

Abstract
Context
Different irrigation materials in pediatric endodontics.
Aims
To evaluate the efficacy of chlorhexidine (CHX), diode laser, and saline in primary teeth root canals.
Settings and design
This manuscript is designed to know the effectiveness of the different root canal irrigants and laser irradiation technology in primary teeth root canals.
Materials and methods
A total of 60 primary teeth from 60 children were selected and divided into three groups of 20 each. Group I (CHX), group II (diode laser), and group III (saline). Pulp tissue was extirpated from the root canals of primary teeth, and samples were collected using sterile paper points. After cleaning and shaping, the root canals of the teeth in each group were disinfected using CHX and saline or irradiated with a diode laser. The samples were collected again and sent for microbiological examination.
Statistical analysis used
Statistical analyzes were performed using the Wilcoxon signed-rank test, Mann–Whitney U test, and Kruskal–Wallis one-way analysis of variance. All analyzes were conducted using the Statistical Package for the Social Sciences version 23.0.
Results
The colony-forming unit (CFU) of the predisinfection sample served as a baseline for comparisons throughout the study. The mean microbial counts of all the postdisinfected samples were reduced after disinfection. Intergroup comparisons showed significant results between groups I and III (CHX and saline) and groups II and III (diode laser and saline) (p < 0.01), whereas groups I and II (CHX and diode laser) showed nonsignificant results (p < 0.092).
Conclusion
Diode laser irradiation succeeded in reducing root canal infection when compared with 2% CHX. Diode laser irradiation can also be used for disinfecting the root canal in primary teeth.
How to cite this article
Botu RK, Rachuri P, Martha S, et al. Comparative Evaluation of the Efficacy of Chlorhexidine, Diode Laser, and Saline in Reducing the Microbial Count in Primary Teeth Root Canals: An In Vivo Study. Int J Clin Pediatr Dent 2023;16(3):459-463.
Keywords: Chlorhexidine, Diode laser, Primary teeth root canal disinfection, Saline
Introduction
The main goal of pulp therapy in primary teeth is to maintain an intact dental arch, a healthy periodontium, whenever possible. The key determinants of the success of endodontic therapy depend on many elements like a precise diagnosis, in-depth canal cleansing, and, more importantly, an irrigation protocol.1 Endodontic treatment for primary teeth is thought to be extremely difficult because of its unusual internal geometry and other characteristics like furcation connections and horizontal anastomoses.2 The mechanical instrumentation approach has limited effectiveness in the elimination of bacterial colonization, which is present in the deeper layers and other irregularities in the root canal. The root canals of primary teeth are filled with a gelatinous mass of necrotic pulpal remnants and tissue fluids in the apical root portion. Hence, irrigation and instrumentation complement each other in complete debridement and disinfection of the root canals.3
As a result, irrigation and instrumentation work together to completely debride and disinfect the root. Hydrogen peroxide, CHX, sodium hypochlorite, and regular saline solutions are the most often utilized intracanal irrigation solutions.4
One of the most recent breakthroughs is cleaning root canals with lasers CO2 erbium-doped yttrium-aluminium-garnet, neodymium-doped yttrium aluminium garnet, argon, and diode lasers, as well as photodynamic treatment are all options for root canal disinfection. It is advantageous to use a laser to treat the young patient for an oral and dental operation because it causes less anxiety in the child and is more well-liked by parents. Children become more cooperative when a doctor uses the laser for a surgical or pulpal operation, and it also improves the treatment result.5
The majority of the current literature concerns in vitro investigations on permanent teeth, with only a small amount including primary teeth. As a result, the current investigation was conducted in primary teeth, which contain a far larger range of pathogens and had greater penetration into tubules than any in vitro system. The goal of this study was to see how effective CHX, diode lasers, and ordinary saline were effective at lowering the amount of bacteria in the root canals of primary teeth.
Materials and Methods
Materials used in the study are shown in Table 1.
Table 1.
The materials used in the study
| Petri dish |
| Eppendorf tubes |
| Blood agar |
| Thioglycolate |
| A 2% CHX gluconate solution |
| Normal saline |
| Diode laser |
| Biosafety cabinet |
| Anaerobic jar |
| Anaerobic gas pack |
| Inoculating loop |
| Armamentarium for pulp therapy |
| Local Anesthesia |
| Incubator |
| Digital colony counter |
Inclusion Criteria
Children who have previously experienced spontaneous pain.
A tooth that is clinically nonvital and has a pus discharge.
Teeth with continuous bleeding after coronal pulp tissue removal but good coronal structure. Deciduous teeth with at least two-thirds of root length.
Exclusion Criteria
Teeth with necrotic pulps and radiolucency in the furcation area are advised for extraction.
Primary teeth with root resorption of more than half of the total root length.
Obliterated root canals.
Within the past 2 months, the child had any systemic sickness, medically compromising circumstances, or had taken antibiotics.
A total of 60 primary teeth were selected from 60 children and placed into three groups of twenty each. Patients were instructed to pick a chit from a box with material names written on it for randomization. Prior to the commencement of the trial, the parents gave their informed consent.
In the current study, the following groups were formed:
Group I: Irrigation was done with 2% CHX.
Group II: Diode laser was used to irrigate the root canals.
Group III: Irrigation was done with saline.
A single operator carried out the procedure. The rubber dam was placed after local anesthesia. In order to access the tooth's root canal and remove any cavities, the round bur with a high-speed handpiece was used under continuous irrigation with sterile distilled water. A sterile barbed broach was put into the tooth root canal before any predisinfection sample is collected, the extirpation of pulp done, then the paper point was inserted into the root canal to relax for 30 seconds after inserting into the root canal. The paper point was transferred immediately into the container containing 1 mL sodium thioglycolate medium, which serves as a transport medium for 30 seconds.6
Samples were collected from each of the three root canals for standardization. Using sterile K files, cleaning and shaping of the canals was done. Root canals in group I were irrigated with 2% CHX, group II root canals with diode laser, and group III with saline.
Group II's root canal irrigation procedure was done four times for 5 seconds using a flexible fiber tip of a diode laser with a 200 m diameter (Denlase, 1.2 Watt) in the inbuilt mode of root canal sterilization. To avoid damaging the periapical region after the first irrigation, the fiber was placed into the root canal 1 mm short of the apex.
Under continual recessing circular motions, from the root canal's apical to coronal ends, the laser fiber is introduced. The laser cycles were separated by a 60 second interval of 5 seconds each. During laser irradiation, both the patient and the operator were wearing safety glasses.1,6
The absorbent paper tip was inserted into the root canal and left to rest after completing cleaning and shaping the canals again. The paper tip was removed after 30 seconds and placed immediately into the sterile sample collecting container. After that, both predisinfection and postdisinfection samples were sent to a microbiological lab.
The culturing was done at the Lenora Institute of Dental Sciences, Department of Microbiology. All of the obtained samples were vortexed before being incubated at 37°C for 2 hours. A micropipette was used to plate 10 µL of the material, which was subsequently placed on blood agar plates with a calibrated loop. The bacterial colonies on the labeled agar plates were counted after being incubated and cultured for 24–48 hours at 37°C. Both before and after the disinfection operation, CFUs were measured (Figs 1 to 3). The colony formation percentage decrease was measured, recorded, and tabulated.
Figs 1A and B.

Pre and postdisinfection with CHX
Figs 3A and B.

Pre and postdisinfection with saline
Figs 2A and B.

Pre and postdisinfection with diode laser
Results
Table 2 shows the predisinfection and postdisinfection descriptive statistics of the three groups, namely group I (CHX), group II (diode laser), and group III (saline) with equally distributed sample size, that is, (n = 20), which shows the mean values for all the three groups, among the predisinfected samples for group I the mean value is 56.1, 14.27 is the standard deviation, the mean for group II 56.30 and the standard deviation is 18.70, and for group III the mean value is 60.30, and the standard deviation is 17.9.
Table 2.
Comparison of the mean CFU of predisinfected and postdisinfected samples of three groups
| Groups | N | Mean CFU/mL | Standard deviation | |
|---|---|---|---|---|
| Predisinfection | Group I CHX | 20 | 56.1000 | 14.27512 |
| Group II diode laser | 20 | 56.3000 | 18.70013 | |
| Group III saline | 20 | 60.3000 | 17.98274 | |
| Total | 60 | 45.4000 | 24.19637 | |
| Postdisinfection | Group I CHX | 20 | 26.1000 | 17.06613 |
| Group II diode laser | 20 | 22.4000 | 19.81068 | |
| Group III saline | 20 | 55.8000 | 18.64234 | |
| Total | 60 | 34.7667 | 23.65097 |
Postdisinfection samples for group I, the mean value is 26.10, group II's mean value is 22.4 and its standard deviation is 19.81; group III's mean value is 55.80 and its standard deviation is 17.0; group III's mean value is 55.80 and in its standard deviation is 18.6, respectively, which shows the reduction of the microbial between the predisinfected and postdisinfected samples.
Table 3 shows the comparison using the Mann–Whitney U test, an intergroup comparison was made, and statistically significant differences were found between group I and group III (CHX and saline) and groups II and III (diode laser and saline) (p < 0.01) where the group I and group II (CHX and diode laser) showed the nonsignificant result (p < 0.092).
Table 3.
Intergroup comparison of postdisinfection samples for group I (CHX), group II (diode laser), and group III (saline)
| Postdisinfection (group I CHX and group II diode laser) | Postdisinfection (group I CHX and group III saline) | Postdisinfetion (group II diode laser and group III saline) | |
|---|---|---|---|
| Mann–Whitney U | 138.000 | 52.000 | 46.000 |
| Wilcoxon W | 348.000 | 262.000 | 256.000 |
| Z | −1.685 | −4.013 | −4.176 |
| p-value | 0.092 | 0.000 HS | 0.000 HS |
Discussion
The establishment of an adequate level of disinfection in the root canals is important to the implementation of successful pulp therapy in primary teeth. Because a large amount of the diseased root canal remains undisturbed, disinfection with simply mechanical equipment is not viable. Dentinal tubules and accessory canals contain necrotic pulpal tissue and dentin debris.1
Shaping with instruments of the root canal system creates an amorphous layer of debris which includes dentinal chips, microorganisms, and their byproducts. The smear layer will occlude and close the orifices of the dentinal tubules, thus preventing or delaying the action of irrigants and filling materials from immediate contact with the root surface dentin. Over a period of time, the loosely attached smear layer may disintegrate by the action of bacteria and their byproducts, leading to microleakage and reinfection. After the smear layer is removed, biocompatible irrigation solutions successfully eradicate microorganisms and their products, assisting the disinfection process for organic waste.1
Chlorhexidine (CHX)'s efficacy as an antiplaque treatment has been demonstrated in a number of in vivo and in vitro experiments. The clinical reaction to CHX is dosage-dependent; frequency and concentration are critical in determining the clinical response. The recommended daily dose of CHX as a mouth rinse is 20 mg twice a day; however, equal levels of plaque inhibition can be reached with larger volumes of lower concentrations. Several investigations have shown that a lower concentration of CHX is beneficial. It was discovered that the bacteriostatic effect lasted for 12 hours.
The controlled release mechanism is credited with CHX's substantivity. The amount of CHX released is regulated and controlled by the presence of cyclodextrin. The more cyclodextrin there is, the more CHX is released gradually. Microfibrillated cellulose may also be used to build a controlled release mechanism from cellulosic substrates.
The mechanism of action of CHX is a matter of considerable debate. It has long been assumed that CHX is attached to the mucosal surfaces of the mouth and gradually releases over time. Jenkins et al. 1988, on the other hand, cast doubt on this mechanism, claiming that the main activity of CHX is due to the release of tooth-bound CHX rather than its oral retention or early bactericidal effects. One cation of CHX molecules may bind to the pellicle, leaving the other free to interact with bacteria colonizing the tooth surface. As a result, the process of bacterial suppression is carried out by CHX on the tooth surface.7
The use of diode lasers in root canal therapy has increased in recent years, owing to the lasers’ antibacterial properties. The use of lasers in conservative dentistry and dental procedures has increased the likelihood of a satisfactory treatment outcome. The diseased pulp tissue and layers of root canal dentin may only be removed to a limited amount during traditional root canal therapy. Chemical irritants are only effective in dentin layers right near to the canal wall, whereas root canal architecture restricts the amount of mechanical preparation. Bacteria can penetrate the peri luminal dentin up to 1000 µm whereas chemical disinfectants have a maximum penetration depth range of about 100–130 µm.8,9
In the present study, 2% CHX solution, saline, and diode laser irradiation were done in the primary molar teeth root canals to know the efficacy of the irrigant, which is similar to the study done by Leonardo et al.10 where the authors concluded that because of its intracanal antibacterial action, 2% CHX gluconate can be utilized as an irrigating solution in root canals.
In another study conducted by Kaiwar et al.,11 a 980 nm diode laser's ability to kill germs that have invaded dentin and so raise the success rate of endodontic therapy was concluded. All of the obtained samples were vortexed before being incubated at 37°C for 2 hours. A micropipette was used to plate 10 µL of the material, which was subsequently placed on blood agar plates with a calibrated loop. The labeled agar plates were incubated anaerobically in the anaerobic jar under anaerobic conditions using Gas Pack at 37°C for 24–48 hours.
According to a study by Pazelli et al.,12 deciduous teeth's root canals with necrotic pulp and chronic periapical lesions displayed a high level of microorganisms and polymicrobial infection, with anaerobic bacteria predominating.
The microbial CFUs were counted using a digital colony counter for accurate results and to reduce the time. CFU/mL was measured before and after the use of the disinfection procedure. The percentage reduction in the microbial colony formation was measured, recorded, and tabulated.
The result of this study had shown the mean CFU of predisinfected samples of all three groups were high initially, and the mean CFU of all the postdisinfected samples was decreased, as shown in Table 1 and Figure 4. In the current study, the mean value of group I (CHX) in predisinfected sample was 56.1, group II (diode laser) was 56.3, and in group III (saline) was 60.3, the mean value of postdisinfected samples in group I (CHX) was 26.0, in group II (diode laser) 22.4 and group III (saline) 55.8, respectively.
Fig. 4.
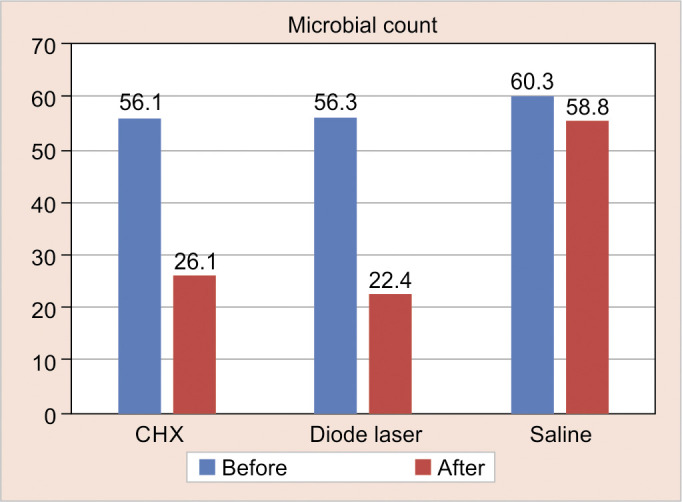
Mean comparison of predisinfection and postdisinfection samples of three groups
The intergroup comparison of the present study showed statistically significant results (p < 0.000) shown in the postdisinfection group between the CHX and saline, diode laser, and saline. The results obtained in the present study can be correlated by the study done by Jain et al.,13 in which they found that on the intergroup comparison, a statistically significant difference was found between the saline and CHX group. Another study conducted by Louwakul and Prucksathamrongkul14 conducted a study at 6, 12, and 18 months, the NSS group's overall success rates were, respectively, 83, 93, and 97%. At 6, 12, and 18 months, the overall success rates in the CHX group were 100, 97, and 93%, respectively.
Similar statistically significant results were found when the 2% CHX and saline were used for the irrigation of the root canals in primary molars in the present study.
Ruiz-Esparza et al.15 observed a statistically significant difference in favor of 2% CHX gluconate when compared with saline. The study conducted by Walia et al.6 showed a statistically significant difference between the diode laser and saline groups. The mean reduction percentage in the diode laser group was 20.00 and in the saline group was 11.0, and the p-value was 0.004, respectively.
This can be correlated with the studies conducted by Sandini et al.,16 Walia et al.,6 and Ashofteh et al.17 In contrast, a study conducted by AA et al.18 results shows the highest change in the mean value percentage of the diode laser group when compared to the 2% CHX group. In comparison to the other groups, the diode laser disinfection was determined to be superior showing a total viable bacterial count.
Diode laser irradiation's stronger antibacterial effect could be ascribed to its deeper penetration when compared to a chemical disinfectant's insufficient ability to penetrate. According to this study's findings, disinfection with 2% CHX and diode laser in the primary tooth root canals dramatically reduced the microbial colony count, with the diode laser is more effective than 2% CHX. A diode laser is more efficient than 2% CHX. Irradiation with a diode laser can be an alternate method for disinfecting primary teeth root canals. Clinical research including root canal procedures on young children's teeth using a bigger sample size is also recommended.
Orcid
B R Kumar https://orcid.org/0000-0002-6532-3113
Punithavathy Naren https://orcid.org/0000-0002-0232-4055
Satyam Martha https://orcid.org/0000-0003-4739-3000
Mythraiye Raparla https://orcid.org/0000-0001-8942-8553
Footnotes
Source of support: Nil
Conflict of interest: None
References
- 1.Naik RG, Raviraj GA, Yavagal CM, et al. Diode lasers for pediatric endodontics: state-of-the-art! J Dent Lasers. 2017;11:7–13. doi: 10.4103/jdl.jdl_1_17. [DOI] [Google Scholar]
- 2.Senthil B, Gurunathan D, Vasantharajan M, et al. Primary tooth root canal irrigants - a review. Int J Pure Appl Math. 2018;120(5):565–589. [Google Scholar]
- 3.Ramachandra JA, Nihal NK, Nagarathna C, et al. Root canal irrigants in primary teeth. World J Dent. 2015;6(3):229–234. doi: 10.5005/jp-journals-10015-1349. [DOI] [Google Scholar]
- 4.Sayadizadeh M, Shojaipour R, Aminizadeh M, et al. Comparing a combination of saline and chlorhexidine with saline as root canal irrigation solutions in pulpectomy of the primary molars in 6-9 years old children, a double blind clinical trial. JDMT. 2019;8(4):174–181. [Google Scholar]
- 5.Root Canal Irrigants and Disinfectants published by the American Association of endodontists. Endodontic Colleagues for Excellence Winter 2011. [Google Scholar]
- 6.Walia V, Goswami M, Mishra S, et al. Comparative evaluation of the efficacy of chlorhexidine, sodium hypochlorite, the diode laser, and saline in reducing the microbial count in primary teeth root canals – an in vivo study. J Lasers Med Sci. 2019;10(4):268–274. doi: 10.15171/jlms.2019.44. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Sajjan P, Laxminarayan N, Kar PP, et al. Chlorhexidine as an antimicrobial agent in dentistry–a review. Oral Health Dent Manag. 2016;15(2):93–100. [Google Scholar]
- 8.Shehab NF, Alshamaa ZA, Taha MYM. Evaluation of antibacterial efficacy of elexxion diode laser 810nm on the infected root canals (in vitro and in vivo study). Int J Dent Sci Res. 2013;1(2):23–27. doi: 10.12691/ijdsr-1-2-1. [DOI] [Google Scholar]
- 9.Preethee T, Kandaswamy D, Arathi G, et al. Bactericidal effect of the 908 nm diode laser on Enterococcus faecalis in infected root canals. J Conserv Dent. 2012;15(1):46–50. doi: 10.4103/0972-0707.92606. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Leonardo MR, Tanomaru Filho M, Silva LA, et al. In vivo antimicrobial activity of 2% chlorhexidine used as a root canal irrigating solution. J Endod. 1999;25(3):167–171. doi: 10.1016/s0099-2399(99)80135-6. [DOI] [PubMed] [Google Scholar]
- 11.Kaiwar A, Usha HL, Meena N, et al. The efficiency of root canal disinfection using a diode laser: in vitro study. Indian J Dent Res. 2013;24(1):14–18. doi: 10.4103/0970-9290.114916. [DOI] [PubMed] [Google Scholar]
- 12.Pazelli LC, Freitas AC, Ito IY, et al. Prevalence of microorganisms in root canals of human deciduous teeth with necrotic pulp and chronic periapical lesions. Pesqui Odontol Bras. 2003;17(4):367–71. doi: 10.1590/s1517-74912003000400013. [DOI] [PubMed] [Google Scholar]
- 13.Jain P, Yeluri R, Garg N, et al. A comparative evaluation of the effectiveness of three different irrigating solution on microorganisms in the root canal: an invivo study. Journal of clinical and diagnostic research. J Clin Diagn Res. 2015;9(12):ZC39–ZC42. doi: 10.7860/JCDR/2015/13133.6991. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Louwakul P, Prucksathamrongkul W. The effect of 2% chlorhexidine as root canal irrigant in pulpectomies of primary molars. Pediatric Dent. 2012;34(7):e192–e196. [PubMed] [Google Scholar]
- 15.Ruiz-Esparza CL, Garrocho-Rangel A, Gonzalez-Amaro AM, et al. Reduction in bacterial loading using 2% chlorhexidine gluconate as an irrigant in pulpectomized primary teeth: a preliminary report. J Clin Pediatric Dent. 2011;35(3):265–270. doi: 10.17796/jcpd.35.3.y052311j23617837. [DOI] [PubMed] [Google Scholar]
- 16.Sandini A, Meidyawati R, Npa DA. The antibacterial effect of a diode laser used as an adjunct irrigant on clinical isolate of enterococcus faecalis biofilm (In vitro). Int J Appl Pharmaceut. 2017;9(2):103–106. [Google Scholar]
- 17.Ashofteh K, Sohrabi K, Iranparvar K, et al. In vitro comparison of the antibacterial effect of three intracanal irrigants and diode laser on root canals infected with Enterococcus faecalis. Iranian journal of microbiology. 2014;6(1):26–30. [PMC free article] [PubMed] [Google Scholar]
- 18.AA M, YS EB, FI B, et al. Comparative evaluation between chlorhexidine and laser in root canal sterilization in pulpectomy of primary teeth. Al-Azhar J Dent Sci. 2018;21(5):475–479. doi: 10.21608/AJDSM.2018.71688. [DOI] [Google Scholar]