

Abstract
Endoscopic retrograde cholangiopancreatography (ERCP) plays a crucial role in the management of pancreaticobiliary disorders. Although the ERCP technique has been refined over the past five decades, it remains one of the endoscopic procedures with the highest rate of complications. Risk factors for ERCP-related complications are broadly classified into patient-, procedure-, and operator-related risk factors. Although non-modifiable, patient-related risk factors allow for the closer monitoring and instatement of preventive measures. Post-ERCP pancreatitis is the most common complication of ERCP. Risk reduction strategies include intravenous hydration, rectal nonsteroidal anti-inflammatory drugs, and pancreatic stent placement in selected patients. Perforation is associated with significant morbidity and mortality, and prompt recognition and treatment of ERCP-related perforations are key to ensuring good clinical outcomes. Endoscopy plays an expanding role in the treatment of perforations. Specific management strategies depend on the location of the perforation and the patient’s clinical status. The risk of post-ERCP bleeding can be attenuated by preprocedural optimization and adoption of intra-procedural techniques. Endoscopic measures are the mainstay of management for post-ERCP bleeding. Escalation to angioembolization or surgery may be required for refractory bleeding. Post-ERCP cholangitis can be reduced with antibiotic prophylaxis in high risk patients. Bile culture-directed therapy plays an important role in antimicrobial treatment.
Keywords: Endoscopic retrograde cholangiopancreatography, Hemorrhage, Infections, Pancreatitis, Perforation
INTRODUCTION
Endoscopic retrograde cholangiopancreatography (ERCP) plays an important role in the management of pancreaticobiliary disorders. ERCP has evolved over the last five decades from being a diagnostic procedure to becoming a predominantly therapeutic one. The number of ERCPs performed has increased steadily over the years, with more than 350,000 performed annually in the United States alone.1 Technological advances, increased operator experience, and improved patient selection have enhanced ERCP safety. However, ERCP is still associated with a significant potential for complications.2 Thus, it is important to develop strategies to identify the risk factors for ERCP-related complications, implement measures that can decrease the risk of complications, and identify elevated-risk patients for closer observation and specific management.
In this review, we enumerate the risk factors for ERCP-related complications, outline the preventive measures that can be undertaken to attenuate these risks, and expound on the management strategies for ERCP-related complications.
POST-ERCP PANCREATITIS
Post-ERCP pancreatitis (PEP) is the most common complication of ERCP.3 A large meta-analysis of 21 prospective studies involving 16,855 patients has estimated the incidence of PEP to be 3.47% (95% confidence interval [CI], 3.19–3.75), with an associated mortality of 3.08% (95% CI, 1.65–4.51).4 The incidence of PEP may be as high as 15% in high risk patients.4 The widely accepted definition and classification of PEP severity was proposed by Cotton et al.5 It is based on clinical progress after ERCP including new or worsening abdominal pain, biochemical findings of elevated serum amylase, and the need for inpatient admission. Longer inpatient admissions and the development of complications necessitating intervention indicated more severe PEP (Table 1). The revised Atlanta classification is also a useful complement for assessing the severity of acute pancreatitis, even though it is not specific to PEP and requires the use of imaging.6
Table 1.
Classification of severity of post-ERCP pancreatitis
| Characteristic | Grade of severity of pancreatitis |
||
|---|---|---|---|
| Mild | Moderate | Severe | |
| Presence of abdominal pain | New or worsening abdominal pain suggestive of pancreatitis | ||
| Hyperamylasemia | Amylase ≥3 times the upper limit of normal at ≥24 hours after ERCP | ||
| Duration of admission | Requiring admission or hospitalization of 2 to 3 days | Requiring hospitalization of 4 to 10 days | Requiring hospitalization >10 days |
| Presence of local complications | Development of hemorrhagic pancreatitis, phlegmon or pseudocyst, or requiring intervention (percutaneous drainage or surgery) | ||
ERCP, endoscopic retrograde cholangiopancreatography.
Risk factors
The risk factors for PEP can be broadly classified into patient-, procedure-, and operator-related factors (Table 2). Patient-related risk factors are non-modifiable, but physician awareness is important for identification of at-risk patients for closer monitoring, and in instituting preventive measures. A prospective multicenter study by Freeman et al. examining 1,963 consecutive ERCPs detailed numerous risk factors for PEP. Patient-related factors that were significant on multivariate analysis included a history of PEP (odds ratio [OR], 5.35; 95% CI, 2.97–9.66), suspected sphincter of Oddi dysfunction (SOD) (OR, 2.60; 95% CI, 1.59–4.26), female gender (OR, 2.51; 95% CI, 1.49–4.24), normal serum bilirubin (<1.0 mg/dL) (OR, 1.89; 95% CI, 1.22–2.93), and absence of chronic pancreatitis (OR, 1.87; 95% CI, 1.00–3.48).7 A matched-cohort study conducted by Inamdar et al.8 involving 907 pregnant patients who underwent ERCP also suggested that pregnancy increases the risk of PEP (OR, 2.80; 95% CI, 2.1-3.8). In another prospective multicenter study involving 1,115 patients, Cheng et al.9 found that young patients (<60 years old) had a higher risk of PEP (OR, 1.6; 95% CI, 1.03–2.40).
Table 2.
Risk factors for post-ERCP pancreatitis
| Specific factors |
|---|
| Patient-related factor |
| Female sex |
| Pregnancy |
| Younger age (<60 years) |
| Sphincter of Oddi dysfunction |
| Previous post-ERCP pancreatitis |
| Absence of chronic pancreatitis |
| Normal serum bilirubin |
| Procedure-related factor |
| Pancreatic duct injection |
| Guidewire entry into pancreatic duct |
| Balloon dilation of intact sphincter of Oddi |
| Difficult cannulation |
| Pancreatic sphincterotomy |
| Minor papilla sphincterotomy |
| Papillectomy |
| Operator-related factor |
| Trainee involvement |
| Low case volume |
ERCP, endoscopic retrograde cholangiopancreatography.
However, some procedure- and operator-related factors are potentially modifiable. Freeman et al.7 found that balloon dilation of the intact SOD (OR, 4.51; 95% CI, 1.51–13.46), moderately difficult cannulation (at least six attempts at cannulation) (OR, 3.41; 95% CI, 2.13–5.47), pancreatic sphincterotomy (OR, 3.07; 95% CI, 1.64–5.75), and contrast injection into the pancreatic duct (PD) (OR, 2.72; 95% CI, 1.43–5.17) were associated with an increased risk of PEP. In an early meta-analysis performed by Masci et al.,10 pre-cut papillotomy was found to elevate the risk of PEP (OR, 2.71; 95% CI, 2.02–3.63). However, subsequent studies showed that the increased rates of PEP were likely due to prolonged procedures and multiple attempts at cannulation rather than pre-cut papillotomy as suggested by Cennamo et al.11 who pooled six randomized controlled trials (RCTs) in a meta-analysis of 966 patients and showed that early pre-cut biliary sphincterotomy was associated with a lower risk of developing PEP than conventional methods that require repeated cannulation attempts (OR, 0.47; 95% CI, 0.24–0.91). Endoscopic papillectomy is associated with a 3% to 25% risk of PEP among other complications.12 Repeated guidewire passage into the PD has been shown to increase the risk of PEP (OR, 2.77; 95% CI, 1.79–4.30).13 In a prospective RCT, Harewood et al.14 found that the risk of PEP can be significantly reduced by placement of a pancreatic stent compared to not inserting a pancreatic stent (0% vs. 33%, p=0.02).
Cheng et al.9 also found that minor papilla sphincterotomy (OR, 3.80; 95% CI, 2.00–7.11) and trainee involvement (OR, 1.50; 95% CI, 1.03–2.06) increased the risk of PEP. A large retrospective study found that a low case volume was a risk factor for post-ERCP pancreatitis in certain scenarios. Syrén et al.15 performed a retrospective analysis of 80,904 ERCPs in Sweden between 2009 and 2018. Endoscopists with higher case volumes were noted to have lower rates of PEP when ERCPs were performed for choledocholithiasis (OR, 1.028; 95% CI, 1.002–1.054) and malignancy (OR, 1.179; 95% CI, 1.045–1.330). Freeman et al.7 also found that the risk factors for PEP are cumulative, and that patients with multiple risk factors are likely to be at an even higher risk of developing PEP.
Preventive measures
Several measures have been progressively introduced to reduce the risk of PEP. Pharmacological measures include administration of rectal nonsteroidal anti-inflammatory drugs (NSAIDs), glyceryl trinitrate (GTN), and intravenous hydration. A multicenter, randomized, placebo-controlled, double-blind clinical trial conducted by Elmunzer et al.16 involving 602 patients showed that patients who were administered rectal indomethacin immediately after ERCP had significantly lower rates of PEP than patients who received placebo (4.4% vs. 8.8%, p=0.03). However, two large prospective studies investigating oral NSAIDs did not demonstrate any benefit when compared with placebo.17,18 The effect of NSAIDs appears to be limited to the transrectal route, which is hypothesized to be related to a faster onset of action and better bioavailability compared to the oral route.
GTN is hypothesized to reduce the pressure of the SOD19 and cause vasodilation of the microvascular vessels, which may improve pancreatic tissue perfusion.20 Bai et al.21 performed a meta-analysis that pooled eight RCTs with 1,920 patients and examined the efficacy of GTN administered via various routes in lowering the risk of PEP. Subgroup analyses found that GTN significantly lowered the risk of PEP only when it was administered via the sublingual route (OR, 0.37; 95% CI, 0.18–0.74) and in patients at high risk of PEP (OR, 0.44; 95% CI, 0.28–0.70). However, the number of patients needed to treat (NNT) was high and there were substantial adverse events, limiting its selective usage in certain patients at elevated risk. Two large prospective studies suggested that sublingual GTN further decreases the risk of PEP when administered in addition to rectal NSAIDs.22,23
Intravenous periprocedural hydration is key to attenuating the risk of PEP. Wu et al.24 performed a meta-analysis pooling 10 RCTs with 2,000 patients that examined the use of intravenous lactated Ringer’s solution for periprocedural hydration in patients undergoing ERCP. Aggressive hydration was found to reduce the incidence of PEP (OR, 0.40; 95% CI, 0.26–0.63) compared to standard hydration, with no difference in fluid overload between the two groups (OR, 0.93; 95% CI, 0.21–4.13). On the contrary, an open-label multi-center RCT involving 826 patients with moderate to high risk of PEP that compared patients who had aggressive hydration and rectal NSAIDs with those who received standard hydration and rectal NSAIDs did not show any difference in the incidence of PEP (risk ratio [RR], 0.84; 95% CI, 0.53–1.33), other ERCP-related complications (RR, 0.90; 95% CI, 0.62–1.31), intensive care unit admissions (RR, 0.37; 95% CI, 0.07–1.80), and 30-day mortality (RR, 0.95; 95% CI, 0.50–1.83).25
Several endoscopic measures can be taken to reduce the risk of PEP. The efficacy of prophylactic PD stenting in preventing PEP was first described by Tarnasky et al.26 in the late 1990s. This was followed by multiple studies that supported the use of prophylactic PD stenting in attenuating the risk of PEP. Fan et al.27 pooled 14 RCTs in a meta-analysis that included 2,510 patients. The results favored the use of PD stenting over no PD stenting in lowering the incidence of PEP (OR, 0.35; 95% CI, 0.25–0.49). A prospective RCT by Ito et al.28 further highlighted the role of PD stenting in reducing the risk of PEP in patients who had guidewire entry into the PD (RR, 0.13; 95% CI, 0.01–0.95) from 23.0% to 2.9%. Given the efficacy of PD stent placement in decreasing the risk of PEP, prophylactic placement of PD stent is recommended in several high-risk scenarios, such as in patients with SOD who require any biliary or pancreatic manipulation, prior to pre-cut papillotomy, and in patients who require endoscopic papillectomy, pancreatic sphincterotomy, pancreatic brush cytology or those who underwent difficult cannulation, guidewire entry into and/or repeated contrast injection of the PD (Table 3).
Table 3.
Clinical scenarios where pancreatic stent placement is recommended
| Clinical scenarios where pancreatic stent placement is recommended | Before pre-cut papillotomy |
| Patients with SOD/ suspected SOD who require any biliary or pancreatic manipulation | |
| Endoscopic papillectomy | |
| Pancreatic sphincterotomy | |
| Pancreatic brush cytology | |
| After difficult cannulation or repeated contrast injection of the pancreatic duct |
SOD, sphincter of Oddi dysfunction.
PD stent placement may be difficult in small and tortuous PDs and may sometimes impede subsequent biliary cannulation. The insertion of a guidewire into the PD (without the placement of a PD stent) is an alternative to PD stent placement. However, a Cochrane systematic review comprising seven RCTs with 577 patients showed that placement of a pancreatic guidewire resulted in higher incidence of PEP than other techniques such as persistent conventional cannulation, pre-cut sphincterotomy, and PD stent placement (RR, 1.98; 95% CI, 1.14–3.42).29 Notwithstanding the proven value of PD stent placement, Freeman et al.30 showed that unsuccessful PD stent placement increased the risk of PEP (OR, 16.1; 95% CI, 1.3–200), and suggested a modified short-wire technique to improve the success rate of PD stent placement in patients with small or tortuous PDs.
Guidewire-led biliary cannulation followed by contrast opacification may decrease the risk of PEP compared to the conventional contrast-assisted cannulation technique. A Cochrane systematic review comprising 15 RCTs with 4,426 patients demonstrated that the risk of PEP was lower with guidewire-led biliary cannulation based on intention-to-treat analysis (RR, 0.51; 95% CI, 0.36–0.72). In addition, the guidewire-assisted cannulation technique may result in an increase in primary cannulation success (RR, 1.06; 95% CI, 1.01–1.12).31
Prevention of PEP involves three main steps. First, patient selection is key to ensuring that ERCP is performed only for patients for whom ERCP is indicated. Identification of patients with risk factors for PEP would allow for appropriate informed consent, closer post-procedure observation, or referral to high-volume centers/endoscopists as appropriate. Second, patients who undergo ERCP should receive pharmacological prophylaxis, which should include rectal NSAIDs, intravenous hydration, and sublingual GTN in selected patients. Third, procedural techniques can be modified; wire-guided biliary cannulation should be performed, and a PD stent should be prophylactically placed when indicated.
PERFORATION
Perforation is defined by the 2010 American Society of Gastrointestinal Endoscopy lexicon on endoscopic adverse events as the presence of air or luminal contents outside the gastrointestinal tract.32 A large systematic review of 259 studies showed that the overall incidence of perforation was 0.6% and the overall mortality rate was 8.0%.33
Risk factors
Few studies have examined the risk factors for ERCP-related perforations. These risk factors can be broadly subdivided into patient- and procedure-related risk factors (Table 4). Enns et al.34 performed a retrospective study of 33 patients with confirmed ERCP-related perforations. Patient-related risk factors included SOD (OR, 3.20; 95% CI, 1.64–8.94) and dilated common bile duct (OR, 2.32; 95% CI, 1.02–5.03), while procedure-related factors included biliary stricture dilatation (OR, 7.20; 95% CI, 1.84–28.11), prolonged procedure duration (OR, 1.021; 95% CI, 1.006–1.036) and performance of sphincterotomy, including pre-cut sphincterotomy (OR, 6.94; 95% CI, 2.43–19.77).
Table 4.
Risk factors for ERCP-related perforations
| Patient-related risk factor | Procedure-related risk factors |
|---|---|
| Surgically-altered anatomy (including Billroth II anatomy) | Endoscopic sphincterotomy |
| Presence of a papillary lesion (including malignancy) | Pre-cut sphincterotomy |
| Sphincter of Oddi dysfunction | Dilation of biliary stricture |
| Longer procedure time |
ERCP, endoscopic retrograde cholangiopancreatography.
An altered gastrointestinal anatomy may contribute to endoscope-related trauma and consequent ERCP-related perforations. A retrospective study by Kumbhari et al.35 reviewed 3,331 patients who underwent ERCP and were admitted with postprocedural abdominal pain. A total of 79 patients had ERCP-related perforations. In five of seven patients diagnosed with Stapfer type I perforations, post-surgical anatomy such as Roux-en-Y (n=3) and Billroth II gastrojejunostomy (n=2) were present.
Various factors increase the risk of mortality in patients with ERCP-related perforations. In a large population-based study of 52,140 ERCPs with 37 perforations, Langerth et al.36 found that age >80 years (OR, 3.8; 95% CI, 2.0–7.4), malignancy (OR, 11.2; 95% CI, 5.8–21.6), and performance of pancreatic sphincterotomy (OR, 2.8; 95% CI, 1.1–7.5) were associated with a higher rate of mortality.
Management
Prompt recognition and treatment of ERCP-related perforations is key to ensuring good clinical outcomes. Management of perforations depends on the site of the perforation, clinical status of the patient, and radiological findings. Management strategies can be broadly classified into (1) local treatment to close the perforation and divert digestive secretions, (2) regional treatment to drain the resultant collections, and (3) general measures. ERCP-related perforations are classified according to the anatomical location and mechanism of injury, as proposed by Stapfer et al.37 Type I to IV perforations carry different clinical implications, which can help guide the treatment. The location, likely mechanism, frequency, and treatment of each perforation type are shown in Table 5.33,37
Table 5.
Classification of ERCP-associated perforation types
| Type | Location | Likely mechanism of injury | Frequency (%) | Local treatment measures |
|---|---|---|---|---|
| I | Lateral/medial wall of duodenum | Endoscope-related trauma | 18 | Immediate endoscopic or surgical closure |
| II | Peri-ampullary | Sphincterotomy | 58 | Immediate endoscopic or surgical closure of defect and diversion of bilious/pancreatic secretions from defect |
| III | Biliary/pancreatic duct | Intra-ductal instrumentation | 13 | Diversion of bilious/pancreatic secretions from defect |
| IV | None; presence of retroperitoneal air alone | Luminal insufflation after guidewire perforation | 11 | Observation |
ERCP, endoscopic retrograde cholangiopancreatography.
Modified from Stapfer et al. Ann Surg 2000;232:191–198.37
Type I perforations occur at the lateral or medial wall of the duodenum and result from endoscope-related trauma. Management of Stapfer type I perforations has traditionally been surgical.35,37 However, morbidity and mortality associated with surgical repair can be significant. Endoscopic closure is feasible if the defect is detected within 12 hours of occurrence and if the patient is clinically well. Various endoscopic closure techniques have been described previously. Through-the-scope clips have been used to close such defects successfully.38 Over-the-scope clips (OTSC) have been used to close defects up to 20 mm in diameter39 (Figs. 1–4). The use of OTSC for the closure of upper gastrointestinal iatrogenic perforation has been reported to decrease the proportion of patients requiring surgery from 62.5% to 12.5% in a retrospective study by Khater et al.40 Endoscopic suturing via an over-the-scope suturing device has also been described for the closure of iatrogenic perforations in the duodenum by Hyun et al.41 More recently, Zhang et al.42 described the use of a novel through-the-scope suturing device to close iatrogenic duodenal defects, potentially obviating the additional step of removing the endoscope from the patient to affix the device. Surgical repair is required immediately in cases where endoscopic measures fail. In a retrospective study, 50 out of 380 patients with ERCP-related perforations required surgery. Forty percent of these patients underwent delayed surgery more than 24 hours after ERCP, and this was associated with higher rates of mortality (50% vs. 20%, p=0.026) and postoperative duodenal leak (75% vs. 23%, p<0.001) than those who underwent surgery within 24 hours.43
Fig. 1.
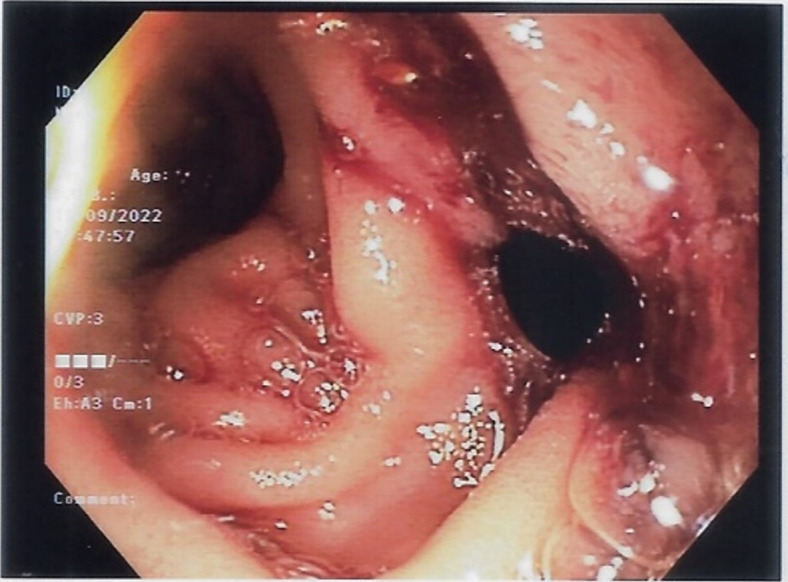
Stapfer type I perforation was seen in the duodenal wall opposite the major papilla.
Fig. 2.

Contrast leak was noted after deployment of one over-the-scope clip, indicating that defect was not completely closed.
Fig. 3.
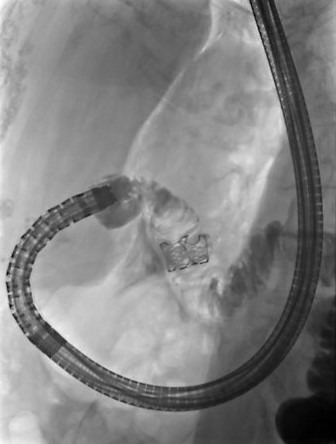
No further contrast leak was noted after placement of the second over-the-scope clip.
Fig. 4.

Nasojejunal tube was inserted for suctioning to reduce the secretions traversing the region of the repaired perforation, as well as to ensure continuation of enteral nutrition.
Type II perforations are peri-ampullary and generally caused by sphincterotomy. A meta-analysis of 18 studies estimated that type II perforations accounted for nearly half of all ERCP-related perforations.44 The mainstay of management is to cover the defect and divert the bile flow via endoscopic biliary drainage. A large retrospective study by Odemis et al.,45 comprising a total of 7,471 ERCPs with 20 Stapfer type II perforations detected intraprocedurally, compared the use of a biliary fully covered self-expanding metal stent (FCSEMS) against the placement of a nasobiliary catheter. The use of biliary FCSEMS was associated with lower rates of abdominal pain (0% vs. 62.5%, p=0.005) and a trend towards a shorter length of hospital stay (11.7±3.2 vs. 15.8±5.2, p=0.053) when compared with nasobiliary catheter placement. Emergency surgery is indicated only in rare cases in which a major contrast leak is insufficiently sealed after endoscopic therapy.
Type III perforations occur in the bile duct or PD and are often associated with instrumentation. They tend to seal spontaneously and are less likely to require intervention. Placement of FCSEMS or plastic stents can be considered if there is substantial contrast extravasation.37
Type IV perforations are evidenced by retroperitoneal air alone and are attributed to luminal insufflation after guidewire-related perforations. They usually do not require intervention.
Regional treatment involves draining collections from the perforation region. Persistent retroperitoneal fluid collection can be drained percutaneously.46 Endoscopic ultrasound (EUS)-guided drainage of biloma can be performed to facilitate internal drainage.47 Surgical management is indicated when there is persistence of contrast medium leak, retroperitoneal fluid collections not amenable to percutaneous or EUS-guided drainage,48 or persistent sepsis despite nonsurgical management.
General measures include hospital admission and the administration of broad-spectrum antibiotics. The patient should be kept nil per os and have a nasogastric/nasojejunal tube placed with suction applied to decrease the amount of fluid at the perforation site until the perforation has sealed.
BLEEDING
Risk factors
Post-ERCP bleeding (PEB) is most frequently observed after endoscopic sphincterotomy (ES).4 The overall incidence of PEB was found to be approximately 1.34% in a large systematic review of prospective studies examining ERCP-related complications in 16,855 patients.4 Risk factors could be divided into patient-, procedure-, and operator-related risk factors (Table 6).
Table 6.
Risk factors for post-ERCP bleeding
| Patient-related risk factors | Procedure-related risk factors | Operator-related risk factors |
|---|---|---|
| Liver cirrhosis | Endoscopic sphincterotomy | Low endoscopist experience (<200 ERCPs) |
| End-stage renal disease requiring dialysis | Intra-procedural bleeding | |
| Use of anti-platelet agents | ||
| Thrombocytopenia (<50,000/mm3) |
ERCP, endoscopic retrograde cholangiopancreatography.
The presence of cirrhosis has been well studied as a risk factor for PEB. A meta-analysis of 15 studies by Mashiana et al.49 involving 6,505 patients showed that cirrhosis increased the likelihood of PEB (OR, 2.05; 95% CI, 1.62–2.58). A retrospective study by Kim et al.50 involving 8,554 patients who underwent ERCP, including 264 patients with cirrhosis, also found that cirrhosis was an independent risk factor for PEB on multivariate analysis (OR, 2.50; 95% CI, 1.38–4.53) after adjusting for prothrombin time, use of antiplatelet and anticoagulant agents, duration of ERCP, and stent insertion. The bleeding risk appeared to increase with the severity of liver cirrhosis. Patients with Child-Pugh class C were found to have an increased incidence of PEB (OR, 6.14; 95% CI, 1.32–28.61).
A retrospective study by Oh et al.51 involving 2,435 cases of ERCP highlighted the importance of the peri-procedural management of anti-platelet agents (APAs). Compared with patients not taking APAs, those who took aspirin (OR, 6.35; 95% CI, 2.97–13.58), other single APAs (OR, 8.61; 95% CI, 2.42–30.59), and multiple APAs (OR, 12.0; 95% CI, 3.86–37.43) were more likely to develop PEB. In patients who require secondary prophylaxis for cardiovascular disease, aspirin can be administered peri-procedurally, given its lower risk of PEB compared with other APAs or multiple APAs.52 With regards to anticoagulation, a retrospective study by Parras Castañera et al.53 showed that patients who underwent ERCP while on direct oral anticoagulants were 3.6 (95% CI 1.0–12.8) times more likely to develop PEB compared to those on low molecular weight heparin or acenocoumarin.
End-stage renal disease requiring hemodialysis was also found to be associated with a higher risk of PEB (OR, 13.30; 95% CI, 5.78–30.80) in a retrospective study performed by Nakaji et al.54 that involved 1,518 patients who underwent ERCP with ES. The study also found that thrombocytopenia <50,000/mm3 (OR, 35.3; 95% CI, 3.81–328) and bleeding during ES (OR, 4.28; 95% CI, 2.30–4.97) were associated with an increased risk of PEB.
While ES is a well-known cause of PEB, the length of the ES is especially associated with an increased risk of PEB. In a retrospective study involving 3,620 patients, of whom 1,121 underwent biliary ES, patients who had a medium ES (defined as an incision from the papillary orifice to the midpoint between the proximal hooding fold and the superior margin of the sphincter opening) had an elevated bleeding risk (OR, 10.97; 95% CI, 5.90–24.87). This was even more pronounced in patients who had a full ES (defined as an incision made from the papillary orifice up to the superior margin of the sphincter opening) (OR, 68.27; 95% CI, 8.74–422.14).55 Endoscopist experience was inversely related to PEB risk. A prospective observational study involving 1,191 patients by Lee et al.56 found that endoscopist experience of <200 ERCPs was associated with a higher bleeding risk (OR, 1.439; 95% CI, 1.003–2.062).
Preventive strategies
The risk of PEB can be attenuated by preprocedural optimization and the adoption of intra-procedural techniques. Endoscopic biliary and pancreatic sphincterotomy are classified by the American Society of Gastrointestinal Endoscopy as procedures with a higher bleeding risk.57 The discontinuation of antithrombotic agents should be considered and weighed against the risk of thrombosis. Patients with thrombocytopenia and coagulopathy should undergo blood product transfusions to reduce the risk of procedure-related bleeding. The use of endoscopic papillary large balloon dilatation, compared to ES, was found to significantly lower the risk of PEB (OR, 0.15; 95% CI, 0.04–0.50) in a meta-analysis of seven RCTs by Feng et al.58 involving 790 patients. Performing sphincterotomy in the 11 to 1 o’clock axis was also thought to reduce the risk of PEB, as this area has been found to contain the lowest concentration of arteries based on a micro-dissection of 19 cadaver pancreatico-duodenal specimens.59
Management
The management of PEB involves a stepwise approach (Fig. 5), with escalation to more advanced measures and treatment modalities if the initial measures are unsuccessful. Conventional measures for hemostasis, such as epinephrine injection and clipping60 can be used first. The duodenoscope elevator makes clip delivery challenging, and a forward-viewing endoscope fitted with a distal cap may be considered for the ease of clip placement.61 Aranez et al.62 illustrated the feasibility of a novel clip designed for delivery using a duodenoscope. Care should be taken to avoid injury to the pancreatic orifice when clips are deployed. Other measures for hemostasis have also been explored, including FCSEMS insertion. Itoi et al.12 described a series of 11 patients with uncontrolled postsphincterotomy bleeding despite balloon tamponade, hypertonic saline epinephrine injection, or endoclip placement. These patients underwent FCSEMS placement and achieved complete hemostasis (Supplementary Video 1), with stent removal later on. A prospective study of 97 patients who underwent FCSEMS insertion after post-ES bleeding showed a technical success rate of 100% and rebleeding rate of 6.2%, with a mean time to FCSEMS removal of 7.7±9.3 weeks.63 In the event that endoscopic techniques are unsuccessful, transcatheter arterial angioembolization or surgical vessel ligation can be performed. Dunne et al.64 described 11 patients with post-sphincterotomy bleeding not controlled by endoscopy who then underwent angioembolization of the gastroduodenal artery, superior pancreaticoduodenal artery, or inferior pancreaticoduodenal artery. Ten of these 11 patients had successful hemostasis, while one patient had to be referred for surgical intervention due to rebleeding.
Fig. 5.
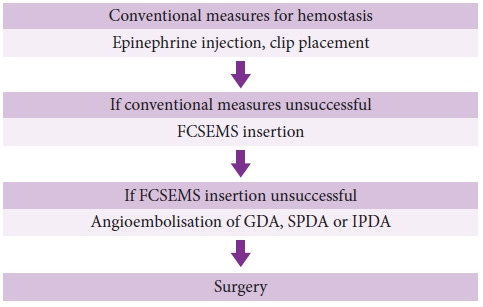
Management algorithm of post-endoscopic retrograde cholangiopancreatography bleeding. FCSEMS, fully covered self-expanding metal stent; GDA, gastroduodenal artery; SPDA, superior pancreaticoduodenal artery; IPDA, inferior pancreaticoduodenal artery.
CHOLANGITIS
Cholangitis may result from ERCP because of contamination of the sterile space by instrumentation or contrast injection. The overall incidence of cholangitis is estimated to between 0.5% to 3%.2 Bacteremia may also occur due to bacterial translocation into the bloodstream through sites of mucosal trauma. The incidence of bacteremia during ERCP ranges from 6.4% in patients with non-obstructed bile ducts to 18% in patients with biliary obstruction due to the presence of stones or strictures.65
The risk of post-ERCP cholangitis (PEC) is related to both patient- and procedure-related factors (Table 7). In a retrospective study by Chen et al.66 involving 4,324 patients, multivariate analysis showed that hilar obstruction (OR, 2.59; 95% CI, 2.07–2.74), age ≥60 years (OR, 1.98; 95% CI, 1.37–2.40), and previous ERCP (OR, 2.48; 95% CI, 2.13–2.71) were risk factors for PEC, whereas successful clearance of choledocholithiasis was a protective factor (OR, 0.70; 95% CI, 0.32–0.92).
Table 7.
Risk factors for post-ERCP cholangitis
| Patient-related factors | Procedure-related factors |
|---|---|
| Hilar obstruction | Incomplete biliary drainage |
| Age ≥60 years | Cholangioscopy |
| Previous ERCP | |
| Primary sclerosing cholangitis |
ERCP, endoscopic retrograde cholangiopancreatography.
Patients who are predisposed to difficult biliary drainage have a higher incidence of PEC. A retrospective study by Navaneethan et al.,67 involving 294 patients with primary sclerosing cholangitis who underwent ERCP, found that the incidence of PEC in this group of patients was elevated by 2.4%, suggesting that primary sclerosing cholangitis is a risk factor for PEC. This was attributed to inadequate biliary drainage and contrast injection.
Cholangioscopy is a risk factor for PEC and post-ERCP bacteremia. This has been postulated to be due to ductal irrigation during the procedure. In a prospective study by Othman et al.68 involving 57 patients who underwent cholangioscopy, 7.0% developed PEC, and 8.8% developed post-ERCP bacteremia. Another retrospective study by Sethi et al.69 involving 4,214 ERCPs showed that the incidence of PEC was higher in patients who underwent cholangioscopy than in those who did not (1.0% vs. 0.2%; OR, 4.98; 95% CI, 1.06–19.67).
Preventive measures
Given the morbidity associated with PEC, the utility of antibiotic prophylaxis has been well-studied. An early meta-analysis of seven RCTs by Harris et al.70 in 1999 for antibiotic prophylaxis prior to ERCP showed that it did not lead to a significant reduction in the incidence of post-ERCP bacteremia (RR, 0.39; 95% CI, 0.12–1.29) nor PEC (RR, 0.91; 95% CI, 0.39–2.15). A Cochrane systematic review of 9 RCTs by Brand et al.71 involving 1,573 patients showed that the overall incidence of bacteremia was reduced (RR, 0.50; 95% CI, 0.33–0.78) in patients who received antibiotic prophylaxis, but this effect was not significant in those who achieved successful biliary drainage after ERCP (RR, 0.98; 95% CI, 0.35–2.69).
A selective approach for antibiotic prophylaxis appeared to be effective. Kager et al.72 performed a retrospective study examining 540 cases of ERCP in 327 patients, in which antibiotic prophylaxis was administered only to those deemed to be at high risk of cholangitis (patients with proximal biliary obstruction such as hilar tumors and sclerosing cholangitis, pancreatic pseudocysts, as well as in cases of incomplete biliary drainage, or non-ERCP-related reasons such as prosthetic heart valves). The overall incidence of PEC in this group of patients on restricted use of antibiotics was 2.7%, which was similar to the prevailing literature. The PEC rates in the low-risk group were comparable to those in the high-risk group (2.5% vs. 3.3%).
Treatment
The management of PEC involves timely imaging with contrast-enhanced computed tomography or magnetic resonance cholangiopancreatography to assess bile duct and stent patency in patients in whom PEC is suspected.73 Bile samples should also be taken if a repeat ERCP is performed for biliary decompression, as bile cultures are much more likely to be positive than blood cultures,74 allowing for the use of culture-directed antibiotics. A prospective study by Negm et al.75 involving 243 patients showed that performing bile cultures for those with cholangitis resulted in a subsequent culture-directed modification in antibiotic treatment for 72.5% of patients.
CONCLUSIONS
Despite extensive research and refinement of this technique, ERCP-related complications remain a major issue. The most common complications of ERCP are pancreatitis, perforation, bleeding, and cholangitis. The identification of risk factors for ERCP-related complications, implementation of measures that decrease the risk of complications, and prompt identification and treatment of complications are key to ensuring good clinical outcomes.
Footnotes
Conflicts of Interest
The authors have no potential conflicts of interest.
Funding
None.
Author Contributions
Conceptualization: CCHW, CJLK; Data curation: CCHW, CJLK; Formal analysis: CCHW, SJML, CJLK; Supervision: CCHW, CJLK; Validation: CCHW, CJLK; Visualization: CCHW, SJML, CJLK; Writing–original draft: CCHW, SJML, CJLK; Writing–review & editing: CCHW, SJML, CJLK.
Supplementary Material
The patient developed bleeding after the endoscopic sphincterotomy. This persisted despite balloon tamponade and irrigation with diluted adrenaline. Hemostasis was secured by the deployment of a biliary fully covered self-expanding metal stent (https://doi.org/10.5946/ce-2023-013.v1).
Supplementary materials related to this article can be found online at https://doi.org/ce.2023.013.
REFERENCES
- 1.Cappell MS, Friedel DM. Stricter national standards are required for credentialing of endoscopic-retrograde-cholangiopancreatography in the United States. World J Gastroenterol. 2019;25:3468–3483. doi: 10.3748/wjg.v25.i27.3468. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Dumonceau JM, Kapral C, Aabakken L, et al. ERCP-related adverse events: European Society of Gastrointestinal Endoscopy (ESGE) Guideline. Endoscopy. 2020;52:127–149. doi: 10.1055/a-1075-4080. [DOI] [PubMed] [Google Scholar]
- 3.ASGE Standards of Practice Committee. Chandrasekhara V, Khashab MA, et al. Adverse events associated with ERCP. Gastrointest Endosc. 2017;85:32–47. doi: 10.1016/j.gie.2016.06.051. [DOI] [PubMed] [Google Scholar]
- 4.Andriulli A, Loperfido S, Napolitano G, et al. Incidence rates of post-ERCP complications: a systematic survey of prospective studies. Am J Gastroenterol. 2007;102:1781–1788. doi: 10.1111/j.1572-0241.2007.01279.x. [DOI] [PubMed] [Google Scholar]
- 5.Cotton PB, Lehman G, Vennes J, et al. Endoscopic sphincterotomy complications and their management: an attempt at consensus. Gastrointest Endosc. 1991;37:383–393. doi: 10.1016/s0016-5107(91)70740-2. [DOI] [PubMed] [Google Scholar]
- 6.Banks PA, Bollen TL, Dervenis C, et al. Classification of acute pancreatitis--2012: revision of the Atlanta classification and definitions by international consensus. Gut. 2013;62:102–111. doi: 10.1136/gutjnl-2012-302779. [DOI] [PubMed] [Google Scholar]
- 7.Freeman ML, DiSario JA, Nelson DB, et al. Risk factors for post-ERCP pancreatitis: a prospective, multicenter study. Gastrointest Endosc. 2001;54:425–434. doi: 10.1067/mge.2001.117550. [DOI] [PubMed] [Google Scholar]
- 8.Inamdar S, Berzin TM, Sejpal DV, et al. Pregnancy is a risk factor for pancreatitis after endoscopic retrograde cholangiopancreatography in a national cohort study. Clin Gastroenterol Hepatol. 2016;14:107–114. doi: 10.1016/j.cgh.2015.04.175. [DOI] [PubMed] [Google Scholar]
- 9.Cheng CL, Sherman S, Watkins JL, et al. Risk factors for post-ERCP pancreatitis: a prospective multicenter study. Am J Gastroenterol. 2006;101:139–147. doi: 10.1111/j.1572-0241.2006.00380.x. [DOI] [PubMed] [Google Scholar]
- 10.Masci E, Mariani A, Curioni S, et al. Risk factors for pancreatitis following endoscopic retrograde cholangiopancreatography: a meta-analysis. Endoscopy. 2003;35:830–834. doi: 10.1055/s-2003-42614. [DOI] [PubMed] [Google Scholar]
- 11.Cennamo V, Fuccio L, Zagari RM, et al. Can early precut implementation reduce endoscopic retrograde cholangiopancreatography-related complication risk?: meta-analysis of randomized controlled trials. Endoscopy. 2010;42:381–388. doi: 10.1055/s-0029-1243992. [DOI] [PubMed] [Google Scholar]
- 12.Itoi T, Yasuda I, Doi S, et al. Endoscopic hemostasis using covered metallic stent placement for uncontrolled post-endoscopic sphincterotomy bleeding. Endoscopy. 2011;43:369–372. doi: 10.1055/s-0030-1256126. [DOI] [PubMed] [Google Scholar]
- 13.Dumonceau JM, Andriulli A, Elmunzer BJ, et al. Prophylaxis of post-ERCP pancreatitis: European Society of Gastrointestinal Endoscopy (ESGE) Guideline: updated June 2014. Endoscopy. 2014;46:799–815. doi: 10.1055/s-0034-1377875. [DOI] [PubMed] [Google Scholar]
- 14.Harewood GC, Pochron NL, Gostout CJ. Prospective, randomized, controlled trial of prophylactic pancreatic stent placement for endoscopic snare excision of the duodenal ampulla. Gastrointest Endosc. 2005;62:367–370. doi: 10.1016/j.gie.2005.04.020. [DOI] [PubMed] [Google Scholar]
- 15.Syrén EL, Sandblom G, Enochsson L, et al. Outcome of ERCP related to case-volume. Surg Endosc. 2022;36:5339–5347. doi: 10.1007/s00464-021-08915-y. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Elmunzer BJ, Scheiman JM, Lehman GA, et al. A randomized trial of rectal indomethacin to prevent post-ERCP pancreatitis. N Engl J Med. 2012;366:1414–1422. doi: 10.1056/NEJMoa1111103. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Ishiwatari H, Urata T, Yasuda I, et al. No benefit of oral diclofenac on post-endoscopic retrograde cholangiopancreatography pancreatitis. Dig Dis Sci. 2016;61:3292–3301. doi: 10.1007/s10620-016-4251-x. [DOI] [PubMed] [Google Scholar]
- 18.Kato K, Shiba M, Kakiya Y, et al. Celecoxib oral administration for prevention of post-endoscopic retrograde cholangiopancreatography pancreatitis: a randomized prospective trial. Pancreas. 2017;46:880–886. doi: 10.1097/MPA.0000000000000852. [DOI] [PubMed] [Google Scholar]
- 19.Staritz M, Poralla T, Ewe K, et al. Effect of glyceryl trinitrate on the sphincter of Oddi motility and baseline pressure. Gut. 1985;26:194–197. doi: 10.1136/gut.26.2.194. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Wehrmann T, Schmitt T, Stergiou N, et al. Topical application of nitrates onto the papilla of Vater: manometric and clinical results. Endoscopy. 2001;33:323–328. doi: 10.1055/s-2001-13687. [DOI] [PubMed] [Google Scholar]
- 21.Bai Y, Xu C, Yang X, et al. Glyceryl trinitrate for prevention of pancreatitis after endoscopic retrograde cholangiopancreatography: a meta-analysis of randomized, double-blind, placebo-controlled trials. Endoscopy. 2009;41:690–695. doi: 10.1055/s-0029-1214951. [DOI] [PubMed] [Google Scholar]
- 22.Sotoudehmanesh R, Eloubeidi MA, Asgari AA, et al. A randomized trial of rectal indomethacin and sublingual nitrates to prevent post-ERCP pancreatitis. Am J Gastroenterol. 2014;109:903–909. doi: 10.1038/ajg.2014.9. [DOI] [PubMed] [Google Scholar]
- 23.Tomoda T, Kato H, Ueki T, et al. Combination of diclofenac and sublingual nitrates is superior to diclofenac alone in preventing pancreatitis after endoscopic retrograde cholangiopancreatography. Gastroenterology. 2019;156:1753–1760. doi: 10.1053/j.gastro.2019.01.267. [DOI] [PubMed] [Google Scholar]
- 24.Wu M, Jiang S, Lu X, et al. Aggressive hydration with lactated ringer solution in prevention of post-endoscopic retrograde cholangiopancreatography pancreatitis: a systematic review and meta-analysis. Medicine (Baltimore) 2021;100:e25598. doi: 10.1097/MD.0000000000025598. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Sperna Weiland CJ, Engels MM, et al. Increased use of prophylactic measures in preventing post-endoscopic retrograde cholangiopancreatography pancreatitis. Dig Dis Sci. 2021;66:4457–4466. doi: 10.1007/s10620-020-06796-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Tarnasky PR, Palesch YY, Cunningham JT, et al. Pancreatic stenting prevents pancreatitis after biliary sphincterotomy in patients with sphincter of Oddi dysfunction. Gastroenterology. 1998;115:1518–1524. doi: 10.1016/s0016-5085(98)70031-9. [DOI] [PubMed] [Google Scholar]
- 27.Fan JH, Qian JB, Wang YM, et al. Updated meta-analysis of pancreatic stent placement in preventing post-endoscopic retrograde cholangiopancreatography pancreatitis. World J Gastroenterol. 2015;21:7577–7583. doi: 10.3748/wjg.v21.i24.7577. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Ito K, Fujita N, Noda Y, et al. Can pancreatic duct stenting prevent post-ERCP pancreatitis in patients who undergo pancreatic duct guidewire placement for achieving selective biliary cannulation?: a prospective randomized controlled trial. J Gastroenterol. 2010;45:1183–1191. doi: 10.1007/s00535-010-0268-7. [DOI] [PubMed] [Google Scholar]
- 29.Tse F, Yuan Y, Bukhari M, et al. Pancreatic duct guidewire placement for biliary cannulation for the prevention of post-endoscopic retrograde cholangiopancreatography (ERCP) pancreatitis. Cochrane Database Syst Rev. 2016;(5):CD010571. doi: 10.1002/14651858.CD010571.pub2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Freeman ML, Overby C, Qi D. Pancreatic stent insertion: consequences of failure and results of a modified technique to maximize success. Gastrointest Endosc. 2004;59:8–14. doi: 10.1016/s0016-5107(03)02530-6. [DOI] [PubMed] [Google Scholar]
- 31.Tse F, Liu J, Yuan Y, et al. Guidewire-assisted cannulation of the common bile duct for the prevention of post-endoscopic retrograde cholangiopancreatography (ERCP) pancreatitis. Cochrane Database Syst Rev. 2022;3(3):CD009662. doi: 10.1002/14651858.CD009662.pub3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Cotton PB, Eisen GM, Aabakken L, et al. A lexicon for endoscopic adverse events: report of an ASGE workshop. Gastrointest Endosc. 2010;71:446–454. doi: 10.1016/j.gie.2009.10.027. [DOI] [PubMed] [Google Scholar]
- 33.Cirocchi R, Kelly MD, Griffiths EA, et al. A systematic review of the management and outcome of ERCP related duodenal perforations using a standardized classification system. Surgeon. 2017;15:379–387. doi: 10.1016/j.surge.2017.05.004. [DOI] [PubMed] [Google Scholar]
- 34.Enns R, Eloubeidi MA, Mergener K, et al. ERCP-related perforations: risk factors and management. Endoscopy. 2002;34:293–298. doi: 10.1055/s-2002-23650. [DOI] [PubMed] [Google Scholar]
- 35.Kumbhari V, Sinha A, Reddy A, et al. Algorithm for the management of ERCP-related perforations. Gastrointest Endosc. 2016;83:934–943. doi: 10.1016/j.gie.2015.09.039. [DOI] [PubMed] [Google Scholar]
- 36.Langerth A, Isaksson B, Karlson BM, et al. ERCP-related perforations: a population-based study of incidence, mortality, and risk factors. Surg Endosc. 2020;34:1939–1947. doi: 10.1007/s00464-019-06966-w. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Stapfer M, Selby RR, Stain SC, et al. Management of duodenal perforation after endoscopic retrograde cholangiopancreatography and sphincterotomy. Ann Surg. 2000;232:191–198. doi: 10.1097/00000658-200008000-00007. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Parlak E, Köksal A, Dişibeyaz S, et al. Endoscopic closure of ERCP-related duodenal perforations by using endoclips: a case series. Surg Laparosc Endosc Percutan Tech. 2013;23:e225–e228. doi: 10.1097/SLE.0b013e31828b8622. [DOI] [PubMed] [Google Scholar]
- 39.Tyberg A, Zerbo S, Sharaiha RZ, et al. Endoscopic management of a GI perforation. Gastrointest Endosc. 2015;82:955. doi: 10.1016/j.gie.2015.05.034. [DOI] [PubMed] [Google Scholar]
- 40.Khater S, Rahmi G, Perrod G, et al. Over-the-scope clip (OTSC) reduces surgery rate in the management of iatrogenic gastrointestinal perforations. Endosc Int Open. 2017;5:E389–E394. doi: 10.1055/s-0043-104862. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Hyun JJ, Kozarek RA, Irani SS. Endoscopic suturing of a large type I duodenal perforation. VideoGIE. 2018;4:78–80. doi: 10.1016/j.vgie.2018.04.008. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Zhang LY, Bejjani M, Ghandour B, et al. Endoscopic through-the-scope suturing. VideoGIE. 2021;7:46–51. doi: 10.1016/j.vgie.2021.08.006. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Patil NS, Solanki N, Mishra PK, et al. ERCP-related perforation: an analysis of operative outcomes in a large series over 12 years. Surg Endosc. 2020;34:77–87. doi: 10.1007/s00464-019-06733-x. [DOI] [PubMed] [Google Scholar]
- 44.Vezakis A, Fragulidis G, Polydorou A. Endoscopic retrograde cholangiopancreatography-related perforations: diagnosis and management. World J Gastrointest Endosc. 2015;7:1135–1141. doi: 10.4253/wjge.v7.i14.1135. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.Odemis B, Oztas E, Kuzu UB, et al. Can a fully covered self-expandable metallic stent be used temporarily for the management of duodenal retroperitoneal perforation during ERCP as a part of conservative therapy? Surg Laparosc Endosc Percutan Tech. 2016;26:e9–e17. doi: 10.1097/SLE.0000000000000240. [DOI] [PubMed] [Google Scholar]
- 46.Theopistos V, Theocharis G, Konstantakis C, et al. Non-operative management of type 2 ERCP-related retroperitoneal duodenal perforations: a 9-year experience from a single center. Gastroenterology Res. 2018;11:207–212. doi: 10.14740/gr1007w. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47.Arvanitakis M, Dumonceau JM, Albert J, et al. Endoscopic management of acute necrotizing pancreatitis: European Society of Gastrointestinal Endoscopy (ESGE) evidence-based multidisciplinary guidelines. Endoscopy. 2018;50:524–546. doi: 10.1055/a-0588-5365. [DOI] [PubMed] [Google Scholar]
- 48.Paspatis GA, Arvanitakis M, Dumonceau JM, et al. Diagnosis and management of iatrogenic endoscopic perforations: European Society of Gastrointestinal Endoscopy (ESGE) position statement: update 2020. Endoscopy. 2020;52:792–810. doi: 10.1055/a-1222-3191. [DOI] [PubMed] [Google Scholar]
- 49.Mashiana HS, Dhaliwal AS, Sayles H, et al. Endoscopic retrograde cholangiopancreatography in cirrhosis - a systematic review and meta-analysis focused on adverse events. World J Gastrointest Endosc. 2018;10:354–366. doi: 10.4253/wjge.v10.i11.354. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 50.Kim JY, Lee HS, Chung MJ, et al. Bleeding complications and clinical safety of endoscopic retrograde cholangiopancreatography in patients with liver cirrhosis. Yonsei Med J. 2019;60:440–445. doi: 10.3349/ymj.2019.60.5.440. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 51.Oh HC, El Hajj II, Easler JJ, et al. Post-ERCP bleeding in the era of multiple antiplatelet agents. Gut Liver. 2018;12:214–218. doi: 10.5009/gnl17204. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 52.Veitch AM, Radaelli F, Alikhan R, et al. Endoscopy in patients on antiplatelet or anticoagulant therapy: British Society of Gastroenterology (BSG) and European Society of Gastrointestinal Endoscopy (ESGE) guideline update. Gut. 2021;70:1611–1628. doi: 10.1136/gutjnl-2021-325184. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 53.Parras Castañera E, Rodríguez López P, Álvarez A, et al. Predictive factors for post-ERCP bleeding: influence of direct oral anticoagulants. Rev Esp Enferm Dig. 2021;113:591–596. doi: 10.17235/reed.2020.7547/2020. [DOI] [PubMed] [Google Scholar]
- 54.Nakaji S, Hirata N, Matsui H, et al. Hemodialysis is a strong risk factor for post-endoscopic sphincterotomy bleeding in patients with choledocholithiasis. Endosc Int Open. 2018;6:E568–E574. doi: 10.1055/a-0587-4470. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 55.Bae SS, Lee DW, Han J, et al. Risk factor of bleeding after endoscopic sphincterotomy in average risk patients. Surg Endosc. 2019;33:3334–3340. doi: 10.1007/s00464-018-06623-8. [DOI] [PubMed] [Google Scholar]
- 56.Lee HJ, Cho CM, Heo J, et al. Impact of hospital volume and the experience of endoscopist on adverse events related to endoscopic retrograde cholangiopancreatography: a prospective observational study. Gut Liver. 2020;14:257–264. doi: 10.5009/gnl18537. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 57.ASGE Standards of Practice Committee. Acosta RD, Abraham NS, et al. The management of antithrombotic agents for patients undergoing GI endoscopy. Gastrointest Endosc. 2016;83:3–16. doi: 10.1016/j.gie.2015.09.035. [DOI] [PubMed] [Google Scholar]
- 58.Feng Y, Zhu H, Chen X, et al. Comparison of endoscopic papillary large balloon dilation and endoscopic sphincterotomy for retrieval of choledocholithiasis: a meta-analysis of randomized controlled trials. J Gastroenterol. 2012;47:655–663. doi: 10.1007/s00535-012-0528-9. [DOI] [PubMed] [Google Scholar]
- 59.Mirjalili SA, Stringer MD. The arterial supply of the major duodenal papilla and its relevance to endoscopic sphincterotomy. Endoscopy. 2011;43:307–311. doi: 10.1055/s-0030-1256229. [DOI] [PubMed] [Google Scholar]
- 60.Wilcox CM, Canakis J, Mönkemüller KE, et al. Patterns of bleeding after endoscopic sphincterotomy, the subsequent risk of bleeding, and the role of epinephrine injection. Am J Gastroenterol. 2004;99:244–248. doi: 10.1111/j.1572-0241.2004.04058.x. [DOI] [PubMed] [Google Scholar]
- 61.Liu F, Wang GY, Li ZS. Cap-assisted hemoclip application with forward-viewing endoscope for hemorrhage induced by endoscopic sphincterotomy: a prospective case series study. BMC Gastroenterol. 2015;15:135. doi: 10.1186/s12876-015-0367-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 62.Aranez JL, Miller J, Hughes M, et al. A novel, duodenoscope-friendly endoscopic clip for treating massive upper-GI bleeding secondary to a Dieulafoy lesion. VideoGIE. 2018;3:205–206. doi: 10.1016/j.vgie.2018.02.003. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 63.Bilal M, Chandnani M, McDonald NM, et al. Use of fully covered self-expanding metal biliary stents for managing endoscopic biliary sphincterotomy related bleeding. Endosc Int Open. 2021;9:E667–E673. doi: 10.1055/a-1380-3268. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 64.Dunne R, McCarthy E, Joyce E, et al. Post-endoscopic biliary sphincterotomy bleeding: an interventional radiology approach. Acta Radiol. 2013;54:1159–1164. doi: 10.1177/0284185113491567. [DOI] [PubMed] [Google Scholar]
- 65.ASGE Standards of Practice Committee. Khashab MA, Chithadi KV, et al. Antibiotic prophylaxis for GI endoscopy. Gastrointest Endosc. 2015;81:81–89. doi: 10.1016/j.gie.2014.08.008. [DOI] [PubMed] [Google Scholar]
- 66.Chen M, Wang L, Wang Y, et al. Risk factor analysis of post-ERCP cholangitis: a single-center experience. Hepatobiliary Pancreat Dis Int. 2018;17:55–58. doi: 10.1016/j.hbpd.2018.01.002. [DOI] [PubMed] [Google Scholar]
- 67.Navaneethan U, Jegadeesan R, Nayak S, et al. ERCP-related adverse events in patients with primary sclerosing cholangitis. Gastrointest Endosc. 2015;81:410–419. doi: 10.1016/j.gie.2014.06.030. [DOI] [PubMed] [Google Scholar]
- 68.Othman MO, Guerrero R, Elhanafi S, et al. A prospective study of the risk of bacteremia in directed cholangioscopic examination of the common bile duct. Gastrointest Endosc. 2016;83:151–157. doi: 10.1016/j.gie.2015.05.018. [DOI] [PubMed] [Google Scholar]
- 69.Sethi A, Chen YK, Austin GL, et al. ERCP with cholangiopancreatoscopy may be associated with higher rates of complications than ERCP alone: a single-center experience. Gastrointest Endosc. 2011;73:251–256. doi: 10.1016/j.gie.2010.08.058. [DOI] [PubMed] [Google Scholar]
- 70.Harris A, Chan AC, Torres-Viera C, et al. Meta-analysis of antibiotic prophylaxis in endoscopic retrograde cholangiopancreatography (ERCP) Endoscopy. 1999;31:718–724. doi: 10.1055/s-1999-153. [DOI] [PubMed] [Google Scholar]
- 71.Brand M, Bizos D, O’Farrell P., Jr Antibiotic prophylaxis for patients undergoing elective endoscopic retrograde cholangiopancreatography. Cochrane Database Syst Rev. 2010;(10):CD007345. doi: 10.1002/14651858.CD007345.pub2. [DOI] [PubMed] [Google Scholar]
- 72.Kager LM, Sjouke B, van den Brand M, et al. The role of antibiotic prophylaxis in endoscopic retrograde cholangiopancreatography; a retrospective single-center evaluation. Scand J Gastroenterol. 2012;47:245–250. doi: 10.3109/00365521.2011.643482. [DOI] [PubMed] [Google Scholar]
- 73.Tonolini M, Pagani A, Bianco R. Cross-sectional imaging of common and unusual complications after endoscopic retrograde cholangiopancreatography. Insights Imaging. 2015;6:323–338. doi: 10.1007/s13244-015-0393-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 74.Chandra S, Klair JS, Soota K, et al. Endoscopic retrograde cholangio-pancreatography-obtained bile culture can guide antibiotic therapy in acute cholangitis. Dig Dis. 2019;37:155–160. doi: 10.1159/000493579. [DOI] [PubMed] [Google Scholar]
- 75.Negm AA, Schott A, Vonberg RP, et al. Routine bile collection for microbiological analysis during cholangiography and its impact on the management of cholangitis. Gastrointest Endosc. 2010;72:284–291. doi: 10.1016/j.gie.2010.02.043. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
The patient developed bleeding after the endoscopic sphincterotomy. This persisted despite balloon tamponade and irrigation with diluted adrenaline. Hemostasis was secured by the deployment of a biliary fully covered self-expanding metal stent (https://doi.org/10.5946/ce-2023-013.v1).