

ABSTRACT
Objective.
To examine the homicide trends among young people (10–24 years), adolescents (10–19 years), and young adults (20–24 years) in 33 countries in the Americas between 2000 and 2019, with a focus on inequalities between countries in the burden of homicides.
Methods.
An ecological study was performed using estimated deaths from 33 countries. Age-adjusted rates, percentage change (PC), average annual percentage change (AAPC), and relative risk (RR) were estimated; besides, analysis on social inequalities was performed.
Results.
In the Americas between 2000 and 2019, homicide has been the leading cause of death with 54 515 deaths on average each year and an age-adjusted rate of 23.6 per 100 000 among young people. The highest rate was found in the Andean subregion (41.1 per 100 000 young people), which also produced the highest decrease (PC = –37.1% and AAPC = –2.4%) in the study period. The risk of homicide in young men is 8.1 times the risk in young women, and the risk in young adults is 2.5 times the risk in adolescents. The three countries with highest risk of homicide for young people are Venezuela (relative risk [RR] = 35.1), El Salvador (RR = 28.1), and Colombia (RR = 26.7). The estimated excess mortality was 26.8 homicides per 100 000 in the poorest 20% of countries compared to the richest 20% of countries in the period 2000–2009, and it decreased to 13.9 in the period 2010–2019.
Conclusions.
The results of this study add to the knowledge of homicide among young people and can be used to inform policy and programming in countries. Given the great burden of homicide on young people in the region, it is critical that prevention opportunities are maximized, beginning early in life.
Keywords: Homicide, mortality registries, socioeconomic factors, social determinants of health, Americas
RESUMEN
Objetivo.
Examinar las tendencias de los homicidios entre la población joven (10-24 años), los adolescentes (10-19 años) y los adultos jóvenes (20-24 años) en 33 países de las Américas entre el 2000 y el 2019, con particular atención a las desigualdades entre los países en materia de cifras de homicidios.
Métodos.
Se realizó un estudio ecológico utilizando las muertes estimadas de 33 países. Se estimaron las tasas ajustadas en función de la edad, el cambio porcentual (CP), el cambio porcentual anual promedio (CPAP) y el riesgo relativo (RR). Además, se realizó un análisis sobre las desigualdades sociales.
Resultados.
Entre el 2000 y el 2019, el homicidio ha sido la principal causa de muerte en las Américas, con un promedio anual de 54 515 muertes y una tasa ajustada en función de la edad de 23,6 por cada 100 000 habitantes en la población joven. La tasa más alta se observó en la subregión andina (41,1 por cada 100 000 habitantes para la población joven), en la cual también se observó la mayor disminución (CP = -37,1% y CPAP = -2,4%) en el período de estudio. El riesgo de homicidio entre los hombres jóvenes es 8,1 veces mayor que entre las mujeres jóvenes, y el riesgo entre los adultos jóvenes es 2,5 veces mayor que el riesgo en adolescentes. Los tres países con mayor riesgo de homicidio para los jóvenes son Venezuela (riesgo relativo [RR] = 35,1), El Salvador (RR = 28,1) y Colombia (RR = 26,7). El exceso de mortalidad estimado fue de 26,8 homicidios por cada 100 000 habitantes en el 20% de los países más pobres, en comparación con el 20% de los países más ricos, durante el período 2000-2009, y disminuyó a 13,9 durante el período 2010-2019.
Conclusiones.
Los resultados de este estudio se suman a los conocimientos sobre el homicidio entre la población joven, y pueden utilizarse para fundamentar las políticas y los programas de los países. Dada la enorme carga de homicidios que sufre la población joven de la región, es fundamental impulsar al máximo las oportunidades de prevención desde las primeras etapas de la vida.
Palabras clave: Homicidio, registros de mortalidad, factores socioeconómicos, determinantes sociales de la salud, Américas
RESUMO
Objetivo.
Examinar as tendências de homicídios entre pessoas jovens (10 a 24 anos), adolescentes (10 a 19 anos) e adultas jovens (20 a 24 anos) em 33 países das Américas entre 2000 e 2019, com foco em desigualdades da carga de homicídios entre países.
Métodos.
Foi realizado um estudo ecológico usando estimativas de óbitos de 33 países. Foram estimadas taxas ajustadas por idade, variação percentual (VP), variação percentual anual média (VPAM) e risco relativo (RR); além disso, foi realizada uma análise das desigualdades sociais.
Resultados.
Entre 2000 e 2019, o homicídio foi a principal causa de morte nas Américas, com uma média de 54.515 óbitos por ano e uma taxa ajustada por idade de 23,6 por 100 mil pessoas entre pessoas jovens. A taxa mais alta foi encontrada na sub-região andina (41,1 por 100 mil jovens), que também registrou a redução mais acentuada (VP = -37,1% e VPAM = -2,4%) no período do estudo. O risco de homicídio entre homens jovens é 8,1 vezes maior que o risco em mulheres jovens, e o risco entre pessoas adultas jovens é 2,5 vezes maior que o risco em adolescentes. Os três países com maior risco de homicídio entre pessoas jovens são Venezuela (RR = 35,1), El Salvador (RR = 28,1) e Colômbia (RR = 26,7). Nos países, o excesso de mortalidade estimado foi de 26,8 homicídios por 100 mil habitantes nos 20% mais pobres comparados aos 20% mais ricos no período de 2000 a 2009. Esse número diminuiu para 13,9 no período de 2010 a 2019.
Conclusões.
Os resultados deste estudo se somam às informações sobre homicídios entre jovens e podem ser usados para embasar políticas e programas nacionais. Dado o grande ônus que os homicídios representam para as pessoas jovens da região, é fundamental que as oportunidades de prevenção sejam maximizadas desde cedo em suas vidas.
Palavras-chave: Homicídio, registros de mortalidade, fatores socioeconômicos, determinantes sociais da saúde, América
Over a decade into the 21st century, the adolescent and youth population* became the largest cohort of young people in the history of the Americas, representing on average 25% of the total population between 2000 and 2019 (1). These young people face a myriad of obstacles that are closely linked with poverty, social marginalization, and discrimination.
Adolescent and youth mortality is shaped by the physical, social, cultural, environmental, and economic factors that young people face throughout their lives (2). In 2018, 48.5% of youth in rural areas in 18 Latin American and Caribbean (LAC) countries live in poverty, and 21.1% in extreme poverty (3). Data show that unemployment among youth is three times higher than the adult rates, and 55.7% of the employed fit in the International Labour Organization (ILO) definition of vulnerable employment.** Furthermore, according to the United Nations Development Programme (UNDP), one-third of the youth living in poverty neither work nor study (4). In Latin America and the Caribbean, the net enrollment rate for primary school in 2018 was 94%, while for secondary school it was 78% (5). In addition, there has been a large movement of young people from rural to urban areas; current estimates indicate that almost 70% of 10–24-year-olds live within metropolitan zones. Data from United Nations Human Settlements Programme (UN-Habitat) show that in 2016, 20.4% of the urban population lived in slums; for 2018 the percentage was 20.8% (6).
In 2019, the regional homicide rate for all ages was 19.2 per 100 000, more than three times the global homicide rate for all ages at 6.2 per 100 000 inhabitants (7). In comparison to other age groups, young people are disproportionately more likely to be affected by homicides, whether as a perpetrator or a victim (8, 9). The Americas has the highest homicide rate for those under 18 years of age in the world (5.8 per 100 000 in 2017, compared to the global average of 1.7 per 100 000). Homicide rates in the Americas are especially high among boys (9.3 per 100 000 for boys under 18, compared to 2.1 for girls), although the girl homicide rate in the Americas is still almost double the rate for girls globally and higher than the rates for girls in all World Health Organization (WHO) Regions, and for boys in all but the African Region (10, 11). Similarly, homicide was the leading cause of death among males aged 10–19 years (25.7%) and 15–24 years (57.3%); while it was the second leading cause of death among females aged 10–19 years (4.2%) and 15–24 years (7.0%) in 2009–2014 (12).
There is no single explanation for the high rates of homicides in the Region as a whole and in specific settings. Rather, a range of social factors at the individual, relational, community, and societal level intersect and may result in increased risk (13). For example, at the individual level, the consumption of alcohol and psychoactive substances is associated with homicides. Other studies have found that lower educational attainment is associated with homicide. A study conducted in Mexico in 2013 (14) found that low educational attainment among young people increased their likelihood of becoming a victim of homicide in comparison to their more educated peers. The homicide rate among males 18 to 40 years of age was 300 per 100 000 people. In contrast, men who had a university degree had a homicide rate of 26 per 100 000 population (14). At the relationship level, use of violence by peers, gang membership, and gang violence are associated with homicide. Within the Americas, homicides due to gangs and organized crime are particularly high in Central America, the Caribbean, and certain South American countries like Brazil. Although there is little empirical evidence on gangs, particularly youth gangs, it is estimated that in Central America, the Caribbean, and South America combined there are as many as 500 000 gang members (15). It is important to note that the relationship between homicides and organized crime is not necessarily linear, with spikes of homicides sometimes occurring due to changes in the power of gangs rather than due to their presence (16). Others have pointed to homicides being more likely to occur in urban areas, in comparison to rural areas, due to higher income inequality, anonymity, and organized criminal activities and gangs (9). It was suggested that homicides are related with the institutional (in)capacity to integrate disadvantaged areas, as well as meet the needs and labor requirements of the population. When urban settings are unable to meet employment needs, this can result in economic deprivation and frustration among males, increasing their likelihood to engage in violence (9, 17). At the societal level, gender and social inequality, weak rule of law, and trafficking of persons, weapons, and drugs, to name only a few, pose additional challenges to homicide prevention. Homicides not only influence individuals and families but also place a heavy burden on health, social, and criminal justice systems. For each young person killed, many more sustain injuries and require treatment. Homicide impacts the local and national economies as it translates into a loss of human capital, workforce absenteeism, and a loss of productivity (17). Estimates from the Americas suggest that homicides cost between 2% and 9% of countries’ gross domestic product (GDP) across the region (18). According to the World Bank, if homicides were reduced by 10% in Central America, the annual GDP per capita would increase by 1% in El Salvador, 0.7% in Guatemala and Honduras, and 0.3% in Panama and Nicaragua (18).
The general objective of this study is to provide an in-depth analysis of the trends in mortality due to homicide among young people (10–24 years), adolescents (10–19 years), and young adults (20–24 years) in the countries of the Americas between 2000 and 2019, as well as the social inequalities between countries in the burden of homicides in these age groups.
MATERIALS AND METHODS
To investigate mortality among young people, adolescents, and young adults in selected countries of the Americas, an ecological study was performed using estimated deaths from 2000 to 2019 by WHO (19); these estimates only have available mortality data before COVID-19. The final data set includes 33 countries in the Region that were analyzed. Subregional analyses were also conducted and included country groupings according to commonly used Pan American Health Organization (PAHO) subregions: Andean (Bolivia [Plurinational State of], Colombia, Ecuador, Peru, and Venezuela [Bolivarian Republic of]), Latin Caribbean (Cuba, Dominican Republic, and Haiti), Mesoamerica (Belize, Costa Rica, El Salvador, Guatemala, Honduras, Mexico, Nicaragua, and Panama), Non-Latin Caribbean (Antigua and Barbuda, Bahamas, Barbados, Grenada, Guyana, Jamaica, Saint Lucia, Saint Vincent and the Grenadines, Suriname, and Trinidad and Tobago ), North America (Canada and United States of America); and the Southern Cone (Argentina, Brazil, Chile, Paraguay, and Uruguay).
The variables considered in the study were: age group (10–24, 10–19, 20–24 years), sex (male, female, and total [both sexes]), subregion (6 subregions), and period (2000–2009, 2010–2019) for studying social inequalities.
A descriptive exploratory data analysis was carried out by computing age-adjusted homicide mortality rates (age-adjusted HMR) for all countries, subregions, and the Region of the Americas overall. For between-country and subregion comparisons, age-adjusted HMR were computed using the standard population, as set by the WHO world population age-structure for the period 2000–2025 (20). Trends analysis on age-adjusted HMR were conducted in the Region, subregions, and selected countries. For the study of the homicide mortality trend, the percentage change (PC) and average annual percentage change (AAPC) were estimated. The PC is estimated as:
PC = 100*[HMR(T1) – HMR(T0)] / HMR(T0)] %,
where HMR(T0) and HMR(T1) are the values of the age-adjusted HMR at times T0 and T1, respectively. To estimate the AAPC, a linear regression model was fitted:
Ln(HMR) = α + β*T, T = 2000, …, 2019,
where Ln is the natural logarithm function, from which the AAPC can be computed:
AAPC = 100*[exp(β) – 1] %,
where exp() is the exponential function and β is the estimate of the slope parameter in the model. In addition, the “join point” regression model was used to estimate the AAPC (access to the software used in this analysis is available [21]). To compute the burden of homicide, relative risks (RR) were estimated by fitting a negative binomial regression model (point estimates and 95% confidence intervals [CI]). To examine the social inequality in homicide, the GDP per capita was considered as equity stratifier; data for this indicator were compiled from the World Bank Group between 2000 and 2019 (22). Two health inequality summary measures were considered, the absolute gap (AG) and relative gap (RG) (23). The AG and RG correspond to the difference and division, respectively, between weighted average homicide mortality rate in the 20% of countries with the lowest and the 20% of countries with the highest GDP per capita. The analyses were performed using the Statistical Analysis System (SAS) v.9.4 software.
RESULTS
In the last 20 years, between 2000 and 2019, homicide has been the first leading cause of death among young people aged 10–24 years in the Americas, and it was estimated that each year, on average, 54 515 young people die from this cause. Of the 3 793 568 total deaths among young people from the 33 countries between 2000 and 2019, homicide accounted for 1 090 302 deaths (28.7% of all deaths); the number of homicides in males and females were 975 487 and 114 815, respectively. For adolescents (10–19 years) and young adults (20–24 years), the number of homicides was 467 258 (25.4% of all adolescent deaths) and 623 044 (32.0% of all young adult deaths), respectively, for the same period.
In the Americas, the age-adjusted HMR among young people was 23.6 per 100 000 (95% CI [21.5, 25.9]) in the period 2000–2019. When disaggregated by age, rates were 15.0 per 100 000 (95% CI [13.5, 16.7]) and 41.2 per 100 000 (95% CI [37.9, 44.9]) among adolescents and young adults, respectively. In the study period, the rate among young people in North America was 7.5 per 100 000 young people (95% CI [7.2, 7.8]), Mesoamerica was 20.6 (95% CI [18.1, 23.5]), Latin Caribbean was 18.9 (95% CI [8.5, 29.5]), Andean was 41.1 (95% CI [36.7, 46.1]), Southern Cone was 33.7 (95% CI [32.2, 35.2]), Non-Latin Caribbean was 21.1 (95% CI [17.4, 25.2]), and the Americas was 23.6 (95% CI [21.5, 25.9]); the highest estimated country rate in each subregion, respectively, was 8.1 per 100 000 young people (95% CI [7.8, 8.3]) in United States of America, 62.2 (95% CI [52.7, 71.5]) in El Salvador, 28.7 (95% CI [7.2, 49.4]) in Haiti, 76.3 (95% CI [68.3, 85.0]) in Venezuela, 42.2 (95% CI [40.7, 43.7]) in Brazil, and 36.1 (95% CI [30.3, 42.6]) in Trinidad and Tobago, respectively. In addition, Canada, Costa Rica, Cuba, Peru, Chile, and Grenada had the lowest mortality rates in each subregion, respectively. Overall, by country, there is wide variability in homicide mortality rates (Table 1). In all countries and subregions, the rates among young people, adolescents, and young adults were higher among men than women (Table 1).
TABLE 1. Homicide mortality rates per 100 000 population and average annual percentage change (in parentheses) for young people (10–24 years), adolescents (10–19 years), and young adults (20–24 years) by sex in the subregions and countries of the Americas in the period 2000–2019.
|
|
|
Young people 10–24 years |
Adolescents 10–19 years |
Young adults 20–24 years |
||||||
|---|---|---|---|---|---|---|---|---|---|---|
|
Subregion/region |
Country |
Total |
Male |
Female |
Total |
Male |
Female |
Total |
Male |
Female |
|
The Americas |
All countries |
23.6 (–0.2%) |
41.8 (–0.2%) |
5.1 (–0.8%) |
15.0 (0.1%) |
25.7 (0.2%) |
3.9 (–0.8%) |
41.2 (–0.6%) |
74.4 (–0.5%) |
7.4 (–0.4%) |
|
Andean |
Bolivia (Plurinational State of) |
10.9 (0.7%) |
17.4 (0.7%) |
4.2 (0.1%) |
7.0 (1.7%) |
10.7 (1.7%) |
3.2 (1.5%) |
19.0 (0.0%) |
31.3 (–0.1%) |
6.2 (0.5%) |
|
Colombia |
57.1 (–5.1%) |
101.6 (–5.3%) |
11.6 (–4.1%) |
35.2 (–4.2%) |
60.8 (–4.3%) |
8.8 (–4.0%) |
101.5 (–5.7%) |
184.5 (–6.0%) |
17.2 (–4.1%) |
|
|
Ecuador |
15.3 (–8.2%) |
27.2 (–8.8%) |
3.1 (–4.1%) |
7.9 (–7.2%) |
13.3 (–7.6%) |
2.2 (–5.2%) |
30.6 (–8.9%) |
55.5 (–9.6%) |
4.9 (–3.0%) |
|
|
Peru |
8.2 (0.0%) |
13.0 (–0.2%) |
3.3 (1.0%) |
5.6 (0.8%) |
8.3 (0.7%) |
2.8 (1.5%) |
13.6 (–0.6%) |
22.6 (–0.7%) |
4.3 (0.4%) |
|
|
Venezuela (Bolivarian Republic of) |
76.3 (1.7%) |
142.2 (1.8%) |
8.8 (0.1%) |
46.1 (2.2%) |
83.4 (2.4%) |
7.5 (0.0%) |
139.2 (1.3%) |
264.7 (1.4%) |
11.4 (0.4%) |
|
|
Total |
41.1 (–2.4%) |
73.9 (–2.4) |
7.4 (–2.1%) |
25.0 (–1.9%) |
43.6 (–1.5%) |
5.9 (–1.3%) |
74.2 (–2.9%) |
136.4 (–2.9%) |
10.7 (–2.3%) |
|
|
Latin Caribbean |
Cuba |
4.3 (–1.8%) |
6.3 (–2.1%) |
2.2 (–1.3%) |
2.4 (–1.2%) |
3.5 (–1.5%) |
1.3 (–0.4%) |
8.1 (–2.2%) |
12.0 (–2.3%) |
4.0 (–2.0%) |
|
Dominican Republic |
19.5 (–0.4%) |
32.2 (–0.1%) |
6.6 (–2.3%) |
11.4 (–1.9%) |
18.0 (–1.5%) |
4.7 (–3.9%) |
36.4 (0.6%) |
61.8 (0.8%) |
10.7 (–0.6%) |
|
|
Haiti |
28.7 (–0.2%) |
47.8 (–0.4%) |
9.8 (0.8%) |
17.2 (–0.7%) |
27.3 (–0.9%) |
6.9 (–0.1%) |
52.9 (0.1%) |
90.5 (–0.2%) |
15.9 (1.6%) |
|
|
Total |
18.9 (0.3%) |
31.0 (0.1%) |
6.7 (0.6%) |
11.3 (–0.3%) |
17.8 (–0.5%) |
4.7 (–0.7%) |
34.3 (0.8%) |
57.6 (0.5%) |
10.8 (1.1%) |
|
|
Mesoamerica |
Belize |
32.1 (2.1%) |
54.3 (2.2%) |
10.0 (2.0%) |
19.0 (1.5%) |
30.9 (1.6%) |
6.9 (1.4%) |
59.7 (2.5%) |
103.3 (2.5%) |
16.4 (2.5%) |
|
Costa Rica |
9.4 (4.3%) |
15.8 (4.9%) |
2.7 (1.2%) |
5.0 (3.6%) |
7.9 (4.0%) |
2.0 (2.3%) |
18.6 (4.8%) |
32.6 (5.4%) |
4.0 (1.1%) |
|
|
El Salvador |
62.2 (0.1%) |
106.9 (0.2%) |
19.7 (–1.5%) |
36.0 (1.1%) |
58.0 (1.6%) |
14.0 (–1.9%) |
116.5 (–0.6%) |
207.9 (–0.6%) |
31.6 (–1.2%) |
|
|
Guatemala |
36.9 (–2.2%) |
64.1 (–2.4%) |
9.7 (–1.3%) |
22.4 (–2.1%) |
36.8 (–2.4%) |
7.6 (–1.3%) |
66.9 (–2.2%) |
120.0 (–2.5%) |
14.0 (–1.3%) |
|
|
Honduras |
49.6 (–0.9%) |
65.7 (–0.7%) |
33.1 (–1.4%) |
33.3 (0.6%) |
40.8 (1.0%) |
25.6 (0.0%) |
82.9 (–2.3%) |
116.8 (–2.0%) |
48.3 (–3.0%) |
|
|
Mexico |
14.0 (5.6%) |
24.5 (5.5%) |
3.7 (5.4%) |
7.8 (4.2%) |
12.9 (4.1%) |
2.7 (4.2%) |
27.2 (6.5%) |
49.2 (6.3%) |
5.7 (6.6%) |
|
|
Nicaragua |
12.4 (–2.0%) |
21.1 (–1.9%) |
3.4 (–3.0%) |
9.2 (–2.9%) |
15.5 (–3.0%) |
2.6 (–2.9%) |
19.0 (–1.1%) |
32.8 (–0.9%) |
4.9 (–3.1%) |
|
|
Panama |
23.4 (3.2%) |
41.2 (3.5%) |
5.0 (1.1%) |
14.9 (3.8%) |
25.4 (4.1%) |
4.1 (2.4%) |
41.0 (2.8%) |
74.0 (3.1%) |
6.9 (–0.6%) |
|
|
Total |
20.6 (2.2%) |
34.6 (2.3%) |
6.7 (1.4%) |
12.3 (1.6%) |
19.3 (1.7%) |
5.1 (1.2%) |
37.6 (2.6%) |
65.8 (2.7%) |
9.9 (1.8%) |
|
|
Non-Latin Caribbean |
Antigua and Barbuda |
3.6 (–6.7%) |
6.0 (–7.3%) |
1.3 (–4.3%) |
2.9 (–5.3%) |
4.9 (–7.0%) |
0.9 (1.3%) |
5.0 (–6.9%) |
8.2 (–5.9%) |
2.0 (–11.6%) |
|
Bahamas |
21.5 (2.8%) |
37.9 (2.4%) |
5.1 (5.2%) |
13.0 (3.0%) |
22.3 (2.6%) |
3.8 (4.9%) |
39.1 (2.6%) |
70.6 (2.3%) |
7.8 (5.4%) |
|
|
Barbados |
10.8 (–1.5%) |
17.3 (–1.2%) |
4.3 (–3.2%) |
7.0 (–1.3%) |
11.6 (–0.7%) |
2.2 (–5.5%) |
18.9 (–1.7%) |
29.0 (–1.7%) |
8.9 (–2.0%) |
|
|
Grenada |
3.3 (1.3%) |
4.9 (1.8%) |
1.6 (–0.7%) |
2.0 (1.7%) |
2.7 (1.3%) |
1.3 (2.4%) |
5.9 (0.7%) |
9.5 (1.6%) |
2.3 (–4.0%) |
|
|
Guyana |
16.4 (–0.1%) |
26.5 (–0.7%) |
6.2 (2.3%) |
7.1 (0.5%) |
10.1 (–1.0%) |
4.1 (5.3%) |
35.3 (–0.2%) |
60.2 (–0.4%) |
10.3 (–0.9%) |
|
|
Jamaica |
20.8 (–2.5%) |
29.1 (–2.4%) |
12.3 (–2.7%) |
14.0 (–3.2%) |
19.1 (–2.8%) |
8.7 (–4.0%) |
34.8 (–1.9%) |
49.6 (–2.0%) |
19.7 (–1.4%) |
|
|
Saint Lucia |
18.7 (–2.1%) |
30.5 (–3.0%) |
7.1 (1.2%) |
11.1 (1.3%) |
16.7 (–0.7%) |
5.7 (6.9%) |
33.4 (–4.6%) |
57.7 (–4.4%) |
9.5 (–6.6%) |
|
|
Saint Vincent and the Grenadines |
17.6 (3.4%) |
27.9 (3.3%) |
7.2 (3.5%) |
7.4 (0.4%) |
9.6 (–2.5%) |
5.0 (6.6%) |
39.1 (4.5%) |
66.0 (5.1%) |
11.6 (0.6%) |
|
|
Suriname |
7.9 (–6.5%) |
12.1 (–6.6%) |
3.4 (–6.4%) |
4.4 (–2.6%) |
6.4 (–3.1%) |
2.4 (–1.1%) |
14.8 (–9.4%) |
23.7 (–8.9%) |
5.6 (–12.9%) |
|
|
Trinidad and Tobago |
36.1 (6.3%) |
64.6 (6.7%) |
6.9 (2.8%) |
19.9 (6.9%) |
34.2 (7.4%) |
5.3 (3.8%) |
70.5 (6.0%) |
129.6 (6.4%) |
10.3 (1.9%) |
|
|
Total |
21.1 (0.5%) |
33.3 (0.7%) |
8.6 (–0.1%) |
12.5 (0.1%) |
18.7 (0.2%) |
6.1 (–0.2%) |
39.4 (1.1%) |
64.7 (1.2%) |
13.6 (0.1%) |
|
|
North America |
Canada |
2.0 (–1.6%) |
3.3 (–2.1%) |
0.8 (0.7%) |
1.3 (–1.7%) |
1.9 (–2.5%) |
0.6 (1.0%) |
3.6 (–1.5%) |
6.0 (–1.9%) |
1.1 (0.4%) |
|
United States of America |
8.1 (–1.7%) |
13.5 (–1.6%) |
2.4 (–2.2%) |
4.9 (–1.1%) |
8.1 (–0.9%) |
1.6 (–1.8%) |
14.5 (–2.1%) |
24.6 (–2.0%) |
4.1 (–2.5%) |
|
|
Total |
7.5 (–1.5%) |
12.5 (–1.4%) |
2.2 (–2.0%) |
4.6 (–0.8%) |
7.5 (–0.9%) |
1.5 (–1.7%) |
13.5 (–1.9%) |
22.8 (–1.8%) |
3.8 (–2.5%) |
|
|
Southern Cone |
Argentina |
7.7 (–0.6%) |
13.4 (–0.6%) |
1.9 (–1.0%) |
5.1 (–0.5%) |
8.6 (–0.5%) |
1.5 (–1.2%) |
13.0 (–0.7%) |
23.2 (–0.8%) |
2.6 (–0.8%) |
|
Brazil |
42.2 (1.0%) |
77.1 (1.0%) |
6.4 (0.4%) |
28.5 (1.8%) |
51.0 (1.9%) |
5.2 (0.4%) |
70.7 (0.3%) |
131.2 (0.3%) |
9.0 (0.4%) |
|
|
Chile |
5.5 (–2.2%) |
9.9 (–2.4%) |
0.9 (0.2%) |
3.4 (–1.2%) |
6.0 (–1.5%) |
0.7 (0.8%) |
9.7 (–2.9%) |
17.8 (–3.1%) |
1.4 (–0.4%) |
|
|
Paraguay |
15.3 (–6.2%) |
26.5 (–6.1%) |
3.6 (–6.4%) |
8.5 (–7.1%) |
14.8 (–7.2%) |
2.0 (–6.6%) |
29.0 (–5.6%) |
50.2 (–5.5%) |
6.8 (–6.3%) |
|
|
Uruguay |
8.1 (2.9%) |
13.6 (3.2%) |
2.4 (1.3%) |
5.5 (3.1%) |
8.9 (3.4%) |
1.9 (1.6%) |
13.5 (2.8%) |
23.5 (3.0%) |
3.3 (1.1%) |
|
|
Total |
33.7 (0.9%) |
61.4 (0.9%) |
5.3 (0.0%) |
22.6 (1.2%) |
40.4 (1.3%) |
4.2 (0.1%) |
56.8 (0.3%) |
105.2 (0.2%) |
7.5 (–0.1%) |
|
Source: Prepared by the authors, based on Global Health Estimates 2020 (19).
Homicide mortality trends
Among all 33 countries of the Americas, overall regional homicide rate trended slightly downward from 24.3 per 100 000 young people (95% CI [22.7, 26.1]) in 2000 to 23.2 (95% CI [19.5, 27.7]) in 2019, representing a PC = –4.4% reduction with an AAPC = –0.2% (95% CI [–1.5, 1.1]) between 2000 and 2019.
Although the highest homicide rate among young people was found in the Andean and Southern Cone subregions, the highest decrease between 2000 and 2019 was presented in the Andean subregion with a PC = –37.1% and an AAPC = –2.4% (95% CI [–3.4, –1.4]), and in North America with a PC = –22.3% and an AAPC = –1.5% (95% CI [–3.2, 0.2]). On the other hand, the highest increase was found in the Mesoamerica subregion with a PC = 47.1% and an AAPC = 2.2% (95% CI [0.9, 3.6]).
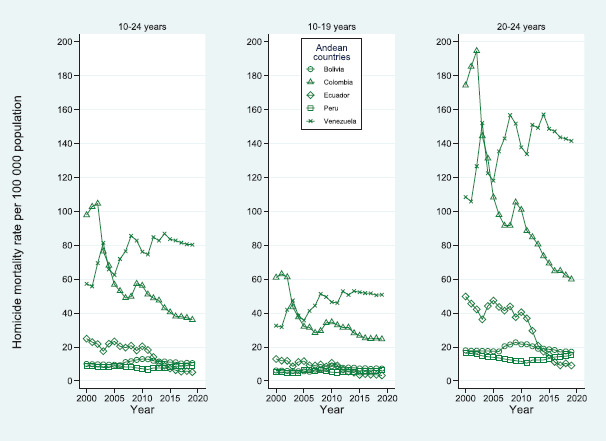
For all countries and subregions, the AAPC was computed by sex and age (Table 1); besides, for all subregions, trends in age-adjusted HMR among young people are shown in Figure 1. Between 2000 and 2019, the five countries with highest annual decrease in age-adjusted HMR among young people were: Ecuador (AAPC = –8.2%), Antigua and Barbuda (AAPC = –6.7%), Suriname (AAPC = –6.5%), Paraguay (AAPC = –6.1%), and Colombia (AAPC = –5.1%); on the other hand, the five countries with the highest annual increase were: Trinidad and Tobago (AAPC = 6.3%), Mexico (AAPC = 5.6%), Costa Rica (AAPC = 4.3%), Saint Vincent and the Grenadines (AAPC = 3.4%), and Panama (AAPC = 3.2%). Figure 2 shows the trends of age-adjusted HMR among young people, adolescents, and young adults for countries of the Andean subregion between 2000 and 2019. Over the study period, Colombia and Ecuador presented a decrease in the age-adjusted HMR of 97.8 per 100 000 young people (95% CI [94.3, 101.4]) in 2000 to 36.1 (95% CI [27.5, 47.3]) in 2019, and 24.9 (95% CI [20.1, 29.9]) in 2000 to 5.1 (95% CI [3.1, 8.1]) in 2019, respectively; Venezuela presented an increase in the age-adjusted HMR of 57.2 (95% CI [53.8, 60.8]) in 2000 to 80.3 (95% CI [59.4, 104.9]) in 2019.
FIGURE 1. Age-adjusted homicide mortality rate per 100 000 young people (both sexes) by subregion of the Americas, 2000–2019.

Source: Prepared by the authors, based on Global Health Estimates 2020 (19).
FIGURE 2. Trends on age-adjusted homicide mortality rate per 100 000 people (both sexes) of all countries within the Andean subregion by age group (10–24, 10–19, 20–24 years), 2000–2019.
Source: Prepared by the authors, based on Global Health Estimates 2020 (19).
Relative risk of homicide mortality
Among young people, the risk of homicide in men is 8.1 (95% CI [7.8, 8.5]) times the risk in women; see Table 2. This RR increases to 10 times (95% CI [9.7, 10.4]) within the young adults. The risk of homicide in young adults was 2.5 (95% CI [2.4, 2.6]) times the risk in adolescents. Compared to North America subregion, the relative burden of dying in the Andean subregion due to homicide among young people was 4.9 (95% CI [4.5, 5.4]) times greater, 3.8 times greater in the Southern Cone, 3.7 times greater in Non-Latin Caribbean, 3.2 times greater in Mesoamerica, and 2.8 times greater in the Latin Caribbean. On the other hand, countries with higher risk of homicide among young people, compared to Canada, were Venezuela (RR = 35.1), El Salvador (RR = 28.1), Colombia (RR = 26.7), Honduras (RR = 22.4), Brazil (RR = 20.2), Trinidad and Tobago (RR = 18.5), Guatemala (RR = 16.4), Belize (RR = 14.5), Haiti (RR = 13.0), and Panama (RR = 10.7) (Table 2).
TABLE 2. Estimate of the relative risk (RR) and 95% confidence interval of the variables sex (female as reference), age group (adolescent as reference), subregion (North America as reference), and country (Canada as reference).
|
Variables |
|
RR |
95% confidence interval |
|
|---|---|---|---|---|
|
Sex |
Male |
8.1 |
7.8 |
8.5 |
|
Female |
-- |
-- |
-- |
|
|
Age group |
Young adults |
2.5 |
2.4 |
2.6 |
|
Adolescent |
-- |
-- |
-- |
|
|
Subregion |
Andean |
4.9 |
4.5 |
5.4 |
|
Southern Cone |
3.8 |
3.5 |
4.2 |
|
|
Non-Latin Caribbean |
3.7 |
3.3 |
4.0 |
|
|
Mesoamerica |
3.2 |
2.9 |
3.5 |
|
|
Latin Caribbean |
2.8 |
2.5 |
3.1 |
|
|
North America |
-- |
-- |
-- |
|
|
Country |
Venezuela (Bolivarian Republic of) |
35.1 |
30.5 |
40.2 |
|
El Salvador |
28.1 |
24.5 |
32.3 |
|
|
Colombia |
26.7 |
23.3 |
30.7 |
|
|
Honduras |
22.4 |
19.5 |
25.8 |
|
|
Brazil |
20.2 |
17.6 |
23.2 |
|
|
Trinidad and Tobago |
18.5 |
16.0 |
21.4 |
|
|
Guatemala |
16.4 |
14.3 |
18.9 |
|
|
Belize |
14.5 |
12.4 |
17.0 |
|
|
Haiti |
13.0 |
11.4 |
15.0 |
|
|
Panama |
10.7 |
9.3 |
12.3 |
|
|
Bahamas |
9.9 |
8.3 |
11.7 |
|
|
Jamaica |
9.6 |
8.4 |
11.1 |
|
|
Dominican Republic |
9.0 |
7.8 |
10.3 |
|
|
Saint Lucia |
8.7 |
7.1 |
10.7 |
|
|
Saint Vincent and the Grenadines |
8.2 |
6.5 |
10.4 |
|
|
Guyana |
7.1 |
6.1 |
8.3 |
|
|
Ecuador |
7.1 |
6.2 |
8.1 |
|
|
Paraguay |
7.0 |
6.1 |
8.1 |
|
|
Mexico |
6.5 |
5.6 |
7.4 |
|
|
Nicaragua |
5.7 |
5.0 |
6.6 |
|
|
Barbados |
5.1 |
4.1 |
6.4 |
|
|
Bolivia (Plurinational State of) |
4.9 |
4.3 |
5.6 |
|
|
Costa Rica |
4.5 |
3.9 |
5.2 |
|
|
Uruguay |
3.8 |
3.3 |
4.5 |
|
|
United States of America |
3.8 |
3.3 |
4.4 |
|
|
Peru |
3.8 |
3.3 |
4.4 |
|
|
Argentina |
3.6 |
3.1 |
4.1 |
|
|
Suriname |
3.6 |
3.0 |
4.4 |
|
|
Chile |
2.6 |
2.3 |
3.0 |
|
|
Cuba |
2.0 |
1.8 |
2.4 |
|
|
Antigua and Barbuda |
1.7 |
1.0 |
2.8 |
|
|
Grenada |
1.5 |
1.0 |
2.5 |
|
|
Canada |
-- |
-- |
-- |
|
Source: Prepared by the authors, based on Global Health Estimates 2020 (19).
Social inequality in homicide mortality
The AG and RG inequalities in homicide among young people were increasing between 2000 and 2009 and then they tended to decrease from 2010 to 2019; similar results were found for homicide among adolescents and young adults (these results are not presented). The median of the AGs and RGs were computed for the periods 2000–2009 and 2010–2019 by sex and age group (Table 3). There was an estimated excess mortality equivalent to 26.8 homicides per 100 000 young people in the poorest 20% of countries in the Americas compared to the richest 20% of countries in the period 2000–2009, and this AG decreased to 13.9 deaths per 100 000 young people in the period 2010–2019. In relative terms, the risk of homicide among young people in the poorest 20% of countries in the Americas is four times the risk of homicide in the richest 20% of countries in the period 2000–2009; this risk decreased to two times in the period 2010–2019 (Table 3). The greatest AG inequality in homicide occurred in young adult males (20–24 years), with estimated values of AG = 80.9 per 100 000 young adults in the period 2000–2009 and AG = 35.7 in the period 2010–2019. Very concerning, the greatest RG inequality in homicide occurred in adolescent females (10–19 years), with RG = 5.9 in the period 2000–2009 and RG = 3.9 in the period 2010–2019. In general, the highest absolute inequalities occurred in men and the highest relative inequalities in women, regardless of age group (Table 3).
TABLE 3. Estimates of the absolute gap (AG) and relative gap (RG) inequalities by sex and age group (10–24, 10–19, and 20–24 years) and sex (total, male, and female) in the periods 2000–2009 and 2010–2019.
|
|
|
Young people 10–24 years |
Adolescents 10–19 years |
Young adults 20–24 years |
|||
|---|---|---|---|---|---|---|---|
|
Sex |
Period |
AG |
RG |
AG |
RG |
AG |
RG |
|
Total |
2000–2009 |
26.8 |
4.2 |
16.3 |
4.2 |
48.2 |
4.2 |
|
2010–2019 |
13.9 |
2.1 |
9.3 |
2.4 |
24.6 |
1.9 |
|
|
Male |
2000–2009 |
43.4 |
4.1 |
24.4 |
3.9 |
80.9 |
4.1 |
|
2010–2019 |
19.2 |
1.9 |
12 |
2.1 |
35.7 |
1.8 |
|
|
Female |
2000–2009 |
10.7 |
5.4 |
7.9 |
5.9 |
16.4 |
5.0 |
|
2010–2019 |
9.9 |
3.6 |
7.8 |
3.9 |
13.9 |
3.5 |
|
AG, absolute gap; RG, relative gap.
Source: Prepared by the authors, based on Global Health Estimates 2020 (19).
DISCUSSION
This study contributes to the limited body of information on mortality among young people, adolescents, and young adults in the Americas by presenting the trends and magnitude of homicides in 33 countries, and identifying social inequalities, and contributing to the knowledge on mortality in these groups. Given the paucity of data on the subject, this study provides an important starting point on which further studies can be based.
The study found that mortality varied across countries. The five countries with higher risk of homicide among young people, compared to Canada, were Venezuela, El Salvador, Colombia, Honduras, and Brazil. Based on the inequality analysis, it was found that low national income levels tended to have higher homicide mortality rates, which may explain the high rates in Venezuela and El Salvador. Other considerations for higher mortality rates may result from limited criminal justice system enforcement, a lack of policies and programs that target violence prevention, and a lack of mental health policies and programs (10, 17). The decrease in homicide rates in the Andean and North America subregions may be attributed to factors such as the implementation of gun control policies, increased policing efforts, and socioeconomic development. In contrast, the increase in homicide rates in the Mesoamerica subregion may be attributed to factors such as gang violence, drug trafficking, and political instability. For example, Venezuela has been experiencing political and economic instability in recent years, El Salvador has a long history of gang violence, and Colombia has experienced decades of armed conflict, which has resulted in high levels of violence and displacement. The glorification of violence in media and entertainment, as well as the normalization of gang culture, including the prevalence of weapons in a neighborhood, may contribute to an environment in which violence is seen as an acceptable means of conflict resolution (24). The implementation of restrictive gun ownership laws has been demonstrated to reduce firearm-related crime and mortality rates (25, 26). In addition, the severity of penalties for violations of restrictive gun ownership laws may also contribute to reductions in homicide (25, 26). Nevertheless, research in these countries is needed to determine why mortality among young people is high and what is being done in other countries with lower mortality rates.
The study found that mortality was higher among young adults compared to adolescents. In accordance with previous literature, homicide mortality increases with age from adolescence to young adults, spiking often in early adulthood. This may be attributed to cognitive development, developmental changes, the impact that critical and sensitive periods have across the life course, and their conceptualization of death. Therefore, prevention efforts should begin early in life to reduce young adult homicide rates (27, 28).
Homicide rates were found to be higher among young men than women, which underlines the need for further gender-sensitive analysis of data (2–4). Although the study did not address this issue, women and girls in the Americas are more likely to experience non-fatal interpersonal violence. Femicide, including intimate partner homicide, are significant challenges in the Region, which this study could not examine (29–31). Moreover, it is important to note that female homicide rates, though lower than male homicide rates, are double the global rate, pointing to a significant challenge in the Region that requires attention in the future.
In addition to gender inequalities, further research into social inequalities related to cultural factors contributing to the burden of homicides in subgroups such as Indigenous and Afro-descendant young people can inform the development of culturally appropriate and context-specific approaches (32). The nature of the data used in this study precluded the possibility of examining mortality rates at the national level by ethnic groups and thus highlights the need for further analysis of disaggregated mortality data. Further research on the social and cultural factors affecting specific groups of adolescents and young adults and their relation to homicide mortality should also be conducted, allowing for the development of culturally appropriate mortality prevention policies. Given that the Americas is one of the regions with the highest economic and social inequalities in the world (33), which have been further exacerbated by the COVID-19 pandemic (34), it is important to build national institutional capabilities to measure and monitor social inequalities related to homicide and interpersonal violence more broadly. The evidence generated from such analysis will enable decisionmakers to formulate equity-oriented public policies, thereby strengthening accountability to the commitment in the 2030 Agenda for Sustainable Development to “leave no one behind.”
Lastly, the study pointed to some additional topics for further research on the connections between homicide and other important health issues. For instance, future research should examine the association between homicide and mental health in adolescents and young people, given that previous studies have shown mental health impacts of violence on young people and opportunities for prevention (35, 36).
Limitations of the study include that homicides may be underreported due to various reasons, including misclassification of homicide deaths. To examine potential misclassification of homicide, some studies have analyzed the association among mortality rates, autopsy rates, and death rates of undetermined and ill-defined causes, respectively (37). To address this limitation, the quality of data in countries must be assessed by checking the completeness and consistency of the information. In the data used in this study, validation processes were performed considering some selected variables: sex, age, and underlying cause of death (38). On the other hand, this study considered the computation of absolute and relative inequality measures, and a limitation is that these may not reflect specific gaps between individuals within countries; this due to the ecological fallacy, as the use of ecological study designs was considered to measure equity gaps between national levels within the Americas. Besides, the GDP per capita level considered in this work is an average value per country and does not reflect the actual income level of people. In addition, the analysis covered the 20 years before the COVID-19 pandemic, and the pandemic may have caused important changes in the number of homicides as well as in inequality within the countries.
In conclusion, this study has aimed to bridge the data gap regarding trends in homicides in young people in 33 countries in the Americas, and the social inequalities associated with the burden of homicides in these countries, in order to increase understanding and inform adolescent and young adult health policy and programming. Homicides are extremely costly to societies in the Region, but these costs can be prevented (35). To guide action and maximize impact, it is essential that policies and programs are guided by up-to-date data and targeted analysis of the evidence on what we know about homicide in the Region and what works to prevent it.
Disclaimer.
Authors hold sole responsibility for the views expressed in the manuscript, which may not necessarily reflect the opinion or policy of the RPSP/PAJPH or the Pan American Health Organization (PAHO).
Acknowledgments.
The authors are grateful to the team of regional advisors from the Department of Evidence and Intelligence for Action in Health (EIH) of the Pan American Health Organization/World Health Organization for their unremitting support in the development of the proposal presented.
Footnotes
Author contributions.
AS, SC, NA, PS, OSR, and BB designed the original study, analyzed the data, and wrote and reviewed the manuscript. All authors reviewed and approved the final version.
Conflict of interest.
None declared.
The World Health Organization (WHO) defines young people as individuals between the ages of 10 and 24 years. Adolescents comprise the 10–19 years age group and youth the 15–24 years age group. In this article, the following age groups are used: young people 10–24, adolescents 10–19, and young adults 20–24.
According to the International Labour Organization (ILO), vulnerable employment is defined as the sum of own-account workers and contributing family workers; it is characterized by informal work arrangements, inadequate earnings, low productivity, and difficult conditions that undermine workers’ rights.
REFERENCES
- 1.United Nations, Department of Economic and Social Affairs, Population Division . Population database. New York: United Nations; 2019. [cited 2023 Mar 23]. World Population Prospects: The 2019 Revision. Internet. Available from: https://population.un.org/wpp/ [Google Scholar]; United Nations, Department of Economic and Social Affairs, Population Division [Internet]. World Population Prospects: The 2019 Revision. Population database. New York: United Nations; 2019 [cited 2023 Mar 23]. Available from: https://population.un.org/wpp/.
- 2.World Health Organization . A Conceptual Framework for Action on the Social Determinants of Health. Geneva: WHO; 2010. Available from: https://apps.who.int/iris/handle/10665/44489. [Google Scholar]; World Health Organization. A Conceptual Framework for Action on the Social Determinants of Health. Geneva: WHO; 2010. Available from: https://apps.who.int/iris/handle/10665/44489.
- 3.United Nations, Working Group on Youth of the Regional Collaborative Platform for Latin America and the Caribbean . Latin American and Caribbean youth and the 2030 Agenda for Sustainable Development: an examination from within the United Nations system. Santiago: United Nations; 2021. Document LC/TS.2021/74. Available from: https://repositorio.cepal.org/handle/11362/47113. [Google Scholar]; United Nations, Working Group on Youth of the Regional Collaborative Platform for Latin America and the Caribbean. Latin American and Caribbean youth and the 2030 Agenda for Sustainable Development: an examination from within the United Nations system. (Document LC/TS.2021/74). Santiago: United Nations; 2021. Available from: https://repositorio.cepal.org/handle/11362/47113.
- 4.United Nations Educational, Scientific and Cultural Organization . Institute for Statistics. Montreal: UNESCO; 2018. [cited 2023 Mar 23]. Internet. Available from: https://uis.unesco.org. [Google Scholar]; United Nations Educational, Scientific and Cultural Organization [Internet]. Institute for Statistics. Montreal: UNESCO; 2018 [cited 2023 Mar 23]. Available from: https://uis.unesco.org.
- 5.World Bank . World Development Indicators (2020). School enrollment, secondary (% net) - Latin America & Caribbean. Washington, DC: World Bank; 2020. [cited 2023 Mar 23]. Internet. Available from: https://data.worldbank.org/indicator/SE.SEC.NENR?end=2019&locations=ZJ&start=2016. [Google Scholar]; World Bank [Internet]. World Development Indicators (2020). School enrollment, secondary (% net) - Latin America & Caribbean. Washington, DC: World Bank; 2020 [cited 2023 Mar 23]. Available from: https://data.worldbank.org/indicator/SE.SEC.NENR?end=2019&locations=ZJ&start=2016.
- 6.World Bank . United Nations Human Settlements Programme (UN-HABITAT) Washington, DC: World Bank; 2018. 2018. [cited 2023 Mar 23]. Population living in slums (% of urban population) - Latin America & Caribbean. Internet. Available from: https://data.worldbank.org/indicator/EN.POP.SLUM.UR.ZS. [Google Scholar]; World Bank [Internet]. Population living in slums (% of urban population) - Latin America & Caribbean. United Nations Human Settlements Programme (UN-HABITAT). 2018. Washington, DC: World Bank; 2018 [cited 2023 Mar 23]. Available from: https://data.worldbank.org/indicator/EN.POP.SLUM.UR.ZS.
- 7.World Health Organization . The Global Health Observatory. Geneva: WHO; c2023. [cited 2023 Mar 23]. Estimates of rate of homicides (per 100 000 population) Internet. Available from: https://www.who.int/data/gho/data/indicators/indicator-details/GHO/estimates-of-rates-of-homicides-per-100-000-population. [Google Scholar]; World Health Organization [Internet]. The Global Health Observatory. Estimates of rate of homicides (per 100 000 population). Geneva: WHO; c2023 [cited 2023 Mar 23]. Available from: https://www.who.int/data/gho/data/indicators/indicator-details/GHO/estimates-of-rates-of-homicides-per-100-000-population.
- 8.Briceño-León R. La comprensión de los homicidios en América Latina: ¿Pobreza o institucionalidad? Cien Saude Colet. 2012;17(12):3159–3170. doi: 10.1590/S1413-81232012001200002. Available from: [DOI] [PubMed] [Google Scholar]; Briceño-León R. La comprensión de los homicidios en América Latina: ¿Pobreza o institucionalidad? Cien Saude Colet. 2012;17(12):3159–70. Available from: 10.1590/S1413-81232012001200002 [DOI] [PubMed]
- 9.United Nations Children’s Fund . Hidden in Plain Sight: A statistical analysis of violence against children. New York: UNICEF; 2014. Available from: https://data.unicef.org/resources/hidden-in-plain-sight-a-statistical-analysis-of-violence-against-children/ [Google Scholar]; United Nations Children’s Fund. Hidden in Plain Sight: A statistical analysis of violence against children. New York: UNICEF; 2014. Available from: https://data.unicef.org/resources/hidden-in-plain-sight-a-statistical-analysis-of-violence-against-children/.
- 10.World Health Organization . Global status report on preventing violence against children 2020. Geneva: WHO; 2020. Available from: https://apps.who.int/iris/handle/10665/332394. [Google Scholar]; World Health Organization. Global status report on preventing violence against children 2020. Geneva: WHO; 2020. Available from: https://apps.who.int/iris/handle/10665/332394.
- 11.Pan American Health Organization . Regional Status Report 2020: Preventing and Responding to Violence against Children in the Americas. Washington, DC: PAHO; 2020. Available from: https://iris.paho.org/handle/10665.2/53038. [Google Scholar]; Pan American Health Organization. Regional Status Report 2020: Preventing and Responding to Violence against Children in the Americas. Washington, DC: PAHO; 2020. Available from: https://iris.paho.org/handle/10665.2/53038.
- 12.Pan American Health Organization . The Health of Adolescents and Youth in the Americas. Implementation of the Regional Strategy and Plan of Action on Adolescent and Youth Health 2010-2018. Washington, DC: PAHO; 2018. Available from: https://iris.paho.org/handle/10665.2/49545. [Google Scholar]; Pan American Health Organization. The Health of Adolescents and Youth in the Americas. Implementation of the Regional Strategy and Plan of Action on Adolescent and Youth Health 2010-2018. Washington, DC: PAHO; 2018. Available from: https://iris.paho.org/handle/10665.2/49545.
- 13.Krug EG, Dahlberg LL, Mercy JA, Zwi AB, Lozano R, editors. World report on violence and health. Geneva: WHO; 2002. Available from: https://apps.who.int/iris/handle/10665/42495. [Google Scholar]; Krug EG, Dahlberg LL, Mercy JA, Zwi AB, Lozano R, editors. World report on violence and health. Geneva: WHO; 2002. Available from: https://apps.who.int/iris/handle/10665/42495.
- 14.Merino J, Zarkin J, Fierro E. Marcado para morir. Nexos. 2013. Jul, Available from: https://www.nexos.com.mx/?p=15375.; Merino J, Zarkin J, Fierro E. Marcado para morir. Nexos. 2013 July. Available from: https://www.nexos.com.mx/?p=15375.
- 15.United Nations Development Programme . Regional Human Development Report 2013-2014. Citizen Security with a Human Face: Evidence from Latin America. New York: UNDP; 2013. Available from: https://www.undp.org/publications/human-development-report-latin-america-2013-2014. [Google Scholar]; United Nations Development Programme. Regional Human Development Report 2013-2014. Citizen Security with a Human Face: Evidence from Latin America. New York: UNDP; 2013. Available from: https://www.undp.org/publications/human-development-report-latin-america-2013-2014.
- 16.United Nations Office on Drugs and Crime . Global study on homicide. Vienna: UNODC; 2019. Available from: https://www.unodc.org/unodc/en/data-and-analysis/global-study-on-homicide.html. [Google Scholar]; United Nations Office on Drugs and Crime. Global study on homicide. Vienna: UNODC; 2019. Available from: https://www.unodc.org/unodc/en/data-and-analysis/global-study-on-homicide.html
- 17.United Nations Office on Drugs and Crime . World Drug Report 2021. Vienna: UNODC; 2021. Available from: https://digitallibrary.un.org/record/3931425. [Google Scholar]; United Nations Office on Drugs and Crime. World Drug Report 2021. Vienna: UNODC; 2021. Available from: https://digitallibrary.un.org/record/3931425.
- 18.World Bank . Crime and Violence in Central America: A Development Challenge. Washington, DC: World Bank; 2011. Available from: https://openknowledge.worldbank.org/handle/10986/2744. [Google Scholar]; World Bank. Crime and Violence in Central America: A Development Challenge. Washington, DC: World Bank; 2011. Available from: https://openknowledge.worldbank.org/handle/10986/2744.
- 19.World Health Organization . Global Health Estimates 2020: Deaths by Cause, Age, Sex, by Country and by Region, 2000-2019. Geneva: WHO; 2020. Internet. Available from: https://www.who.int/data/global-health-estimates. [Google Scholar]; World Health Organization [Internet]. Global Health Estimates 2020: Deaths by Cause, Age, Sex, by Country and by Region, 2000-2019. Geneva: WHO; 2020. Available from: https://www.who.int/data/global-health-estimates.
- 20.Ahmad OB, Boschi-Pinto C, Lopez AD, Murray CJL, Lozano R, Inoue M. Age standardization of rates: A new WHO standard. Geneva: World Health Organization; 2001. (GPE Discussion Paper Series No. 31). Available from: https://cdn.who.int/media/docs/default-source/gho-documents/global-health-estimates/gpe_discussion_paper_series_paper31_2001_age_standardization_rates.pdf. [Google Scholar]; Ahmad OB, Boschi-Pinto C, Lopez AD, Murray CJL, Lozano R, Inoue M. Age standardization of rates: A new WHO standard. (GPE Discussion Paper Series No. 31) Geneva: World Health Organization; 2001. Available from: https://cdn.who.int/media/docs/default-source/gho-documents/global-health-estimates/gpe_discussion_paper_series_paper31_2001_age_standardization_rates.pdf.
- 21.National Cancer Institute . Joinpoint regression program. Bethesda, MD: NCI; 2020. [cited 2020 Jan 12]. Internet. Available from: https://surveillance.cancer.gov/joinpoint/ [Google Scholar]; National Cancer Institute [Internet]. Joinpoint regression program. Bethesda, MD: NCI; 2020 [cited 2020 Jan 12]. Available from: https://surveillance.cancer.gov/joinpoint/.
- 22.World Bank . Databank. World Development Indicators. Washington, DC: World Bank; c2023. [cited 2023 Mar 20]. Internet. Available from: https://databank.worldbank.org/reports.aspx?dsid=2&series=NY.GDP.MKTP.KD. [Google Scholar]; World Bank [Internet]. Databank. World Development Indicators. Washington, DC: World Bank; c2023 [cited 2023 Mar 20]. Available from: https://databank.worldbank.org/reports.aspx?dsid=2&series=NY.GDP.MKTP.KD.
- 23.World Health Organization . Handbook on health inequality monitoring with a special focus on low- and middle-income countries. Geneva: WHO; 2013. [cited 2020 Aug 19]. Available from: https://apps.who.int/iris/handle/10665/85345. [Google Scholar]; World Health Organization. Handbook on health inequality monitoring with a special focus on low- and middle-income countries. Geneva: WHO; 2013 [cited 2020 Aug 19]. Available from: https://apps.who.int/iris/handle/10665/85345.
- 24.Zeoli AM, Grady S, Pizarro JM, Melde C. Modeling the movement of homicide by type to inform public health prevention efforts. Am J Public Health. 2015 Oct;105(10):2035–2041. doi: 10.2105/AJPH.2015.302732. https://doi.org/10.2105%2FAJPH.2015.302732 [DOI] [PMC free article] [PubMed] [Google Scholar]; Zeoli AM, Grady S, Pizarro JM, Melde C. Modeling the movement of homicide by type to inform public health prevention efforts. Am J Public Health. 2015 Oct;105(10):2035–41. https://doi.org/10.2105%2FAJPH.2015.302732. [DOI] [PMC free article] [PubMed]
- 25.Kalesan B, Mobily ME, Keiser O, Fagan JA, Galea S. Firearm legislation and firearm mortality in the USA: a cross-sectional, state-level. Lancet. 2016;387(10030):1847–1855. doi: 10.1016/s0140-6736(15)01026-0. [DOI] [PubMed] [Google Scholar]; Kalesan B, Mobily ME, Keiser O, Fagan JA, Galea S. Firearm legislation and firearm mortality in the USA: a cross-sectional, state-level. Lancet. 2016;387(10030):1847–55. 10.1016/s0140-6736(15)01026-0. [DOI] [PubMed]
- 26.Santaella-Tenorio J, Cerdá M, Villaveces A, Galea S. What Do We Know About the Association Between Firearm Legislation and Firearm-Related Injuries? Epidemiol Rev. 2016;38(1):140–157. doi: 10.1093/epirev/mxv012. [DOI] [PMC free article] [PubMed] [Google Scholar]; Santaella-Tenorio J, Cerdá M, Villaveces A, Galea S. What Do We Know About the Association Between Firearm Legislation and Firearm-Related Injuries? Epidemiol Rev. 2016;38(1):140–57. 10.1093/epirev/mxv012. [DOI] [PMC free article] [PubMed]
- 27.U.S. Centers for Disease Control and Prevention, National Center for Injury Prevention and Control, Division of Violence Prevention . Preventing Multiple Forms of Violence: A Strategic Vision for Connecting the Dots. Atlanta, GA: National Center for Injury Prevention and Control, CDC; 2016. Available from: https://www.cdc.gov/violenceprevention/pdf/strategic_vision.pdf. [Google Scholar]; U.S. Centers for Disease Control and Prevention, National Center for Injury Prevention and Control, Division of Violence Prevention. Preventing Multiple Forms of Violence: A Strategic Vision for Connecting the Dots. Atlanta, GA: National Center for Injury Prevention and Control, CDC; 2016. Available from: https://www.cdc.gov/violenceprevention/pdf/strategic_vision.pdf.
- 28.Wilkins N, Tsao B, Hertz M, Davis R, Klevens J. Connecting the Dots: An Overview of the Links Among Multiple Forms of Violence. Atlanta, GA: National Center for Injury Prevention and Control, Centers for Disease Control and Prevention; Oakland, CA: Prevention Institute; 2014. and. Available from: https://www.cdc.gov/violenceprevention/pdf/connecting_the_dots-a.pdf. [Google Scholar]; Wilkins N, Tsao B, Hertz M, Davis R, Klevens J. Connecting the Dots: An Overview of the Links Among Multiple Forms of Violence. Atlanta, GA: National Center for Injury Prevention and Control, Centers for Disease Control and Prevention, and Oakland, CA: Prevention Institute; 2014. Available from: https://www.cdc.gov/violenceprevention/pdf/connecting_the_dots-a.pdf.
- 29.World Health Organization . Understanding and addressing violence against women: Femicide. Geneva: WHO; 2012. Available from: http://apps.who.int/iris/10665/77421. [Google Scholar]; World Health Organization. Understanding and addressing violence against women: Femicide. Geneva: WHO; 2012. Available from: http://apps.who.int/iris/10665/77421.
- 30.UN Women Gender-motivated killings of women, including femicide. Side event at the 57th session of the Commission on the Status of Women; 2013; New York: UN Women; 2013. Apr 4, Internet. Available from: https://www.unwomen.org/en/news/stories/2013/4/femicide-in-latin-america. [Google Scholar]; UN Women [Internet]. Gender-motivated killings of women, including femicide. Side event at the 57th session of the Commission on the Status of Women (CSW57) 2013. New York: UN Women; 2013 Apr 4. Available from: https://www.unwomen.org/en/news/stories/2013/4/femicide-in-latin-america.
- 31.Nowak M. Research Notes: Armed Violence. Number 14. Geneva: Small Arms Survey; Feb, 2012. 2012. Femicide: A Global Problem. Available from: https://www.smallarmssurvey.org/sites/default/files/resources/SAS-Research-Note-14.pdf. [Google Scholar]; Nowak M. Femicide: A Global Problem. Research Notes: Armed Violence, Number 14, February 2012. Geneva: Small Arms Survey; 2012. Available from: https://www.smallarmssurvey.org/sites/default/files/resources/SAS-Research-Note-14.pdf.
- 32.Economic Commission for Latin America and the Caribbean . Social Panorama of Latin America, 2019. Santiago: ECLAC; 2019. LC/PUB.2019/22-P/Rev.1. Available from: https://repositorio.cepal.org/handle/11362/44989. [Google Scholar]; Economic Commission for Latin America and the Caribbean. Social Panorama of Latin America, 2019. (LC/PUB.2019/22-P/Rev.1). Santiago: ECLAC; 2019. Available from: https://repositorio.cepal.org/handle/11362/44989.
- 33.Sanhueza A, Carvajal-Velez L, Mujica OJ, Vidaletti LP, Victora CG, Barros AJ. SDG3-related inequalities in women’s, children’s and adolescents’ health: an SDG monitoring baseline for Latin America and the Caribbean using national cross-sectional surveys. BMJ Open. 2021;11(8):e047779. doi: 10.1136/bmjopen-2020-047779. [DOI] [PMC free article] [PubMed] [Google Scholar]; Sanhueza A, Carvajal-Velez L, Mujica OJ, Vidaletti LP, Victora CG, Barros AJ. SDG3-related inequalities in women’s, children’s and adolescents’ health: an SDG monitoring baseline for Latin America and the Caribbean using national cross-sectional surveys. BMJ Open. 2021;11(8):e047779. 10.1136/bmjopen-2020-047779. [DOI] [PMC free article] [PubMed]
- 34.Etienne CF, Fitzgerald J, Almeida G, Birmingham ME, Brana M, Bascolo E, et al. COVID-19: transformative actions for more equitable, resilient, sustainable societies and health systems in the Americas. BMJ Glob Health. 2020;5(8):e003509. doi: 10.1136/bmjgh-2020-003509. [DOI] [PMC free article] [PubMed] [Google Scholar]; Etienne CF, Fitzgerald J, Almeida G, Birmingham ME, Brana M, Bascolo E, et al. COVID-19: transformative actions for more equitable, resilient, sustainable societies and health systems in the Americas. BMJ Glob Health. 2020;5(8):e003509. 10.1136/bmjgh-2020-003509. [DOI] [PMC free article] [PubMed]
- 35.Leeb TR, Lewis T, Zolotor AJ. A review of physical and mental health consequences of child abuse and neglect and implications for practice. Am J Lifestyle Med. 2011;5(5):454–468. doi: 10.1177/1559827611410266. [DOI] [Google Scholar]; Leeb TR, Lewis T, Zolotor AJ. A review of physical and mental health consequences of child abuse and neglect and implications for practice. Am J Lifestyle Med. 2011;5(5):454–68. 10.1177/1559827611410266. [DOI]
- 36.Andrews GJ, Corry J, Slade T, Issakidis C, Swanton H. In: Comparative quantification of health risks: global and regional burden of disease attributable to selected major risk factors (Vol. 1) Ezzati M, Lopez AD, Rodgers A, Murray CJL, editors. Geneva: World Health Organization; 2004. Child sexual abuse; pp. 1851–1940.https://apps.who.int/iris/handle/10665/42770 [Google Scholar]; Andrews GJ, Corry J, Slade T, Issakidis C, Swanton H. Child sexual abuse. In: Ezzati M, Lopez AD, Rodgers A, Murray CJL, editors. Comparative quantification of health risks: global and regional burden of disease attributable to selected major risk factors (Vol. 1). Geneva: World Health Organization; 2004:1851–940. https://apps.who.int/iris/handle/10665/42770.
- 37.Kapusta ND, Tran US, Rockett IR, De Leo D, Naylor CPE, Niederkrotenthaler T, et al. Declining autopsy rates and suicide misclassification: A cross-national analysis of 35 countries. Arch Gen Psychiatry. 2011;68:1050–1057. doi: 10.1001/archgenpsychiatry.2011.66. [DOI] [PubMed] [Google Scholar]; Kapusta ND, Tran US, Rockett IR, De Leo D, Naylor CPE, Niederkrotenthaler T, et al. Declining autopsy rates and suicide misclassification: A cross-national analysis of 35 countries. Arch Gen Psychiatry. 2011;68:1050–7. 10.1001/archgenpsychiatry.2011.66. [DOI] [PubMed]
- 38.World Health Organization, U.S. Centers for Disease Control, Global Partnership to End Violence against Children, Pan American Health Organization, Together for Girls, United Nations Children’s Fund et al. INSPIRE: seven strategies for ending violence against children. Geneva: WHO; 2016. Available from: https://apps.who.int/iris/handle/10665/207717. [Google Scholar]; World Health Organization, U.S. Centers for Disease Control, Global Partnership to End Violence against Children, Pan American Health Organization, Together for Girls, United Nations Children’s Fund, et al. INSPIRE: seven strategies for ending violence against children. Geneva: WHO; 2016. Available from: https://apps.who.int/iris/handle/10665/207717.