

Abstract
This study uses data from IQVIA’s National Prescription Audit to assess the association of the Inflation Reduction Act’s cap on cost sharing with insulin fills by Medicare beneficiaries.
Medicare beneficiaries’ out-of-pocket costs for insulin exceeded $1 billion in 2020 vs $236 million in 2007.1 High costs lead some patients with diabetes to reduce adherence to insulin, increasing the risk of adverse health outcomes.2,3,4
Although efforts to cap patients’ cost sharing for insulin have existed in some states since 2020, and in certain Medicare Part D plans since 2021, in January 2023 the Inflation Reduction Act5 capped cost sharing for insulin at $35 for a 1-month supply for all Part D beneficiaries and, therefore, may have a greater effect on adherence. This study measures the association of this cost-sharing cap with insulin fills.
Methods
We used data from IQVIA’s National Prescription Audit, which includes 92% of retail pharmacies and 70% of mail-order and long-term care facility pharmacies. Monthly prescription fills from September 2021 through April 2023 were included.
To determine the association between the Inflation Reduction Act and the number of insulin fills (primary outcome) and insulin fills with cost sharing of $35 or less (secondary outcome) for Medicare Part D beneficiaries, we adapted an established quasi-experimental difference-in-differences design.6 We compared changes in outcomes for Medicare enrollees aged 65 to 74 years with Part D insurance (affected by the cost-sharing cap) vs changes in people who were about to age into Medicare (aged 60-64 years without Part D insurance).
We compared outcomes before (September 2021-December 2022) and after (January 2023-April 2023) the cost-sharing cap went into effect. The difference-in-differences estimates were analyzed using negative binomial regression models with heteroscedasticity-robust SEs and adjustment for trends in insulin fills by year and calendar month. The plausibility of the parallel trends assumption was examined using data from September 2021 through December 2022. Additional details appear in the eMethods in Supplement 1.
The institutional review board at the University of Southern California approved this research. Stata version 16.1 (StataCorp) was used for all analyses. Two-sided hypothesis tests were conducted with P = .05 as the threshold for statistical significance.
Results
The study sample included 14 million insulin fills. Before 2023, trends in monthly insulin fills were similar among patients with Medicare Part D aged 65 to 74 years and patients without Medicare Part D aged 60 to 64 years (Figure). Between December 2021 and January 2022, there was a parallel decline in insulin fills in both groups. However, between December 2022 and January 2023, the group with Medicare Part D did not show this decrease.
Figure. Insulin Fills With and Without Medicare Part D From September 2021 Through April 2023.
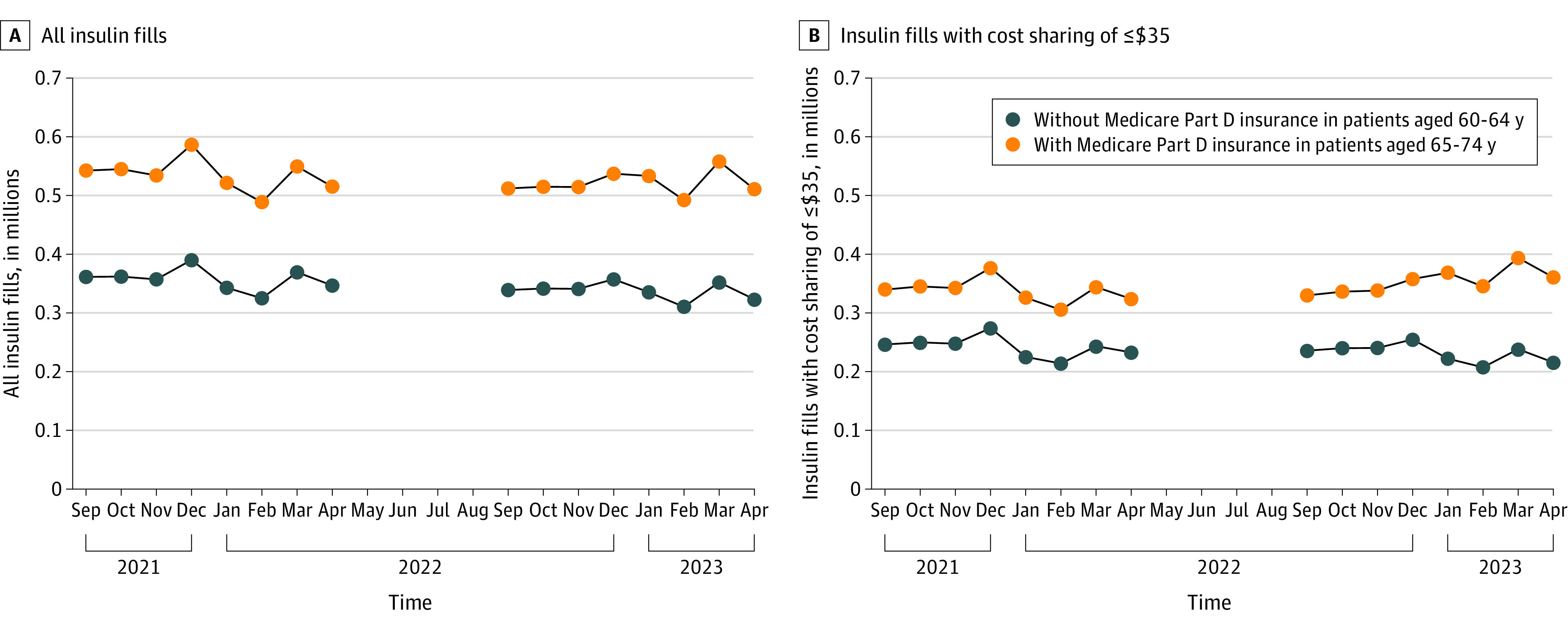
The data are from IQVIA’s National Prescription Audit on monthly prescription fills for insulin dispensed at retail and mail-order pharmacies in the US. Data from May through August 2022 are omitted to focus on the changes between the end of 1 calendar year and the beginning of the next calendar year.
The number of insulin fills among Medicare enrollees increased from 519 588 per month in September 2022 through December 2022 to 523 564 per month in January 2023 through April 2023 (Table). Over the same time frame, the number of insulin fills decreased among those without Medicare from 344 719 per month to 330 229 per month. In a regression analysis, the adjusted difference-in-differences estimate was 21 719 (95% CI, 20 797-22 641) fills per month (P < .001).
Table. Insulin Fills With and Without Medicare Part D Before and After the Cap on Cost Sharinga.
| Insulin fills, mean/mo | Beginning of 2023 vs end of 2022, mean difference | Regression analysisb | ||||
|---|---|---|---|---|---|---|
| Sep 2022-Dec 2022 | Jan 2023-Apr 2023 | Individual group | Between-group difference | Difference-in-differences estimate for fills/mo (95% CI) | P value | |
| All insulin fills | ||||||
| With Medicare Part D insurance in those aged 65-74 y | 519 588 | 523 564 | 3976 | 18 466 | 21 719 (20 797 to 22 641) | <.001 |
| Without Medicare Part D insurance in those aged 60-64 y | 344 719 | 330 229 | −14 490 | |||
| Insulin fills with cost sharing of ≤$35 | ||||||
| With Medicare Part D insurance in those aged 65-74 y | 340 509 | 366 928 | 26 419 | 48 285 | 49 515 (48 480 to 50 549) | <.001 |
| Without Medicare Part D insurance in those aged 60-64 y | 242 733 | 220 867 | −21 866 | |||
The data are from IQVIA’s National Prescription Audit and measure monthly prescription fills for insulin dispensed at retail and mail-order pharmacies in the US.
The data were adjusted for trends in insulin fills by year and calendar month.
The mean number of monthly fills with cost sharing of $35 or less increased from 340 509 in September 2022 through December 2022 to 366 928 in January 2023 through April 2023 for Medicare enrollees and decreased from 242 733 to 220 867 for those without Medicare (adjusted difference-in-differences estimate, 49 515 [95% CI, 48 480-50 549] fills per month; P < .001).
Discussion
The Inflation Reduction Act’s cap on cost sharing was associated with increases in the total number of insulin fills and insulin fills with cost sharing of $35 or less for Medicare enrollees aged 65 to 74 years compared with patients aged 60 to 64 years without Part D insurance. This analysis examined changes in insulin fills between the end of 1 calendar year and the beginning of the next, a time when deductibles reset and many patients must pay out of pocket for care. In contrast to the prior year, Medicare enrollees aged 65 to 74 years did not experience a decline in insulin fills between the end of 2022 and the beginning of 2023.
Limitations of this study include the short period for analysis after the passage of the Inflation Reduction Act, the lack of data on demographic characteristics, and the possibility for confounding by concurrent changes in other determinants of insulin use. These data reflect the additional change associated with the Inflation Reduction Act policy above and beyond the effects of preexisting policies. The long-term effects of the cost-sharing caps from the Inflation Reduction Act, how these effects vary across enrollees, and how other cost-sharing caps affect insulin fills are worthy of further study.
Section Editors: Jody W. Zylke, MD, Deputy Editor; Kristin Walter, MD, Senior Editor.
eMethods
Data sharing statement
References
- 1.Cubanski J, Damico A; KFF (formerly the Kaiser Family Foundation) . Insulin out-of-pocket costs in Medicare Part D. Published July 28, 2022. Accessed April 7, 2023. https://www.kff.org/medicare/issue-brief/insulin-out-of-pocket-costs-in-medicare-part-d/
- 2.Goldman DP, Joyce GF, Zheng Y. Prescription drug cost sharing: associations with medication and medical utilization and spending and health. JAMA. 2007;298(1):61-69. doi: 10.1001/jama.298.1.61 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Cefalu WT, Dawes DE, Gavlak G, et al. Insulin Access and Affordability Working Group: conclusions and recommendations. Diabetes Care. 2018;41(6):1299-1311. doi: 10.2337/dci18-0019 [DOI] [PubMed] [Google Scholar]
- 4.McAdam-Marx C, Ruiz-Negron N, Sullivan JM, Tucker JM. The effects of patient out-of-pocket costs on insulin use among people with type 1 and type 2 diabetes with Medicare Advantage insurance—2014-2018. Health Serv Res. 2023;290(6):1-8. doi: 10.1111/1475-6773.14152 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Inflation Reduction Act of 2022, HR 5376, 117th Congress. Accessed July 12, 2023. https://www.congress.gov/bill/117th-congress/house-bill/5376
- 6.McWilliams JM, Zaslavsky AM, Meara E, Ayanian JZ. Impact of Medicare coverage on basic clinical services for previously uninsured adults. JAMA. 2003;290(6):757-764. doi: 10.1001/jama.290.6.757 [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
eMethods
Data sharing statement