

Abstract
Anatomic lateral ankle ligament reconstruction using free tendon graft with osseous tunnels has become a popular technique for revision reconstruction of the lateral ankle ligaments. With the procedure’s burgeoning popularity, an accompanying increase in postoperative complications is likely to occur. We report on one such complication: traumatic distal fibula fracture through the transosseous tunnels.
Keywords: lateral ankle ligament reconstruction, complications, ankle instability, fibular tunnel, ankle fracture
Commentary: A case report about a fracture through the tunnels used for allograft reconstruction of the lateral ankle ligmants. This uncommon complication can occur if tunnels are not well planned with respect to the location of the suture anchors from the previous repair.
Introduction
Lateral ankle instability that has failed conservative management is commonly treated with anatomic repair of the anterior talofibular (ATFL) and/or calcaneofibular ligaments (CFL) using the modified Broström or Karlsson techniques.1,5,12,15,17,20,21 These procedures have been shown to be effective in 70% to 97% of patients. 11 When instability persists despite anatomic repair, many surgeons turn to anatomic lateral ankle ligament reconstruction with autogenous or allogenic tendons. Several techniques have been described and most require the creation of two transosseous tunnels in the distal fibula, one for the ATFL and one for the CFL.2,4,7,13,14 The popularity of these procedures has been increasing over the last decade with good success reported in terms of high patient satisfaction postoperatively and decreased ankle instability with improved talar tilt and ligamentous laxity.8,9,19,23,25 With this increasing popularity has come increased risk of postoperative complications. One potential problem in the use of this procedure for revision surgery after anatomic suture anchor-based repair is the proximity of these tunnels to each other and to the previously placed suture anchors. This may create a stress riser in the distal fibula and the opportunity for fracture. Tunneled tendon grafts have been safely used in many ligament reconstruction surgeries,16,22,24,26,27 but there are a number of differences between anatomic lateral ankle ligament reconstruction and other tunneled ligament reconstructions: (1) the size of the tunnels relative to the size of the distal fibula (usually 5-6-mm tunnels), (2) the proximity of the 2 tunnels (the center of the origin of the ATFL and CFL are separated by only 1.6 mm), 6 and (3) the frequent existence of suture anchors from the previous repair adjacent to the tunnels. Any of these factors may predispose the anatomic lateral ankle ligament reconstruction to complications. However, little has been written about the potential complications arising from distal fibular tunnels used in anatomic lateral ankle ligament reconstruction.
Case Report
We report on the case of a 34-year-old woman with an extensive history of ankle injury and instability. At age 17, she experienced multiple ankle sprains while playing soccer, resulting in functional instability and causing her to stop competitive play. Her instability was managed nonoperatively until 2011 when she elected to undergo an ankle arthroscopy with microfracture of a medial talar dome osteochondral lesion, excision of the lateral process of the talus, and modified Broström lateral ankle ligament reconstruction of the ATFL. The surgery was uncomplicated and she had an uneventful postoperative course. After the procedure, she continued to have lateral ankle instability symptoms and in 2012 underwent revision surgery with anatomic allograft reconstruction using a cadaveric ligament through a distal fibular tunnel. The surgery was without complication and she did well for 2 years until her most recent injury.
The patient presented to our emergency department at the age of 34 with right ankle pain, swelling, and deformity after falling down several steps. She was found to have a distal fibular fracture and was placed in a walking boot for follow-up in the orthopedic clinic as an outpatient. She was then seen in the orthopedic clinic almost 2 weeks after her injury. Radiographs taken in the clinic demonstrated a transverse, mildly displaced fracture involving the right distal fibula through the distal fibular tunnel that had been used for anatomic allograft lateral ankle ligament reconstruction (Figure 1). Her medical history was significant only for a 10-pack-year smoking history and asthma.
Figure 1.
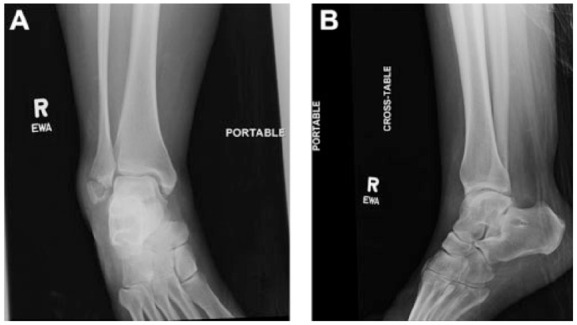
(A) Anteroposterior and (B) lateral radiographs of the right ankle taken postinjury demonstrating a transverse, mildly displaced fracture involving the right distal fibula through the distal fibular tunnel.
Fourteen days after her injury, the patient was taken to the operating room for open reduction and internal fixation of her ankle fracture. A 10-cm longitudinal incision was made over the distal fibula and the fracture site was identified, opened, and cleaned of debris. A fracture was discovered through the sclerotic right limb of the distal fibular tunnel and the allograft ligament was still attached to the distal fragment. The suture anchors from the initial reconstruction were found to be loose in the distal fragment and were removed (Figure 2). The sclerotic bone of the fibular tunnel was curetted back to healthy cancellous bone. The fracture was then reduced with a pointed reduction clamp, and fluoroscopic images were obtained to ensure that the fracture had been adequately reduced. Two K wires were placed as provisional fixation. Next, 10 mL of iliac crest bone marrow was aspirated and mixed with 2 mL of cancellous bone harvested from the calcaneus. The bone graft was impacted into the anterior distal fibular defect and the periosteum was then closed over the fracture site and bone graft. A 5-hole distal fibula periarticular locking plate was applied and fixed with 3 locking screws distally and 3 locking screws proximally (Figure 3).
Figure 2.
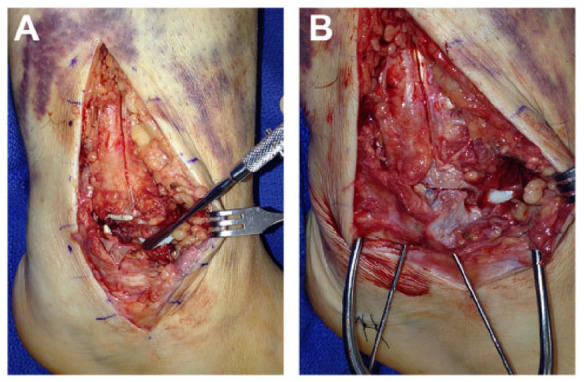
Intraoperative photographs showing (A) the fracture through the distal fibular tunnel with the 2 suture anchors in place. The ligament graft was found to be intact and can be seen at the tip of the elevator. The anchor for the ATFL was grossly loose and became separated from the distal fragment during opening of the fracture site. It was accidentally replaced upside-down before obtaining this photograph. (B) The fracture following reduction and temporary pin fixation. The intact ligament graft can be seen just distal (inferior) to the fracture line and anterior anchor defect.
Figure 3.

Intraoperative fluoroscopic images showing (A) The distal fragment reduced and held with a clamp, (B) mortise view, and (C) lateral view of final reduction and fixation.
The postoperative protocol consisted of 3 weeks nonweightbearing in a short leg cast and then 3 weeks nonweightbearing in a walking boot. Radiographs taken 6 months after surgery (Figure 4) showed consolidation of the fracture and healing of the bone tunnels. The patient was weaned from the boot into a stirrup splint inside a shoe and began physical therapy. At 3 months after surgery, she had no pain or instability and she was allowed to return to all activities. The patient’s only complication was some irritation secondary to the hardware rubbing along her shoe. A moleskin was fashioned to relieve the rubbing and her symptoms improved after a change in her footwear, allowing her hardware to remain in place.
Figure 4.
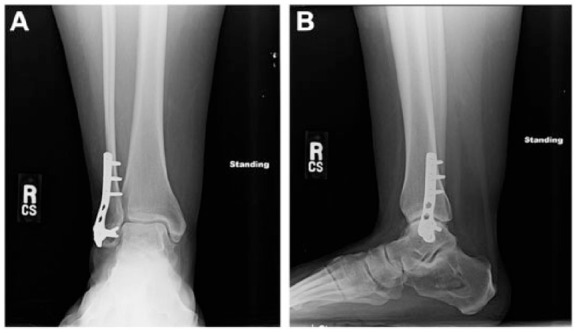
(A) Anteroposterior and (B) lateral radiographs of the right ankle taken 6 months after surgery showing reduction of the distal fibular fracture and improved alignment with distal fibular periarticular locking plate in place.
Discussion
Anatomic graft reconstruction has become a common procedure as both a primary and secondary technique for repair of lateral ankle ligamentous injuries. The success of these surgeries has been well documented8,11; however, reinjury and the use of multiple tunnels for ligamentous repair has been studied less frequently, especially in terms of ankle injuries.
Tunnels have been used extensively for repairs of other joints, including common procedures such as ACL reconstruction and nonanatomic ankle repair. These surgical tunnels for ligament reconstruction have been used in multiple operative procedures in order to create anatomic grafts. Procedures such as those used to repair the ACL have been completed with high rates of success.16,22,24,26,27 More recently, tunnels have begun to be used to repair ligamentous injuries in the ankle, making use of reconstructive tunnels through the distal fibula. These procedures are often required after a previous failed Broström or other procedure, after which patients further injure their lateral ankle or continue to have instability and laxity.10,28 Unlike other reconstructive tunnels, complications and risks associated with fibular tunnels have not been studied or reported, leaving a gap in knowledge as more of these procedures are performed.
The fibula presents a challenge for the creation of safe surgical tunnels without complications and further fracture through the tunnel. The fibula is a bone of less density and strength than those used in other tunnel procedures. 18 The structure of the fibula itself allows for the possibility of injury to the fibula and fractures through weak tunnels with small diameters that are unable to provide proper support. In addition to this, patients will often undergo tunnel procedures after previous surgeries that have failed. These previous surgeries can predispose the patients to sclerotic bone that is unable to properly heal after undergoing a tunnel procedure, as seen in our patient.
Our patient experienced multiple lateral ankle injuries following her first fracture at the age of 17. For 16 years, the patient experienced ankle joint instability and further injuries while attempting conservative management of the joint until finally consenting to surgical treatment. The patient first underwent a modified Broström procedure in 2011 to attempt to correct this laxity. She later underwent an anatomic ligamentous reconstruction using a tunnel through the distal fibula, which then proceeded to a fracture through this tunnel requiring further surgical procedures. The use of a tunnel in a relatively weak bone with smaller diameter, sclerotic changes, and previous injury or surgery can all predispose the patient to further complications. The fracture our patient sustained through her distal fibular tunnel raises concerns for the possibility of other patients experiencing similar fractures and injuries of the tunnel and the need for revision of the ligamentous reconstructions. The true question is how to prevent future similar complications. Tunnel size, placement, and creation in bone that had previously been weakened by anchors are all possible factors leading to fracture. In addition, sclerotic bone and further trauma worsen the chance of fracture. Further study is needed to understand the true cause of fracture and prevent complications in future patients.
Conclusion
Anatomic reconstructions of lateral ankle ligaments using distal fibular tunnels have recently been used successfully for surgical treatment of patients with ankle instability and laxity. These repairs have generally been successful, but research has not looked into the complications that can arise as a result of this operation. Although the Broström procedure has been recommended for repair of lateral ankle ligamentous injuries and often has very favorable outcomes, 3 the use of anatomic fibular tunnels have become more popular, especially to repair failed Broström repairs. The consequences of these tunnels must be better understood as more patients, who are often most at risk for additional complications, undergo the procedure and possibly sustain further injury to the lateral ankle.
Footnotes
This article was originally published as: Roward Z, Latt LD. Fracture through a distal fibular tunnel used for an anatomic lateral ankle ligament reconstruction. Foot Ankle Orthop. 2018 May 9;3(2):2473011418763593. doi:10.1177/2473011418763593.
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. ICMJE forms for all authors are available online.
Funding: The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
- 1. Ahlgren O, Larsson S. Reconstruction for lateral ligament injuries of the ankle. J Bone Joint Surg Br. 1989;71(2):300–303. [DOI] [PubMed] [Google Scholar]
- 2. Bahr R, Pena F, Shine J, Lew WD, Tyrdal S, Engebretsen L. Biomechanics of ankle ligament reconstruction. An in vitro comparison of the Broström repair, Watson-Jones reconstruction, and a new anatomic reconstruction technique. Am J Sports Med. 1997;25(4):424–432. [DOI] [PubMed] [Google Scholar]
- 3. Baumhauer JF, O’Brien T. Surgical considerations in the treatment of ankle instability. J Athl Train. 2002;37(4):458–462. [PMC free article] [PubMed] [Google Scholar]
- 4. Boyer D, Younger A. Anatomic reconstruction of the lateral ligament complex of the ankle using a gracilis autograft. Foot Ankle Clin. 2006;11(3):585–595. [DOI] [PubMed] [Google Scholar]
- 5. Broström L. Surgical treatment of “chronic” ligament ruptures. Acta Chir Scand. 1966;132(5):551–565. [PubMed] [Google Scholar]
- 6. Burks RT, Morgan J. Anatomy of the lateral ankle ligaments. Am J Sports Med.1994;22(1):72–77. [DOI] [PubMed] [Google Scholar]
- 7. Caprio A, Oliva F, Treia F, Maffuli N. Reconstruction of the lateral ankle ligaments with allograft in patients with chronic ankle instability. Foot Ankle Clin. 2006;11(3):597–605. [DOI] [PubMed] [Google Scholar]
- 8. Colville MR. Surgical treatment of the unstable ankle. J Am Acad Orthop Surg. 1998;6(6):368–377. [DOI] [PubMed] [Google Scholar]
- 9. Coughlin MJ, Schenck RC, Grebing BR, Treme G. Comprehensive reconstruction of the lateral ankle for chronic instability using a free gracilis graft. Foot Ankle Int. 2004;25(4):231–241. [DOI] [PubMed] [Google Scholar]
- 10. Dierckman BD, Ferkel RD. Anatomic reconstruction with a semitendinosus allograft for chronic lateral ankle instability. Am J Sports Med. 2015;43(8):1941–1950. [DOI] [PubMed] [Google Scholar]
- 11. DiGiovanni CW, Brodsky A. Current concepts: lateral ankle instability. Foot Ankle Int. 2006;27(10):854–866. [DOI] [PubMed] [Google Scholar]
- 12. Gould N, Seligson D, Gassman J. Early and late repair of lateral ligament of the ankle. Foot Ankle. 1980;1(2):84–89. [DOI] [PubMed] [Google Scholar]
- 13. Guillo S, Archbold P, Perera A, Bauer T, Sonnery-Cottet B. Arthroscopic anatomic reconstruction of the lateral ligaments of the ankle with gracilis autograft. Arthrosc Tech. 2014;22(3):e593–e598. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14. Guillo S, Cordier G, Sonnery-Cottet B, Bauer T. Anatomical reconstruction of the anterior talofibular and calcaneofibular ligaments with an all-arthroscopic surgical technique. Orthop Traumatol Surg Res. 2014;100(8 suppl):S413–S417. [DOI] [PubMed] [Google Scholar]
- 15. Hamilton WG, Thompson FM, Snow SW. The modified Broström procedure for lateral ankle instability. Foot Ankle. 1993;14(1):1–7. [DOI] [PubMed] [Google Scholar]
- 16. Helito CP, Bonadio MB, Demange MK, et al. Functional assessment of combined reconstruction of the anterior cruciate ligament and posterolateral corner with a single femoral tunnel: a two-year minimum follow-up. Int Orthop. 2015;39(3):543–548. [DOI] [PubMed] [Google Scholar]
- 17. Hennrikus WL, Mapes RC, Lyons PM, Lapoint JM. Outcomes of the Chrisman-Snook and modified-Broström procedures for chronic lateral ankle instability. A prospective, randomized comparison. Am J Sports Med. 1996;24(4):400–404. [DOI] [PubMed] [Google Scholar]
- 18. Ide Y, Matsunaga S, Harris J, O’ Connell D, Seikaly H, Wolfaardt J. Anatomical examination of the fibula: digital imaging study for osseointegrated implant installation. J Otolaryngol Head Neck Surg. 2015;44:1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19. Jung HG, Kim TH, Park JY, Bae EJ. Anatomic reconstruction of the anterior talofibular and calcaneofibular ligaments using a semitendinosus tendon allograft and interference screws. Knee Surg Sports Traumatol Arthrosc. 2012;20(8):1432–1437. [DOI] [PubMed] [Google Scholar]
- 20. Karlsson J, Bergsten T, Lansinger O, Peterson L. Reconstruction of the lateral ligaments of the ankle for chronic lateral instability. J Bone Joint Surg Am. 1988;70(4):581–588. [PubMed] [Google Scholar]
- 21. Karlsson J, Bergsten T, Lansinger O, Peterson L. Surgical treatment of chronic lateral instability of the ankle joint. A new procedure. Am J Sports Med. 1989;17(2):268–273; discussion 273-274. [DOI] [PubMed] [Google Scholar]
- 22. Matava MJ, Arciero RA, Baumgarten KM, et al. Multirater agreement of the causes of anterior cruciate ligament reconstruction failure: a radiographic and video analysis of the MARS cohort. Am J Sports Med. 2015;43(2):310–319. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23. Miller A, Raikin S, Ahmad J. Near-anatomic allograft tenodesis of chronic lateral ankle instability. Foot Ankle Int. 2013;34(11):1501–1507. [DOI] [PubMed] [Google Scholar]
- 24. Sinha S, Naik AK, Meena D, Jain VK, Arya RK. Creation of femoral tunnel by outside-in technique for ACL reconstruction: an analysis. Arch Orthop Trauma Surg. 2014;134(12):1709–1716. [DOI] [PubMed] [Google Scholar]
- 25. Takao M, Oae K, Uchio Y, Ochi M, Yamamoto H. Anatomical reconstruction of the lateral ligaments of the ankle with a gracilis autograft: a new technique using an interference fit anchoring system. Am J Sports Med. 2005;33(6):814–823. [DOI] [PubMed] [Google Scholar]
- 26. Vališ P, Sklenský J, Repko M, Rouchal M, Novák J, Otaševič T. Most frequent causes of autologous graft failure in anterior cruciate ligament replacement [in Czech]. Acta Chir Orthop Traumatol Cech. 2014;81(6):371–379. [PubMed] [Google Scholar]
- 27. Youm YS, Cho SD, Lee SH, Youn CH. Modified transtibial versus anteromedial portal technique in anatomic single-bundle anterior cruciate ligament reconstruction: comparison of femoral tunnel position and clinical results. Am J Sports Med. 2014;42(12):2941–2947. [DOI] [PubMed] [Google Scholar]
- 28. Yong R, Lai KW, Ooi LH. Ankle lateral ligament reconstruction for chronic instability. J Orthop Surg (Hong Kong). 2015;23(1):62–65. [DOI] [PubMed] [Google Scholar]