

Abstract
Introduction
Medical education and medical education research are growing industries that have become increasingly globalised. Recognition of the colonial foundations of medical education has led to a growing focus on issues of equity, absence and marginalisation. One area of absence that has been underexplored is that of published voices from low-income and middle-income countries. We undertook a bibliometric analysis of five top medical education journals to determine which countries were absent and which countries were represented in prestigious first and last authorship positions.
Methods
Web of Science was searched for all articles and reviews published between 2012 and 2021 within Academic Medicine, Medical Education, Advances in Health Sciences Education, Medical Teacher, and BMC Medical Education. Country of origin was identified for first and last author of each publication, and the number of publications originating from each country was counted.
Results
Our analysis revealed a dominance of first and last authors from five countries: USA, Canada, UK, Netherlands and Australia. Authors from these five countries had first or last authored 70% of publications. Of the 195 countries in the world, 43% (approximately 83) were not represented by a single publication. There was an increase in the percentage of publications from outside of these five countries from 23% in 2012 to 40% in 2021.
Conclusion
The dominance of wealthy nations within spaces that claim to be international is a finding that requires attention. We draw on analogies from modern Olympic sport and our own collaborative research process to show how academic publishing continues to be a colonised space that advantages those from wealthy and English-speaking countries.
Keywords: Health services research, Health systems
WHAT IS ALREADY KNOWN ON THIS TOPIC.
Authors from a small number of high-income countries (HICs) are over-represented in published journal articles on medical education.
WHAT THIS STUDY ADDS
This study shows that almost three-quarters of first and last authorship positions in several prominent medical education journals are held by authors from only five countries: USA, Canada, UK, Netherlands, Australia.
Authors from low-income and middle-income countries (LMICs), and from countries where English is not the dominant language, are under-represented in prestigious first and last authorship positions within the medical education literature.
As a field that claims to be international in scope, perspectives from outside of these five dominant countries are under-represented, limiting the breadth of views that make up the field of medical education.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
This study provides support for academics, academic institutions and academic publishers in establishing policies that prioritise the inclusion of authors from LMICs and from countries in which English is not the dominant language.
Explicitly including descriptions of the ways research teams address potential power imbalances in research studies that involve collaboration between HIC and LMIC authors, as well as fluent English and less-fluent English speakers in English language publications may allow further development of more inclusive models of international research collaboration.
Introduction
The global need for well-educated doctors, and other health professionals, who are able to provide high-quality healthcare, is undisputed, given the many health challenges societies face in the 21st century. Scaling up of health professions education opportunities has been proposed as one means of generating an educated workforce for addressing health system needs and has been a priority of the WHO since the 1950s.1 2 With global recognition of significant health worker shortages,3–6 this focus on increasing health worker output is necessary and unsurprising, leading to the creation of many new education programmes worldwide.
Rizwan et al 5 recently mapped trends in the globalisation of medical education programmes: USA, India, Pakistan, China and Brazil currently house the largest number of medical schools.7 While medical education programmes in LMIC and transitional countries8 are being established to improve health human resources within home countries, they are also drawing foreign students, both from countries lacking education opportunities and from countries where student selection is highly competitive.5 Countries in Eastern Europe (such as Poland, Hungary and the Czech Republic), Russia, Ukraine and China have increasingly established English language medical education programmes to attract international students.5 Similarly, in an attempt to attract learners from Canada and the USA, medical education programmes with curricula that emulate the American model have expanded within the Caribbean.6 As a global phenomenon, educating doctors is a growth industry.
Medical education is generally conceptualised as an academic endeavour, best achieved through well-planned delivery of science-informed education practices, tools, structures and processes.9 To support this, research in medical and health professions education has become an area of increasing scholarly attention. This has led to a proliferation of academic activity, including publications, international conference attendance and increasing diversity of professions, perspectives, disciplines and theoretical approaches being recognised as advancing new knowledge in the field.10 In examining the burgeoning literature, it is important to recognise that medical education research is, by academic measures, a relatively recent area of scholarship. It first emerged as an academic field in the 1950s in North America at a time when there was an explosion of scientific medical knowledge, an influx of financial incentives to support research, and a mandate to demonstrate greater public accountability.11 As an area of inquiry, its development was firmly entrenched in EuroAmerican healthcare and higher education structures. The colonial underpinnings of these structures are well documented, including ways that notions of academic legitimacy are based in biomedicine (which ignore traditional and Indigenous healing practices which developed in many different global contexts over millennia12) and are inextricably intertwined with European colonisation of parts of Africa, the Americas and Asia.12–17 In North America and Europe, Flexner’s report in 1910 had enormous impact, entrenching legitimacy of doctor education in high status university settings, which led to the closing of non-university-based programmes including most that provided training for women and black students.18–21
Recognising the colonial and Flexnerian foundations of medical education provides a helpful starting point for examining issues of equity, absence and marginalisation of diverse perspectives within current structures.22 In recent years, explorations of representation, discrimination, harassment, silencing and power differentials have begun to appear in medical education journals. Many are written as commentaries and perspectives pieces, providing reflections on personal experiences and theoretical explorations of ways that dominant approaches (generally white and EuroAmerican centric) constrain and limit the field.23–31 There are some empirical studies examining various aspects of representation within medical education, with recent attention given to gender, sociocultural and racial equity within academic medicine’s leadership, student body and curricula.32–47 There is also growing documentation of the paucity of published voices from low-income and middle-income countries (LMICs) and non-English speaking scholars in medical education journals that position their reach as international.48–52 This parallels the relative absence of authors from LMIC and non-English speaking countries in leading academic journals in many other areas of academia, including health and education.26 53–61
Within medicine, the use of bibliometric methodologies emerged during the late 1700s and early 1800s, but rose exponentially through the 1990s and remained high until 2015 when a moderate decline ensued.62 Bibliometric analyses are one way to identify imbalances, and a growing set of papers are exploring the under-representation of authors from outside of North America and Europe through the application of bibliometrics.56 57 63 64 Maggio et al 64 specifically examined authorship of knowledge syntheses by country, with authors from highly ranked North American institutions being dominant. By categorising lead authors by UN region,65 Buffone et al 56 found that the majority of authors in the medical education literature were from North America, Northern Europe, Western Europe or Australia. Thomas57 analysed authorship by country of affiliation over a 2-year period, comparing medical education journals to those in education, medicine and biomedical sciences. Examining for all authorship positions, he found that there was greater dominance of authors from the USA, the UK, Canada and Australia in medical education than in other areas. While these studies show that there is an overall dominance of authors from high-income English-speaking countries, there has not yet been a quantification of prestigious authorship positions by country.
In medical education research, first and last author positions are often considered more prestigious and desirable. For many researchers, numbers of first and last authored publications contribute to academic recognition including promotions, tenure, awards, salary support and access to financial support for graduate students and research projects. In addition to individual academic accomplishment, regularly publishing in highly regarded journals in one’s field allows authors to engage in academic debates and shape understandings of which topics are deemed meritorious, noteworthy and interesting. Powerful voices in these academic journals thus help to map the academic landscape, drawing boundaries and labelling worthy areas of exploration. While it is acknowledged that first and last authorship positions denote a higher level of credit for the work, Hedt-Gauthier et al 49 found that health research conducted in Africa, or about Africa, was less likely to have first and last authors from LMICs when the publication included collaborating authors from high-income countries (HICs).
While well-established guidelines for defining what constitutes authorship exist and are endorsed by many medical journal editors,55 66 67 guidelines for how authorship positions should be distributed across authors are underdeveloped. Thatje67 provided rules of thumb for determining first and last authorship positions within the natural sciences, noting that disciplinary and national culture may play a role in how decisions are made. Rees et al 68 recently noted that while standards of authorship exist within global health research, they do not address power imbalances that exist between authors from LMIC and HIC. A recent consensus statement by Morton et al 69 provided guidelines for determining author order in partnerships between LMIC and HIC scholars. However, given the recency of these guidelines, it is yet to be determined whether they will be incorporated into authorship decisions among partnering researchers in the field of medical education.
We undertook a bibliometric analysis of five top medical education journals to determine which countries were represented in first and last authorship positions. Our aim was to provide empirical data about which countries or regions of the world were more or less prominent in the academic spaces dedicated to medical education. While recognising that many other journals, including predominantly clinical journals, also publish medical education research, we chose to focus on journals specifically designed to publish in this area. Thomas’s57 previous work was able to capture articles on the topic of medical education that were published within a broad range of clinical, specialty and disciplinary journals with scopes not exclusive to medical education research. We aimed to build on the work of Thomas57 and chose to focus on journals that primarily published within the field of medical education and health professions education, as they constitute spaces where debates and critiques are intended for audiences who tend to live and breathe within the sphere of medical education. In doing so, our aim was to capture the boundaries of a field that asserts to be international in scope.
In addition to conducting this research, we recognised that the process of doing the research was itself illustrative of issues that may affect publication trends. As a collaborative research team distributed across four continents, we realised that it was important to explicitly discuss issues of power and privilege as part of our analysis meetings. We recognised that we were working our way through specific and concrete research processes and practices in which issues of power, voice, legitimacy and representation were ever-present. As such, we agreed to keep an explicit focus on our research decisions, processes and practices with a view to identifying ways privilege and power were manifest and managed in the shared work. We have included description of relevant aspects of these reflections in the manuscript.
Methods
This study was conducted in two phases. In phase 1, the methodology for this study was conceptualised and designed by the three Portuguese authors (ER, AC and MJC) on this paper. In July 2018, these authors performed a search of the Web of Science database for citable items (reviews and articles) that had been published between 1 January 2012 and 31 December 2016 in the five top ranking medical education journals at that time. To identify the top ranking journals of the field, a topic search for ‘medical education’ was conducted in Web of Science and the categories for ‘healthcare sciences services’, ‘education scientific disciplines’ and ‘education educational research’ were further expanded. The journals with the highest impact factor within these categories were: Academic Medicine, Medical Education, Advances in Health Sciences Education, Medical Teacher and BMC Medical Education. Metadata for all reviews and articles from these five journals were extracted and downloaded into Microsoft Excel for data analysis. While Web of Science allowed for the export of author affiliations for all authors as a single data field, it was not possible to have author affiliation for first and last authors extracted separately. Consequently, there was the need to review each item and identify the country of author affiliation for first and last authors (when articles included multiple authors). Though time-consuming, this manual process of identifying country of origin for each first and last author allowed for a more accurate determination than what might be expected from assigning country of origin through the use of geocoding tools or software.57 70 The number of reviews and articles for each country with affiliated first and last authors were counted: For items in which first and last author had a single country affiliation and were from the same country, the item was counted only once. For items in which first and last authors were from different countries, or for which a first or last author had multiple country affiliations, the item was counted the same number of times as the number of countries that was listed. Articles were counted separately for each year and for each journal. This allowed for further evaluation of longitudinal variations over the 10 years of study and between publication sources. While some bibliometric studies include only a subsample of publications, our inclusion of all published articles allowed for an extremely accurate count of first and last authored publications originating from each country.57
Preliminary results from phase 1 were presented by the Portuguese team at the Association for Medical Education in Europe 2018 conference.71 A few years later, this paper’s cofirst authors were writing a commentary for which we wanted to cite the results presented at the conference. We learnt that the Portuguese-led work had not yet been able to move forward for publication (limited local research resources and extra work required for authors from a non-English first language setting), and, with approval of the Portuguese team, found resources in Canada to update the search and move manuscript writing forward. While acknowledging that the ability to advance the work was—ironically and problematically—contingent on specific HIC resource availability, we agreed that continuing this empirical work on publishing inequities was important. In addition of two Canadians to the Portuguese team, we also embraced the opportunity to include team members from Ethiopia and Brazil, as respected colleagues and as part of a commitment to ensure representation of LMIC perspectives in research being done about global research imbalances.
In phase 2 of this project, the reconstituted team decided to update the data collection, adding years 2017–2021 to the dataset, while following the same methodology as the original strategy. While we were aware that journal rankings within the field of medical education had shifted since phase 1 of the study, we opted to limit our analysis to the five journals originally identified to ensure consistency in methodology and in recognition of the longstanding role these journals have played in shaping the field. All aspects of data extraction, assignment of country of origin for first and last authors and counting techniques were replicated from the earlier analysis. Final analyses treated data from both phase 1 (years 2012–2016) and phase 2 (years 2017–2021) as a single dataset. Data analyses were conducted using Microsoft Excel and differences in proportions were compared using 95% CIs.72 73 Neither patients nor the public were engaged in the study design, conduct, reporting or distribution plans of the research. The datasets used and analysed during the current study have been archived as supplemental files.74
Results
A total of 8756 articles were extracted from Web of Science and country of origin was assigned to first and last authors based on listed institutional addresses. After articles were counted multiple times to reflect multiple geographic affiliations for first and last authors, 9948 unique items remained for subsequent analyses.
At the time of writing, there were 195 countries in the world, including 193 UN Member States, the Holy See and the State of Palestine.75 For these 195 countries, across all 5 journals and 7 years of analysis, the number of first or last authored publications originating from each country ranged from 0 to 3016. Over 42% of countries were not represented by a single first or last authored publication, approximately 12% were represented by a single first or last authored publication and under 7% were represented by more than 100 first or last authored publications (see table 1).
Table 1.
Number (per cent) of countries by number of publications in top five medical education journals, 2012-2021
| First or last authored publications, n | Countries, n | Per cent (%) |
| 0 publications | 83 | 42.6 |
| 1 publication | 23 | 11.8 |
| 2–10 publications | 32 | 16.4 |
| 11–50 publications | 30 | 15.4 |
| 51–100 publications | 11 | 5.6 |
| 101–500 publications | 8 | 4.1 |
| >500 publications | 5 | 2.6 |
The 5 countries with the greatest proportion of first and last authored publications included the USA with 3016 (30.3%) publications, Canada with 1313 (13.2%) publications, the UK with 1047 (10.5%) publications, the Netherlands with 791 (8.0%) publications and Australia with 776 (7.8%) publications (see table 2). Figure 1 shows the percentage of all publications with first or last authors from these five countries, and the remaining percentage (30.2%) of publications that originated from all ‘other’ countries combined. Together, these ‘big five’ nations of the USA, Canada, the UK, the Netherlands and Australia contributed 69.7% of all first and last authored publications across all journals and years of study. Figure 2 further shows the number of publications originating from each country across the globe between 2012 and 2021.
Table 2.
Number and per cent* of first/last authored publications from the USA, Canada, the UK, the Netherlands, Australia and ‘other’ countries, by journal, 2012–2021
| Impact factor (2018) | Acad Med | Med Educ | AHSE | Med Teach | BMC Med Educ | Total |
| 4.937 | 4.619 | 2.761 | 2.706 | 1.87 | ||
| USA | 1620 | 246 | 123 | 504 | 523 | 3016 |
| 72.7% | 20.6% | 16.7% | 23.7% | 14.3% | 30.3% | |
| (70.8%–74.5%) | (18.3%–22.9%) | (14.0%–19.4%) | (21.9%–25.5%) | (13.1%–15.4%) | (29.4%–31.2%) | |
| Canada | 347 | 299 | 169 | 278 | 220 | 1313 |
| 15.6% | 25.1% | 23.0% | 13.1% | 6.0% | 13.2% | |
| (14.1%–17.1%) | (22.6%–27.5%) | (20.0%–26.0%) | (11.6%–14.5%) | (5.2%–6.8%) | (12.5%–13.9%) | |
| UK | 48 | 197 | 68 | 368 | 366 | 1047 |
| 2.2% | 16.5% | 9.3% | 17.3% | 10.0% | 10.5% | |
| (1.6%–2.8%) | (14.4%–18.6%) | (7.2%–11.3%) | (15.7%–18.9%) | (9.0%–11.0%) | (9.9%–11.1%) | |
| Netherlands | 92 | 136 | 131 | 214 | 218 | 791 |
| 4.1% | 11.4% | 17.8% | 10.1% | 5.9% | 8.0% | |
| (3.3%–5.0%) | (9.6%–13.2%) | (15.1%–20.6%) | (8.8%–11.3%) | (5.2%–6.7%) | (7.4%–8.5%) | |
| Australia | 29 | 124 | 72 | 187 | 364 | 776 |
| 1.3% | 10.4% | 9.8% | 8.8% | 9.9% | 7.8% | |
| (0.8%–1.8%) | (8.7%–12.1%) | (7.6%–11.9%) | (7.6%–10.0%) | (9.0%–10.9%) | (7.3%–8.3%) | |
| Other | 93 | 190 | 172 | 575 | 1975 | 3005 |
| 4.2% | 15.9% | 23.4% | 27.0% | 53.9% | 30.2% | |
| (3.3%–5.0%) | (13.9%–18.0%) | (20.3%–26.5%) | (25.2%–29.0%) | (52.3%–55.5%) | (29.3%–31.1%) | |
| Total | 2229 | 1192 | 735 | 2126 | 3666 | 9948 |
*Percentages were calculated with a 95% CI
Acad Med, Academic Medicine; AHSE, Advances in Health Sciences Education; BMC Med Educ, BMC Medical Education; Med Educ, Medical Education; Med Teach, Medical Teacher.
Figure 1.
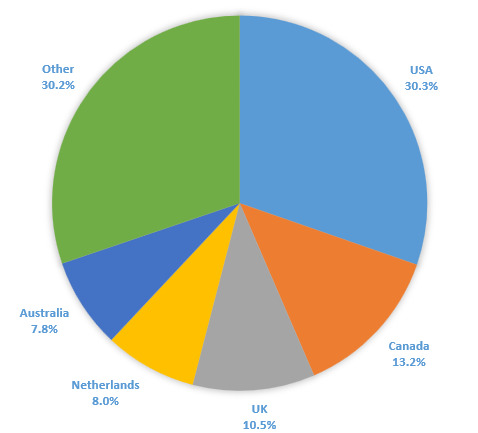
Per cent first/last authored publications from the USA, Canada, the UK, the Netherlands, Australia, all ‘other’ countries, all journals, 2012–2021.
Figure 2.

Number of first and last authored publications originating from each country, 2012–2021.
The inequitable presence of first and last authored publications from these ‘big five’ Global North countries was not evenly distributed across the five medical education journals. Furthermore, there was a strong positive relationship between the impact factor (2018) of each journal and the percentage of articles that were published by first and last authors from these five dominant countries. For example, in 2018 (when our first phase of data collection ended), of the five journals studied, Academic Medicine had the highest impact factor at 4.937 and the highest percentage (95.8%) of articles with first and last authors from these five dominant countries (table 2). BMC Medical Education, on the other hand, had the lowest impact factor at 1.87 and the lowest percentage (46.1%) of articles with first and last authors from these same countries (table 2). Impact factor is considered one measure of prestige within academic publishing,76 and these results suggest that only a small number of countries are represented in first and last authorship positions within the most prestigious journals.
While most of our analyses combined years 2012 to 2021 together, we also looked at how the percentage of first and last authored publications from ‘other’ countries outside of the USA, Canada, the UK, the Netherlands and Australia had changed over time. Across all journals, there was a statistically significant increase in the percentage of first and last authored publications from ‘other’ countries from 22.8% (95% CI 19.9% to 25.7%) in 2012 to 40.3% (95% CI 37.7% to 42.9%) in 2021 (figure 3). Most of this increase was driven by an increase in the total number of publications from BMC Medical Education. Although the proportion of publications from ‘other’ countries in BMC Medical Education did not significantly increase between 2012 and 2021, BMC Medical Education’s total number of publications more than quadrupled between 2012 and 2021 while the total number of publications from other journals remained relatively consistent across these years. For example, in 2012, Academic Medicine published 11 first or last authored publications from ‘other’ countries (5.1%) while BMC Medical Education published 74 first or last authored publication from ‘other’ countries (51.0%). In 2021, Academic Medicine published 14 articles from ‘other’ countries (6.5%), while BMC Medical Education published 423 first and last authored articles from ‘other’ countries (61.0%). This increase in total publications from BMC Medical Education translates into an increasing trend in the proportion of publications from ‘other’ countries when all five journals are grouped together. Of the five journals studied, BMC Medical Education has the lowest impact factor, and while it waives fees for corresponding authors from low-income countries and partially waives fees for corresponding authors from some lower-middle-income countries, it usually charges a fee for open access publication. Using the current World Bank classification of low-income countries, approximately 65 of BMC Medical Education’s 3666 publications (1.8%) would have been eligible for a full fee waiver between 2012 and 2021. While this overall increase in publications from ‘other’ countries will be encouraging if it is a permanent trend, this could be a temporary or pandemic-related fluctuation. Despite improvement, the proportion of publications from ‘other’ countries remains relatively low within the highest impact medical education journals.
Figure 3.
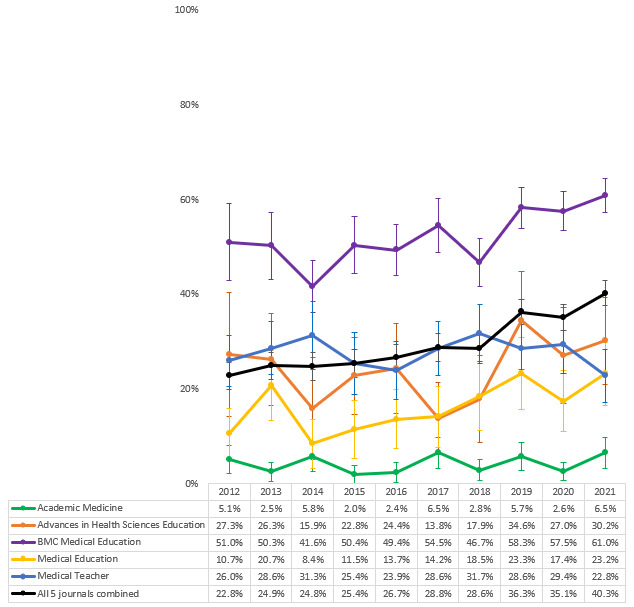
Per cent* of first/last authored publications from ‘other’ countries outside of the USA, Canada, the UK, the Netherlands and Australia, for each journal separately and for all journals combined, from 2012 to 2021.*Error bars were calculated using a 95% CI.
Discussion
Our data revealed a dominance of first and last authors from five countries in five top ranked journals within the international field of medical education. Being a bibliometric analysis, the results do not provide an explanation for why there is such significant dominance by these five countries. Also, as we did not include middle authors in our research design, there may be greater presence of authors from the other 190 countries of the world than we were able to capture by looking only at first and last authorship positions. Nevertheless, the prominence of five countries in prestigious authorship positions is a finding that requires attention. While our research was not designed to identify how this dominance compared with other fields, Thomas57 previously found that there were greater geographic disparities within medical education research than within education, medicine and the biological sciences. Our current research reiterated this pattern when analysing prestigious authorship positions. Our study only included articles that had been published in the five medical education journals which had the highest impact factor at a single point in time in 2018. As a measure of journal importance, impact factor is only one metric, and one that is in constant flux. Future research might expand on our strategy and include additional journals that publish on the topic of medical education, including journals which have experienced a significant increase in impact factor since we first devised our research strategy in 2018.
Tracking and decision-making about country assignation in bibliometric research is not always straightforward. As evidenced in previous bibliometric studies, there are many ways in which geographic origin might be determined. For the current study, we chose to double, or even triple-count publications as unique items when first or last authors claimed affiliations in multiple countries. In some instances, this led to confusion in determining whether an author had more authentic cultural connections to the Global North or the Global South. We view this as a limitation of the bibliometric nature of our study: in quantifying the geographic representation of first and last authors, we were unable to more meaningfully determine the cultural perspective from which each author was writing.
As an international research team deliberately designed to include representation from HICs and LMICs across several continents, we tried to be reflexive as we collectively advanced this project. We explicitly discussed aspects of the research process in our meetings. It was readily apparent that access to academic resources (both material resources and time) significantly shaped the research process. This included the fact that one of the Canadian authors holds a research chair that was able to provide funds for the second phase of data collection. The two Canadian authors therefore had more protected time to advance this project, which in and of itself is evidence of unearned privilege and showcases research inequities. As a team, we discussed this fact, recognised that it materially influenced the research process, while aiming to watch that it did not manifest as greater voice for these authors. We also saw this privilege as requiring greater responsibility from the Canadian authors to do the ‘heavy lifting’ in order to move the project forward. The team also discussed the fact of English language fluency (including the genres of academic writing) and the extent to which that made the writing process more efficient for the Canadian authors to lead. We recognised that no matter how careful we were, the fact of writing in English made it easier for the Canadians to shape the words, and spent time discussing details of language in our meetings. The team decided that it was acceptable for the Canadian authors to update the preliminary research of the Portuguese team. Given both time and English language facility, the Canadian authors also led the process of manuscript writing, with the other team members making substantial edits and comments. In discussions about authorship order and thinking about contributions and ICMJE guidelines,77 we initially thought it might be most appropriate to have a Canadian first author and Portuguese last author based on currently accepted publishing practices and given the role that MJC had played in the original design of the study. The irony of producing a manuscript in this space with a ‘big five’ first author was not lost on us, and we sought options to publish in other spaces that would acknowledge the significant work of authors less easily represented in current criteria. We know that HIC academics’ ability to engage in critical global work is significantly enabled by their learnings from and relationships with LMIC academic colleagues. Current authorship guidelines do not fully recognise this invisible intellectual labour on the part of LMIC academics, but as a team we decided that it was critical to incorporate these contributions into authorship decisions. As a result, we determined that cofirst authorship by an LIC and HIC academic on the team was the most accurate representation of authorship. The need for such conversations further highlights the structural issues that determine who can play the sport of international academic publishing. The fact that our effort to showcase structural inequities in academia had the potential to lead to the reproduction of dominant voices is telling. In thinking about ways to increase representation in medical education research, it is clear that neither recognition of inequities nor good intentions will in and of themselves lead to structural change.
Attention to privilege and power across all aspects of a research project can lead to different conversations and different choices, with potential to help trouble assumptions that maintain HIC academic dominance. Engaging in these processes is essential, but may require additional effort that in many cases will slow research output. We believe that this ‘extra’ work is necessary to improve knowledge creation and as a way to advance appropriate models of HIC–LMIC collaborative research practice. We also realise that this form of academic activity is not currently recognised in terms of academic metrics, and know there is more to do to find ways for such work to be valued.
The dominance of wealthy nations within spaces that claim to be international, though troubling, is not unique to medical education, the health professions or academia in general. The prominence of the ‘big five’ countries in medical education research brings to mind the colonisation of many Global South countries during the 19 Century when Global North sportsmen hunted for ‘big five’ trophy animals: elephants, lions, rhinos, leopards and buffalo. Symbolically, the hunting of big game in Africa and India served the purpose of solidifying the triumph of colonists over those being colonised.78 As a more modern sporting analogy, we are reminded of the Tokyo 2020/2021 Olympic and Paralympic games, an event that represents one of the world’s largest international sporting events. Within the popular media, Tokyo 2020/2021 was touted as one of the most equitable games in history. However, of the 206 nations and territories competing at the games, 98 countries had less than 10 athletes participating. In contrast, the games were host to 613 athletes from the USA, 552 from Japan, 478 from Australia, 425 from Germany, 406 from China, 398 from France, 376 from Great Britain, 372 from Italy and 370 from Canada.79
Rather than being a recent phenomenon, modern Olympic history, especially after World War I, has been described as paradoxically espousing universal ideals and providing an opportunity for the colonised to participate and win against the colonisers, while simultaneously reinforcing exclusionary, elitist and racist practices.80 Houghton81 traced the history of the inclusion of Indigenous Latin American athletes and other ‘recently conquered’ Indigenous peoples in the early 20th century Olympics. In addition to participating in primitive sideshows that were aimed at showcasing the ‘barbaric’ sporting practices of Indigenous tribes, these Indigenous peoples were also then made to compete alongside developed nations in modern Olympic events that set themselves up for ridicule, infantilisation and as a way to prove the inferiority of Global South nations.81 Of course, decisions about ‘what counts’ as an Olympic sport also contribute to the dominance of wealthy nations. Sports with long colonial histories, such as football and athletics82 continue to be included, as do sports with more recent histories that rely on extensive and expensive sporting infrastructure, such as velodrome cycling, bobsledding and sailboat racing. However, traditional African sports such as Nguni (stick fighting), Capoeira, donkey racing and Dambe boxing continue to be absent, despite recognition of their value to local peoples.83 We draw attention to this sporting analogy to show not only that North–South disparities are omnipresent and surreptitious, but that they are also engrained in structures and inequities that are built on historical and colonial roots that continue to be perpetuated through international spaces, even those that aim to unite humanity and have the allure of being inclusive.
In comparing medical education research to the Olympics, we hope that looking at structures elsewhere may open up new ways of seeing a space we take for granted. Bourdieu84 effectively examined sport as a way to highlight that in every sphere there are philosophical underpinnings that are inherently political. Bourdieu also emphasised social spheres as spaces of conflict and struggle, including the field of science.85 Albert and Kleinman85 drew on Bourdieu’s concepts in suggesting that it was necessary to understand how interactions that may appear to be based on cooperation may more accurately reflect domination and subordination. More recently, Martimianakis et al 86 drew attention to the need to consider the inevitable knowledge politics that inform discussions about research quality and rigour within medical education. We suggest that representation in the academic literature is an area which would benefit from further exploration of the ways knowledge politics shape what is considered legitimate in these spaces. Acknowledging the skewed proportion of authors from different countries does not lead directly to solutions designed to ‘add’ voices from LMICs without attention to the historical and colonial roots from which disparities have developed.
This leads to some potentially uncomfortable questions. For HIC researchers, it is pleasing to consider academic conversations with peers from other HICs to constitute international debates. But is it possibly a conceit to think that medical education research in its current form is truly globally relevant? To what extent is the new knowledge being shared in academic publications able to be implemented and evaluated in lower resource settings? Are important knowledges excluded from currently accepted content in medical education journals? How relevant is the content of top medical education journals in diverse contexts? How willing might HIC academics be to probe the layers of privilege that serves them well in terms of impact factor, academic promotions and claims of international recognition? Beyond individuals, are HIC academic institutions open to questioning the structures that maintain their high international rankings? LMIC academic institutions are also driven by academic rankings so individual LMIC researchers may be encouraged to preferentially aim for international journal publications. A related issue explored by others87 88 is how researchers from non-English speaking countries make choices about when to publish in ‘international’ English-language journals versus reaching audiences in their own country and language. These are not decisions that English-language country researchers need to make, adding to the burden placed on those academics. The concept of bibliodiversity (or diversity in scholarly publishing)89 90 has been adopted by Global South authors as a way of supporting the decolonization of Southern knowledge,91 and multilingual publishing may be one way that bibliodiversity can be achieved.92
Conclusions
There have been a recent series of calls to action and incisive analyses, most prominent in critical global health spaces,30 49 51 53 55 93 94 but also in medical education journals,31 47 56 57 64 95 that are contributing to a body of literature that demonstrates the ways academic publishing structures continue to privilege HIC academics. Continued conceptual and empirical work in these spaces is essential. It is also important to ensure that academics from diverse contexts are included in teams undertaking this work and that in these collaborations, close attention is paid to privilege, voice and representation.
As a research team, we believe that we must start and sustain these conversations across all aspects of our scholarly work. HIC academics, academic institutions and academic publishers must not view the opening of cracks into privileged spaces as a way of being ‘nice’ or as proof of benevolence. There is an ethical and moral imperative to examine and disassemble colonial structures. A recent call from the United Nations Educational, Scientific, and Cultural Organization (UNESCO)96 and the International Science Council92 compels us to consider scientific advancement a global public good to which open access is required. Eight recommendations were recently endorsed by the International Science Council,97 including ensuring that new scientific knowledge is accessible to all without limitations based on institutional privilege, geography, an ability to pay or language. UNESCO also calls for more collaborative and inclusive scientific practices aimed at the achievement of the Sustainable Development Goals98 and reducing global inequities.
HIC also have much to learn from LMIC colleagues, and must find the humility and will to listen. As HIC countries face severe health human resource shortages, there will be learnings from LMIC colleagues who have chronically grappled with these issues. Many LMIC countries spectacularly outshone HIC countries in effectively managing successive waves of the COVID-19 pandemic99 100 with far fewer resources. Making academic space for traditional knowledges from many global contexts, as well as deep examination of the effects of colonisation on health, are opportunities we must embrace. For science to be universal, it must be inclusive of a wide range of global knowledges.97 If scholarly medical education communities are willing to re-envisage the rules of the game to focus on ways we can be faster, higher and stronger together, we may better harness the transformative aspects of education to contribute to a healthier world.
Footnotes
Handling editor: Seye Abimbola
Contributors: DW, CRW, ER, AC and MJC made substantial contributions to the conceptualisation of this work. ER, AC and CC made contributions to the acquisition and analysis of the study data. All authors made contributions to the interpretation of the data. DW, CRW, CC and MJC drafted this manuscript, and ER, AC and TSL critically reviewed the manuscript for intellectual content. MJC is responsible for the overall content as guarantor and accepts full responsibility for the finished work and/or the conduct of the study, had access to the data, and controlled the decision to publish. All authors approved the final version of this manuscript, agreed to being accountable for all aspects of the work, and to investigating and resolving any questions that arise in relation to the accuracy and integrity of this work. All authors consented to having this manuscript published in BMJ Global Health.
Funding: This study did not receive external funding but did receive support from Cynthia Whitehead’s BMO Chair.
Map disclaimer: The inclusion of any map (including the depiction of any boundaries therein), or of any geographic or locational reference, does not imply the expression of any opinion whatsoever on the part of BMJ concerning the legal status of any country, territory, jurisdiction or area or of its authorities. Any such expression remains solely that of the relevant source and is not endorsed by BMJ. Maps are provided without any warranty of any kind, either express or implied.
Competing interests: CRW is the holder of the BMO Financial Group Chair in Health Professions Education Research at University Health Network. No other authors have any competing interests to declare.
Patient and public involvement: Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review: Not commissioned; externally peer reviewed.
Data availability statement
Data are available in a public, open access repository. The datasets generated and analysed during this study have been archived as online supplemental information files with medRxiv: https://doi.org/10.1101/2022.03.29.22273128.
Ethics statements
Patient consent for publication
Not applicable.
Ethics approval
No institutional ethics review was sought for this work since it did not involve human subjects.
References
- 1. Frenk J, Chen L, Bhutta ZA, et al. Health professionals for a new century: transforming education to strengthen health systems in an interdependent world. The Lancet 2010;376:1923–58. 10.1016/S0140-6736(10)61854-5 [DOI] [PubMed] [Google Scholar]
- 2. Weisz G, Nannestad B. The world health organization and the global standardization of medical training, a history. Global Health 2021;17:96. 10.1186/s12992-021-00733-0 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3. Nichols BL, Davis CR, Richardson DR, et al. Appendix J: International models of nursing. In: the future of nursing: leading change, advancing health [Internet]. Washington, DC, USA: National Academies Press; 2011. Available: https://www.ncbi.nlm.nih.gov/books/NBK209879/ [Accessed 24 Dec 2022]. [Google Scholar]
- 4. Bates I, John C, Seegobin P, et al. An analysis of the global Pharmacy workforce capacity trends from 2006 to 2012. Hum Resour Health 2018;16:3. 10.1186/s12960-018-0267-y [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5. Rizwan M, Rosson NJ, Tackett S, et al. Opportunities and challenges in the current era of global medical education. Int J Med Educ 2018;9:111–2. 10.5116/ijme.5ad1.ce9a [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6. Eckhert NL. Perspective: private schools of the Caribbean: Outsourcing medical education. Acad Med 2010;85:622–30. 10.1097/ACM.0b013e3181d2aee1 [DOI] [PubMed] [Google Scholar]
- 7. Duvivier RJ, Boulet JR, Opalek A, et al. Overview of the world's medical schools: an update. Med Educ 2014;48:860–9. 10.1111/medu.12499 [DOI] [PubMed] [Google Scholar]
- 8. Organization for Economic Co-operation and Development . Next steps for development in transition: A background paper [Internet]. presented during the 18 may 2017 meeting in Brussels, Belgium, Co-hosted by the directorate-general for international cooperation and development of the European Commission, the OECD development centre and the economic Commission for Latin America and the Caribbean. 2017. Available: https://www.oecd.org/dev/BackgroundPaper_DiT.pdf [Accessed 24 Dec 2022].
- 9. Harden RM, Grant J, Buckley G, et al. Best evidence medical education. Adv Health Sci Educ Theory Pract 2000;5:71–90. 10.1023/A:1009896431203 [DOI] [PubMed] [Google Scholar]
- 10. Norman G. Where we’ve come from, where we might go. Adv Health Sci Educ Theory Pract 2020;25:1191–201. 10.1007/s10459-020-10018-7 [DOI] [PubMed] [Google Scholar]
- 11. Kuper A, Albert M, Hodges BD. The origins of the field of medical education research. Acad Med 2010;85:1347–53. 10.1097/ACM.0b013e3181dce9a7 [DOI] [PubMed] [Google Scholar]
- 12. Pande I. Medicine, race and liberalism in British Bengal: Symptoms of empire. Abingdon, UK: Routledge, 2010. [Google Scholar]
- 13. Grosfoguel R, Hernandez R, Valasouez ER. Decolonizing the Westernized University: Interventions in philosophy of education from within and without. Lanham, Maryland: Lexington Books, 2016. [Google Scholar]
- 14. Grosfoguel R. The structure of knowledge in Westernized universities: Epistemic racism/Sexism and the four Genocides/Epistemicides of the long 16TH century. 2013. Available: https://www.niwrc.org/sites/default/files/images/resource/2%20The%20Structure%20of%20Knowledge%20in%20Westernized%20Universities_%20Epistemic.pdf [Accessed 24 Dec 2022].
- 15. Stein S, de Oliveira Andreotti V. Higher education and the modern/colonial global imaginary. Cultural Studies ↔ Critical Methodologies 2017;17:173–81. 10.1177/1532708616672673 [DOI] [Google Scholar]
- 16. Naidu T, Abimbola S. How medical education holds back health equity. The Lancet 2022;400:556–7. 10.1016/S0140-6736(22)01423-4 [DOI] [PubMed] [Google Scholar]
- 17. Bleakley A, Brice J, Bligh J. Thinking the post-colonial in medical education. Med Educ 2008;42:266–70. 10.1111/j.1365-2923.2007.02991.x [DOI] [PubMed] [Google Scholar]
- 18. Flexner A. Medical education in Europe: A report to the Carnegie foundation for the advancement of teaching. Boston, MA: DB Updike, The Merrymount Press, 1912. [Google Scholar]
- 19. Ludmerer KM. Time to heal: American medical education from the turn of the century to the era of managed care. Oxford, New York: Oxford University Press, 1999. [Google Scholar]
- 20. Whitehead C. The Good Doctor in Medical Education 1910-2010: A Critical Discourse Analysis. Germany: LAP Lambert Academic Publishing, 2013. [Google Scholar]
- 21. Flexner A. Medical education in the united states and canada. Science 1910;32:41–50. 10.1126/science.32.810.41 [DOI] [PubMed] [Google Scholar]
- 22. Paton M, Kuper A, Paradis E, et al. Tackling the void: the importance of addressing absences in the field of health professions education research. Adv Health Sci Educ Theory Pract 2021;26:5–18. 10.1007/s10459-020-09966-x [DOI] [PubMed] [Google Scholar]
- 23. Castillo EG, Isom J, DeBonis KL, et al. Reconsidering systems-based practice: advancing structural competency, health equity, and social responsibility in graduate medical education. Acad Med 2020;95:1817–22. 10.1097/ACM.0000000000003559 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24. Crampton PES, Afzali Y. Professional identity formation, Intersectionality and equity in medical education. Med Educ 2021;55:140–2. 10.1111/medu.14415 [DOI] [PubMed] [Google Scholar]
- 25. Fernandez A. Further incorporating diversity, equity, and inclusion into medical education research. Acad Med 2019;94:S5–6. 10.1097/ACM.0000000000002916 [DOI] [PubMed] [Google Scholar]
- 26. Naidu T. Modern medicine is a colonial Artifact: introducing Decoloniality to medical education research. Acad Med 2021;96:S9–12. 10.1097/ACM.0000000000004339 [DOI] [PubMed] [Google Scholar]
- 27. Naidu T. Southern exposure: levelling the northern tilt in global medical and medical humanities education. Adv Health Sci Educ Theory Pract 2021;26:739–52. 10.1007/s10459-020-09976-9 [DOI] [PubMed] [Google Scholar]
- 28. Norman G, Ellaway R. Looking back, looking forward. Adv in Health Sci Educ 2020;25:1–6. 10.1007/s10459-020-09961-2 [DOI] [PubMed] [Google Scholar]
- 29. Paton M, Naidu T, Wyatt TR, et al. Dismantling the master’s house: new ways of knowing for equity and social justice in health professions education. Adv in Health Sci Educ 2020;25:1107–26. 10.1007/s10459-020-10006-x [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30. Khan SA. Decolonising global health by Decolonising academic publishing. BMJ Glob Health 2022;7:e007811. 10.1136/bmjgh-2021-007811 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31. Kusurkar RA. The leaky pipeline of publications and knowledge generation in medical education. Perspect Med Educ 2022;11:70–2. 10.1007/s40037-022-00700-4 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32. Calhoun A, Genao I, Martin A, et al. Moving beyond implicit bias in Antiracist academic medicine initiatives. Acad Med 2022;97:790–2. 10.1097/ACM.0000000000004562 [DOI] [PubMed] [Google Scholar]
- 33. McKivett A, Paul D. How can medical educators be good ancestors. Med Educ 2022;56:1056–8. 10.1111/medu.14886 [DOI] [PubMed] [Google Scholar]
- 34. Sukhera J. Bridging health equity and quality improvement in medical education. Med Educ 2023;57:7–9. 10.1111/medu.14957 [DOI] [PubMed] [Google Scholar]
- 35. Slavin S. Is medical education Systemically racist. J Natl Med Assoc 2022;114:498–503. 10.1016/j.jnma.2022.06.002 [DOI] [PubMed] [Google Scholar]
- 36. Bhandal T. Ethical globalization? Decolonizing theoretical perspectives for internationalization in Canadian medical education. Can Med Educ J 2018;9:e33–45. [PMC free article] [PubMed] [Google Scholar]
- 37. Giuliani M, Frambach J, Broadhurst M, et al. A critical review of representation in the development of global oncology curricula and the influence of Neocolonialism. BMC Med Educ 2020;20:1–9. 10.1186/s12909-020-1989-9 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38. Larkins S, Michielsen K, Iputo J, et al. Impact of selection strategies on representation of Underserved populations and intention to practise: International findings. Med Educ 2015;49:60–72. 10.1111/medu.12518 [DOI] [PubMed] [Google Scholar]
- 39. Lorello GR, Silver JK, Moineau G, et al. Trends in representation of female applicants and Matriculants in Canadian Residency programs across specialties, 1995-2019. JAMA Netw Open 2020;3:e2027938. 10.1001/jamanetworkopen.2020.27938 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40. Soklaridis S, Kuper A, Whitehead CR, et al. Gender bias in hospital leadership: A qualitative study on the experiences of women Ceos. J Health Organ Manag 2017;31:253–68. 10.1108/JHOM-12-2016-0243 [DOI] [PubMed] [Google Scholar]
- 41. Soklaridis S, Black G, LeBlanc C, et al. Academic productivity of equity-deserving physician scholars during COVID-19: A Scoping review. Acad Med 2023;98:123–35. 10.1097/ACM.0000000000004971 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42. Franks AM, Calamur N, Dobrian A, et al. Rank and tenure amongst faculty at academic medical centers: A study of more than 50 years of gender disparities. Acad Med 2022;97:1038–48. 10.1097/ACM.0000000000004706 [DOI] [PubMed] [Google Scholar]
- 43. Jackson D, Ward D, Agwu JC, et al. Preparing for selection success: Sociodemographic differences in opportunities and obstacles. Med Educ 2022;56:922–35. 10.1111/medu.14811 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44. Mulder L, Wouters A, Twisk JWR, et al. Selection for health professions education leads to increased inequality of opportunity and decreased student diversity in the Netherlands, but lottery is no solution: A retrospective multi-cohort study. Med Teach 2022;44:790–9. 10.1080/0142159X.2022.2041189 [DOI] [PubMed] [Google Scholar]
- 45. Lee CR, Gilliland KO, Beck Dallaghan GL, et al. Race, Ethnicity, and gender representation in clinical case vignettes: A 20-year comparison between two institutions. BMC Med Educ 2022;22:585. 10.1186/s12909-022-03665-4 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46. Sukhera J, Goez H, Brown A, et al. Freedom from discrimination or freedom to discriminate? Discursive tensions within discrimination policies in medical education. Adv in Health Sci Educ 2022;27:387–403. 10.1007/s10459-022-10090-1 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47. Yip SWL, Rashid MA. Editorial diversity in medical education journals. Clin Teach 2021;18:523–8. 10.1111/tct.13386 [DOI] [PubMed] [Google Scholar]
- 48. Gibbs WW. Lost science in the third world. Sci Am 1995;273:92–9. 10.1038/scientificamerican0895-92 [DOI] [Google Scholar]
- 49. Hedt-Gauthier BL, Jeufack HM, Neufeld NH, et al. Stuck in the middle: A systematic review of authorship in collaborative health research in Africa, 2014-2016. BMJ Glob Health 2019;4:e001853. 10.1136/bmjgh-2019-001853 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 50. Lancet Global Health . Closing the door on parachutes and parasites. Lancet Glob Health 2018;6. 10.1016/S2214-109X(18)30239-0 [DOI] [PubMed] [Google Scholar]
- 51. Mbaye R, Gebeyehu R, Hossmann S, et al. Who is telling the story? A systematic review of authorship for infectious disease research conducted in Africa, 1980-2016. BMJ Glob Health 2019;4:e001855. 10.1136/bmjgh-2019-001855 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 52. Wondimagegn D, Soklaridis S, Yifter H, et al. Passing the microphone: broadening perspectives by amplifying Underrepresented voices. Adv Health Sci Educ Theory Pract 2020;25:1139–47. 10.1007/s10459-020-10012-z [DOI] [PMC free article] [PubMed] [Google Scholar]
- 53. Abimbola S. The foreign gaze: authorship in academic global health. BMJ Glob Health 2019;4:e002068. 10.1136/bmjgh-2019-002068 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 54. Balon R, Roberts LW, Coverdale J, et al. Globalization of medical and psychiatric education and the focus of academic psychiatry on the success of "International" authors. Academic Psychiatry 2008;32:151–3. 10.1176/appi.ap.32.2.151 [DOI] [PubMed] [Google Scholar]
- 55. Sam-Agudu NA, Abimbola S. Using scientific authorship criteria as a tool for equitable inclusion in global health research. BMJ Glob Health 2021;6:e007632. 10.1136/bmjgh-2021-007632 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 56. Buffone B, Djuana I, Yang K, et al. Diversity in health professional education scholarship: A document analysis of international author representation in leading journals. BMJ Open 2020;10:e043970. 10.1136/bmjopen-2020-043970 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 57. Thomas MP. The geographic and topical landscape of medical education research. BMC Med Educ 2019;19:189. 10.1186/s12909-019-1639-2 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 58. Asplund K, Eriksson M, Persson O. Country comparisons of human stroke research since 2001: A Bibliometric study. Stroke 2012;43:830–7. 10.1161/STROKEAHA.111.637249 [DOI] [PubMed] [Google Scholar]
- 59. Allik J, Lauk K, Realo A. Factors predicting the scientific wealth of nations. Cross-Cultural Research 2020;54:364–97. 10.1177/1069397120910982 [DOI] [Google Scholar]
- 60. Ravi K, Bentounsi Z, Tariq A, et al. Systematic analysis of authorship demographics in global surgery. BMJ Glob Health 2021;6:e006672. 10.1136/bmjgh-2021-006672 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 61. Stockemer D, Wigginton MJ. Publishing in English or another language: an inclusive study of scholar’s language publication preferences in the natural, social and Interdisciplinary sciences. Scientometrics 2019;118:645–52. 10.1007/s11192-018-2987-0 [DOI] [Google Scholar]
- 62. Kokol P, Blažun Vošner H, Završnik J. Application of Bibliometrics in medicine: A historical Bibliometrics analysis. Health Info Libr J 2021;38:125–38. 10.1111/hir.12295 [DOI] [PubMed] [Google Scholar]
- 63. Maggio LA, Ninkov A, Frank JR, et al. Delineating the field of medical education: Bibliometric research Approach(Es). Med Educ 2022;56:387–94. 10.1111/medu.14677 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 64. Maggio LA, Ninkov A, Costello JA, et al. Knowledge syntheses in medical education: meta-research examining author gender, geographic location, and institutional affiliation. PLoS ONE 2021;16:e0258925. 10.1371/journal.pone.0258925 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 65. United . Standard country or area codes for statistical use (M49) Department of economic and social affairs. Geneva, Switzerland: statistics division, United Nations. 2018. Available: https://unstats.un.org/unsd/methodology/m49/ [Accessed 24 Dec 2022].
- 66. Uijtdehaage S, Mavis B, Durning SJ. Whose paper is it anyway? authorship criteria according to established scholars in health professions education. Acad Med 2018;93:1171–5. 10.1097/ACM.0000000000002144 [DOI] [PubMed] [Google Scholar]
- 67. Thatje S. Reaching out for scientific legacy: how to define authorship in academic publishing. Naturwissenschaften 2016;103:10. 10.1007/s00114-016-1335-6 [DOI] [PubMed] [Google Scholar]
- 68. Rees CA, Sirna SJ, Manji HK, et al. Authorship equity guidelines in global health journals. BMJ Glob Health 2022;7:e010421. 10.1136/bmjgh-2022-010421 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 69. Morton B, Vercueil A, Masekela R, et al. Consensus statement on measures to promote equitable authorship in the publication of research from international partnerships. Anaesthesia 2022;77:264–76. 10.1111/anae.15597 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 70. Geocoding API. Developer guide Google developers [Internet]. 2022. Available: https://developers.google.com/maps/documentation/geocoding/intro [Accessed 24 Dec 2022].
- 71. Costa MJ, Van Schalkwyk S, Ho M-J, et al. Equity in the global health sciences education community: levelling the playing fields. Association for Medical Education in Europe Annual Conference; Basel, Switzerland, August 2018. [Google Scholar]
- 72. Williams R, Bornmann L. Sampling issues in Bibliometric analysis. Journal of Informetrics 2016;10:1225–32. 10.1016/j.joi.2015.11.004 [DOI] [Google Scholar]
- 73. Koepsell TD, Weiss NS. Epidemiologic methods: Studying the occurrence of illness. New York, NY, USA: Oxford University Press, 2003. [Google Scholar]
- 74. Wondimagegn D, Whitehead C, Cartmill C, et al. Faster, higher, stronger – together? A bibliometric analysis of author distribution in top medical education journals. MedRxiv [Preprint] 2022. 10.1101/2022.03.29.22273128 [DOI] [PMC free article] [PubMed]
- 75. United . About us. 2021. Available: https://www.un.org/en/about-us [Accessed 11 Jul 2022].
- 76. Saha S, Saint S, Christakis DA. Impact factor: A valid measure of Journal quality. J Med Libr Assoc 2003;91:42–6. [PMC free article] [PubMed] [Google Scholar]
- 77. International Committee of Medical Journal Editors (ICMJE) . Defining the role of authors and contributors. 2022. Available: http://www.icmje.org/recommendations/browse/roles-and-responsibilities/defining-the-role-of-authors-and-contributors.html [Accessed 27 Sep 2022].
- 78. Storey WK. Big cats and imperialism: lion and tiger hunting in Kenya and northern India, 1898-1930. J World Hist 1991. [Google Scholar]
- 79. Whereig.com . List of participating countries in the Tokyo Olympics 2020-21. Available: https://www.whereig.com/olympics/summer-olympics-participating-countries.html [Accessed 11 Jul 2022].
- 80. Chatziefstathiou D. Paradoxes and Contestations of Olympism in the history of the modern Olympic movement. Sport in Society 2011;14:332–44. 10.1080/17430437.2011.557269 [DOI] [Google Scholar]
- 81. Houghton F. Latin America and the Olympic ideal of progress: an athletes perspective. Int J Hist Sport 2005;22:158–76. 10.1080/09523360500035719 [DOI] [Google Scholar]
- 82. Charitas P. Imperialisms in the Olympics of the Colonization in the Postcolonization: Africa into the International Olympic Committee, 1910-1965. Int J Hist Sport 2015;32:909–22. 10.1080/09523367.2015.1027153 [DOI] [Google Scholar]
- 83. Robertson ECJ. 7 traditional African sports that should be in the Olympics. Available: https://www.okayafrica.com/7-traditional-african-sports-olympics/ [Accessed 11 Jul 2022].
- 84. Bourdieu P. Sport and social class. Social Science Information 1978;17:819–40. 10.1177/053901847801700603 [DOI] [Google Scholar]
- 85. Albert M, Kleinman DL. Bringing Pierre Bourdieu to science and technology studies. Minerva 2011;49:263–73. 10.1007/s11024-011-9174-2 [DOI] [Google Scholar]
- 86. Martimianakis MA, Mylopoulos M, Woods NN. Developing experts in health professions education research: knowledge politics and adaptive expertise. Adv Health Sci Educ Theory Pract 2020;25:1127–38. 10.1007/s10459-020-10014-x [DOI] [PubMed] [Google Scholar]
- 87. Englander K. The Globalized world of English scientific publishing: an Analytical proposal that Situates a Multilingual scholar. In: López-Bonilla G, Englander K, eds. Discourses and Identities in Contexts of Educational Change: Contributions from the United States and Mexico 387. Bern, Switzerland: Peter Lang AG, 2011: 209–28. Available: https://www.jstor.org/stable/42980952 [Google Scholar]
- 88. Mu E, Pereyra-Rojas M. Impact on society versus impact on knowledge: why Latin American scholars do not participate in Latin American studies. Latin American Research Review 2015;50:216–38. 10.1353/lar.2015.0021 [DOI] [Google Scholar]
- 89. Jussieu call for open science and Bibliodiversity. 2017. Available: https://jussieucall.org/jussieu-call/ [Accessed 24 Dec 2022].
- 90. Shearer K, Chan L, Kuchma I, et al. Fostering Bibliodiversity in scholarly communications: A call for action. 2020. Available: https://zenodo.org/record/3752923#.Yehzky2z3s0 [Accessed 24 Dec 2022].
- 91. Berger M. Bibliodiversity at the centre: Decolonizing open access. Development and Change 2021;52:383–404. 10.1111/dech.12634 [DOI] [Google Scholar]
- 92. Balula A, Leão D. Multilingualism within scholarly communication in SSH. A literature review. JLISIt 2021;12:88–98. 10.4403/jlis.it-12672 [DOI] [Google Scholar]
- 93. Naidu T. Says who? northern Ventriloquism, or Epistemic disobedience in global health scholarship. The Lancet Global Health 2021;9:e1332–5. 10.1016/S2214-109X(21)00198-4 [DOI] [PubMed] [Google Scholar]
- 94. Sayegh H, Harden C, Khan H, et al. Global health education in high-income countries: confronting Coloniality and power asymmetry. BMJ Glob Health 2022;7:e008501. 10.1136/bmjgh-2022-008501 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 95. Wyatt TR. The sins of our forefathers": Reimagining research in health professions education. Adv Health Sci Educ Theory Pract 2022;27:1195–206. 10.1007/s10459-022-10111-z [DOI] [PubMed] [Google Scholar]
- 96. United Nations Educational ,. Scientific and cultural Organization (UNESCO). recommendations on open science. 2021. Available: https://en.unesco.org/science-sustainable-future/open-science/recommendation [Accessed 24 Dec 2022].
- 97. International Science Council . Opening the record of science: making scholarly publishing work for science in the Digital era. Paris, France: International Science Council, 24 December 2021. Available: https://council.science/wp-content/uploads/2020/06/202104_Opening-the-Record-of-Science-Summary_01-ENGLISH-online.pdf [accessed 11 Jul 2022]. [Google Scholar]
- 98. United Nations General Assembly . Transforming our world: the 2030 agenda for sustainable development. Geneva, Switzerland: United Nations, 2015. Available: https://sdgs.un.org/2030agenda [Google Scholar]
- 99. Kapata N, Ihekweazu C, Ntoumi F, et al. Is Africa prepared for tackling the COVID-19 (SARS-Cov-2) epidemic. lessons from past outbreaks, ongoing Pan-African public health efforts, and implications for the future. Int J Infect Dis 2020;93:233–6. 10.1016/j.ijid.2020.02.049 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 100. Wondimagegn D, Petros A, Asrat Y, et al. COVID-19 in Ethiopia: A Contextual approach to explaining its slow growth. J Glob Health 2020;10:020369. 10.7189/jogh.10.020369 [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
Data are available in a public, open access repository. The datasets generated and analysed during this study have been archived as online supplemental information files with medRxiv: https://doi.org/10.1101/2022.03.29.22273128.