

Abstract
OBJECTIVE
We examine the interplay of acculturation orientation, cultural stress, and hurricane trauma exposure with behavioral health among Puerto Rican crisis migrants who relocated to the US mainland after Hurricane Maria.
METHOD
Participants were 319 adult (Mage = 39 years; 71% female; 90% arriving in 2017–2018) Hurricane Maria survivors surveyed on the US mainland. Latent profile analysis was used to model acculturation subtypes. In turn, OLS regression was executed to examine the associations of cultural stress and hurricane trauma exposure with behavioral health while stratifying by acculturation subtype.
RESULTS
Five acculturation orientation subtypes were modeled, three of which—Separated (24%), Marginalized (13%), and Full Bicultural (14%)—align closely with prior theorizing. We also identified Partially Bicultural (21%) and Moderate (28%) subtypes. Stratifying by acculturation subtype, with behavioral health (depression/anxiety symptoms) specified as the dependent variable, hurricane trauma and cultural stress accounted for only 4% of explained variance in the Moderate class, a somewhat greater percentage in the Partial Bicultural (12%) and Separated (15%) classes, and substantially greater amounts of variance in the Marginalized (25%) and Full Bicultural (56%) classes.
CONCLUSION
Findings underscore the importance of accounting for acculturation in understanding the relationship between stress and behavioral health among climate migrants.
Keywords: Acculturation, Cultural Stress, Hurricane, Puerto Rico, Behavioral Health
Introduction
Following the devastation of Hurricane Maria in 2017, tens of thousands of Puerto Ricans fled the island territory to seek safe haven on the mainland United States (US). Five years later, although a proportion of Puerto Ricans have returned to the island, many “Maria migrants” have remained as long-term or permanent residents of communities across the mainland US. To varying degrees, Maria migrants are tasked with navigating new cultural contexts, confronting identity-based stressors, and managing the enduring impact of hurricane trauma exposure. Emerging research has begun to examine the importance of these three types of challenges vis-à-vis behavioral health, but no prior research has considered their conjoint importance.
Integrating three distinct theoretical frameworks—Berry’s model of acculturation, cultural stress theory, and the crisis migration stress framework—we aim to provide fresh insights by examining the interplay of acculturation orientation, migration-related cultural stress, and hurricane trauma exposure vis-à-vis the behavioral health of Maria migrants in the US. We begin by modeling a multidimensional acculturation orientation typology and, in turn, examining crisis migration experiences, cultural stressors, and behavioral health outcomes among individuals classified into distinct acculturation subtypes. Next, drawing from the subtypes emerging from our analysis, we examine the degree to which the relationship between cultural stress/crisis migration factors and behavioral health varies as a function of acculturation orientation. Having provided a basic introduction to the present study, we now provide a more in-depth overview of relevant theoretical and empirical contributions before articulating specific research questions.
Theoretical Frameworks
An important body of scholarship examines the processes of cultural change and adaptation within the framework of international or intercultural migration. Berry’s (1992, 2017) seminal work focused on the construct of acculturation with a particular emphasis on the ways in which—to varying degrees and in a variety of combinations—migrants retain and/or shed aspects of their heritage culture while simultaneously adopting (or not) elements of the destination culture. Within Berry’s model, intersecting heritage and destination cultural dimensions allow us to identify four potential permutations conceptualized as acculturation types or orientations: assimilation (heritage culture is minimized/rejected, destination culture is valued/embraced), separation (heritage culture is valued/embraced, destination culture is minimized/rejected), integration or bicultural (both heritage and destination cultures are valued/embraced), and marginalization (both heritage and destination cultures are minimized/rejected). Subsequent work has modeled each of the aforementioned orientations with an array of Latino samples in the US (e.g., college students, undocumented adults, national probability sample) by employing person-centered approaches (Meca et al., 2018; Salas-Wright et al., 2015; Schwartz & Zamboanga, 2008).
Separate from work in the domain of acculturation orientation, recent years have seen the emergence of two additional theoretical frameworks focused on the experiences of immigrants from Latin America: cultural stress theory and the crisis migration stress framework. Cultural stress theory focuses on the ways in which exposure to a constellation of post-migration stressors can lead to psychological distress (Salas-Wright & Schwartz, 2019). Key constructs within this framework include perceived discrimination (i.e., tangible instances of direct interpersonal slights, mistreatment, or hostility based on one’s ethnic identity or migrant status), negative context of reception (i.e., a general sense of unwelcomeness or coldness towards one’s ethnic or immigrant group), and language-related stress (i.e., language difficulty or discomfort/marginalization related to lack of fluency or a non-native accent). The crisis migration stress framework extends cultural stress theory by considering how exposure to macro-level pre-migration stressors may also relate to post-migration behavioral health both independently and in combination with post-migration stressors (Vos et al., 2021). This framework builds upon the broader construct of crisis migration, which refers to large-scale emigration in the face of a crisis event that takes place in a context of pre-existing social vulnerability (McAdam, 2014). The large-scale movement of Puerto Ricans to the US mainland following Hurricane Maria is an example of crisis migration—it resulted from the confluence of pre-hurricane economic downturn, infrastructure vulnerability, and a powerful climate event (Salas-Wright et al., 2021). This migration was facilitated by an already existing cycle of migration between Puerto Rico and the US mainland where downturns in the island economy pushed people off island and later downturns in the US mainland allowed the allure of the island to pull people back home (Silver, 2020).
A New Angle: Acculturation May Shape the Migration Stress-Behavioral Health Link
Prior research has examined the ways in which acculturation orientation, cultural stress, and crisis migration stress relate to behavioral health (see Schwartz, Zamboanga, et al., 2023 for an in-depth review). At the risk of oversimplifying this vast literature, we generally see that bicultural integration often emerges as the most adaptive acculturation orientation (Schwartz et al., 2010) and that elevated levels of exposure to pre-migration crisis stressors (Salas-Wright et al., 2022; Scaramutti et al., 2019) and post-migration cultural stress (Cano et al., 2015; Lorenzo-Blanco et al., 2016) is detrimental to mental health and wellbeing. Emerging work has begun to examine how crisis factors and cultural stress interrelate (Schwartz et al., 2023) and interact (Montero-Zamora et al., in press), but generally these constructs are examined separately from one another. This tendency toward conceptual “siloing” risks overlooking the interplay among a set of constructs that are likely to touch upon one another in the lives of many migrants.
Of particular relevance to the present study, we note that migration stress-health research is often conducted with the tacit assumption that pre- and post-migration stressors relate to behavioral health in the same way for all migrants. It seems quite plausible, however, that such an assumption is untenable. Consider the differences in how an individual who endorses a separation orientation (in which the value of the receiving country’s culture is largely minimized or rejected) may differ from an individual of a bicultural orientation (in which both the heritage and receiving cultures are valued and embraced). It seems plausible that individuals who place less value on—or are less connected with—their receiving cultures (i.e., a separation orientation) may experience discrimination or negative context of reception differently compared to individuals who actively seek to integrate their heritage and receiving cultures (i.e., an integrated or bicultural orientation). In this hypothetical case, our expectation is that a bicultural individual would experience, compared to a “separated” individual, a more acute sense of rejection and distress given that they have opened themselves up for cultural engagement and, presumably, hope for social or cultural acceptance. There are many potential comparisons we could suggest, but the primary issue at play here is the notion that pre- and post-migration stressors may relate differently to behavioral health outcomes on the basis of one’s acculturation orientation.
The Present Study
Drawing from a sample of Puerto Rican Maria migrants residing on the US mainland, in the present study we aimed to examine the interplay of acculturation orientation, cultural stress, and crisis migration stress with behavioral health. To achieve our aims, we executed this study in two general steps or “parts.” In part one, we generate a typology of acculturation orientations using a person-centered approach. Although our analytic approach for this initial analysis (latent profile analysis [LPA]) is inherently exploratory, we expect—based on prior theory and research—to identify subtypes that align with Berry’s bidimensional model of acculturation. In part two, in turn, we examine the associations of cultural stress and hurricane trauma with behavioral health both in the full sample and while stratifying our sample by acculturation orientation. This approach is a departure from the de facto approaches used in cultural stress/crisis migration research (which tend to assume that migration-related factors will impact behavioral health in the same way for all migrants), and it thereby promises to provide new evidence as to how acculturation shapes the relationships of pre- and post-migration stressors with behavioral health.
Method
Recruitment and Sample
Participants were recruited using a referral system where initial seed participants are referred through community partners, and participants refer others to the study in exchange for additional compensation (Heckathorn, 2002). Participants were compensated $100 for completing the study measures, and an additional $30 per successful referral (i.e., referred participant who joined the study). Each participant was allowed to refer up to five additional participants.
Participants in the present study were 319 adult Hurricane Maria survivors (92 males, 227 females; mean age 38.7, range 18–77, 80% under age 50) residing on the US mainland. A majority (59.3%) of participants arrived on the US mainland in 2017; 29.2% in 2018; and 10.1% in 2019 or 2020. The majority of participants (75.3%) were living in Central Florida at the time of data collection, but participants were also recruited from other locations including Texas (6.3%), New England (3.8%), Illinois (3.2%), and other US locations (11.4%).
Procedures
Data were collected between August 2020 and October 2021. Because data collection took place during the COVID-19 pandemic, all data collection activities occurred virtually. Participants were recruited in partnership with our community partner organizations in Central Florida and elsewhere, and via peer referrals from existing participants. Research team members, along with assessors working in the local community, distributed flyers and recruited eligible participants to enroll in the study. Anyone who was a Maria survivor and was 18 or older was eligible to take part in the study. Those who agreed to participate were consented/enrolled, receiving their surveys via e-mail. Study staff members were available to help troubleshoot technical difficulties as needed. All participants completed the survey in Spanish, although an English version was available.
Measures
Acculturation
Items from Szapocznik et al.’s (1980) Bicultural Involvement Questionnaire were used to model participant endorsement of involvement in Puerto Rican / Latino and US activities. Separate sets of items measure the degree to which individuals endorse enjoyment of music, dances, places, recreation, television, radio, and books/magazines that are either (a) Puerto Rico/Latino oriented (first set) or US oriented (second set). Response options for each item range from 1 (Not at All) to 5 (Very Much).
Hurricane Trauma
Items from the Hurricane-Related Traumatic Experiences Questionnaire (HURTE; La Greca et al, 1996) were used to assess life threatening trauma associated with Hurricane Maria. The measure is a checklist where the respondent is asked to indicate whether or not each event occurred during their experiences of the storm. Example items include thinking that one might die and being hit by flying or falling debris or objects. The total HURTE score is computed as the number of items that the person endorsed, ranging from zero to five.
Cultural Stress
Cultural stress was examined in terms of discrimination, negative context of reception, and language stress. Perceived discrimination (α = .95) was assessed via Phinney et al.’s (1998) 7-item instrument. This measure includes events such as being called hurtful names and being treated unfairly by employers or other authority figures. Participants were asked how often each event occurred in their lives, using a Likert scale ranging from 1 (Not at All) to 5 (Almost Every Day).
Negative context of reception (α = .84) was measured via the 6-item Negative Context of Reception Scale (Schwartz et al., 2014; Salas-Wright et al., 2021). Items refer to a lack of opportunities available to Puerto Ricans compared to other migrant groups and to a perception that the receiving community does not welcome or accept Puerto Ricans. Participants responded to each item using a 5-point Likert scale ranging from 1 (Strongly Disagree) to 5 (Strongly Agree).
Language stress (α = .88) was measured via the corresponding subscale from the Hispanic Stress Inventory (Cervantes et al., 1990) to assess stress stemming from the switch from a Spanish-dominant to an English-dominant context. Items refer to feelings and experiences such as being embarrassed about one’s accent when speaking English, having difficulty understanding English speakers, and feeling uncomfortable around people who speak only English. Participants responded to each item using a 5-point Likert scale ranging from 1 (Strongly Disagree) to 5 (Strongly Agree).
Behavioral Health
Behavioral health was assessed in terms of depression and anxiety symptoms. For depressive symptoms (α = .89), we used the Boston Form of the Centers for Epidemiologic Studies Depression Scale (Grzywacz et al., 2006). This instrument taps into symptoms such as listlessness, anhedonia, and lack of interest in activities during the week prior to assessment. Consistent with other cross-cultural and non-English language studies (Yu et al., 2013), the two positively phrased items in the ten-item scale (“I was happy,” “I enjoyed life”) were removed due to very low (i.e., .05 and −.04, respectively) item-total correlation values. Participants responded to each item using a 4-point Likert scale ranging from 0 (Rarely or None of the Time) to 3 (All of the Time).
For anxiety symptoms (α = .93), we used the 7-item Generalized Anxiety Disorder (GAD) scale (Spitzer et al., 2006) to assess anxiety. This measure assesses symptoms of anxiety, such as excessive worrying, tension, irritability, and difficulty sleeping, during the two weeks prior to the assessment. Sample items include “feeling nervous, anxious or on edge”. Participants responded to each item using a 4-point Likert scale ranging from 0 (Not at all) to 3 (Nearly Every Day). In part two of our analyses, we also created a behavioral health variable in which depression and anxiety scores were aggregated as one total behavioral health outcome (α = .88).
Demographic Factors
Sociodemographic factors included: age, gender, education level, migration year, number of prior US mainland visits, and English proficiency (see Table 2 for response categories).
Table 2.
Migration Related Cultural Stress and Mental Health Outcomes, by Latent Classes
| #1: Moderate (n = 91; 28.3%) |
#2: Separated (n = 77; 24.0%) |
#3: Partial Bicultural (n = 66; 20.6%) |
#4: Marginalized (n = 43; 13.4%) |
#5: Full Bicultural (n = 44; 13.7%) |
|||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| M (SD) | M (SD) | RR | 95% CI | M (SD) | RR | 95% CI | M (SD) | RR | 95% CI | M (SD) | RR | 95% CI | |
| Migration-Related Stress | |||||||||||||
| Hurricane Trauma | 1.14 (1.22) | 1.12 (1.00) | 0.94 | (0.7–1.3) | 1.36 (1.13) | 1.21 | (0.9–1.6) | 1.05 (0.88) | 0.80 | (0.5–1.2) | 1.02 (1.04) | 1.01 | (0.7–1.5) |
| Negative Context | 2.51 (0.74) | 2.56 (0.75) | 0.98 | (0.6–1.5) | 2.42 (0.88) | 0.85 | (0.5–1.3) | 2.59 (0.75) | 1.10 | (0.6–1.9) | 2.03 (0.86) | 0.38 | (0.2–0.6) |
| Discrimination | 2.21 (0.84) | 2.33 (0.90) | 1.08 | (0.8–1.5) | 2.12 (0.95) | 0.90 | (0.6–1.3) | 2.37 (0.86) | 1.15 | (0.7–1.8) | 1.49 (0.90) | 0.31 | (0.2–0.5) |
| Language Stress | 2.36 (0.74) | 2.71 (0.64) | 1.93 | (1.1–3.4) | 2.40 (0.76) | 1.11 | (0.6–2.0) | 2.56 (0.54) | 1.50 | (0.8–2.9) | 1.72 (0.79) | 0.29 | (0.1–0.6) |
| Behavioral Health Outcomes | |||||||||||||
| Depression | 1.76 (0.66) | 1.94 (0.67) | 1.56 | (0.9–2.6) | 1.73 (0.61) | 0.97 | (0.6–1.6) | 1.85 (0.67) | 1.26 | (0.7–2.3) | 1.32 (0.50) | 0.24 | (0.1–0.5) |
| Anxiety | 1.78 (0.85) | 2.01 (0.85) | 1.53 | (1.0–2.3) | 1.76 (0.74) | 1.02 | (0.7–1.6) | 1.87 (0.80) | 1.15 | (0.7–1.9) | 1.24 (0.50) | 0.20 | (0.1–0.4) |
Notes. Class #1 is reference class. M = Mean value for latent class. SD = Standard deviation. RR = Risk ratio. CI = Confidence interval.
Data Analysis
In the first part of the analyses, we began by identifying a sequence of latent profile models, ranging from one to six classes, using the Latent GOLD® 5.1 software. LPA is a statistical procedure that assigns individual cases to their most likely latent subgroups—“profiles” or “classes,” terms we use interchangeably—on the basis of observed data (McLachlan et al., 2019). The fourteen acculturation items (7 for Puerto Rico/Latino orientation and 7 for US orientation) were specified as indicator variables.
Five statistical criteria were used to identify the best fitting model: the Bayesian Information Criterion (BIC), Akaike Information Criterion (AIC), Consistent Akaike Information Criterion (CAIC), log likelihood (LL), and entropy. Lower BIC, AIC, and CAIC values, and higher LL values, reflect better model fit. Higher entropy values indicate clearer class delineation, with values above .80 generally viewed as acceptable (Weller et al., 2020). When selecting the best fitting model, it is also essential to consider the substantive interpretability of the solution.
After modeling the latent profiles, multinomial regression was conducted—with the nominal class solution specified as the dependent variable—using Stata 16.1 SE to examine key correlates of class membership. Multinomial regression is a statistical procedure designed for nominal outcomes that contain categories assumed to be unordered (Long & Freese, 2006).
Finally, in part two, we examined the associations of hurricane trauma and cultural stress with behavioral health (depression and anxiety scores aggregated as one total behavioral health outcome) among the full sample and by latent class. Specifically, ordinary least squares (OLS) regression was conducted with hurricane trauma and cultural stress specified as independent variables and behavioral health as the dependent variable—both for the full sample and within each of the subpopulations identified during the LPA modeling in the first part of the analyses.
Results
The Selection of a Solution
The statistical criteria suggested that a five-class solution provided the best fit to the data. Although the log likelihood, BIC, AIC, and CAIC values for the six-class solution were slightly superior to that of the five-class solution, these were relatively minor differences. As shown in Figure 1, the accelerated flattening of the fit statistics suggested that the addition of a sixth class would not be parsimonious. The entropy values for 2–6 class solutions were all above .90. Beyond fit statistics, the clear, coherent conceptual interpretability of the five-class solution provided further evidence for excluding the sixth class (in contrast, the sixth class was challenging to distinguish from the Moderate class described below).
Figure 1.
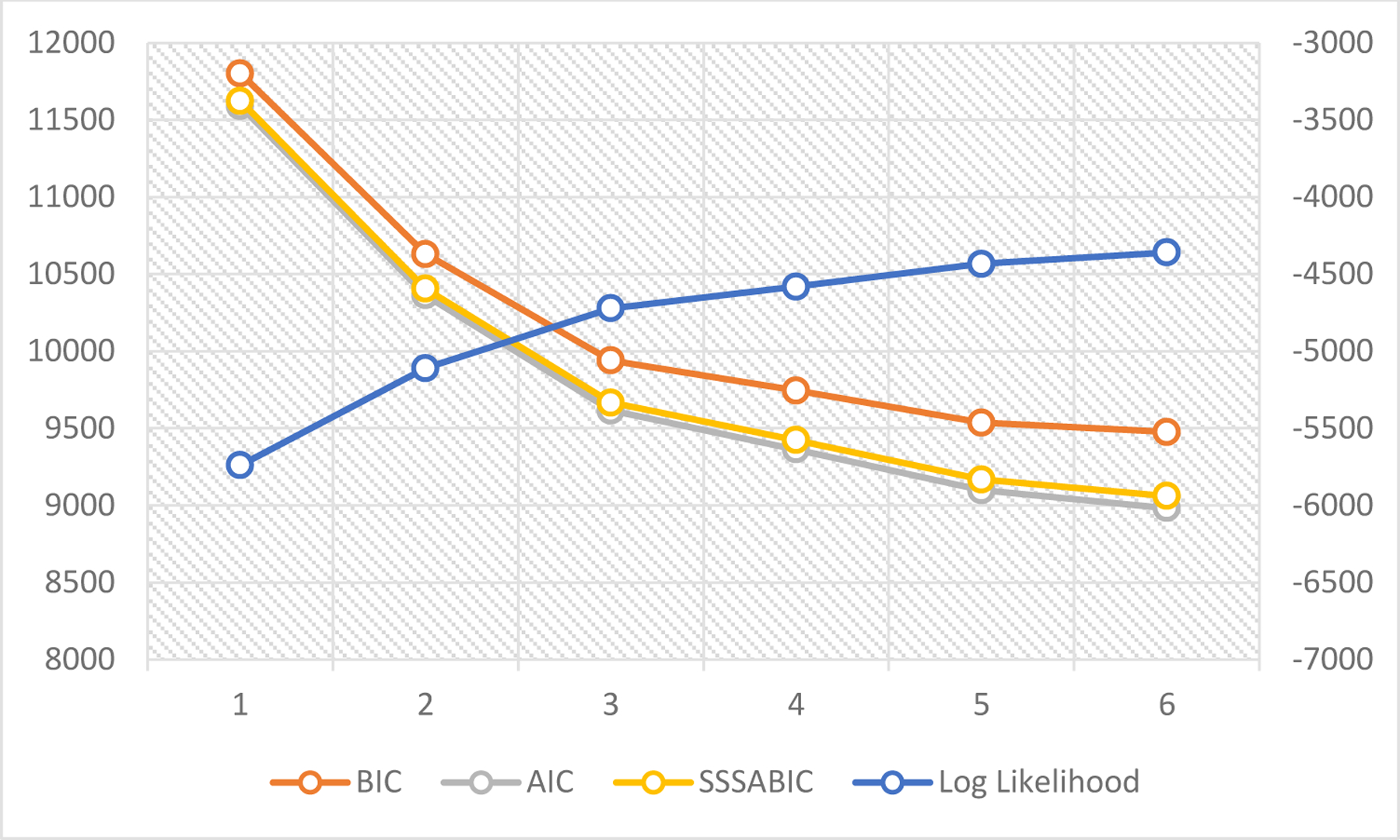
Visualization of Goodness of Fit Indices. Bayesian Information Criterion (BIC), Akaike’s Information Criterion, and Sample Adjusted Bayesian Information Criterion (SSABIC) are displayed on the y-axis to the left of the figure. Log likelihood statistics correspond with the y-axis to the right of the figure. Numbers along the x-axis represent the number of classes modeled.
Characteristics of the Latent Classes
The five-class solution consisted of Class 1, labeled Moderate (28.3%); Class 2, labeled Separated (24.0%); Class 3, labeled Partial Bicultural (20.6%); Class 4, labeled Marginalized (13.4%); and Class 5, labeled Full Bicultural (13.7%). Class 1 was characterized by mean scores in the moderate range for endorsement of Puerto Rican and US activities. Class 2 was characterized by high engagement with Puerto Rican activities and low-to-neutral engagement in US activities. Notably, as shown in Table 1, this class had the highest proportion of respondents who were female, arrived in 2017, and spoke very poor/poor English. Additionally, as shown in Table 2, members of this class were more likely—compared to Class 1, the reference class—to report elevated language stress (RR = 1.93, 95% CI = 1.1–3.4) and anxiety symptoms (RR = 1.53, 95% CI = 1.0–2.3). Class 4 was defined by having the lowest scores in terms of engagement with either Puerto Rican or US activities. Classes 3 and 5 were similar in terms of engagement with Puerto Rican activities, but Class 3 reported relatively lower levels of engagement with US activities whereas Class 5 was defined by universally high levels of engagement for all US activities. Class 5 had the highest proportion of respondents arriving in 2019/2020 and the highest proportion of respondents reporting good/very good English proficiency. Compared to the reference class, Members of Class 5 were less likely to endorse all cultural stress experiences and report behavioral health symptoms. No differences in hurricane trauma were noted for any of the classes.
Table 1.
Demographic Characteristics of the Latent Classes
| #1: Moderate (n = 91; 28.3%) |
#2: Separated (n = 77; 24.0%) |
#3: Partial Bicultural (n = 66; 20.6%) |
#4: Marginalized (n = 43; 13.4%) |
#5: Full Bicultural (n = 44; 13.7%) |
||
|---|---|---|---|---|---|---|
| n (%) | n (%) | n (%) | n (%) | n (%) | chi 2 | |
| Age | ||||||
| 18–34 | 43 (49.43) | 26 (33.77) | 29 (43.94) | 12 (27.91) | 14 (31.82) | ns |
| 35–49 | 34 (39.08) | 31 (40.26) | 28 (42.42) | 17 (39.53) | 20 (45.45) | |
| 50 and older | 10 (11.49) | 20 (25.97) | 9 (13.64) | 14 (32.56) | 10 (22.73) | |
| Gender | ||||||
| Male | 31 (34.83) | 11 (14.29) | 15 (22.73) | 16 (37.21) | 19 (43.18) | 16.58** |
| Female | 58 (65.17) | 66 (85.71) | 51 (77.27) | 27 (62.79) | 25 (56.82) | |
| Education | ||||||
| High school only or less | 27 (30.34) | 30 (38.96) | 17 (25.76) | 20 (46.51) | 10 (22.73) | ns |
| Some college or more | 62 (69.66) | 47 (61.04) | 49 (74.24) | 23 (53.49) | 34 (77.27) | |
| Migration Year | ||||||
| 2017 | 55 (63.22) | 52 (68.42) | 40 (61.54) | 22 (52.38) | 20 (45.45) | 26.13** |
| 2018 | 24 (27.59) | 19 (25.00) | 21 (32.31) | 18 (42.86) | 11 (25.00) | |
| 2019/2020 | 8 (9.20) | 5 (6.58) | 4 (6.15) | 2 (4.76) | 13 (29.55) | |
| Prior Mainland U.S. Visits | ||||||
| None | 15 (17.05) | 14 (18.18) | 10 (15.15) | 12 (27.91) | 4 (9.09) | na |
| One | 13 (14.77) | 13 (16.88) | 12 (18.18) | 11 (25.58) | 4 (9.09) | |
| Two+ | 60 (68.18) | 50 (64.94) | 44 (66.67) | 20 (46.51) | 36 (81.82) | |
| English Proficiency | ||||||
| Very poor/poor | 53 (59.55) | 57 (74.03) | 39 (59.09) | 29 (67.44) | 18 (40.91) | 13.92** |
| Good/very good | 36 (40.45) | 20 (25.97) | 27 (40.91) | 14 (32.56) | 26 (59.09) |
Notes. Class #1 is reference class. M = Mean value for latent class. SD = Standard deviation. RR = Risk ratio. CI = Confidence interval.
Migration-Related Stress and Behavioral Health vis-à-vis Acculturation
As shown in Table 3, hurricane trauma was not significantly associated with behavioral health in the full sample, but greater cultural stress was associated with greater behavioral health symptoms (β = .403, p < .001). In the full sample, the R2 was .186 with the use of the rego module—which decomposes the share of explained variance—indicating that 89.5% of the variance was explained by cultural stress.
Table 3.
Regressing Migration Related Stress on Behavioral Health, by Latent Classes
| Full Sample | #1: Moderate (n = 91; 28.3%) |
#2: Separated (n = 77; 24.0%) |
#3: Partial Bicultural (n = 66; 20.6%) |
#4: Marginalized (n = 43; 13.4%) |
#5: Full Bicultural (n = 44; 13.7%) |
|||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| B(SE) | β | B(SE) | β | B(SE) | β | B(SE) | β | B(SE) | β | B(SE) | β | |
| Hurricane Trauma | .052 (.032) | .084 | −.063 (.066) | −.105 | .140 (.078) | .194 | .118 (.059) | .254 | .139 (.108) | .174 | .162 (.045) | .372** |
| Cultural Stress | .409 (.053) | .403*** | .294 (.129) | .253* | .391 (.124) | .342** | .175 (.115) | .195 | .573 (.153) | .505** | .413 (.070) | .607*** |
| Model: | F (2,311) = 7.83*** | F (2,84) = 2.64 | F (2,72) = 7.67** | F (2,63) = 5.23** | F (2,39) = 7.83** | F (2,41) = 28.0** | ||||||
| R 2 | .186 | .059 | .176 | .142 | .286 | .577 | ||||||
| Adjusted R2 | .181 | .037 | .153 | .115 | .250 | .557 | ||||||
Notes.
p < .05,
p < .01,
p < .001
In terms of the relationship between hurricane stress and behavioral health, no significant association was observed for Classes 1–4; however, greater hurricane trauma exposure was associated with greater behavioral health symptoms in Class 5 (β = .372, p < .01). With the exception of Class 3, cultural stress was significantly associated with behavioral health symptoms for all of the subgroups. Notably, the variance explained by hurricane trauma and cultural stress differed substantially across the latent classes. These variables (hurricane trauma, cultural stress) accounted for only 3.7% of explained variance in Class 1, a somewhat greater percentage in Classes 2 (15.3%) and 3 (11.5%), and substantially greater amounts of variance in Classes 4 (25.0%) and 5 (55.7%).
Discussion
Drawing from a sample of Puerto Rican adults displaced to the US mainland following Hurricane Maria, findings from the present study shed new light on our understanding of the connections among acculturation, migration-related stress, and behavioral health. Below we highlight key findings corresponding with the study’s two primary goals.
Part One: Toward a Typology of Acculturation Orientation
The first key finding is that a clear acculturation typology emerged using our unique sample of Puerto Rican crisis migrants. Three of the five classes modeled fit cleanly into Berry’s (2017) typology—the “Separated” class (24%), characterized by high endorsement of Puerto Rican activities and low-to-neutral endorsement of US activities; the “Marginalized” class (13%), characterized by neutral endorsement of Puerto Rican activities and low endorsement of US activities; and the “Full Bicultural” class (14%), characterized by high endorsement of both Puerto Rican and US activities. We also identified two additional classes that, although they fit less neatly into Berry’s typology, were coherent and distinct: a “Partially Bicultural” (21%) class and a “Moderate” class (28%). Not surprisingly, given the fairly recent arrival of these individuals on the US mainland, no “Assimilated” class emerged.
In terms of the characteristics and experiences of latent class members, several salient points can be noted. First, members of the Separated class were more likely than members of other classes to report limited English language ability (74% versus 57% in the remainder of the sample). This finding is consistent with a clear pattern observed in prior acculturation typology-focused research (Salas-Wright et al., 2015), and is generally in keeping with the logic that language proficiency/acquisition and overall destination cultural engagement are profoundly interconnected (Portes & Rumbaut, 2014). Second, we found that members of the Separated class reported significantly elevated anxiety symptom scores as well as noteworthy but not statistically elevated levels of depressive symptomatology. This finding is in keeping with prior research with migrant populations that points to a robust association between the separation orientation and anxiety, but more mixed findings in terms of separation and depressive symptoms (Choy et al., 2021).
With respect to the Full Bicultural class, members of this class were much more likely to be proficient in English as compared to the rest of the sample (59% spoke well or very well, compared to 35% of the full sample) and reported substantially lower levels of self-reported discrimination, negative context of reception, and language stress. This finding is consistent with other research conducted with migrant samples suggesting that bicultural individuals are far less likely than other migrants to endorse culturally stressful experiences (Meca et al., 2018; Schwartz & Zamboanga, 2008). Notably, Full Bicultural class members also scored substantially lower on measures of depression and anxiety symptom severity than did members of all other classes. This finding is in keeping with a broad literature suggesting that biculturalism is generally the most adaptive approach to acculturation, and that biculturalism often yields positive mental health benefits (Choy et al., 2021; Schwartz et al., 2010; Zamboanga et al., 2020).
Part Two: Migration Stress and Behavioral Health Links vis-à-vis Acculturation Orientation
In part one, we provided clear evidence that bicultural Maria survivors were substantially less likely—compared to all other survivors in the sample—to endorse migration-related cultural stress and to report symptoms of mental health problems. In Part Two, we take our inquiry one step further to examine the relationships between pre- and post-migration stress and behavioral health as a function of acculturation orientation.
Findings in the Full Sample
In our full sample of Maria migrants, the associations between pre-migration and post-migration stress and behavioral health symptoms are relatively clear and straightforward: For each 1 SD increase in cultural stress, we see a corresponding significant (p < .001) beta increase of .40 SD, but no association is observed between hurricane trauma and behavioral health. Together, hurricane trauma and cultural stress explain roughly 18% of the variation in behavioral health in the model, with 89% of the explained variability being attributable to cultural stress and only 11% attributable to hurricane trauma.
The cultural stress finding is broadly consistent with an array of studies examining migration-related cultural stress and behavioral health among a variety of samples, including post-Maria Puerto Rican migrants (see Salas-Wright et al., 2021; Schwartz et al., 2023), as well as a broad literature on discrimination and mental health (Vargas et al., 2020). The null finding for hurricane trauma is unexpected, but it is noteworthy that the trauma-behavioral health link is significant if cultural stress is excluded from the model—thereby suggesting that the outsized importance of cultural stress with respect to behavioral health seems to displace the impact of pre-migration hurricane trauma.
Findings Within Acculturation Orientations
In examining the connections among hurricane trauma, cultural stress, and behavioral health within particular acculturation subtypes, a more complex portrait emerges, with the Full Bicultural class standing out (again) as a unique subset. Indeed, among members of the Full Bicultural class, we see that both hurricane trauma (β = .37, p < .01) and cultural stress (β = .61, p < .001) were robustly associated with behavioral health, together explaining 56% of the variance in the model (with 70% of this explained variance accounted for by cultural stress).
These findings are remarkable for at least two reasons. First, we see that hurricane trauma is not a significant predictor of behavioral health symptoms in the full sample or within any of the other latent classes, but it is among the Bicultural Class (even when accounting for cultural stress). This suggests that hurricane trauma has a unique, sizeable, and otherwise hidden effect among fully bicultural individuals. This finding carries obvious clinical implications, but the precise dynamics of why this is the case are less clear and, unfortunately, our data do not provide direct answers. One possibility is that, on average, bicultural individuals may find it easier to navigate the myriad (linguistic, logistical, interpersonal, and vocational) challenges vis-à-vis life on the US mainland than may other Maria migrants who are less culturally adroit. Whereas these countless “micro-stressors” may combine to be critical or even primary drivers of behavioral health symptoms for most migrants, fully bicultural individuals are less affected by cross-cultural dynamics (thereby allowing hurricane trauma to emerge as a significant predictor of behavioral health symptoms). As such, among bicultural Maria survivors, hurricane trauma, rather than representing one stressor among many, may manifest as a primary stressor that is uniquely connected to behavioral health. Also of note is the fact that no mean differences were observed in terms of hurricane exposure among the acculturation orientation subgroups, which suggests that differences in exposure to the storm are not driving these findings for Full Bicultural migrants.
The findings for the Full Bicultural class are also remarkable in terms of variance explained. Indeed, the adjusted R2 for the model with the Full Bicultural class (Adj. R2 = .56) is more than five times greater than for the rest of the sample combined (Adj. R2 = .11)—and it is more than twice that of the class with the second largest R2 value (the Marginalized class, which has an adjusted R2 value of .25) and more than 15 times greater than that of the class with the lowest R2 value (the Moderate class, which has an R2 value of .04). The critical implication here is that these variance-explained differences provide evidence that the relationship of migration-related stressors (especially cultural stress, which accounts for most of the variance in the full sample and in the Full Bicultural class) with behavioral health is not uniform, but varies quite dramatically as a function of acculturation orientation. In other words, these findings point compellingly to the importance of accounting for acculturation orientation in understanding the impact of migration-related stress on behavioral health.
To be sure, these findings beg the question of why cultural stressors may be especially deleterious for Full Bicultural individuals. Although our data do not allow us to understand the precise mechanisms in play, we can offer several possibilities as to why cultural stress relates so powerfully to behavioral health among this subgroup. One possible explanation relates to the fact that bicultural individuals in our sample were specifically identified based on their high endorsement of not only Puerto Rican but also US cultural activities. In other words, these are individuals who are open to robust engagement with their new receiving context—it may be that such openness to engagement makes Full Bicultural individuals more psychologically vulnerable to rejection compared to others in our sample (who fall on a spectrum of full disengagement to partial engagement with US culture). A related possibility is that Full Bicultural individuals may expect, consciously or unconsciously, to be granted a warm welcome in the receiving context, given their openness to and familiarity with US culture. In the face of such expectations, it may be that exposure to cultural stress is experienced as a “rude awakening” that, despite one’s best efforts, new environments (including the US mainland for US citizens from Puerto Rico) are not universally welcoming.
Limitations
Findings from the present study should be interpreted in light of several limitations. First, all data are based on respondents’ self-report. It would be optimal to have data from additional reporters in terms of acculturation and cultural stress. Additionally, although our measures of depression and anxiety symptom severity are psychometrically sound, they are not equivalent to a clinical psychiatric interview. Second, our data are cross-sectional. As such, we cannot speak to the ways in which acculturation orientation may relate to cultural stress experiences and behavioral health over time. Future research into the prospective relationships between these constructs would provide additional insights. Third, although our sample is large enough to comfortably conduct latent profile analysis, we are somewhat limited in our ability to examine the associations among variables within latent classes. A larger sample would facilitate additional comparisons and more complex modeling. Additionally, our sample size does not allow us to examine differences between migrants in distinct regions across the US—it is possible that a migrant’s experience in Texas may be quite distinct from those in New England or Central Florida, and future research should account for this. Finally, our sample of Maria migrants cannot be described as representative of the full population of Puerto Ricans who relocated to the US mainland in the aftermath of Hurricane Maria. Therefore, we are careful to note that our results may not be generalizable to the broader population or to other populations of crisis/climate migrants.
Conclusion
Despite these and other limitations, findings from the present study provide new insights into the experiences of Puerto Ricans who relocated to the US mainland following Hurricane Maria. Analyses were conducted in two primary phases. In the first phase, using a person-centered approach, we identified five acculturation orientation subtypes, three of which—Separated, Marginalized, and Full Bicultural—align closely with prior theorizing. Notably, members of the Full Bicultural class scored substantially lower on all measures of cultural stress and reported better behavioral health compared to the other classes. Across the board, no differences were observed in terms of hurricane trauma exposure vis-à-vis acculturation orientation.
In the second phase of analysis, we examined the relationship between migration-related stress and behavioral health in the full sample and by acculturation orientation. Two primary findings emerged. First, although hurricane trauma did not predict behavioral health symptoms in the full sample, it emerged as a robust predictor within the Full Bicultural class. Second, considerable variation was observed in terms of the magnitude of the associations of and percentage of variance explained by hurricane trauma and cultural stress, with the Full Bicultural class standing out as the subgroup for which, by far, the most variability in mental health outcomes was explained. Overall, findings underscore the critical importance of accounting for acculturation orientation in understanding the relationship between migration-related cultural stressors and behavioral health among Maria migrants in the US. We hope that the present study will inspire additional work in this important direction.
Figure 2.
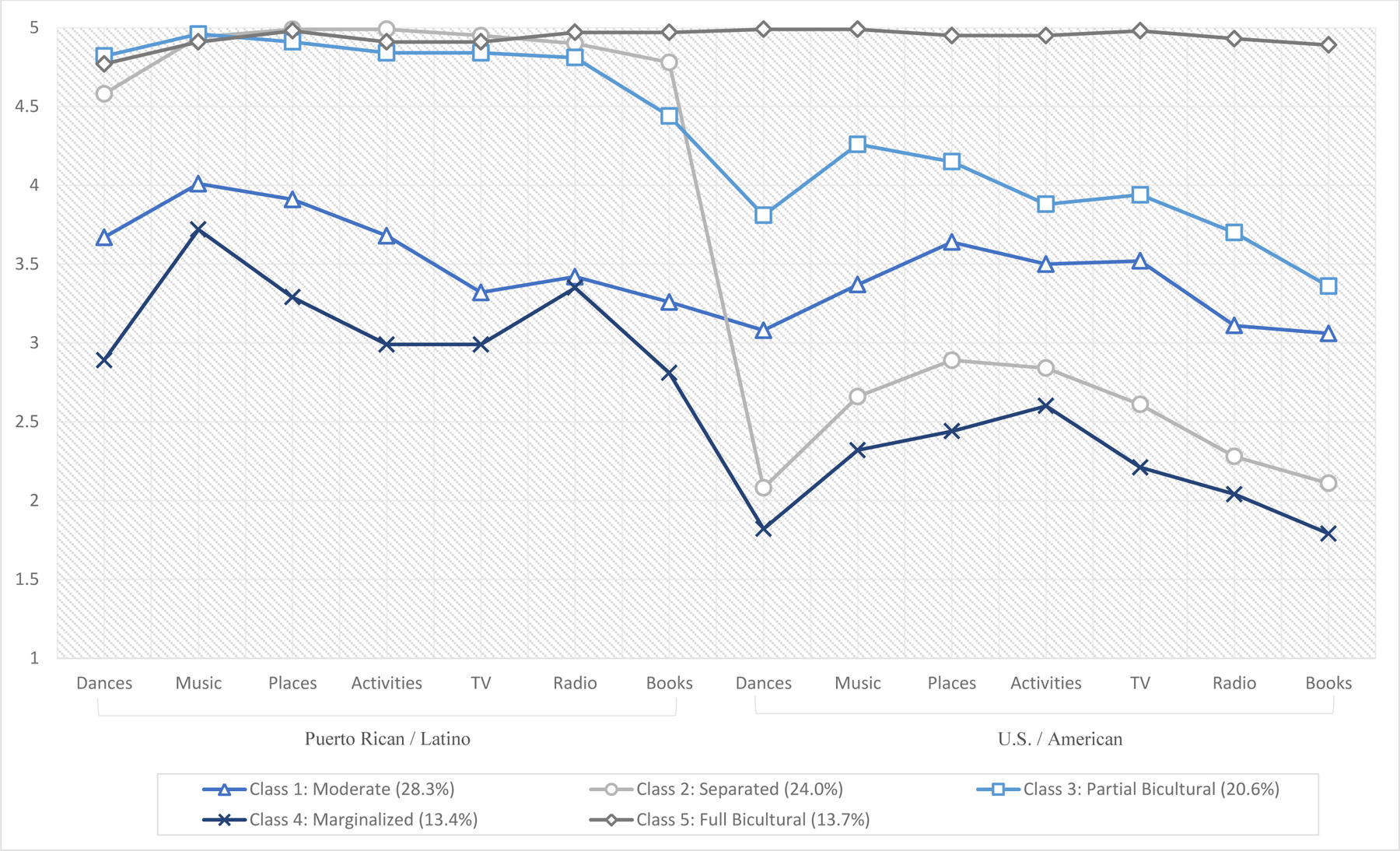
Characteristics of Latent Classes
Acknowledgements:
We would like to thank our community partners and Community Advisory Boards who have been essential to the development of the study.
Funding:
This work was supported by the National Institute on Minority Health and Health Disparities [NIMHD; Award Numbers R01MD014694] and the National Institute on Alcohol Abuse and Alcoholism [NIAAA; Award Number K01AA026645] of the National Institutes of Health. The content is solely the responsibility of the authors and does not necessarily represent the official views of NIMHD, NIAAA, or the NIH.
References
- Berry JW (1992). Acculturation and adaptation in a new society. International migration, 30, 69–69. [Google Scholar]
- Berry JW (2017). Theories and models of acculturation. In Schwartz SJ & Unger J (Eds.), The Oxford handbook of acculturation and health (pp.15–28). Oxford University Press. [Google Scholar]
- Cano MÁ, Schwartz SJ, Castillo LG, Romero AJ, Huang S, Lorenzo-Blanco EI, … & Szapocznik J. (2015). Depressive symptoms and externalizing behaviors among Hispanic immigrant adolescents: Examining longitudinal effects of cultural stress. Journal of adolescence, 42, 31–39. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cervantes RC, Padilla AM, & De Snyder NS (1990). Reliability and validity of the Hispanic Stress Inventory. Hispanic journal of behavioral sciences, 12(1), 76–82. [Google Scholar]
- Grzywacz JG, Hovey JD, Seligman LD, Arcury TA, & Quandt SA (2006). Evaluating short-form versions of the CES-D for measuring depressive symptoms among immigrants from Mexico. Hispanic Journal of Behavioral Sciences, 28(3), 404–424. [PMC free article] [PubMed] [Google Scholar]
- Choy B, Arunachalam K, Gupta S, Taylor M, & Lee A (2021). Systematic review: Acculturation strategies and their impact on the mental health of migrant populations. Public Health in Practice, 2, 100069. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Heckathorn DD (2002). Respondent-driven sampling II: deriving valid population estimates from chain-referral samples of hidden populations. Social problems, 49(1), 11–34. [Google Scholar]
- La Greca AM, Silverman WK, Vernberg EM, & Prinstein MJ (1996). Symptoms of posttraumatic stress in children after Hurricane Andrew: a prospective study. Journal of consulting and clinical psychology, 64(4), 712–723. [DOI] [PubMed] [Google Scholar]
- Long JS, & Freese J (2006). Regression models for categorical dependent variables using Stata (Vol. 7). Stata press. [Google Scholar]
- Lorenzo-Blanco EI, Meca A, Piña-Watson B, Zamboanga BL, Szapocznik J, Cano MÁ, … & Schwartz SJ (2019). Longitudinal trajectories of family functioning among recent immigrant adolescents and parents: Links with adolescent and parent cultural stress, emotional well-being, and behavioral health. Child development, 90(2), 506–523. [DOI] [PMC free article] [PubMed] [Google Scholar]
- McAdam J (2014). The concept of crisis migration. Forced migration review, 45. [Google Scholar]
- McLachlan GJ, Lee SX, & Rathnayake SI (2019). Finite mixture models. Annual review of statistics and its application, 6, 355–378. [Google Scholar]
- Meca A, Cobb C, Xie D, Schwartz SJ, Allen C, & Hunter R (2017). Exploring adaptive acculturation approaches among undocumented Latinos: A test of Berry’s model. The Counseling Psychologist, 45(8), 1115–1140. [Google Scholar]
- Montero-Zamora P, Salas-Wright CP, Maldonado-Molina MM, Brown EC, Vos SR, García MF, Scaramutti C, Rodríguez J, Bates M, & Schwartz SJ (in press). Trauma, cultural stress, and mental health among Hurricane Maria migrants in the U.S mainland. American Journal of Orthopsychiatry [DOI] [PubMed] [Google Scholar]
- Phinney JS, Madden T, & Santos LJ (1998). Psychological variables as predictors of perceived ethnic discrimination among minority and immigrant adolescents 1. Journal of Applied Social Psychology, 28(11), 937–953. [Google Scholar]
- Salas-Wright CP, Oh S, Vaughn MG, Pérez-Gómez A, Mejía-Trujillo J, Montero-Zamora P, … & Schwartz SJ (2021). A validation of the Perceived Negative Context of Reception Scale with recently-arrived Venezuelan immigrants in Colombia and the United States. Cultural Diversity and Ethnic Minority Psychology, 27(4), 649–658. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Salas-Wright CP, Maldonado-Molina MM, Pérez-Gómez A, Trujillo JM, & Schwartz SJ (2022). The Venezuelan diaspora: Migration-related experiences and mental health. Current Opinion in Psychology, 101430. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Salas-Wright CP, & Schwartz SJ (2019). The study and prevention of alcohol and other drug misuse among migrants: toward a transnational theory of cultural stress. International Journal of Mental Health and Addiction, 17(2), 346–369. [Google Scholar]
- Salas-Wright CP, Clark TT, Vaughn MG, & Córdova D (2015). Profiles of acculturation among Hispanics in the United States: Links with discrimination and substance use. Social psychiatry and psychiatric epidemiology, 50(1), 39–49. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Salas-Wright CP, Maldonado-Molina MM, Brown EC, Bates M, Rodríguez J, García MF, & Schwartz SJ (2021). Cultural stress theory in the context of family crisis migration: implications for behavioral health with illustrations from the Adelante Boricua study. American journal of criminal justice, 46(4), 586–608. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Scaramutti C, Salas-Wright CP, Vos SR, & Schwartz SJ (2019). The mental health impact of hurricane Maria on Puerto Ricans in Puerto Rico and Florida. Disaster medicine and public health preparedness, 13(1), 24–27. [DOI] [PubMed] [Google Scholar]
- Schwartz SJ, Unger JB, Lorenzo-Blanco EI, Des Rosiers SE, Villamar JA, Soto DW, … & Szapocznik J (2014). Perceived context of reception among recent Hispanic immigrants: conceptualization, instrument development, and preliminary validation. Cultural Diversity and Ethnic Minority Psychology, 20(1), 1–15. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Schwartz SJ, Montero-Zamora P, Salas-Wright CP, Brown EC, Garcia MF, Scaramutti C, … & Maldonado-Molina MM (2022). After Hurricane Maria: Effects of disaster trauma on Puerto Rican survivors on the US mainland. Psychological trauma: theory, research, practice, and policy. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Schwartz SJ, Salas-Wright CP, Perez-Gomez A, Mejia-Trujillo J, Brown EC, Montero-Zamora P, … & Dickson-Gomez J (2018). Cultural stress and psychological symptoms in recent Venezuelan immigrants to the United States and Colombia. International Journal of Intercultural Relations, 67, 25–34. [Google Scholar]
- Schwartz SJ, Unger JB, Zamboanga BL, & Szapocznik J (2010). Rethinking the concept of acculturation: implications for theory and research. American Psychologist, 65(4), 237. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Schwartz SJ, & Zamboanga BL (2008). Testing Berry’s model of acculturation: a confirmatory latent class approach. Cultural diversity and ethnic minority psychology, 14(4), 275. [DOI] [PubMed] [Google Scholar]
- Schwartz SJ, Zamboanga BL, Unger JB, Salas-Wright CP, Cobb CL, Maldonado-Molina MM, Cano MA, & Szapocznik J (2023). A program of research on culture, identity, and migration: Acculturation, cultural stress, and crisis migration. In Gelfand M, Chiu CY, & Hong HY (Eds.) Handbook of Advances in Culture and Psychology. New York, NY: Oxford University Press. [Google Scholar]
- Silver P (2020). Sunbelt Diaspora: Race, Class, and Latino Politics in Puerto Rican Orlando. University of Texas Press. [Google Scholar]
- Spitzer RL, Kroenke K, Williams JB, & Löwe B (2006). A brief measure for assessing generalized anxiety disorder: the GAD-7. Archives of internal medicine, 166(10), 1092–1097. [DOI] [PubMed] [Google Scholar]
- Szapocznik J, Kurtines WM, & Fernandez T (1980). Bicultural involvement and adjustment in Hispanic-American youths. International Journal of intercultural relations, 4(3–4), 353–365. [Google Scholar]
- Vargas SM, Huey SJ Jr, & Miranda J (2020). A critical review of current evidence on multiple types of discrimination and mental health. American Journal of Orthopsychiatry, 90(3), 374. [DOI] [PubMed] [Google Scholar]
- Vos SR, Clark-Ginsberg A, Puente-Duran S, Salas-Wright CP, Duque MC, Herrera IC, … & Schwartz SJ (2021). The family crisis migration stress framework: A framework to understand the mental health effects of crisis migration on children and families caused by disasters. New directions for child and adolescent development, 2021(176), 41–59. [DOI] [PubMed] [Google Scholar]
- Weller BE, Bowen NK, & Faubert SJ (2020). Latent class analysis: a guide to best practice. Journal of Black Psychology, 46(4), 287–311. [Google Scholar]
- Yu SC, Lin YH, & Hsu WH (2013). Applying structural equation modeling to report psychometric properties of Chinese version 10-item CES-D depression scale. Quality & Quantity, 47(3), 1511–1518. [Google Scholar]
- Zamboanga BL, Lui PP, & Pham S (2020). Acculturation, enculturation, and bicultural orientations: Conceptualizations and links to alcohol use. In Hall GC (Ed.), Mental and behavioral health of immigrants in the United States (pp. 45–69). Academic Press. [Google Scholar]