

Dear Editor,
Mid-dermal elastolysis is a rare acquired disorder characterized by loss of elastic fibers in mid-dermis. It was first reported by Wood in 1977.[1] Elastin provides mechanical strength and elastic recoil properties to the skin. Clinically, it has three variants—type I consisting of fine wrinkles arranged parallel to the skin cleavage lines; type II consisting of small, soft papular lesions made up of tiny perifollicular protrusions, and type III manifests as frank inflammation characterized by reticulate erythema and is more common in men at older age.[2] Lesions are usually seen on trunk and upper extremities. We report a case of type I variant of mid-dermal elastolysis in a male.
A 25-years-old male presented with asymptomatic multiple, fine wrinkled areas over back, chest, and limbs for a duration of six months. There was no history of any other preceding cutaneous disease or inflammation. Patient denied any history of high-risk sexual behavior or of similar complaints in any family member or drug exposure. Examination revealed multiple discrete areas of wrinkling over back, chest, and limbs [Figures 1 and 2] with no follicular prominence. The areas appeared to follow the cleavage lines. There were no areas of sac-like bulging or loose folds of skin, erythema, or scaling seen anywhere on the trunk. To aid in the diagnosis, dermoscopy was performed with Illuco 1100 dermatoscope which showed irregular focal white areas (blue arrow) and accentuated pigment network (black arrow) with wrinkling, widened skin lines, and without vessel involvement [Figure 3]. Skin biopsy revealed tiny broken fragments of elastic tissue involving mid-papillary to reticular dermis [Figure 4]. Orcein stain highlighted the elastic tissue [Figures 5 and 6]. Clinically and histopathologically, a diagnosis of mid-dermal elastolysis was made, patient was counseled, and emollients were prescribed.
Figure 1.

Multiple discrete areas of wrinkling over the back
Figure 2.
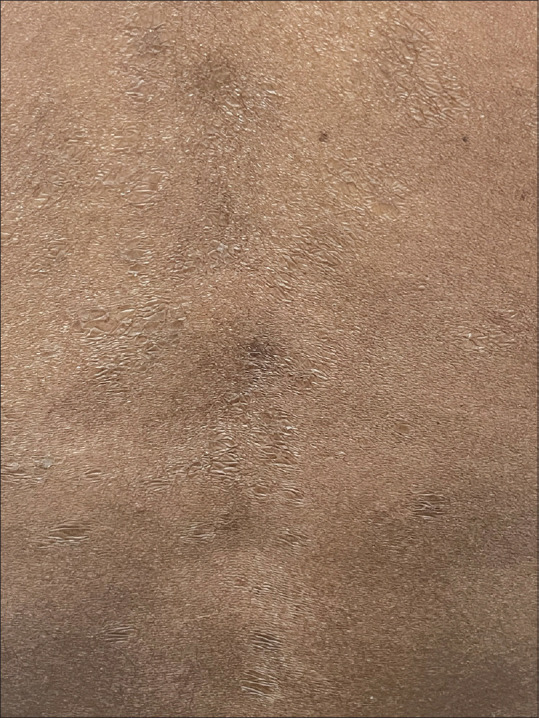
Close-up view of wrinkled areas over the back
Figure 3.
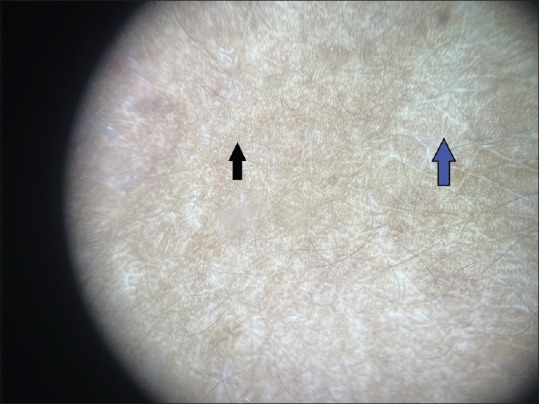
Dermoscopy showed irregular focal white areas (blue arrow) and accentuated pigment network (black arrow) with wrinkling, widened skin lines and without vessel involvement (Illuco 1100)
Figure 4.
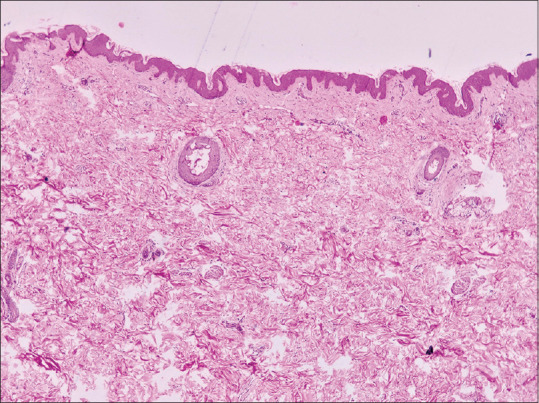
(H & E 100x): Histopathological examination revealed tiny broken fragments of elastic tissue involving mid-papillary to reticular dermis
Figure 5.
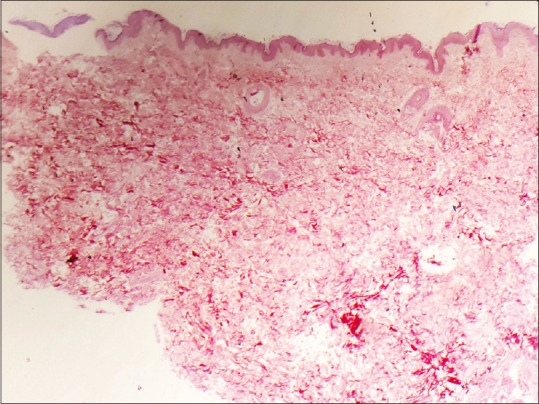
Orcein stain (scanner view 100x) highlighted the elastic tissue
Figure 6.
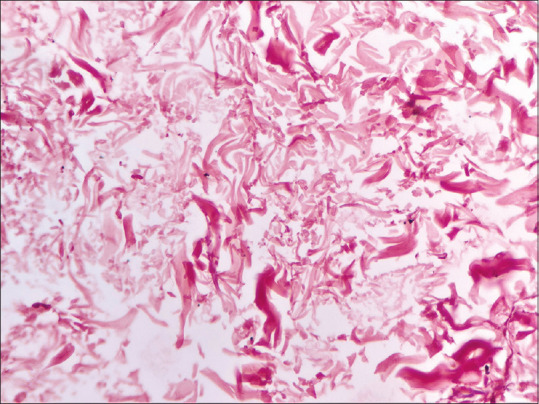
Orcein stain (400x) highlighted the elastic tissue
Mid-dermal elastolysis (MDE) is a clinical and histopathological diagnosis. MDE was known to occur predominantly in North America and Central Europe, affecting Caucasians, mostly females.[3]
Elastin degradation in MDE is caused by increased activity of elastases which can be released from cells like granulocytes, monocytes, lymphocytes, skin fibroblasts, cancer cells, and others. Elastin degeneration produces elastin-derived peptides (marker of elastolysis). The matrix metalloproteinases, gelatinase A (MMP-2) and gelatinase B (MMP-9), are implicated in the breakdown of several extracellular matrix proteins. Catalytic properties of MMPs are regulated by TIMPs (tissue inhibitors of matrix metalloproteinase) and alpha-2-macroglobulin. There is imbalance between TIMP-MMP causing degradation of elastin.[4] Elastolytic activity then produces the zonal degradation and the loss of elastic tissue in the mid-dermis. Damage to elastic fibers is through the release of elastase by inflammatory cells and autoimmunity against elastic fibers. The causes of increased elastolytic activity are based on predisposing factors and environmental co-factors such as ultraviolet radiation as seen in 50% of cases of MDE.
MDE has been reported in association with wide range of inflammatory skin conditions including urticaria, atopic dermatitis, pityriasis rosea, sweet syndrome, phototoxic dermatitis, guttate psoriasis, and granuloma annulare supporting theories that suggest the destruction of elastic fibers by preceding inflammation; however, in our case it is found as idiopathic.[5]
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form, the patient(s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- 1.Shelley WB, Wood MG. Wrinkles due to idiopathic loss of mid-dermal elastic tissue. Br J Dermatol. 1977;97:441–5. doi: 10.1111/j.1365-2133.1977.tb14255.x. [DOI] [PubMed] [Google Scholar]
- 2.Patroi I, Annessi G, Girolomoni G. Mid-dermal elastolysis: A clinical, histologic, and immunohistochemical study of 11 patients. J Am Acad Dermatol. 2003;48:846–51. doi: 10.1067/mjd.2003.452. [DOI] [PubMed] [Google Scholar]
- 3.Gambichler T. Mid-dermal elastolysis revisited. Arch Dermatol Res. 2010;302:85–93. doi: 10.1007/s00403-009-1004-0. [DOI] [PubMed] [Google Scholar]
- 4.Lewis KG, Bercovitch L, Dill SW, Robinson-Bostom L. Acquired disorders of elastic tissue. Part II. Decreased elastic tissue. J Am Acad Dermatol. 2004;51:165–85. doi: 10.1016/j.jaad.2004.03.016. [DOI] [PubMed] [Google Scholar]
- 5.Hardin J, Dupuis E, Haber RM. Mid-dermal elastolysis: A female-centric disease;Case report and updated review of the literature. Int J Womens Dermatol. 2015;1:126–30. doi: 10.1016/j.ijwd.2015.05.004. [DOI] [PMC free article] [PubMed] [Google Scholar]