

Key Points
Question
Was political party affiliation a risk factor associated with excess mortality during the COVID-19 pandemic in Florida and Ohio?
Findings
In this cohort study evaluating 538 159 deaths in individuals aged 25 years and older in Florida and Ohio between March 2020 and December 2021, excess mortality was significantly higher for Republican voters than Democratic voters after COVID-19 vaccines were available to all adults, but not before. These differences were concentrated in counties with lower vaccination rates, and primarily noted in voters residing in Ohio.
Meaning
The differences in excess mortality by political party affiliation after COVID-19 vaccines were available to all adults suggest that differences in vaccination attitudes and reported uptake between Republican and Democratic voters may have been a factor in the severity and trajectory of the pandemic in the US.
Abstract
Importance
There is evidence that Republican-leaning counties have had higher COVID-19 death rates than Democratic-leaning counties and similar evidence of an association between political party affiliation and attitudes regarding COVID-19 vaccination; further data on these rates may be useful.
Objective
To assess political party affiliation and mortality rates for individuals during the initial 22 months of the COVID-19 pandemic.
Design, Setting, and Participants
A cross-sectional comparison of excess mortality between registered Republican and Democratic voters between March 2020 and December 2021 adjusted for age and state of voter registration was conducted. Voter and mortality data from Florida and Ohio in 2017 linked to mortality records for January 1, 2018, to December 31, 2021, were used in data analysis.
Exposures
Political party affiliation.
Main Outcomes and Measures
Excess weekly deaths during the COVID-19 pandemic adjusted for age, county, party affiliation, and seasonality.
Results
Between January 1, 2018, and December 31, 2021, there were 538 159 individuals in Ohio and Florida who died at age 25 years or older in the study sample. The median age at death was 78 years (IQR, 71-89 years). Overall, the excess death rate for Republican voters was 2.8 percentage points, or 15%, higher than the excess death rate for Democratic voters (95% prediction interval [PI], 1.6-3.7 percentage points). After May 1, 2021, when vaccines were available to all adults, the excess death rate gap between Republican and Democratic voters widened from −0.9 percentage point (95% PI, −2.5 to 0.3 percentage points) to 7.7 percentage points (95% PI, 6.0-9.3 percentage points) in the adjusted analysis; the excess death rate among Republican voters was 43% higher than the excess death rate among Democratic voters. The gap in excess death rates between Republican and Democratic voters was larger in counties with lower vaccination rates and was primarily noted in voters residing in Ohio.
Conclusions and Relevance
In this cross-sectional study, an association was observed between political party affiliation and excess deaths in Ohio and Florida after COVID-19 vaccines were available to all adults. These findings suggest that differences in vaccination attitudes and reported uptake between Republican and Democratic voters may have been factors in the severity and trajectory of the pandemic in the US.
This cross-sectional study examines the differences in excess death rates between Republican and Democratic voters in Florida and Ohio after the COVID-19 vaccine became available for all adults.
Introduction
As of May 2023, there had been approximately 1.1 million deaths from COVID-19 in the US.1 There is evidence that Republican-leaning counties have had higher COVID-19 death rates than Democratic-leaning counties and similar evidence of an association between political party affiliation and attitudes regarding COVID-19 vaccination, social distancing, and other mitigation strategies based on political party affiliation.2,3,4,5,6
Prior studies7,8 have found that Republican-leaning counties have had higher COVID-19 death rates than Democratic-leaning counties. It is unknown whether this county-level association persists at the individual level and whether it may be subject to the ecologic fallacy.9 The ecologic fallacy is the incorrect assumption that associations observed at an aggregated level (eg, a county) will be the same at the individual level. Republican-leaning and Democratic-leaning counties differ in ways other than political party affiliation,10,11 such as racial and ethnic composition, rurality, and educational levels, making it difficult to establish whether the differences in COVID-19 death rates are associated with political party affiliation or other differences in county-level characteristics. Research before the COVID-19 pandemic has also found evidence of higher death rates in Republican-leaning counties than Democratic-leaning counties.12
To assess the association between political party affiliation and excess mortality for individuals during the COVID-19 pandemic, we linked voter registration data in Florida and Ohio to mortality data at the individual level to calculate excess death rates for Republican and Democratic voters and compare excess death rates before and after vaccines became available to the full adult population.13,14 Because individual-level vaccination status was not included in the available data, we were able to assess excess death rates and vaccination rates only at the county level.
Methods
Data Source
The eMethods in Supplement 1 provides additional details of all the methods. We obtained detailed US weekly mortality data from January 1, 2018, to December 31, 2021, from Datavant, an organization that augments the Social Security Administration Death Master File with information from newspapers, funeral homes, and other sources to construct an individual-level database containing 10 325 730 deaths in the US to individuals aged 25 or older during this period. This data set, which includes deaths reported to Datavant through March 31, 2023, covers approximately 83.5% of the Centers for Disease Control and Prevention death count for individuals who died at age 25 or older during the period from January 1, 2018, to December 31, 2021. Because the Datavant mortality data do not contain state identifiers, we are unable to assess data completeness in our individual study states of Florida and Ohio. During the COVID-19 pandemic, Datavant mortality data have been used in other peer-reviewed15 and publicly available16 research on excess mortality. The Yale University Institutional Review Board exempted the study from review because the data were deidentified, and reporting adheres to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) reporting guideline.
We linked the mortality data at the individual level to 2017 Florida and Ohio voter registration files; these were the only states for which historical publicly available voter registration data were readily available. The linkage was performed from April 11 to 14, 2023. For each record, the linked data included week of death, age of deceased, county of residence, and 2017 political party affiliation. Political party affiliation in Ohio was defined by whether an individual voted in a party’s primary election within the preceding 2 calendar years; in Florida, political party affiliation was based on party registration. We excluded individuals whose political party affiliation was independent and those who were affiliated with third parties. Because COVID-19 deaths are most common at older ages,17 we included only death records for individuals who died at age 25 years or older.
We also obtained death counts for the study period from the National Center for Health Statistics18 and county-level vaccination rates from the Centers for Disease Control and Prevention.19 We selected May 1, 2021, as the date for the county-level vaccination rate—1 month after eligibility for vaccines opened to all adults in the study states—because it represented the approximate date when all adults would have had the opportunity to receive at least 1 dose of a COVID-19 vaccine if they so desired, taking into account the time that states required during April 2021 to schedule and administer vaccines to newly eligible adults seeking them. As a robustness check, we assessed the sensitivity of our findings to using county-level vaccination rates on alternative dates before (March 1, 2021) and after (October 1, 2021) May 1, 2021.
Statistical Analysis
We aggregated weekly death counts from January 1, 2018, to December 31, 2021, at the county-by-party-by-age level. The age ranges used were 25 to 64, 65 to 74, 75 to 84, and 85 years or older. The observed death counts included all the deaths from our mortality data that linked to Republican or Democratic voters who were registered in Florida and Ohio as of 2017.
To calculate the number of excess deaths, we estimated the number of deaths we would expect in the absence of the COVID-19 pandemic. First, we estimated expected weekly deaths at the county-by-party-by-age level by fitting a Poisson regression model to observed weekly death counts at the county-by-party-by-age-level for January 1, 2018, through December 31, 2019.20,21 We then predicted expected deaths over our full sample. Excess deaths were defined as the difference between observed and expected deaths for January 1, 2018, to December 31, 2021. As a check on the model, we used predictions from the model in the weeks before the onset of COVID-19 (January 1, 2018, to March 31, 2020) to estimate excess deaths during this period.
We calculated excess death rates (the primary outcome) as the ratio of observed deaths (the numerator) to expected deaths (the denominator). To obtain estimates of excess death rates at aggregated levels, we used a weighted average of estimated excess death rates in each of the underlying cells (eg, county-by-party-by-age), weighted by their expected death counts. We estimated Poisson 95% prediction intervals (PIs), simulating from the coefficient distribution and outcome distribution, with SEs clustered by county.22 We additionally adjusted estimated differences in excess death rates between Republican and Democratic voters—the primary estimate of interest—for differences in excess death rates by age group and state during the COVID-19 pandemic. Intuitively, this approach compared excess death rates between Democratic and Republican voters of the same age residing in the same states during the same week of the pandemic and then weighted those differences in excess death rates to either the weekly level, when plotting weekly differences in excess death rates, or to 3 broader time periods: (1) April 1, 2020, to December 31, 2021 (the part of the study period overlapping the COVID-19 pandemic); (2) April 1, 2020, to March 31, 2021 (the period during the pandemic before open vaccine eligibility for all adults); and (3) April 1, 2021, to December 31, 2021 (the period during the pandemic after open vaccine eligibility for all adults).
We also assessed county-level vaccination rates (as of May 1, 2021) and excess death rates by plotting average excess death rates for Republican and Democratic voters against the county-level vaccination rate during (1) the pre–COVID-19 pandemic period, (2) the period during the pandemic before open vaccine eligibility for all adults, and (3) the period during the pandemic after open vaccine eligibility for all adults.
In sensitivity analyses, we altered the Poisson model used to predict baseline death counts by including a linear time trend (and in one analysis allowing it to vary by state) and additional seasonality terms to capture higher frequency season-of-the-year trends.23 For transparency, we calculated differences in the excess death rates between Republican and Democratic voters with no adjustments (removing our state and age group adjustments) and, separately, with a model that included our primary adjustments (state and age group) and additional adjustments for county-by-age differences in excess death rates during the pandemic.
We performed all calculations using R, version 4.1.3 (R Foundation for Statistical Computing). Statistical analyses report 95% PIs using simulations from the coefficient distribution and outcome distribution, with SEs clustered by county. Significance testing was 2-sided, and a P < .05 was considered statistically significant.
Results
Our study included 538 159 deaths for individuals aged 25 years and older in Florida and Ohio between January 2018 and December 2021 linked to their 2017 voter data (eTable 1 in Supplement 1). The median age at death was 78 years (IQR, 71-89 years). The pattern of death counts in our linked data and in the National Center for Health Statistics data was similar (Figure 1).
Figure 1. County-Level Death Counts in Florida and Ohio in Linked Voter-Mortality Data vs Centers for Disease Control and Prevention (CDC) National Center for Health Statistics Data, 2018-2021.
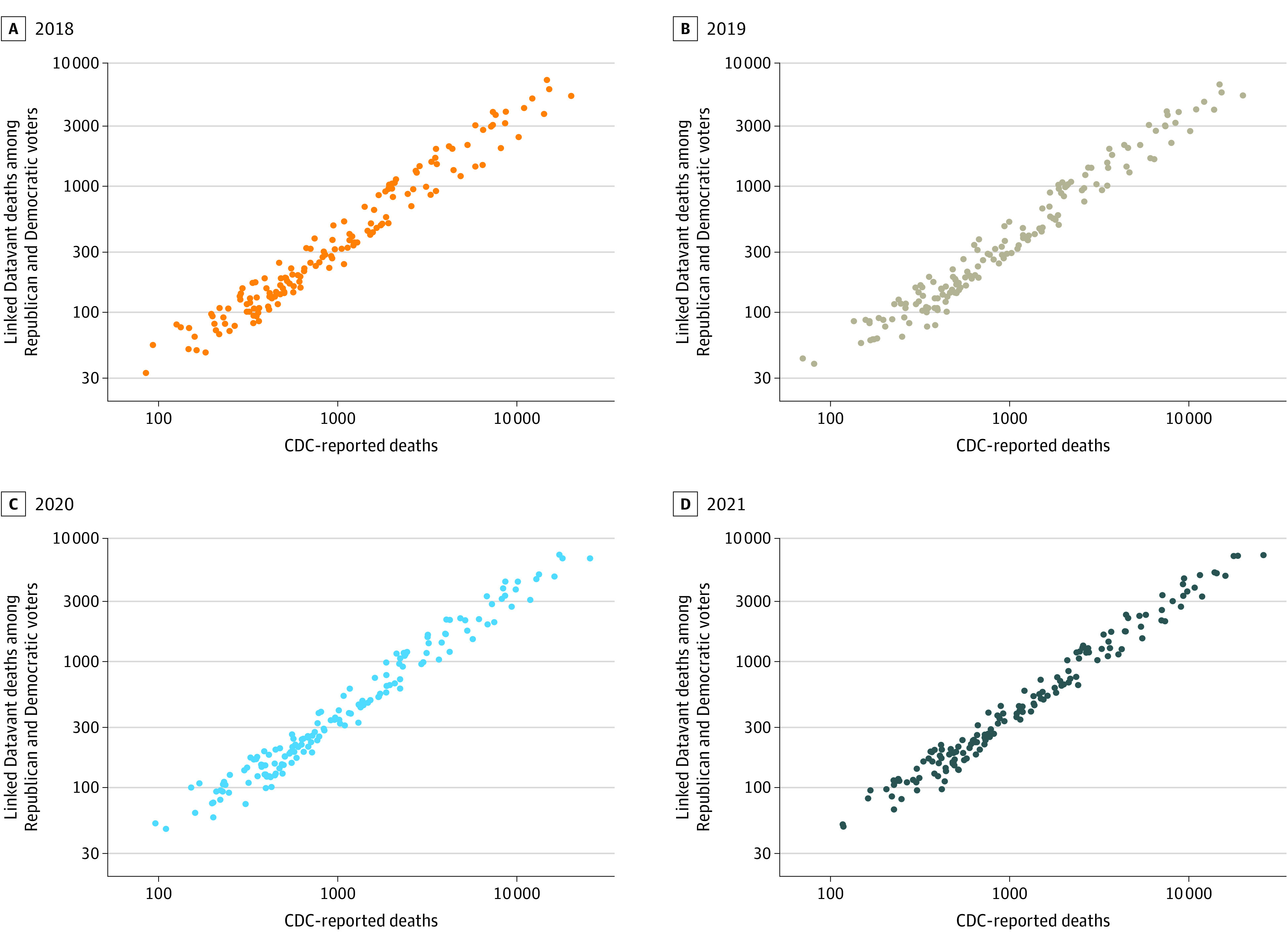
County-level death counts for Florida and Ohio based on Datavant data that link mortality records to voter registration files against the CDC data. Each observation represents a single county. Additional details on the data are provided in the eMethods in Supplement 1.
Using these data, we found a 20.5 percentage-point (95% PI, 15.6-25.6 percentage points) increase in weekly death counts in Florida and Ohio in the March 2020 to December 2021 period relative to the expected death counts for those weeks (Figure 2A and Table). By comparison, for the time periods before the pandemic, we found only small fluctuations in excess death rates around 0.
Figure 2. Excess Death Rates in Florida and Ohio, 2018-2021.

Weekly excess deaths for Florida and Ohio based on mortality records linked to voter registration files. A, Overall excess death rates in Florida and Ohio. B, Excess death rates by registered party. C, The percentage-point difference between the registered parties, after adjusting for age and state-level differences; the smooth brown curve was fit with locally estimated scatterplot smoothing. A-C, Excess death rates were calculated for each week by comparing the observed deaths in that week with expected deaths based on a Poisson model. The 95% prediction intervals (shaded areas) were determined using simulations from the Poisson coefficient and outcome distribution, with SEs clustered at the county level. Additional details on the excess death methods and statistical analyses are presented in the eMethods in Supplement 1.
Table. Heterogeneity in Excess Deaths in Florida and Ohio, 2020-2021a.
| Time | Overall death count in linked data, No. | % (95% CI) | |||
|---|---|---|---|---|---|
| Overall excess deaths | Republican excess deaths | Democrat excess deaths | Adjusted difference in excess deaths, percentage points | ||
| Early years of COVID-19 pandemicb | 258 470 | 20.5 (15.6 to 25.6) | 22.1 (15.6 to 29.3) | 18.5 (11.8 to 26.0) | 2.8 (1.6 to 3.7) |
| Before open vaccine eligibilityc | 146 691 | 19.1 (14.3 to 24.2) | 19.4 (13.0 to 26.4) | 18.8 (12.1 to 26.4) | −0.9 (−2.5 to 0.3) |
| After open vaccine eligibilityd | 111 779 | 22.3 (17.3 to 27.6) | 25.8 (19.0 to 33.2) | 18.1 (11.3 to 25.6) | 7.7 (6.0 to 9.3) |
Linked death counts do not match overall death counts during this period because not all US residents are registered to vote, and the mortality data set included approximately 83.5% of deaths in the US. Excess death rates were calculated by comparing observed deaths in a particular week to expected deaths based on a regression model. Additional details on the excess death methods and statistical analyses are provided in the eMethods in Supplement 1.
From March 13, 2020, to December 31, 2021.
From March 13, 2020, to March 31, 2021.
From April 1, 2021, to December 31, 2021.
Before the pandemic, excess death rates for Republican and Democratic voters were centered around 0 (Figure 2B). In the winter of 2021, both groups experienced sharp increases of similar magnitude in excess death rates. However, in the summer of 2021, after vaccines were available to all adults, the excess death rate among Republican voters began to increase relative to the excess death rate among Democratic voters; in the fall of 2021, the gap widened further. Between March 2020 and December 2021, excess death rates were 2.8 percentage points (15%) higher for Republican voters compared with Democratic voters (95% PI, 1.6-3.7 percentage points) (Table). After April 1, 2021, when all adults were eligible for vaccines in Florida and Ohio, this gap widened from −0.9 percentage point (95% PI, −2.5 to 0.3 percentage points) between March 2020 and March 2021, to 7.7 percentage points (95% PI, 6.0-9.3 percentage points) in the adjusted analysis, or a 43% difference (Table).
The estimates of differences in excess death rates between Republican and Democratic voters (adjusted for age, time, and state) were small until the summer of 2021, when excess death rates among Republican voters began to increase compared with excess death rates among Democratic voters (Figure 2C). The analyses stratified by age showed that Republican voters had significantly higher excess death rates compared with Democratic voters for 2 of the 4 age groups in the study, the differences for the age group 25 to 64 years were not significant (Figure 3; eFigure 1 in Supplement 1). Democratic voters had significantly higher excess death rates compared with Republican voters for the age group 65 to 74 years. The analyses stratified by state showed that differences in excess death rates between Republican and Democratic voters were primarily seen in voters residing in Ohio, with smaller, and generally nonsignificant, differences in weekly excess death rates between Republican and Democratic voters in Florida (eFigure 2 and eFigure 3 in Supplement 1). In analyses that pooled data from March 2020 to December 2021, Republican voters in Florida did not have a statistically significantly higher excess death rate than Democratic voters in Florida (Figure 3). Additional sensitivity analyses supported our main conclusions (eTable 2 in Supplement 1).
Figure 3. Differences in Excess Death Rates for Registered Republican and Democratic Voters in Florida and Ohio During the COVID-19 Pandemic.

The analyses were additionally adjusted for age and state-level differences in subgroup analyses where these covariates were not used for stratification. The 95% prediction intervals (horizontal lines) were determined using simulations from the Poisson coefficient and outcome distribution, with SEs clustered at the county level. Additional details on the excess death methodology and statistical analyses are presented in the eMethods in Supplement 1.
Before the COVID-19 pandemic, there was no association between county-level excess death rates, which hovered around 0, and the county-level vaccination rates (Figure 4A). During the pandemic, there was generally a negative association between county-level excess death rates and the share of the county population administered at least 1 dose of the vaccine as of May 1, 2021 (Figure 4B and C). In the period before open vaccine eligibility for adults (April 2020 to March 2021), the association between excess death rates and county-level vaccination rates was nearly identical for Republican and Democratic voters (Figure 4B). In the period after open vaccine eligibility (April to December 2021), there was a clear difference between Republican and Democratic voters, with higher excess death rates for Republicans in counties with lower overall vaccination rates (Figure 4C). Sensitivity analyses supported our main conclusions (eFigure 4 and eFigure 5 in Supplement 1).
Figure 4. Excess Death Rates and Vaccination Rates in Florida and Ohio During the COVID-19 Pandemic.
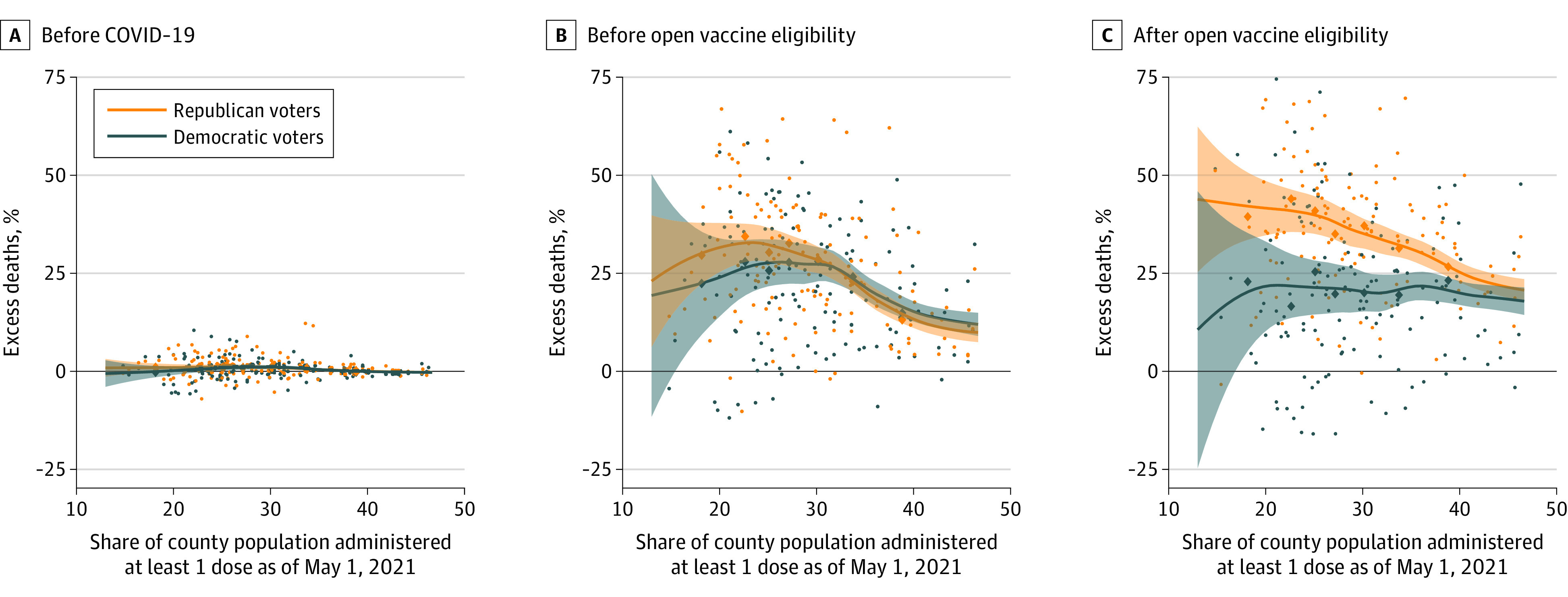
The diamonds are binned means; counties with similar vaccination rates were binned to form 8 equally sized bins. The curves were fit to the underlying data using locally estimated scatterplot smoothing. In the pre–COVID-19 period (before April 2020), excess death rates for both Republican and Democratic voters hover around 0. During the beginning pandemic but before open vaccine eligibility (April 2020 to March 2021), the association between excess death rates and county-level vaccination rates were generally negative and nearly identical for Republican and Democratic voters. However, in the period after open vaccine eligibility (April 2021 to December 2021), there was a clear difference between Republican and Democratic voters, with higher excess death rates for Republicans concentrated in counties with lower overall vaccination rates and minimal differences in counties with the highest vaccination rates.
Discussion
During the initial years of the COVID-19 pandemic, political party affiliation in the US was associated with excess death rates in Florida and Ohio at the individual level. Republican voters had higher excess death rates than Democratic voters, as noted in a large mortality gap in the period after, but not before, all adults were eligible for vaccines in Florida and Ohio. With adjustments for differences in age and state of residence between Republican and Democratic voters, our findings suggest that, among individuals in the same age groups living in the same states, there were significant differences in excess death rates during the COVID-19 pandemic associated with political party affiliation. The results were robust to alterations in the methods used to estimate excess mortality as well as the statistical model used to estimate the difference in excess death rates between Republican and Democratic voters.
Our findings suggest that political party affiliation became a substantial factor only after COVID-19 vaccines were available to all adults in the US. Although the lack of individual-level vaccination status limited our ability to note further associations, the results suggest that well-documented differences in vaccination attitudes and reported uptake between Republican and Democratic voters24,25 may have been factors in the severity and trajectory of the pandemic. However, one alternative explanation is that political party affiliation is a proxy for other risk factors (beyond age, which we adjusted for) for excess mortality during the COVID-19 pandemic, such as rates of underlying medical conditions, race and ethnicity, socioeconomic status, or health insurance coverage,26,27,28,29 and these risk factors may be associated with differences in excess mortality by political party, even though we only observed differences in excess mortality after vaccines were available to all adults. It is also possible that specific risk factors for excess mortality interact with the emergence of COVID-19 variants (eg, Delta) or changes in vaccine-associated protection over time to be more consequential at different stages of the pandemic. Because data limitations prevented us from directly adjusting for these factors, their potential influence remains an important question for future research.
In addition to vaccines, nonpharmaceutical interventions, including facial masks and restrictions on large gatherings, have been reported to contribute to reductions in transmission of COVID-19 or its severe outcomes, including death, in experimental, quasi-experimental, and modeling studies.30,31,32,33 However, differences in support for these measures by political party affiliation emerged early in the pandemic,34 and the gradual loosening of the strictest government policies regarding the use of facial masks and restrictions on large gatherings predated April 2021, when vaccines became available to all adults in the study states. The extent of public adherence to these and other interventions at various stages of the pandemic, associations between individual political party affiliation and the adoption over time of these interventions in specific geographic areas, and their relative contribution to trends in individual and community COVID-19 mortality over time are also worthwhile areas for further investigation.
Since the fall of 2022, the focus of the US COVID-19 vaccination program has turned to the administration of updated, bivalent booster doses to those who have already received a primary vaccine series and, in many cases, 1 or more prior booster dose. Federal health officials have also begun considering future strategies for COVID-19 vaccination, including annual revaccination campaigns using vaccines reformulated to match circulating variants.35 Yet more than 2 years into the vaccination effort, more than 50 million adults in the US have not completed a primary series, and these individuals remain at a substantially increased risk of hospitalization and death.36 The causes of this vaccine hesitancy and refusal are varied and extend beyond political beliefs or party affiliation alone.37 It therefore remains imperative for public health officials to continue and enhance activities intended to improve initial vaccination coverage, in tandem with current or future booster campaigns. To be most effective, these efforts—and corresponding messages—should be tailored to their intended audiences, address the particular sources of vaccine hesitancy among those groups, and seek to include direct participation from members of those communities as trusted ambassadors of provaccine messages.38 As part of this work, engagement with conservative and Republican leaders, in particular, has been identified as a promising approach to promoting COVID-19 vaccine acceptance.38
Limitations
Our study has several limitations. First, there are plausible alternative explanations for the difference in excess death rates by political party affiliation beyond the explanatory role of vaccines discussed herein. Second, our mortality data, although detailed and recent, only included approximately 83.5% of deaths in the US and did not include cause of death. Although overall excess death patterns in our data are similar to those in other reliable sources, such as the Centers for Disease Control and Prevention National Center for Health Statistics data, it is possible that the deaths that our study data did not include may disproportionately occur among individuals registered with a particular political party, potentially biasing our results. In addition, the completeness of our mortality data may vary across states or time, potentially biasing our estimates of excess death rates. Third, all excess death models rely on fundamentally untestable assumptions to construct the baseline number of deaths we would expect in the absence of the COVID-19 pandemic. Fourth, because we did not have information on individual vaccination status, analyses of the association between vaccination rates and excess deaths relied on county-level vaccination rates. Fifth, our study was based on data from 2 states with readily obtainable historical voter registration information (Florida and Ohio); hence, our results may not generalize to other states.
Conclusions
Our study found evidence of higher excess mortality for Republican voters compared with Democratic voters in Florida and Ohio after, but not before, COVID-19 vaccines were available to all adults in the US. These differences in excess death rates were larger in counties with lower vaccination rates. If differences in COVID-19 vaccination by political party affiliation persist, particularly in the absence of other pandemic mitigation strategies, the higher excess death rate observed among Republican voters may continue through subsequent stages of the pandemic.
eMethods. Supplemental Description of Methods
eFigure 1. Excess Death Rates by Age in Florida and Ohio: 2018-2021
eFigure 2. Excess Death Rates in Florida: 2018-2021
eFigure 3. Excess Death Rates in Ohio: 2018-2021
eFigure 4. Excess Death Rates and Vaccination Rates in Florida and Ohio During the COVID-19 Pandemic Using October 1, 2021, Vaccination Rates
eFigure 5. Excess Death Rates and Vaccination Rates in Florida and Ohio During the COVID-19 Pandemic Using March 1, 2021, Vaccination Rates
eTable 1. Summary Statistics
eTable 2. Sensitivity of Estimated Difference in Excess Death Rates Between Republican and Democratic Voters to Alterations in Excess Death Methodology and Statistical Model
Data Sharing Statement
References
- 1.National Center for Health Statistics . Provisional death counts for coronavirus disease 2019. (COVID-19). COVID-19 mortality overview. 2023. Accessed May 24, 2023. https://www.cdc.gov/nchs/covid19/mortality-overview.htm
- 2.Allcott H, Boxell L, Conway J, Gentzkow M, Thaler M, Yang D. Polarization and public health: partisan differences in social distancing during the coronavirus pandemic. J Public Econ. 2020;191:104254. doi: 10.1016/j.jpubeco.2020.104254 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Grossman G, Kim S, Rexer JM, Thirumurthy H. Political partisanship influences behavioral responses to governors’ recommendations for COVID-19 prevention in the United States. Proc Natl Acad Sci U S A. 2020;117(39):24144-24153. doi: 10.1073/pnas.2007835117 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Callaghan T, Moghtaderi A, Lueck JA, et al. Correlates and disparities of intention to vaccinate against COVID-19. Soc Sci Med. 2021;272:113638. doi: 10.1016/j.socscimed.2020.113638 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Cowan SK, Mark N, Reich JA. COVID-19 vaccine hesitancy is the new terrain for political division among Americans. Socius. Published online June 17, 2021. doi: 10.1177/23780231211023657 [DOI] [Google Scholar]
- 6.Pink SL, Chu J, Druckman JN, Rand DG, Willer R. Elite party cues increase vaccination intentions among Republicans. Proc Natl Acad Sci U S A. 2021;118(32):e2106559118. doi: 10.1073/pnas.2106559118 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Leonhardt D. The partisan gap in US Covid deaths is still growing, but more slowly. New York Times. February 18, 2022. Accessed March 1, 2023. https://www.nytimes.com/2022/02/18/briefing/the-morning-the-partisan-gap-in-us-covid-deaths-is-still-growing-but-more-slowly.html
- 8.Sehgal NJ, Yue D, Pope E, Wang RH, Roby DH. The association between COVID-19 mortality and the county-level partisan divide in the United States: study examines the association between COVID-19 mortality and county-level political party affiliation. Health Aff (Millwood). 2022;41(6):853-863. doi: 10.1377/hlthaff.2022.00085 [DOI] [Google Scholar]
- 9.Piantadosi S, Byar DP, Green SB. The ecological fallacy. Am J Epidemiol. 1988;127(5):893-904. doi: 10.1093/oxfordjournals.aje.a114892 [DOI] [PubMed] [Google Scholar]
- 10.Morrill R, Knopp L, Brown M. Anomalies in red and blue: exceptionalism in American electoral geography. Polit Geogr. 2007;26(5):525-553. doi: 10.1016/j.polgeo.2007.03.006 [DOI] [Google Scholar]
- 11.Scala DJ, Johnson KM. Political polarization along the rural-urban continuum? the geography of the presidential vote, 2000–2016. Ann Am Acad Pol Soc Sci. 2017;672(1):162-184. doi: 10.1177/0002716217712696 [DOI] [Google Scholar]
- 12.Warraich HJ, Kumar P, Nasir K, Joynt Maddox KE, Wadhera RK. Political environment and mortality rates in the United States, 2001-19: population based cross sectional analysis. BMJ. 2022;377:e069308. doi: 10.1136/bmj-2021-069308 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Wallace J, Goldsmith-Pinkham P, Schwartz JL. Excess death rates for Republicans and Democrats during the COVID-19 pandemic. NBER Work Pap Ser. 2022;30512:1-11. doi: 10.3386/w30512 [DOI] [Google Scholar]
- 14.Wallace J, Goldsmith-Pinkham P, Schwartz JL. Excess death rates for Republicans and Democrats during the COVID-19 pandemic. arXiv. Preprint published online 2022. doi: 10.3386/w30512 [DOI]
- 15.Wallace J, Lollo A, Ndumele CD. Evaluation of the association between Medicare eligibility and excess deaths during the COVID-19 pandemic in the US. JAMA Health Forum. 2021;2(9):e212861. doi: 10.1001/jamahealthforum.2021.2861 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Ziedan E, Simon KI, Wing C. Mortality effects of healthcare supply shocks: evidence using linked deaths and electronic health records. NBER Working Paper Series. October 2022. Accessed March 24, 2023. https://www.nber.org/system/files/working_papers/w30553/w30553.pdf
- 17.Truman BI, Chang M-H, Moonesinghe R. Provisional COVID-19 age-adjusted death rates, by race and ethnicity—United States, 2020-2021. MMWR Morb Mortal Wkly Rep. 2022;71(17):601-605. doi: 10.15585/mmwr.mm7117e2 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.National Center for Health Statistics; Weekly Counts of Deaths by Jurisdiction and Age Group . Updated June 1, 2022. Accessed June 8, 2022. https://data.cdc.gov/NCHS/Weekly-counts-of-deaths-by-jurisdiction-and-age-gr/y5bj-9g5w/
- 19.Centers for Disease Control and Prevention . COVID-19 vaccinations in the United States, county. March 24, 2023. Accessed June 23, 2022. https://data.cdc.gov/Vaccinations/COVID-19-Vaccinations-in-the-United-States-County/8xkx-amqh
- 20.Weinberger DM, Chen J, Cohen T, et al. Estimation of excess deaths associated with the COVID-19 pandemic in the United States, March to May 2020. JAMA Intern Med. 2020;180(10):1336-1344. doi: 10.1001/jamainternmed.2020.3391 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Woolf SH, Chapman DA, Sabo RT, Weinberger DM, Hill L, Taylor DDH. Excess deaths from COVID-19 and other Causes, March-July 2020. JAMA. 2020;324(15):1562-1564. doi: 10.1001/jama.2020.19545 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Lauer SA, Sakrejda K, Ray EL, et al. Prospective forecasts of annual dengue hemorrhagic fever incidence in Thailand, 2010-2014. Proc Natl Acad Sci U S A. 2018;115(10):E2175-E2182. doi: 10.1073/pnas.1714457115 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Islam N, Shkolnikov VM, Acosta RJ, et al. Excess deaths associated with covid-19 pandemic in 2020: age and sex disaggregated time series analysis in 29 high income countries. BMJ. 2021;373:n1137. doi: 10.1136/bmj.n1137 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Funk C, Gramlich J. 10 Facts about Americans and coronavirus vaccines. Pew Research Center. Published online September 20, 2021. Accessed March 24, 2023. https://www.pewresearch.org/fact-tank/2021/09/20/10-facts-about-americans-and-coronavirus-vaccines/
- 25.Kates J, Tolbert J, Rouw A. The red/blue divide in COVID-19 vaccination rates continues: an update. Kaiser Family Foundation. January 19, 2022. Accessed March 24, 2023. https://www.kff.org/policy-watch/the-red-blue-divide-in-covid-19-vaccination-rates-continues-an-update/
- 26.Stokes AC, Lundberg DJ, Elo IT, Hempstead K, Bor J, Preston SH. COVID-19 and excess mortality in the United States: a county-level analysis. PLoS Med. 2021;18(5):e1003571. doi: 10.1371/journal.pmed.1003571 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Chang D, Chang X, He Y, Tan KJK. The determinants of COVID-19 morbidity and mortality across countries. Sci Rep. 2022;12(1):5888. doi: 10.1038/s41598-022-09783-9 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Chen JT, Krieger N. Revealing the unequal burden of COVID-19 by income, race/ethnicity, and household crowding: US county versus zip code analyses. J Public Health Manag Pract. 2021;27(1)(suppl 1, COVID-19 and Public Health: Looking Back, Moving Forward):S43-S56. doi: 10.1097/PHH.0000000000001263 [DOI] [PubMed] [Google Scholar]
- 29.The White House Council of Economic Advisers . Excess mortality during the pandemic: the role of health insurance. July 12, 2022. Accessed March 24, 2023. https://www.whitehouse.gov/cea/written-materials/2022/07/12/excess-mortality-during-the-pandemic-the-role-of-health-insurance/
- 30.Abaluck J, Kwong LH, Styczynski A, et al. Impact of community masking on COVID-19: a cluster-randomized trial in Bangladesh. Science. 2022;375(6577):eabi9069. doi: 10.1126/science.abi9069 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Singh S, Shaikh M, Hauck K, Miraldo M. Impacts of introducing and lifting nonpharmaceutical interventions on COVID-19 daily growth rate and compliance in the United States. Proc Natl Acad Sci U S A. 2021;118(12):e2021359118. doi: 10.1073/pnas.2021359118 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Courtemanche C, Garuccio J, Le A, Pinkston J, Yelowitz A. Strong social distancing measures in the United States reduced the COVID-19 growth rate: study evaluates the impact of social distancing measures on the growth rate of confirmed COVID-19 cases across the United States. Health Aff (Millwood). 2020;39(7):1237-1246. doi: 10.1377/hlthaff.2020.00608 [DOI] [PubMed] [Google Scholar]
- 33.Brauner JM, Mindermann S, Sharma M, et al. Inferring the effectiveness of government interventions against COVID-19. Science. 2021;371(6531):eabd9338. doi: 10.1126/science.abd9338 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Pew Research Center . Republicans, Democrats move even further apart in coronavirus concerns. June 25, 2020. Accessed March 24, 2023. https://www.pewresearch.org/politics/2020/06/25/republicans-democrats-move-even-further-apart-in-coronavirus-concerns/
- 35.US Food and Drug Administration . Future vaccination regimens addressing COVID-19. December 16, 2022. Accessed March 24, 2023. https://www.fda.gov/news-events/press-announcements/coronavirus-covid-19-update-fda-hold-advisory-committee-meeting-discuss-future-vaccination-regimens
- 36.Centers for Disease Control and Prevention . COVID data tracker. 2023. Accessed November 7, 2022. https://covid.cdc.gov/covid-data-tracker
- 37.King WC, Rubinstein M, Reinhart A, Mejia R. Time trends, factors associated with, and reasons for COVID-19 vaccine hesitancy: a massive online survey of US adults from January-May 2021. PLoS One. 2021;16(12):e0260731. doi: 10.1371/journal.pone.0260731 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Omer SB, Benjamin RM, Brewer NT, et al. Promoting COVID-19 vaccine acceptance: recommendations from the Lancet Commission on Vaccine Refusal, Acceptance, and Demand in the USA. Lancet. 2021;398(10317):2186-2192. doi: 10.1016/S0140-6736(21)02507-1 [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
eMethods. Supplemental Description of Methods
eFigure 1. Excess Death Rates by Age in Florida and Ohio: 2018-2021
eFigure 2. Excess Death Rates in Florida: 2018-2021
eFigure 3. Excess Death Rates in Ohio: 2018-2021
eFigure 4. Excess Death Rates and Vaccination Rates in Florida and Ohio During the COVID-19 Pandemic Using October 1, 2021, Vaccination Rates
eFigure 5. Excess Death Rates and Vaccination Rates in Florida and Ohio During the COVID-19 Pandemic Using March 1, 2021, Vaccination Rates
eTable 1. Summary Statistics
eTable 2. Sensitivity of Estimated Difference in Excess Death Rates Between Republican and Democratic Voters to Alterations in Excess Death Methodology and Statistical Model
Data Sharing Statement