

Abstract
Aim
To assess and correlate dactyloscopy and behavior of children undergoing dental treatment.
Materials and methods
A total of 30 children aged 4–8 years who needed at least one restoration without administration of local anesthesia were included. Two examiners recorded the behavior of the child as per Frankl's behavior rating scale and after the treatment, the subjects’ fingerprints were taken using an ink pad and white paper. The data were analyzed using Statistical Package for the Social Sciences (SPSS) versions 23 and a Chi-squared test was carried out (p < 0.05).
Results
The loop type fingerprint had the highest frequency, while the archtype had the lowest. The child's behavior differed greatly (p < 0.05) based on dermatoglyphic characteristics, with the loop pattern being seen in cooperative children and the whorl pattern in uncooperative children.
Conclusion
There is a positive correlation between fingerprint type and children's dental care.
Clinical significance
Dactyloscopy can be used to determine the behavior of children coming for dental treatment and hence help in their management.
How to cite this article
Janiani P, Subramanian EMG. Assessment and Correlation between Dactyloscopy and Behavior of Children Undergoing Dental Treatment: A Cross-sectional Study. Int J Clin Pediatr Dent 2023;16(3):444–447.
Keywords: Behavior, Children, Dental, Fingerprint, Frankl behavior rating scale
Introduction
Pediatric dentistry revolves around the premise of assessing the behavior and reactions of children1 as every child develops emotionally and mentally at different rates causing varied reactions to the same modalities; some children could be highly cooperative and unfazed while others can react in a rather noncooperative manner rejecting any or all forms of attempted treatment.2 This behavior of the child in a dental setup is influenced by environmental factors such as the outlook of the operatory, the doctor's attire and attitude amongst others, and by genetic factors.3
Fingerprint patterns have been identified as a genetic trait that is both distinct and consistent over one's existence. Dactyloscopy, more commonly known as dermatoglyphics, is the science of comparing the fingerprint patterns, lines, mounts, and shapes of the hands of an individual.4 The uniqueness and permanent nature of a fingerprint over a lifespan make it an appropriate tool to identity recognition. Cummin and Midlo divided these prints into three major groups namely loop, whorl, and arch types.5,6 The most commonly seen pattern is a loop and it is described as a series of ridges that reach the pattern area on one side of the digit, suddenly recurve, and exit the pattern area on the opposite side. The ridges in a whorl are concentrically arranged and the arch ridge pattern shows parallel ridges crossing the finger from one side to the other without recurving.7
Despite their distinctive nature, it's been hypothesized that fingerprints have an inheritable quality.8 Most studies available in the literature have correlated systemic medical problems such as bronchial asthma,9 congenital heart disease, and rheumatoid arthritis with fingerprint patterns. In the field of dentistry, fingerprint patterns have been correlated to malocclusion,10 dental caries,11 as well as periodontal diseases.12
According to genetic and biological research, fingerprints may also be used to understand behavioral patterns, abilities, capabilities, and personality qualities.13 However, very few studies have showcased a link between the behavioral aspects of an individual and fingerprints. One such study conducted by Shrestha et al. reported that those individuals with a loop type of fingerprint patterns display emotions making them appear as shy, whorl type as those who are strong-headed with an unwavering mind when it comes to their beliefs whereas arch types do not like to socialize. Hurray showed a connection between the lobes of the brain and fingers.14 Thus going to show how one's behavior could be linked to their fingerprints.
There are very few studies in the literature that correlate dermatoglyphic patterns and the behavior of children undergoing dental treatment. Understanding their behavior from a genetic basis might enable us to manage a child better when they come for treatment. Therefore, the aim of the present study was to assess and correlate dactyloscopy and the behavior of children reporting for dental treatment.
Materials and Methods
In this cross-sectional study, a random sampling method was used to include 30 children reporting to the Department of Pediatric and Preventive Dentistry, Saveetha Dental College and Hospital, Saveetha Institute of Medical & Technical Sciences (SIMATS) (Deemed to be University), Chennai, Tamil Nadu, India. Ethical clearance was obtained from the Institutional Review Board. Those aged 4–8 years, requiring at least one restoration that did not need local anesthesia administration and who consented to participate were included. Mentally or physically challenged children, those with developmental anomalies, skin disorders, trauma, or any pathology to the fingertips, and those allergic to ink pads were excluded from the study. Participants who complained of dental pain were also omitted from the study.
On the child's first visit to the dental clinic, the intraoral examination was carried out by a single investigator. If there were any restorations to be done which would not need the administration of local anesthesia, the parent was informed and consent was obtained. In the same visit, the same principal investigator restored one tooth by preparing a cavity with a 169L bur in a high-speed handpiece (NSK, Japan) followed by the use of a spoon excavator GDC for caries excavation. The tooth was etched with 37% phosphoric acid for 15–20 seconds, washed, and air-dried. This was followed by bonding agent application with an applicator tip. It was light cured and the tooth was finally restored with composite. During the use of the high-speed handpiece, the investigator recorded the child's behavior as per Frankl's behavior rating scale. Another examiner was also asked to independently record the behavior during the treatment process. The behavior was decided by a mutual agreement between both the principal investigator and the examiner to avoid bias. The behavior of a child was rated as per Frankl's behavior rating scale.15
After the treatment, the fingerprints were recorded. Both hands were washed with soap water, wiped, and softly pressed on the blue ink stamp pad (Faber-Castell, Germany) before being placed on the white bond paper to make impressions. A roller was used to apply some pressure. Right-hand prints were taken followed by left-hand prints. The trained and calibrated dentist magnified, categorized, and analyzed the prints twice using the Cummins system of fingerprint recognition. If there was a discrepancy between the findings, another qualified dentist was blinded, and calibrated to verify and classify it.
The results of the study were tabulated in a spreadsheet (Microsoft Excel datasheet), exported, and statistically analyzed using SPSS software 23.0 (IBM Corporation, New York, United States of America). Descriptive statistics and Chi-squared tests were carried out to compare the groups. The p < 0.05 was considered statistically significant.
Results
In this study, 30 children (19 girls and 11 boys) aged 4–8 years were included with a mean age of 6.2 years.
Overall, the fingerprint with the highest frequency was the loop type, while the archtype had the lowest. The distribution of fingertip patterns and behavior is seen in Figure 1 and Table 1. In children with definitely positive behavior, the loop pattern was the only pattern seen. In subjects with definitely negative behavior, the whorl pattern was the most common. Hence, our results show that the behavior of the child varied significantly depending on dermatoglyphic patterns (p < 0.05).
Fig. 1.
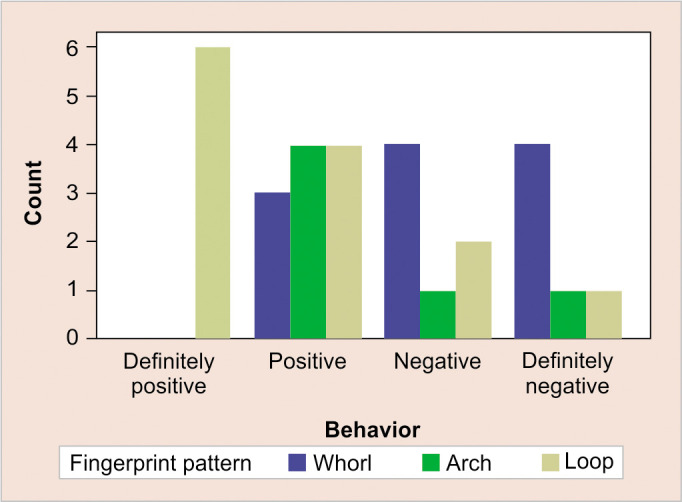
Graphical representation of the relationship between fingerprint types and behavior
Table 1.
Relationship between fingerprint types in terms of behavior
| Fingerprint pattern | p-value | |||
|---|---|---|---|---|
| Whorl | Arch | Loop | ||
| Behavior | 0.036* | |||
| Definitely positive | 0 | 0 | 6 | |
| Positive | 3 | 4 | 4 | |
| Negative | 4 | 1 | 2 | |
| Definitely negative | 4 | 1 | 1 | |
*Statistically significant p-value (p < 0.05)
In terms of age and gender, there was no significant difference between the groups (Table 2).
Table 2.
Relationship between fingerprint types in terms of gender
| Fingerprint pattern | Total | p-value | |||
|---|---|---|---|---|---|
| Whorl | Arch | Loop | |||
| Gender | 0.977# | ||||
| Female | 7 | 4 | 8 | 19 | |
| Male | 4 | 2 | 5 | 11 | |
| Total | 11 | 6 | 13 | 30 | |
#Statistically insignificant p-value (p > 0.05)
Discussion
Human personality and attitudes are vague and uncertain as they behave in a variety of ways depending on the situation. Given their impressionable age, a child's behavior is often more varied and is also easily influenced.
Penfield and Rasmussen, Canadian neurobiologists were the first to discover a functional connection between fingerprints and different parts of the human brain.16 The neocortex is the brain's main intelligence hub. Its neural makeup has a big impact on a person's ability to interpret, understand, and respond to stimuli. The distinctive pattern of grooves formed in the prenatal stage defines the degree of intellect exhibited by each person. According to developmental biology, dermal ridge development is timed to match that of the neocortex.17 As a result, fingerprints or dermal ridge patterns may be used to determine children's behavior.
The purpose of this study was to conduct a preliminary investigation into the relationship between fingerprint types and children's behavior and cooperation in a dental setting. It was seen that the whorl and loop types were commonly found in the uncooperative and cooperative groups, respectively.
In a study conducted by Mokhtari et al., a statistically significant relation was found between fingerprint patterns and behavior. Their results were consistent with ours, where the loop pattern was predominantly seen in cooperative children and whorl in the uncooperative ones.1
According to Singh and Majmudar, dermal ridge patterns can provide information about a person's feelings, motives, and success in a given situation.13
Individuals with the loop fingerprint form are incredibly adaptable to changes. They find it easier to voice their feelings, adjust to their environments, and interact than most others. This trait explains why cooperative children have such a high percentage of this fingerprint type. Individuals with a high degree of adaptability will be best suited to the current dental environment.13
The whorl fingerprint type is synonymous with powerful personalities and intellect. This category is known for its diverse identity and behavior. The lower cooperation, as well as the higher proportion of this fingerprint type in the uncooperative group, can be clarified by their sensitivity, and vulnerability to the presence of feelings in relationships.13
About 5–10% of the overall fingerprints contained in any random sampling space are arched. Singh et al. reported that people with archtype fingerprints choose a simple lifestyle and enjoy interacting with others. They have outstanding memories and are imaginative in the field of research and medicine. These people are not likely to dream about the future and want to enjoy the present, and as a result, they are more likely to have problems.18
Studies have also looked at the connection between fingerprints and psychological conditions including autism, dementia, and bipolar illness. Kazemi et al. discovered that people with autism had more loops in their fingerprints than those without autism, implying that fingerprints may be a factor in autism screening.19 According to Zarghami et al. individuals with bipolar disorder have whorl patterns more commonly than the control population. The arch form, on the contrary, was less common in schizophrenia patients than in the control group.20
Drawbacks of this study included that a digitized method of fingerprint recording was not used making fingerprint recording not only difficult but maybe even inaccurate. The current research was conducted on South Indian subjects; the findings should be confirmed in samples with a wide range of demographic and ethnic characteristics. Lastly, studies with larger sample sizes should be conducted to ascertain these findings.
Conclusion
Despite the limitations of this study, it can be concluded that there is a significant correlation between fingerprint patterns and children's behavior during dental care. Loop pattern was associated with cooperative children whereas whorl pattern was seen in uncooperative children. If the presence of such an association is verified in larger-scale research, it may be used to determine the type of behavior children would exhibit in the dental setting based on their fingerprint type.
Clinical Significance
Assessing the type of behavior a child will exhibit in a dental setting based on their fingerprint shape will aid in their management and care.
Orcid
Palak Janiani https://orcid.org/0000-0002-4957-3083
Footnotes
Source of support: Nil
Conflict of interest: Dr Erulappan MG Subramanian is associated as the National Editorial Board member of this journal and this manuscript was subjected to this journal's standard review procedures, with this peer review handled independently of this editorial board member and his research group.
References
- 1.Mokhtari S, Mokhtari S, Salehi Shahrabi M. Fingerprints as an index for investigating cooperation by children in dentistry: a pilot study. Eur Arch Paediatr Dent. 2021;22(2):203–207. doi: 10.1007/s40368-020-00570-6. [DOI] [PubMed] [Google Scholar]
- 2.Berge MT, Veerkamp JSJ, Hoogstraten J, et al. Childhood dental fear in the Netherlands: prevalence and normative data. Community Dent Oral Epidemiol. 2002;30(2):101–117. doi: 10.1034/j.1600-0528.2002.300203.x. [DOI] [PubMed] [Google Scholar]
- 3.Hetherington EM, Mavis Hetherington E. Review of child psychology. Contemporary psychology: A Journal of Reviews. (7th Ed) 1975;20:597–598. [Google Scholar]
- 4.Fuller IC. Dermatoglyphics: a diagnostic aid? J Med Genet. 1973;10(2):165–169. doi: 10.1136/jmg.10.2.165. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Cummins HG, Midlo C. Palmar and plantar epidermal ridge configurations (dermatoglyphics) in European-Americans. Am J Phys Anthropol. 2005;9(4):471–502. doi: 10.1002/ajpa.1330090422. [DOI] [Google Scholar]
- 6.Agarwal KK, Dutt HK, Chandra S, et al. General assumption of psychological behavior based on finger print pattern. Am Int J Biol Life Sci. 2012;3(1):59–65. doi: 10.5296/jbls.v3i1.1499. [DOI] [Google Scholar]
- 7.Agarwal M, Alex A, Konde S. Relationship between dermatoglyphics, cheiloscopy, rugoscopy, and dental caries: a cross-sectional study in Bengaluru, Karnataka. Contemp Clin Dent. 2018;9(4):577–581. doi: 10.4103/ccd.ccd_611_18. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Slatis HM, Katznelson MB, Bonné-Tamir B. The inheritance of fingerprint patterns. Am J Hum Genet. 1976;28(3):280–289. [PMC free article] [PubMed] [Google Scholar]
- 9.Singh S, Khurana AK, Harode HA, et al. Study of fingerprint patterns to evaluate the role of dermatoglyphics in early detection of bronchial asthma. J Nat Sci Biol Med. 2016;7(1):43–46. doi: 10.4103/0976-9668.175066. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Jindal G, Pandey RK, Gupta S, et al. A comparative evaluation of dermatoglyphics in different classes of malocclusion. Saudi Dent J. 2015;27(2):88–92. doi: 10.1016/j.sdentj.2014.11.012. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Singh KK, Menka K, Anand K, et al. Correlation between dermatoglyphics and dental caries in children: a case-control study. J Family Med Prim Care. 2020;9(6):2670–2675. doi: 10.4103/jfmpc.jfmpc_108_20. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Vaidya P, Mahale S, Badade P, et al. Dermatoglyphics in periodontics: an assessment of the relationship between fingerprints and periodontal status - a cross-sectional observation study. Indian J Dent Res. 2017;28(6):637–641. doi: 10.4103/ijdr.IJDR_621_16. [DOI] [PubMed] [Google Scholar]
- 13.Singh M, Majumdar O. Dermatoglyphics: blueprints of human cognition on fingerprints. Int J Comput Sci Commun. 2015;6(2):124–146. [Google Scholar]
- 14.Shrestha DB, Gupta VP, Chaurasiya PS, et al. Study of correlation between different fingerprint patterns, blood groups, and social behavior among medical students (Nepalese Citizens). PJST. 2016;17(2):288–292. [Google Scholar]
- 15.Narayan VK, Samuel SR. Appropriateness of various behavior rating scales used in pediatric dentistry: a review. J Glob Health. 2020;2(2):112–117. doi: 10.25259/JGOH_64_2019. [DOI] [Google Scholar]
- 16.Penfield W, Rasmussen T. The cerebral cortex of man; a clinical study of localization of function, by Wilder Penfield and Theodore Rasmussen. 1950:248p. [Google Scholar]
- 17.Altan MZ, Gardner H, Altan MZ. Intelligence reframed: multiple intelligences for the 21st Century [Internet]. TESOL Quarterly. 2001;35:204. [Google Scholar]
- 18.Prabhu R, Ravikumar CN. A novel extended biometric approach for human character recognition using fingerprints. Int J Comput Appl. 2013;77(1):37–44. doi: 10.5120/13361-0954. [DOI] [Google Scholar]
- 19.Kazemi M, Fayyazi-Bordbar MR, Mahdavi-Shahri N. Comparative dermatoglyphic study between autistic patients and normal people in Iran. Iran J Med Sci. 2017;42(4):392–396. [PMC free article] [PubMed] [Google Scholar]
- 20.Zarghami M, Mahmoudi M, Daneshpour SMM. Relationship between dermatoglyphic patterns in bipolar I disorder and schizophrenia. J Mazandaran Univ Med Sci. 2010;20(76):33–41. [Google Scholar]