

A wide disparity is present regarding accessing high-quality healthcare services in low-income countries (LICs). In such regions, safe and affordable clinical care and/or surgical interventions are difficult to provide due to several political and socioeconomic factors1. Of note, among invasive surgical disciplines, cardiovascular, and robotic surgery continues to be cited as some of the least accessible operations in LICs2. Considering that deficient healthcare infrastructures are not able to ensure the provision of decent dental, pediatric, and public health services in poor countries, access to cardiovascular surgery and its heavy financial outlay is more difficult and complicated, and often unavailable in several countries3.
Cardiovascular surgery is a surgical subspecialty focused on the invasive treatment of pathologies within the heart chambers, valves, and large thoracic vessels. Currently, it remains one of the most competitive fields sought by medical school graduates, with a notoriously demanding training pathway4. Also of note, cardiovascular disease (CVD) is the leading cause of mortality worldwide, with more than 17 million attributable deaths annually; 80% of which occur in middle- and low-income countries. However, despite such drastic statistics, interventional cardiac care remains a relatively low priority on the global public health and global surgery agenda5.
Currently, a large disparity in access to cardiac surgical care exists between low- and middle-income countries compared to high-income regions. In fact, of the 313 million surgical interventions made every year, ~6% are performed in the poorest one-third of the world’s population6. This statistic is made more frightening when considering that these regions account for 80% of the globe’s CVD burden5. More so, when comparing the availability of cardiac surgery centers, in sub-Saharan Africa, excluding South Africa7, there is ~1 center per 38 million persons, compared to one center per 120,000 persons in North America and Europe8.
In a study by Vervoort et al 9. utilizing the Cardiothoracic Surgery Network database, the authors noted a worldwide maldistribution in adult and pediatric cardiothoracic surgeons. In the case of adult cardiac surgeons, there were 11.12 adult cardiac surgeons per one million persons in North America, yet this number decreased dramatically to only 0.12 per one million persons in sub-Saharan Africa. More so, despite their massive population in sub-Saharan Africa, no cardiac surgeons were registered in Congo and Ethiopia, while only 1.04 adult cardiac surgeons per million population were documented in South Africa (Fig. 1). Conversely, in the United States, there were 11.54 adult cardiac surgeons per one million people and Monaco was the nation with the highest density of adult cardiac surgeons with 181.82 adult cardiac surgeons per million persons. In the case of pediatric cardiac surgeons, only 0.08 pediatric cardiothoracic surgeons were registered per one million people in Angola and Tanzania, compared to 2.08 per one million people in North America. Similarly to their adult cardiac surgeon counterparts, Congo and Ethiopia did not have any registered pediatric cardiothoracic surgeons (Fig. 2), while countries like the United States and Monaco had ~2.12 and 25.97 pediatric cardiothoracic surgeons per one million persons, respectively9.
Figure 1.
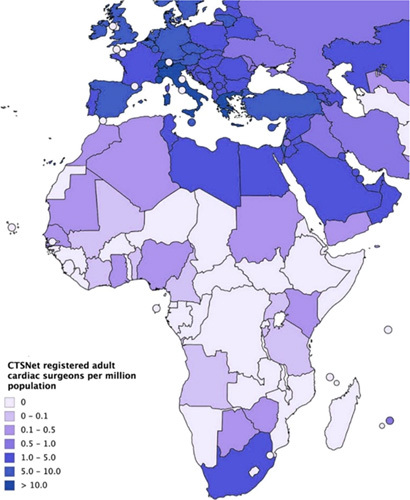
Adult cardiac surgeons per million population registered with the CTSNet in August 2017 (n=12,180). Map created at http://www.mapchart.net. CTSNet, Cardiothoracic Surgery Network.
Figure 2.
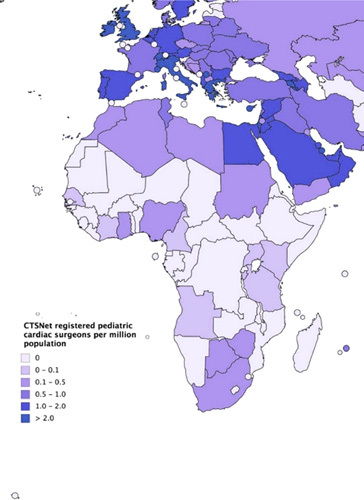
Pediatric cardiac surgeons per million population registered with the CTSNet in August 2017 (n=3858). Map created at http://www.mapchart.net. CTSNet, Cardiothoracic Surgery Network.
Several pertinent limitations hinder cardiovascular surgery access in LICs, including but not limited to a lack of established hospital infrastructures/resources, a low number of trained surgeons/interventionalists, and decreased suitable medical centers for the management of complex cardiovascular pathologies. Moreover, perceived limitations in the quality of regional medical services dissuade many patients from seeking care at local institutions and push those with adequate resources to pursue their cardiovascular surgeries in more developed countries10. For example, in Algeria, it is estimated that more than half a million of the population seek medical treatment abroad, a large percentage of which is cardiovascular patients (https://laddh-algerie.org/?P=1412). In addition, the insufficient number of highly skilled cardiac surgeons is one of the strongest reasons for the lack of access to cardiac surgery in poor countries as the availability of qualified surgeons requires several training programs, as well as improved hospital structures and clinical research, all of which remain limited11. Finally, the lack of financial stability in LICs continues to be arguably the most challenging limitation to overcome due to regional sociopolitical instability and lack of established funding sources. In addition, while several underserved areas have historically been able to receive medical services provided by humanitarian/philanthropic efforts, the high cost of invasive cardiovascular operations makes it unfeasible to provide to a large number of patients10 (https://www.acc.org/latest-in-cardiology/articles/2020/11/19/14/33/financing-cardiac-surgery-in-low-and-middle-income-countries).
Improving access to high-quality cardiovascular surgery in LICs require a multifaceted targeted initiative, with an emphasis on improved hospital resources, clinical care, and surgical training pathways for postgraduate applicants. We highlight the following: First, establishing high-quality training pathways for cardiovascular surgeons in LICs, as well as increasing the number of available academic and surgical positions is paramount. This may be facilitated through scientific and medical interchangeable conferences and webinars with developed countries such as the United States and European countries. It is also imperative to improve clinical research, which is the keystone of medical and surgical disciplines and crucial to the progression of cardiac surgery. Also, workforce educational meetings, practice facilitation, professional society feedback and guidance, and conferences are strongly recommended to be included in future cardiac surgeon’s paths12. Next, there is an urgent need for the development of a more comprehensive and responsive primary healthcare system, equipped with a strong knowledge of the quality of health services, funding, models of care, management policies, and reimbursement strategies. Taking inspiration from other nations that have perfected such modalities and the formation of international partnerships seems to be a strong starting point9,12 In addition, community involvement plays a vital role in improving healthcare and especially cardiac surgery. Community participation in Global Cardiac surgery research13 will offer various advantages through solving problem skills, taking responsibility, and making decisions14.
Regarding financial stability, there is no denying that improved economies in these regions will be needed to ensure sustainable progress. Of note, the high cost of cardiac surgery, supporting underserved patients and communities, building suitable infrastructures, improving clinical research, and ensuring regular patient follow-up monitoring and visitations can only be achieved in the presence of a strong economy that will finance all these aspects12,15. Local leaders should seek financial support through professional societies, humanitarian organizations, and local government entities, when available. In this regard, transparency is crucial; hospital and healthcare leaders must make active efforts to disclose where funding is going and use quantitative metrics to record, analyze, and showcase progress to foster improved trust and increase donor interest. Mobilizing social media campaigns may also be helpful in this regard.
In closing, despite having a large proportion of civilians with CVD, access to invasive cardiac care in LICs remains limited and far beneath access seen in more affluent regions. Efforts must be made to improve economic stability in these regions and to provide healthcare institutions with adequate resources to train and employ qualified surgeons and interventionalists. Advocacy by professional surgery societies and stakeholders, as well as community participation in Global Cardiac surgery research may also be utilized to help provide sustainable change. A healthy heart should not be looked at as a privilege for those who can afford it, but as a human right in a just world. Initiative is needed to help fulfill this promise, and it is needed now more than ever.
Ethical approval
No ethical approval was given as it is not an experimental or observational study.
Informed consent
None required.
Sources of funding
There was no funding for this research.
Author contribution
A.K.A. contributed in data collection and writing and accepted the final draft. A.A. contributed in data collection and writing and accepted the final draft. Both A.K.A. and A.A. are first authors to this paper. O.A.A.M. contributed in data collection and writing and figure format. M.A.R. contributed in writing and data collection and revised the paper.
Conflicts of interest disclosure
The authors do not have any conflicts of interest.
Research registration unique identifying number (UIN)
None.
Guarantor
Omar Abdelnasser A. Mohamed
Data availability statement
This manuscript does not contain original data.
Footnotes
Sponsorships or competing interests that may be relevant to content are disclosed at the end of this article.
Published online 29 March 2023
Contributor Information
Ahmed K. Awad, Email: ahmedkawad@gmail.com.
Adham Ahmed, Email: aahmed.018@citymail.cuny.edu.
Omar A.A. Mohamed, Email: 200429@med.asu.edu.eg.
Mohammed A. Rais, Email: raismohammedamir@gmail.com.
References
- 1.Banks LM, Kuper H, Polack S. Poverty and disability in low- and middle-income countries: a systematic review. PLoS One 2017;12:e0189996; Erratum in: PLoS One. September 26, 2018;13(9):e0204881. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Vervoort D, Swain JD, Pezzella AT, et al. Cardiac surgery in low- and middle-income countries: a state-of-the-art review. Ann Thorac Surg 2021;111:1394–400. [DOI] [PubMed] [Google Scholar]
- 3.Byiringiro S, Nyirimanzi N, Mucumbitsi J, et al. Cardiac surgery: increasing access in low- and middle-income countries. Curr Cardiol Rep 2020;22:37. [DOI] [PubMed] [Google Scholar]
- 4.Spiliopoulos K, Gansera L, Weiland HC, et al. Chronic stress and coping among cardiac surgeons: a single center study. Rev Bras Cir Cardiovasc 2014;29:308–15. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Mensah GA, Roth GA, Fuster V. The global burden of cardiovascular diseases and risk factors: 2020 and beyond. J Am Coll Cardiol 2019;74:2529–32. [DOI] [PubMed] [Google Scholar]
- 6.Meara JG, Leather AJM, Hagander L, et al. Global Surgery 2030: evidence and solutions for achieving health, welfare, and economic development. Lancet 2015;386:569–624. [DOI] [PubMed] [Google Scholar]
- 7.Yankah C, Fynn-Thompson F, Atunes M, et al. Cardiac surgery capacity in sub-Saharan Africa: Quo Vadis? Thorac Cardiovasc Surg 2014;62:393–401. [DOI] [PubMed] [Google Scholar]
- 8.Pezzella AT. Global aspects of cardiothoracic surgery with focus on developing countries. Asian Cardiovasc Thorac Ann 2010;18:299–310. [DOI] [PubMed] [Google Scholar]
- 9.Vervoort D, Meuris B, Meyns B, et al. Global cardiac surgery: access to cardiac surgical care around the world. J Thorac Cardiovasc Surg 2020;159:987–996.e6. [DOI] [PubMed] [Google Scholar]
- 10.Reichert HA, Rath TE. Cardiac surgery in developing countries. J Extra Corpor Technol 2017;49:98–106. [PMC free article] [PubMed] [Google Scholar]
- 11.Yu TH, Hou YC, Chung KP. Do low-income coronary artery bypass surgery patients have equal opportunity to access excellent quality of care and enjoy good outcome in Taiwan? Int J Equity Health 2014;13:64. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Falase B, Sanusi M, Majekodunmi A, et al. Open heart surgery in Nigeria; a work in progress. J Cardiothorac Surg 2013;8:6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Awad AK, Rais MA, Ahmed A. The beat heard around the world: making the case for global cardiac surgery. J Cardiac Surg 2022;37:3958–60. [DOI] [PubMed] [Google Scholar]
- 14.Dearani JA, Jacobs JP, Bolman RM, III, et al. Humanitarian outreach in cardiothoracic surgery: from setup to sustainability. Ann Thorac Surg 2016;102:1004–11. [DOI] [PubMed] [Google Scholar]
- 15.Ghandour H, Vervoort D, Ravishankar R, et al. Cardiac surgery and the sustainable development goals: a review. Cardiothorac Surg 2022;30:14. [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
This manuscript does not contain original data.