. Obesity and cardiovascular diseases: implications regarding fitness, fatness, and severity in the obesity paradox. J Am Coll Cardiol. 2014 Apr 15;63(14):1345–54. doi: 10.1016/j.jacc.2014.01.022. https://linkinghub.elsevier.com/retrieve/pii/S0735-1097(14)00334-9 .S0735-1097(14)00334-9 [DOI] [PubMed] [Google Scholar]
- 10.Fabricatore AN, Wadden TA, Womble LG, Sarwer DB, Berkowitz RI, Foster GD, Brock JR. The role of patients' expectations and goals in the behavioral and pharmacological treatment of obesity. Int J Obes (Lond) 2007 Nov;31(11):1739–45. doi: 10.1038/sj.ijo.0803649.0803649 [DOI] [PubMed] [Google Scholar]
- 11.Linde JA, Jeffery RW, Finch EA, Ng DM, Rothman AJ. Are unrealistic weight loss goals associated with outcomes for overweight women? Obes Res. 2004 Mar;12(3):569–76. doi: 10.1038/oby.2004.65. https://onlinelibrary.wiley.com/doi/10.1038/oby.2004.65 . [DOI] [PubMed] [Google Scholar]
- 12.Dalle Grave R, Calugi S, Magri F, Cuzzolaro M, Dall'aglio E, Lucchin L, Melchionda N, Marchesini G, QUOVADIS Study Group Weight loss expectations in obese patients seeking treatment at medical centers. Obes Res. 2004 Dec;12(12):2005–12. doi: 10.1038/oby.2004.251. https://onlinelibrary.wiley.com/doi/10.1038/oby.2004.251 .12/12/2005 [DOI] [PubMed] [Google Scholar]
- 13.Pétré B, Scheen A, Ziegler O, Donneau AF, Dardenne N, Husson E, Albert A, Guillaume M. Weight loss expectations and determinants in a large community-based sample. Prev Med Rep. 2018 Aug 04;12:12–9. doi: 10.1016/j.pmedr.2018.08.005. https://linkinghub.elsevier.com/retrieve/pii/S2211-3355(18)30132-3 .S2211-3355(18)30132-3 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Cervone D, Jiwani N, Wood R. Goal setting and the differential influence of self-regulatory processes on complex decision-making performance. J Pers Soc Psychol. 1991 Aug;61(2):257–66. doi: 10.1037//0022-3514.61.2.257. [DOI] [PubMed] [Google Scholar]
- 15.Klinger E. Consequences of commitment to and disengagement from incentives. Psychol Rev. 1975 Jan;82(1):1–25. doi: 10.1037/h0076171. https://psycnet.apa.org/doiLanding?doi=10.1037%2Fh0076171 . [DOI] [Google Scholar]
- 16.Marston AR, Criss J. Maintenance of successful weight loss: incidence and prediction. Int J Obes. 1984;8(5):435–9. [PubMed] [Google Scholar]
- 17.Klem ML, Wing RR, McGuire MT, Seagle HM, Hill JO. A descriptive study of individuals successful at long-term maintenance of substantial weight loss. Am J Clin Nutr. 1997 Aug;66(2):239–46. doi: 10.1093/ajcn/66.2.239. [DOI] [PubMed] [Google Scholar]
- 18.Dalle Grave R, Calugi S, Molinari E, Petroni ML, Bondi M, Compare A, Marchesini G, QUOVADIS Study Group Weight loss expectations in obese patients and treatment attrition: an observational multicenter study. Obes Res. 2005 Nov;13(11):1961–9. doi: 10.1038/oby.2005.241. https://onlinelibrary.wiley.com/doi/10.1038/oby.2005.241 .13/11/1961 [DOI] [PubMed] [Google Scholar]
- 19.Dalle Grave R, Calugi S, Compare A, El Ghoch M, Petroni ML, Tomasi F, Mazzali G, Marchesini G. Weight loss expectations and attrition in treatment-seeking obese women. Obes Facts. 2015;8(5):311–8. doi: 10.1159/000441366. doi: 10.1159/000441366.000441366 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Wadden TA, Womble LG, Sarwer DB, Berkowitz RI, Clark VL, Foster GD. Great expectations: "I'm losing 25% of my weight no matter what you say". J Consult Clin Psychol. 2003 Dec;71(6):1084–9. doi: 10.1037/0022-006X.71.6.1084.2003-09784-014 [DOI] [PubMed] [Google Scholar]
- 21.De Vet E, Nelissen RM, Zeelenberg M, De Ridder DT. Ain't no mountain high enough? Setting high weight loss goals predict effort and short-term weight loss. J Health Psychol. 2013 May;18(5):638–47. doi: 10.1177/1359105312454038.1359105312454038 [DOI] [PubMed] [Google Scholar]
- 22.Lent MR, Vander Veur SS, Peters JC, Herring SJ, Wyatt HR, Tewksbury C, Wojtanowski AC, Hill JO, Foster GD. Initial weight loss goals: have they changed and do they matter? Obes Sci Pract. 2016 Jun;2(2):154–61. doi: 10.1002/osp4.45. https://europepmc.org/abstract/MED/27840688 .OSP445 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Avery A, Langley-Evans SC, Harrington M, Swift JA. Setting targets leads to greater long-term weight losses and 'unrealistic' targets increase the effect in a large community-based commercial weight management group. J Hum Nutr Diet. 2016 Dec;29(6):687–96. doi: 10.1111/jhn.12390. https://europepmc.org/abstract/MED/27302147 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Foster GD, Wadden TA, Vogt RA, Brewer G. What is a reasonable weight loss? Patients' expectations and evaluations of obesity treatment outcomes. J Consult Clin Psychol. 1997 Feb;65(1):79–85. doi: 10.1037//0022-006x.65.1.79. [DOI] [PubMed] [Google Scholar]
- 25.Teixeira PJ, Going SB, Houtkooper LB, Cussler EC, Martin CJ, Metcalfe LL, Finkenthal NR, Blew RM, Sardinha LB, Lohman TG. Weight loss readiness in middle-aged women: psychosocial predictors of success for behavioral weight reduction. J Behav Med. 2002 Dec;25(6):499–523. doi: 10.1023/a:1020687832448. [DOI] [PubMed] [Google Scholar]
- 26.Kincey J. Target setting, self-reinforcement pattern and locus of control orientation as predictors of outcome in a behavioural weight-loss programme. Behav Res Ther. 1980;18(2):139–45. doi: 10.1016/0005-7967(80)90108-4.0005-7967(80)90108-4 [DOI] [PubMed] [Google Scholar]
- 27.Teixeira PJ, Carraça EV, Markland D, Silva MN, Ryan RM. Exercise, physical activity, and self-determination theory: a systematic review. Int J Behav Nutr Phys Act. 2012 Jun 22;9:78. doi: 10.1186/1479-5868-9-78. https://ijbnpa.biomedcentral.com/articles/10.1186/1479-5868-9-78 .1479-5868-9-78 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Teixeira PJ, Palmeira AL, Branco TL, Martins SS, Minderico CS, Barata JT, Silva AM, Sardinha LB. Who will lose weight? A reexamination of predictors of weight loss in women. Int J Behav Nutr Phys Act. 2004 Aug 02;1(1):12. doi: 10.1186/1479-5868-1-12. https://ijbnpa.biomedcentral.com/articles/10.1186/1479-5868-1-12 .1479-5868-1-12 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Mroz JE, Pullen CH, Hageman PA. Health and appearance reasons for weight loss as predictors of long-term weight change. Health Psychol Open. 2018 Dec 05;5(2):2055102918816606. doi: 10.1177/2055102918816606. https://journals.sagepub.com/doi/10.1177/2055102918816606?url_ver=Z39.88-2003&rfr_id=ori:rid:crossref.org&rfr_dat=cr_pub0pubmed .10.1177_2055102918816606 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.LaRose JG, Leahey TM, Hill JO, Wing RR. Differences in motivations and weight loss behaviors in young adults and older adults in the national weight control registry. Obesity (Silver Spring) 2013 Mar;21(3):449–53. doi: 10.1002/oby.20053. https://europepmc.org/abstract/MED/23404944 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Kwan S. Competing motivational discourses for weight loss: means to ends and the nexus of beauty and health. Qual Health Res. 2009 Sep;19(9):1223–33. doi: 10.1177/1049732309343952.19/9/1223 [DOI] [PubMed] [Google Scholar]
- 32.Santos I, Mata J, Silva MN, Sardinha LB, Teixeira PJ. Predicting long-term weight loss maintenance in previously overweight women: a signal detection approach. Obesity (Silver Spring) 2015 May;23(5):957–64. doi: 10.1002/oby.21082. https://onlinelibrary.wiley.com/doi/10.1002/oby.21082 . [DOI] [PubMed] [Google Scholar]
- 33.Vartanian LR, Wharton CM, Green EB. Appearance vs. health motives for exercise and for weight loss. Psychol Sport Exerc. 2012 May;13(3):251–6. doi: 10.1016/j.psychsport.2011.12.005. https://www.sciencedirect.com/science/article/abs/pii/S1469029211001750 . [DOI] [Google Scholar]
- 34.Meyer AH, Weissen-Schelling S, Munsch S, Margraf J. Initial development and reliability of a motivation for weight loss scale. Obes Facts. 2010 Jun;3(3):205–11. doi: 10.1159/000315048. doi: 10.1159/000315048.000315048 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Michie S, van Stralen MM, West R. The behaviour change wheel: a new method for characterising and designing behaviour change interventions. Implement Sci. 2011 Apr 23;6:42. doi: 10.1186/1748-5908-6-42. https://implementationscience.biomedcentral.com/articles/10.1186/1748-5908-6-42 .1748-5908-6-42 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Michie S, Richardson M, Johnston M, Abraham C, Francis J, Hardeman W, Eccles MP, Cane J, Wood CE. The behavior change technique taxonomy (v1) of 93 hierarchically clustered techniques: building an international consensus for the reporting of behavior change interventions. Ann Behav Med. 2013 Aug;46(1):81–95. doi: 10.1007/s12160-013-9486-6. [DOI] [PubMed] [Google Scholar]
- 37.The English indicies of deprivation 2019. Government DfCaL. [2022-02-01]. https://www.gov.uk/government/statistics/english-indices-of-deprivation-2019 .
- 38.Wren G, Koutoukidis D, Scragg J, Whitman M, Jebb S. The association between goal setting and weight loss outcomes: study protocol 2022. OSF. 2022. [2022-08-01]. https://osf.io/whtcs/ [DOI] [PMC free article] [PubMed]
- 39.Idris I, Hampton J, Moncrieff F, Whitman M. Effectiveness of a digital lifestyle change program in obese and type 2 diabetes populations: service evaluation of real-world data. JMIR Diabetes. 2020 Jan 20;5(1):e15189. doi: 10.2196/15189. https://diabetes.jmir.org/2020/1/e15189/ v5i1e15189 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Baron RM, Kenny DA. The moderator-mediator variable distinction in social psychological research: conceptual, strategic, and statistical considerations. J Pers Soc Psychol. 1986 Dec;51(6):1173–82. doi: 10.1037//0022-3514.51.6.1173. [DOI] [PubMed] [Google Scholar]
- 41.Deci EL, Ryan RM. The "what" and "why" of goal pursuits: human needs and the self-determination of behavior. Psychol Inq. 2000 Oct;11(4):227–68. doi: 10.1207/s15327965pli1104_01. https://www.tandfonline.com/doi/abs/10.1207/S15327965PLI1104_01 . [DOI] [Google Scholar]
- 42.Teixeira PJ, Silva MN, Mata J, Palmeira AL, Markland D. Motivation, self-determination, and long-term weight control. Int J Behav Nutr Phys Act. 2012 Mar 02;9:22. doi: 10.1186/1479-5868-9-22. https://ijbnpa.biomedcentral.com/articles/10.1186/1479-5868-9-22 .1479-5868-9-22 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Crane MM, Jeffery RW, Sherwood NE. Exploring gender differences in a randomized trial of weight loss maintenance. Am J Mens Health. 2017 Mar;11(2):369–75. doi: 10.1177/1557988316681221. https://journals.sagepub.com/doi/10.1177/1557988316681221?url_ver=Z39.88-2003&rfr_id=ori:rid:crossref.org&rfr_dat=cr_pub0pubmed .1557988316681221 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Epton T, Currie S, Armitage CJ. Unique effects of setting goals on behavior change: Systematic review and meta-analysis. J Consult Clin Psychol. 2017 Dec;85(12):1182–98. doi: 10.1037/ccp0000260.2017-53491-007 [DOI] [PubMed] [Google Scholar]
- 45.Houser-Marko L, Sheldon KM. Eyes on the prize or nose to the grindstone? The effects of level of goal evaluation on mood and motivation. Pers Soc Psychol Bull. 2008 Nov;34(11):1556–69. doi: 10.1177/0146167208322618.0146167208322618 [DOI] [PubMed] [Google Scholar]
- 46.Frie K, Hartmann-Boyce J, Jebb S, Oke J, Aveyard P. Patterns in weight and physical activity tracking data preceding a stop in weight monitoring: observational analysis. J Med Internet Res. 2020 Mar 17;22(3):e15790. doi: 10.2196/15790. https://www.jmir.org/2020/3/e15790/ v22i3e15790 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47.Cooper Z, Fairburn CG. A new cognitive behavioural approach to the treatment of obesity. Behav Res Ther. 2001 May;39(5):499–511. doi: 10.1016/s0005-7967(00)00065-6.S0005-7967(00)00065-6 [DOI] [PubMed] [Google Scholar]
- 48.Kar P, Goward C, Whitman M, Davies M, Willner T, Shaw K. Engagement and effectiveness of digitally enabled behavioural change support for people living with type 2 diabetes. Pract Diab. 2020 Oct 07;37(5):167–72. doi: 10.1002/pdi.2295. https://wchh.onlinelibrary.wiley.com/doi/pdf/10.1002/pdi.2295 . [DOI] [Google Scholar]
- 49.Carey A, Yang Q, DeLuca L, Toro-Ramos T, Kim Y, Michaelides A. The relationship between weight loss outcomes and engagement in a mobile behavioral change intervention: retrospective analysis. JMIR Mhealth Uhealth. 2021 Nov 08;9(11):e30622. doi: 10.2196/30622. https://mhealth.jmir.org/2021/11/e30622/ v9i11e30622 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 50.Toro-Ramos T, Michaelides A, Anton M, Karim Z, Kang-Oh L, Argyrou C, Loukaidou E, Charitou MM, Sze W, Miller JD. Mobile delivery of the diabetes prevention program in people with prediabetes: randomized controlled trial. JMIR Mhealth Uhealth. 2020 Jul 08;8(7):e17842. doi: 10.2196/17842. https://mhealth.jmir.org/2020/7/e17842/ v8i7e17842 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 51.Krukowski RA, Harvey-Berino J, Ashikaga T, Thomas CS, Micco N. Internet-based weight control: the relationship between web features and weight loss. Telemed J E Health. 2008 Oct;14(8):775–82. doi: 10.1089/tmj.2007.0132. https://europepmc.org/abstract/MED/18954247 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 52.Kim Y, Oh B, Shin HY. Effect of mHealth with offline antiobesity treatment in a community-based weight management program: cross-sectional study. JMIR Mhealth Uhealth. 2020 Jan 21;8(1):e13273. doi: 10.2196/13273. https://mhealth.jmir.org/2020/1/e13273/ v8i1e13273 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 53.Kalarchian MA, Levine MD, Klem ML, Burke LE, Soulakova JN, Marcus MD. Impact of addressing reasons for weight loss on behavioral weight-control outcome. Am J Prev Med. 2011 Jan;40(1):18–24. doi: 10.1016/j.amepre.2010.09.019. https://europepmc.org/abstract/MED/21146763 .S0749-3797(10)00535-0 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 54.West DS, Gorin AA, Subak LL, Foster G, Bragg C, Hecht J, Schembri M, Wing RR, Program to Reduce Incontinence by Diet and Exercise (PRIDE) Research Group A motivation-focused weight loss maintenance program is an effective alternative to a skill-based approach. Int J Obes (Lond) 2011 Feb;35(2):259–69. doi: 10.1038/ijo.2010.138. https://europepmc.org/abstract/MED/20680012 .ijo2010138 [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Second Nature privacy policy.
Cross-tabulation analyses, baseline characteristics by goal aspect, full results of mixed effects models, and mediation analyses by engagement.
Mean engagement with program components.
Data Availability Statement
The participants of this study did not provide written consent for their data to be shared publicly; thus, supporting data are not available.