

Abstract
Background
The use of beta-tricalcium phosphate (beta-TCP) in dental surgery is limited owing to its rapid absorption compared to mixed formulations of hydroxyapatite. However, newly developed pure beta-TCP crystals have demonstrated slow absorption; hence, they last longer within the defect and act as a scaffold until new bone formation. The oral environment is unique and can prove unfavorable for bone grafts due to the high infection rate in the oral cavity and the fragile condition of the oral mucosa. The aim of this study was to evaluate the feasibility of using pure beta-TCP bone grafts in various dental treatments.
Methods
Panoramic X-ray images of 25 patients who underwent bone grafting during dental surgery were analyzed. A specially treated pure beta-TCP crystal, Neo Bone® (Neo Bone®, SN Biologics Co., Ltd, Seoul, Korea), was used in this study. The bone density at the graft site was compared with that of the surrounding bone using the ImageJ software (Wayne Rasband, NIH USA).
Results
Six months after surgery, the bone graft density was similar to that of the surrounding bone in 20 patients and increased in 5 patients. No adverse effects, such as infection, dehiscence, or graft failure, were observed.
Conclusion
The newly developed pure beta-TCP crystal was slowly absorbed and served as support until new bone formation at the defect site, thus demonstrating its potential for use in various oral conditions requiring bone grafting.
Keywords: Odontogenic cyst, Socket preservation, Sinus bone graft, Bone graft, Beta-tricalcium phosphate
Background
Bone graft materials, such as autografts, allografts, and synthetic substitutes, are widely used in dental surgery to promote bone healing and new bone formation. Although autografts have been used in most cases [1, 2], there is an increasing demand for other bone graft sources due to donor site morbidity and grafted bone volume limitations [2–5]. Xenografts and allografts can be used as alternatives for autografts, but these materials have been associated with cross-infection, low bone regeneration capacity (compared to autografts), and high costs. The use of synthetic materials has gained popularity, mainly because it eliminates the possibility of disease transmission from the donor [6].
Several synthetic materials, including polymers and ceramics, have been proposed for bone grafting. Among them, calcium phosphate ceramics, particularly hydroxyapatite (HA), beta-tricalcium phosphate (beta-TCP), and their combinations, are most commonly used [7]. HA is non-degradable and can maintain the volume at the graft site; however, HA grafts cannot be entirely replaced by newly regenerated bone, which is a drawback in some cases, such as dental implant placement at the graft site. On the other hand, beta-TCP is osteoinductive and can provide osteoconduction for bone formation at the graft site. Furthermore, beta-TCP has excellent biocompatibility and biodegradability, thus making it one of the most potent bone graft substitutes. Additionally, beta-TCP can be resorbed by osteoclasts [7], but it is highly brittle and resorbs quickly owing to its interconnected porous structure [8].
Therefore, pure beta-TCP grafts are required to develop a support system that maintains the mechanical strength during bone union while the grafted bone is resorbed and biodegraded at the same rate as that of the newly formed bone.
The requirements for an ideal scaffold include biocompatibility, biodegradability, mechanical strength, adequate porosity, and sufficient pore dimensions. Beta-TCP has good biocompatibility and biodegradability but low mechanical strength due to its porous structure [9].
A specially treated pure beta-TCP crystal, Neo Bone® (Neo Bone®, SN Biologics Co., Ltd, Seoul, Korea), was used in this study. Unlike other pure beta-TCP products, Neo Bone® beta-TCP obtains independent structure support through nanocrystal coating. Consequently, the mechanical limitations of existing pure beta-TCP were overcome, and the structure was used to facilitate molding in this study (Fig. 1). Nanoparticle treatment maximizes blood supply by improving the surface area and reproducing the structure of cancellous bone; the absorption rate, structure, and mechanical properties are similar to that of human bone (Fig. 2).
Fig. 1.
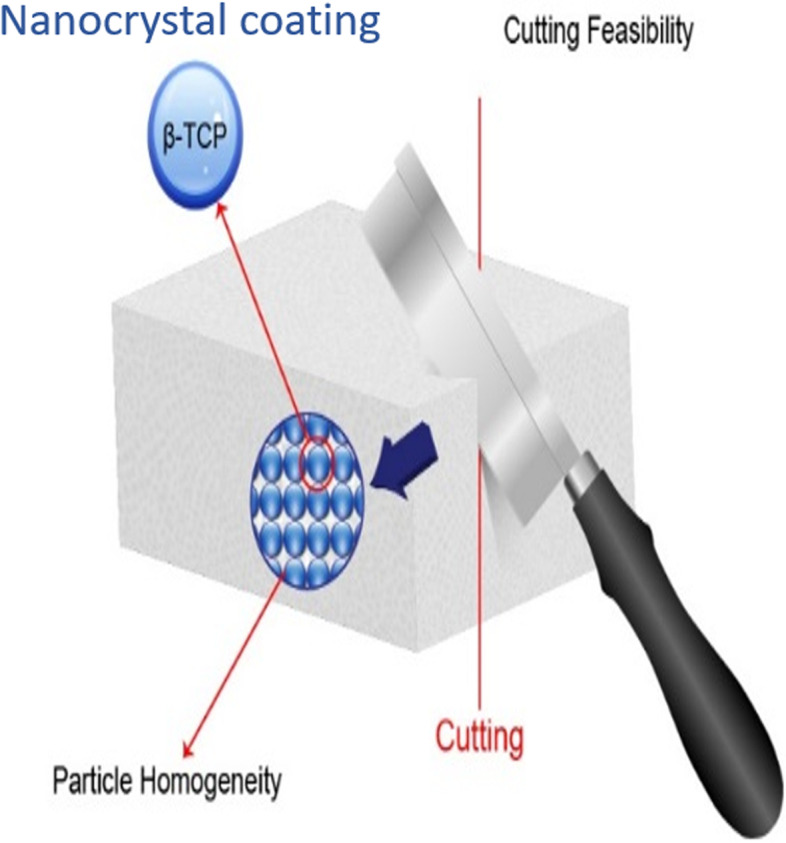
Particle homogeneity can be obtained using nanocrystal coating technology
Fig. 2.
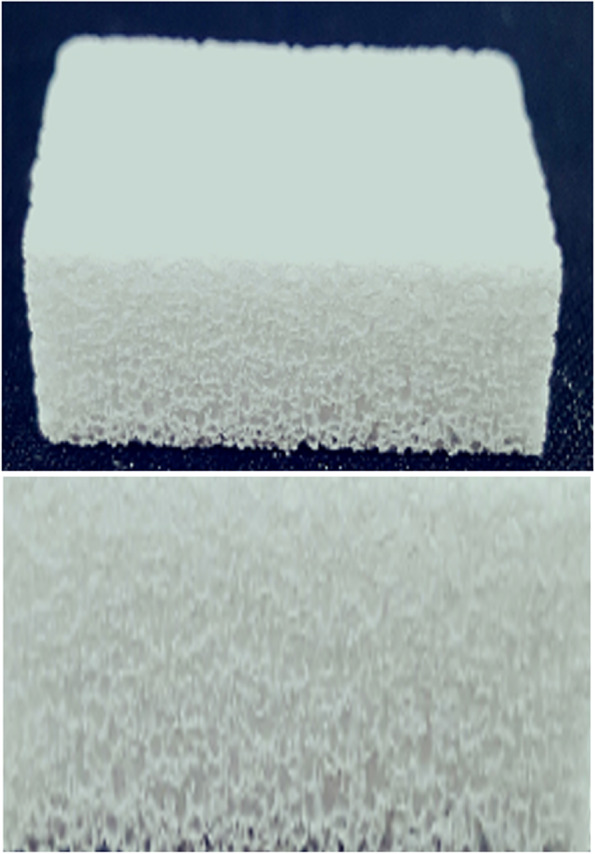
Structure of Neobone. It has a similar structure to the human cancellous bone and improves blood supply
Bone grafting for dental treatments is usually performed using the intraoral approach by elevating the oral mucosa. However, the condition of the oral cavity is not favorable for grafting due to the presence of large numbers of pathologic bacteria and the mechanical forces from food chewing. Moreover, the oral mucosa on the graft site is generally thin and fragile. In addition, the biocompatibility of the pure beta-TCP with the oral mucosal tissues remains unclear. Therefore, the grafts in the oral cavity might be more vulnerable to infection than those used for orthopedic treatment.
This study aimed to evaluate the feasibility of using a pure beta-TCP product for intraoral bone grafting in various dental treatments.
Methods
The study protocol was reviewed and approved by the institutional review board of the Asan Medical Center, Seoul, Korea (IRB approval No. S2021-2426–0001).
The density of the bone graft material was evaluated and analyzed in 25 bone graft patients after surgery using the pure beta-TCP crystal, Neo Bone® (SN Biologics Co.). The “relative bone density” measurement was used to evaluate the healing process after using the bone graft material, wherein
Two panoramic X-ray imaging equipment (Promax, Planmeca, Finland, and CS 8100, Carestream Dental, USA) were used to evaluate the bone grafting sites. The regions of interest (ROI) were determined by free hand selection using the ImageJ software (Wayne Rasband, NIH USA) [10].
Measurement of bone density and area
The relative bone density was determined by calculating the bone density of the ROI relative to that of the normal bone tissue around the graft. The freehand selection measurement method has a high possibility of error depending on the measurer; therefore, the standard operating procedure method proposed by Manuel was used in this study [10]. This method is free of cost, simple, and easy to compare radiography taken with dental clinic.
One investigator evaluated the repeatability of the measurement by taking re-measurements 2 weeks after the first measurement. The relative bone density was calculated using panoramic radiographs immediately and 6 months after surgery. The value for each sinus was calculated in the case of a bilateral maxillary sinus.
As shown in Fig. 3, the densities of the bone graft site and the bone around the site were calculated by marking them on the panoramic radiograph during the 1st visit after surgery. (The area and mean gray values of Fig. 3 are shown in Table 1.) A membrane was applied to prevent the loss of bone graft material, and the graft material was maintained in all the patients.
Fig. 3.
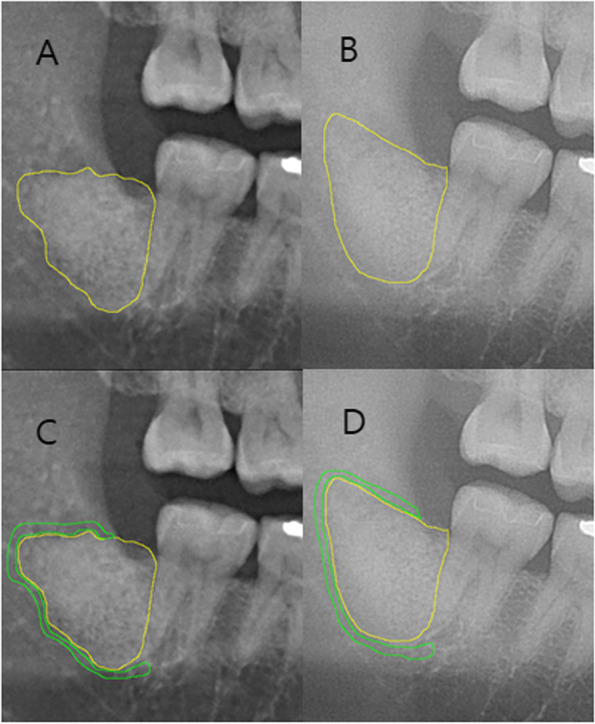
Method for measuring bone density using panoramic radiographs. A Postoperation 1st visit defect region. B Postoperation 2nd visit defect region. C Postoperation 1st visit surrounding bone. D Postoperation 2nd visit surrounding bone
Table 1.
Results of Fig. 3
| Area | Mean | Min | Max | |
|---|---|---|---|---|
| A | 19,415 | 132.019 | 72 | 167 |
| C | 5236 | 106.779 | 70 | 145 |
| B | 21,593 | 163.068 | 116 | 189 |
| D | 6054 | 146.206 | 115 | 174 |
Management of patients
To prevent infection and complications after surgery, the primary closure was performed in all cases. In addition, the antibiotics commonly used after oral surgery, amoxicillin and clavulanic acid, were used three times a day for a week.
Results
Table 2 shows the relative bone densities calculated immediately (1st visit) and 6 months after surgery. The average grafted area in the 25 patients is shown in Table 3. As shown in Table 4, 11 patients received bone grafts after odontogenic cyst enucleation, 7 received them for socket preservation, 4 for sinus augmentation, and 3 for implants. Eleven cases were in the maxilla, and 7 were in the mandible (Table 5).
Table 2.
The average relative bone densities in the 25 patients in this study
| Patient number | 1st visit post-surgery | 6 months after surgery |
|---|---|---|
| Case 1 | 1.071 | 1.182 |
| Case 2 | 0.839 | 1.093 |
| Case 3 | 1.27 | 1.118 |
| Case 4 | 0.89 | 1.039 |
| Case 5 | 1.119 | 1.06 |
| Case 6 | 1.06 | 0.999 |
| Case 7—right | 1.26 | 1.065 |
| Case 7—left | 1.182 | 1.048 |
| Case 8 | 1.061 | 1.017 |
| Case 9—right | 1.595 | 1.531 |
| Case 9—left | 1.417 | 1.225 |
| Case 10 | 1.087 | 1.067 |
| Case 11 | 1.019 | 1.016 |
| Case 12 | 1.149 | 1.274 |
| Case 13 | 1.592 | 1.337 |
| Case 14 | 0.893 | 0.935 |
| Case 15 | 1.066 | 1.098 |
| Case 16 | 0.914 | 1.008 |
| Case 17 | 0.997 | 1.033 |
| Case 18 | 1.03 | 1.083 |
| Case 19 | 1.227 | 1.07 |
| Case 20 | 1.298 | 1.232 |
| Case 21 | 1.002 | 1.001 |
| Case 22 | 1.069 | 1.062 |
| Case 23 | 1.429 | 1.057 |
| Case 24 | 1.231 | 1.004 |
| Case 25 | 1.214 | 1.13 |
| Average | 1.147 ± 0.2 | 1.103 ± 0.13 |
Table 3.
Average bone graft area in the 25 patients
| Patient number | 1st visit | 6 months later | % |
|---|---|---|---|
| Case 1 | 23,360 | 15,366 | 65.78 |
| Case 2 | 10,236 | 11,886 | 116.12 |
| Case 3 | 17,868 | 21,253 | 118.94 |
| Case 4 | 15,501 | 21,253 | 137.11 |
| Case 5 | 22,386 | 21,386 | 95.53 |
| Case 6 | 24,972 | 17,485 | 70.02 |
| Case 7—right | 15,052 | 14,051 | 93.35 |
| Case 7—left | 16,125 | 17,206 | 106.7 |
| Case 8 | 5823 | 5618 | 96.48 |
| Case 9—right | 14,677 | 18,617 | 126.84 |
| Case 9—left | 13,370 | 12,157 | 90.93 |
| Case 10 | 10,740 | 11,773 | 109.62 |
| Case 11 | 9514 | 8772 | 92.2 |
| Case 12 | 26,805 | 18,328 | 68.38 |
| Case 13 | 4041 | 6953 | 172.06 |
| Case 14 | 3123 | 4158 | 133.14 |
| Case 15 | 6035 | 5345 | 88.57 |
| Case 16 | 1841 | 1041 | 56.55 |
| Case 17 | 4837 | 5058 | 104.57 |
| Case 18 | 2617 | 2408 | 92.01 |
| case 19 | 10,154 | 13,251 | 130.5 |
| case 20 | 18,650 | 19,660 | 105.42 |
| case 21 | 14,380 | 11,981 | 83.32 |
| case 22 | 14,153 | 17,988 | 127.1 |
| case 23 | 8914 | 10,835 | 121.55 |
| case 24 | 12,074 | 10,698 | 88.6 |
| case 25 | 14,290 | 8464 | 59.23 |
| Average | 12,650 | 12,333 | 97.5 ± 26.8 |
The % was calculated by dividing the value immediately after surgery by the value 6 months later × 100
Table 4.
Dental surgical procedures where the bone graft was used
| Cases | Number of patients |
|---|---|
| Cyst enucleation | 11 |
| Socket preservation | 7 |
| Sinus bone graft | 4 |
| Implant with bone graft | 3 |
Table 5.
Surgical sites
| Surgical sites | Cases |
|---|---|
| Maxilla | 12 |
| Mandible | 13 |
Twenty patients presented with relative bone density values close to 1, whereas the relative bone densities of 5 patients were further away from 1 (Table 6). In addition, the relative densities of the bone graft materials were increased in 9 and decreased in 16 patients at the 6 months after surgery. The area of the graft site was increased in 13 sites and decreased in 14 sites (Tables 2, 3, 4, 5, and 6).
Table 6.
Changes in bone density
| Changes in bone density | Number of patients |
|---|---|
| Similar | 20 |
| Increased | 5 |
No complications or side effects were observed in any of the patients.
Discussion
Allogeneic, xenogeneic, and synthetic bone have been widely used in dentistry. Among them, synthetic bone has a lower risk of cross-infection and is more competitively priced than the others. However, the clinical use of synthetic bone graft materials is limited because of their structural properties and decreased osteogenic activities [7].
A new synthetic material, beta-TCP, has recently gained popularity owing to its high biocompatibility [11] and osteogenic potential [12, 13]. Nonetheless, it has poor mechanical strength and is easily absorbed [14]; hence, it is usually applied as a mixture with HA to improve the mechanical properties while maintaining the graft volume. HA cannot be replaced with natural bone at the graft site; therefore, a new technology was applied to develop a pure beta-TCP with improved mechanical strength and a lower resorption rate [15, 16].
Neo Bone® is manufactured using the nanocrystal particle treatment method [16], which increases the mechanical strength of the pure beta-TCP by forming uniform particles [17]. Neo Bone® can preserve the high osteogenic potential (osteoconduction and osteoblast activation) of beta-TCP. It ensures high chemical purity and uniformity of the chemical composition and crystal phase by calcifying beta-TCP below the phase transition temperature to minimize the aggregation of raw materials. The micro-crystal coating between the beta-TCP particles guarantees uniformity and improves the mechanical strength and brittleness, so it is not easily broken [17].
Beta-TCP is absorbed by macrophages and multinucleated giant cells [18, 19]. In one study, the volume retention rate of NeoBone® was higher than those of an allogeneic bone graft (survival rate of 80.3% at 6 months after surgery) and a 1:1 mixture of allogeneic and xenogeneic bone (84.1%), thus acting as a scaffold [20]. In another study using conventional pure beta-TCPs, 75.6% of the original graft area was retained 6 months after surgery [20, 21]. Interestingly, 97.5% ± 26.8 of the original graft area remained 6 months after surgery in the current study. This finding indicates that Neo Bone® can achieve preservation of the volume by overcoming the disadvantages of conventional pure beta-TCP grafts. NeoBone® showed a higher volume retention rate 6 months after surgery than the hydroxyapatite and beta-TCP mixture, which retained 82% of the original graft area [17]. Thus, Neo Bone® has served as a support for an extended period until new bone was formed, while the implanted bone was resorbed during the osteosynthesis period. Furthermore, it overcame the clinical weaknesses of existing pure beta-TCP grafts, maintained the volume and height of the bone graft site after surgery, and achieved better volume preservation compared to other bone graft materials.
Conventionally, a mixture of hydroxyapatite and beta-TCP has been used to maintain the volume of the implantation site and improve the mechanical properties [11, 18, 19]. However, conventional synthetic bone to which HA is added has a disadvantage in that the implant must remain in the body for life after bone transplantation. Alternatively, the pure beta-TCP used in the present study not only serves as an adequate scaffold for new bone formation when used alone, but also has the advantage of significantly lowering the possibility of infection caused by the complete absorption of implants at a later point. The findings of the present study indicate that Neo Bone® may be considered as an alternative to a successful bone graft material in various dental surgery cases.
According to the radiological findings, 97.5% ± 26.8% of the Neo Bone® graft area supported volume preservation until 6 months after surgery, and most of the 25 patients had the same or increased relative bone density values. Thus, the graft was gradually replaced by new bone after 6 months.
Histomorphometric analysis to confirm the formation of new bone tissue was not performed for ethical reasons. However, previous studies have reported these findings using histomorphometric analyses of beta-TCP and radiologic evaluations [16, 22].
Okada et al. found that high-purity beta-TCP is safe with excellent osteoconductive properties, even in patients who underwent maxillary sinus augmentation with beta-TCP alone [20] Furthermore, a histological analysis comparing beta-TCP with other materials showed that the rate of new bone formation was significantly increased between 6 months and 1 year, followed by a significant decrease. These findings were corroborated in the present study. Thus, the radiologic data in this study might represent new bone formation in the defect. The relative bone density of the graft was similar to or increased with time when compared to that of the surrounding bone (Table 6). This change in graft density implies that some degree of bone regeneration has progressed into the graft area during the observation period. A retrospective study using a beta-TCP bone graft showed similar results under favorable conditions [23].
Dentoalveolar bone grafting is mainly performed by elevating the oral mucosa in the oral cavity. The oral cavity consists of a large number of bacteria and is exposed to masticatory forces. Furthermore, the mucosa covering the upper part of the graft is mechanically weaker than the skin or muscle layer. These factors increase the likelihood of wound dehiscence at the graft site. Therefore, the infection rate after bone graft during dental treatment is high, and it is expected to be higher in the case of synthetic bone [24]. Accordingly, postoperative systemic antibiotics have been prescribed to reduce infection [25]. No infection or wound dehiscence was observed in the present study; this, Neo Bone® might prove to be biocompatible with the oral mucosa.
The beta-TCP used in this study has the advantage of being able to gradually replace the scaffold with new bone while maintaining its role for a sufficient period of time, unlike conventional beta-TCP. As shown in Fig. 4, it was confirmed that the volume was well maintained up to 6 months after surgery even in CBCT. However, this study has limitations as it did not include histological examination and did not use a control group for retrospective analysis. Therefore, prospective comparative studies with control groups and histological examinations will be necessary in the future.
Fig. 4.

Preoperative and postoperative cone beam CT
Conclusion
In the present study, the specially treated pure-beta TCP, Neo Bone®, could be successfully grafted in various popular clinical dental bone defects. Neo Bone® might be another useful graft option for diverse dentoalveolar bony defects.
Acknowledgements
No acknowledgement.
Abbreviations
- ROI
Regions of interest
- HA
Hydroxyapatite
- TCP
Tricalcium phosphate
- Beta TCP
Beta tricalcium phosphate
Authors’ contributions
YJ Choi, HJ Chang, and MJ Kim collected and analyzed the data. YJ Choi wrote the manuscript. JH Lee and BK Lee participated in the design of this study and revised the manuscript. The authors read and approved the final manuscript.
Funding
No funding source.
Availability of data and materials
Data sharing is not applicable to this article as no data sets were generated or analyzed during the current study.
Declarations
Ethics approval and consent to participate
This study was conducted after approval from the Institutional Review Board of Asan Medical Center (IRB approval No. S2021-2426–0001), and the informed consent was waived.
Consent for publication
This manuscript does not contain any individual person’s identifier (including individual details, images, or videos).
Competing interests
The authors declare that they have no competing interests.
Footnotes
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
References
- 1.McAllister BS, Haghighat K. Bone augmentation techniques. J Periodontol. 2007;78(3):377–396. doi: 10.1902/jop.2007.060048. [DOI] [PubMed] [Google Scholar]
- 2.Yamada M, Egusa H. Current bone substitutes for implant dentistry. J Prosthodont Res. 2018;62(2):152–161. doi: 10.1016/j.jpor.2017.08.010. [DOI] [PubMed] [Google Scholar]
- 3.Bohner M, Santoni BLG, Dobelin N (2020) beta-tricalcium phosphate for bone substitution: Synthesis and properties. Acta Biomater 113:23–41 [DOI] [PubMed]
- 4.Papageorgiou SN, Papageorgiou PN, Deschner J, Gotz W. Comparative effectiveness of natural and synthetic bone grafts in oral and maxillofacial surgery prior to insertion of dental implants: Systematic review and network meta-analysis of parallel and cluster randomized controlled trials. J Dent. 2016;48:1–8. doi: 10.1016/j.jdent.2016.03.010. [DOI] [PubMed] [Google Scholar]
- 5.Sheikh Z, Najeeb S, Khurshid Z, Verma V, Rashid H, Glogauer M. Biodegradable materials for bone repair and tissue engineering applications. Materials (Basel) 2015;8(9):5744–94. doi: 10.3390/ma8095273. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Sheikh Z, Hamdan N, Ikeda Y, Grynpas M, Ganss B, Glogauer M. Natural graft tissues and synthetic biomaterials for periodontal and alveolar bone reconstructive applications: a review. Biomater Res. 2017;21:9. doi: 10.1186/s40824-017-0095-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Bohner M, Santoni BLG, Döbelin N. β-tricalcium phosphate for bone substitution: Synthesis and properties. Acta Biomater. 2020;113:23–41. doi: 10.1016/j.actbio.2020.06.022. [DOI] [PubMed] [Google Scholar]
- 8.Roca-Millan E, Jane-Salas E, Mari-Roig A, Jimenez-Guerra A, Ortiz-Garcia I, Velasco-Ortega E, et al. The application of beta-tricalcium phosphate in implant dentistry: a systematic evaluation of clinical studies. Materials (Basel) 2022;15(2):655. doi: 10.3390/ma15020655. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.YunZhi Shi JL, Lingmin Yu, Zhong LZ, Jiang HB. β-TCP scaffold coated with PCL as biodegradable materials for dental applications. Ceram Int. 2018;44(13):15086–15091. doi: 10.1016/j.ceramint.2018.05.142. [DOI] [Google Scholar]
- 10.M G. Evaluation of ImageJ for relative bone density measurement and clinical application. J Oral Health Craniofac Sci. 2016;1(1):012–21. doi: 10.29328/journal.johcs.1001002. [DOI] [Google Scholar]
- 11.Rosa AL, Brentegani LG, Grandini SA. Hydroxylapatite and tricalcium phosphate implants in the dental alveolus of rats. A histometric study. Braz Dent J. 1995;6(2):103–109. [PubMed] [Google Scholar]
- 12.Knabe C, Koch C, Rack A, Stiller M. Effect of beta-tricalcium phosphate particles with varying porosity on osteogenesis after sinus floor augmentation in humans. Biomaterials. 2008;29(14):2249–2258. doi: 10.1016/j.biomaterials.2008.01.026. [DOI] [PubMed] [Google Scholar]
- 13.Brkovic BM, Prasad HS, Konandreas G, Milan R, Antunovic D, Sandor GK, et al. Simple preservation of a maxillary extraction socket using beta-tricalcium phosphate with type I collagen: preliminary clinical and histomorphometric observations. J Can Dent Assoc. 2008;74(6):523–528. [PubMed] [Google Scholar]
- 14.Cheah CW, Al-Namnam NM, Lau MN, Lim GS, Raman R, Fairbairn P, et al. Synthetic material for bone, periodontal, and dental tissue regeneration: where are we now, and where are we heading next? Materials (Basel) 2021;14(20):6123. doi: 10.3390/ma14206123. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Chappard D, Guillaume B, Mallet R, Pascaretti-Grizon F, Basle MF, Libouban H. Sinus lift augmentation and beta-TCP: a microCT and histologic analysis on human bone biopsies. Micron. 2010;41(4):321–326. doi: 10.1016/j.micron.2009.12.005. [DOI] [PubMed] [Google Scholar]
- 16.Horowitz RA, Mazor Z, Miller RJ, Krauser J, Prasad HS, Rohrer MD. Clinical evaluation alveolar ridge preservation with a beta-tricalcium phosphate socket graft. Compend Contin Educ Dent. 2009;30(9):588–90, 92, 94 passim; quiz 604, 6. [PubMed] [Google Scholar]
- 17.Hyungseok Park JEM, Cho Yong Jin. Radiologic outcome of beta-tricalcium phosphate as a bone substitute in orthopaedic surgery. KJ-HSM. 2019;13(4):133–44. doi: 10.12811/kshsm.2019.13.4.133. [DOI] [Google Scholar]
- 18.Eggli PS, Muller W, Schenk RK. Porous hydroxyapatite and tricalcium phosphate cylinders with two different pore size ranges implanted in the cancellous bone of rabbits. A comparative histomorphometric and histologic study of bony ingrowth and implant substitution. Clin Orthop Relat Res. 1988;232:127–138. doi: 10.1097/00003086-198807000-00017. [DOI] [PubMed] [Google Scholar]
- 19.Renooij W, Hoogendoorn HA, Visser WJ, Lentferink RH, Schmitz MG, Van Ieperen H, et al. Bioresorption of ceramic strontium-85-labeled calcium phosphate implants in dog femora. A pilot study to quantitate bioresorption of ceramic implants of hydroxyapatite and tricalcium orthophosphate in vivo. Clin Orthop Relat Res. 1985;197:272–285. doi: 10.1097/00003086-198507000-00034. [DOI] [PubMed] [Google Scholar]
- 20.Okada T, Kanai T, Tachikawa N, Munakata M, Kasugai S. Long-term radiographic assessment of maxillary sinus floor augmentation using beta-tricalcium phosphate: analysis by cone-beam computed tomography. Int J Implant Dent. 2016;2(1):8. doi: 10.1186/s40729-016-0042-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Kim ES, Moon SY, Kim SG, Park HC, Oh JS. Three-dimensional volumetric analysis after sinus grafts. Implant Dent. 2013;22(2):170–174. doi: 10.1097/ID.0b013e31827f3576. [DOI] [PubMed] [Google Scholar]
- 22.Brkovic BM, Prasad HS, Rohrer MD, Konandreas G, Agrogiannis G, Antunovic D, et al. Beta-tricalcium phosphate/type I collagen cones with or without a barrier membrane in human extraction socket healing: clinical, histologic, histomorphometric, and immunohistochemical evaluation. Clin Oral Investig. 2012;16(2):581–590. doi: 10.1007/s00784-011-0531-1. [DOI] [PubMed] [Google Scholar]
- 23.Harel NMO, Palti A, Ormianer Z (2013) Long-term results of implants immediately placed into extraction sockets grafted with β-tricalcium phosphate: a retrospective study. J Oral Maxillofac Surg 71(2):e63–e8 [DOI] [PubMed]
- 24.Camps-Font O, Figueiredo R, Valmaseda-Castellon E, Gay-Escoda C. Postoperative infections after dental implant placement: prevalence, clinical features, and treatment. Implant Dent. 2015;24(6):713–719. doi: 10.1097/ID.0000000000000325. [DOI] [PubMed] [Google Scholar]
- 25.Esposito M, Grusovin MG, Worthington HV (2013) Interventions for replacing missing teeth: antibiotics at dental implant placement to prevent complications. Cochrane Database Syst Rev 7(7):CD004152 [DOI] [PMC free article] [PubMed]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
Data sharing is not applicable to this article as no data sets were generated or analyzed during the current study.