

Abstract
Objective:
Root canal treatment (RCT) is a major procedure in dentistry. It aims to relieve the pain of pulpal origin and maintain the affected tooth as a functional unit on the arch. Despite these achievable goals, RCT is sometimes rejected by patients. This study, therefore, sought to assess the reasons for rejection in patients planned for endodontic/RCT.
Materials and Methods:
This was a cross-sectional pilot survey of patients planned for RCT using a self-administered questionnaire. The questionnaire included sociodemographics, the Index for Dental Anxiety and Fear (IDAF-4C), and questions to assess the reasons for rejection of endodontic treatment. Data collected were analysed with IBM Statistical Package for the Social Sciences software program, version 23.0. Descriptive statistics were used; chi-square was used to test the association between categorical variables. Statistical significance was set at P ≤ 0.05.
Result:
Thirty-one patients between the age range of 16 and 81 years, with a mean age of 38.16 ± 17.87, participated in the survey. Only nine (29.03%) of the participants declined to have the treatment. The majority 6(66.7%), and 7(77.8%) of those that refused the treatment did so, due to fear of drilling (P = 0.014) and cost of treatment (P = 0.001), respectively. Mean IDAF-4C was 1.86 ± 0.9 (standard deviation).
The rejection was, however, not affected by past experience, the risk of taking multiple radiographs, and the number of hours or visits for the procedure.
Conclusion:
The cost of treatment and fear of drilling were the major reasons for the rejection of RCT in this study. Therefore, there is a need to further look into making endodontic treatment a more comfortable, less costly, and less fear-provoking procedure for patients.
Keywords: Dental anxiety, endodontics, IDAF-4C, rejection, root canal treatment (RCT)
Introduction
Root canal treatment (RCT) is one of the major and common procedures in dentistry with the aim of relieving the pain of pulpal origin and maintaining the affected tooth as a functional unit on the arch.[1,2]
The procedure involves cleaning and shaping the root canal to remove the infected soft and hard tissue, allow disinfecting irrigants’ access to the apical canal space, create space for the delivery of medicaments with subsequent obturation, and the utmost aim of retaining the integrity of radicular structures and the tooth as a whole.[3] Root canal treatment is a major anxiety-provoking procedure in dentistry,[2,4,5] but despite the advances in the procedure and materials, the fear of the treatment still persists. Hence, the treatment is sometimes rejected by patients.
In addition, dental anxiety (DA) is described as a patient’s specific reaction to stress related to dental treatment, with the stimulus unknown, or not present at that moment.[2] Also, it is a “vague unpleasant feeling accompanied by a premonition that something undesirable is going to happen.”[6] According to Weiner and Sheehan,[7] anxiety and its associated symptoms are most often anticipatory in nature, thus, slightly different from fear. Despite the recent improvements and technological advances in modern dentistry, anxiety about dental treatment and fear of pain associated with dentistry remain widespread.[8] Fear as well as anxiety, are common reasons for many patients not visiting a dentist with consequent avoidance of dental care.[9] This avoidance of dental treatment, leads to poorer oral health and oral health-related quality of life.[10,11] Also, anxiety can result from a conditioned response to a previously painful or traumatic experience with a dentist or can arise from negative beliefs and perceptions of dental situations.[12] It may render patients particularly sensitive to the reception and communication they receive from dental staff and to the outcome of dental treatment in general.[5] Although some studies have reported DA being significantly associated with age, gender, and educational status,[13,14] other studies have reported an increased relationship between DA and type of dental treatment, with RCT and extraction rated high.[15]
Endodontic treatment is one of the feared dental procedures and can sometimes result in tooth extraction because of fear and third-party reports of negative experiences. Anxiety in patients undergoing RCT, as with most patients undergoing invasive medical procedures, may be due to concerns about the physical discomfort caused by the procedure itself.[16] A previous study has shown that patients often do not get to understand the nature of endodontic treatment and many of them rely solely on the professional’s explanation and follow-up care.[17] This further observed that, although some patients evaluated the procedure positively, endodontic procedures were largely viewed negatively.
Patients who need endodontic treatment are often burdened by two main concerns, the length of the procedure and the pain of endodontic treatment which is often accompanied by negative connotations caused by the patient’s unfounded perceptions.[17] The latter reasons may lead to some patients refusing endodontic treatment and preferring to undergo extraction of their teeth rather than RCT. In other cases, patients that are booked for endodontic treatment may not show up without any cogent reason. The foregoing may suggest that fear and anxiety (among others) may be responsible for certain individuals’ turning down endodontic treatment.
Furthermore, assessment of DA has been majorly with the Corah Dental Anxiety Scale (CDAS) and the modified version (MDAS).[18,19] The shortcoming of these scales, however, is taken care of by the Index of Dental Anxiety and Fear (IDAF-4C), which includes the multidimensional construct of fear and anxiety.[20] The IDAF-4C therefore, measures the core fear module with eight questions each for the four components which are; cognitive, physiological, behavioural, and emotional. The IDAF-4C has been validated and found to correlate with MDAS by many researchers.[21,22] There is, however, a lack of studies on endodontic fear as a cause of rejection of RCT as well as the use of the IDAF-4C to measure DA in our environment. This study, therefore, set out to assess the reasons for the rejection of RCT and assess the level of fear in patients being planned for endodontic treatment/RCT.
Materials and Methods
This was a cross-sectional pilot survey of patients planned for RCT in a tertiary dental clinic, in Southwest Nigeria. The study was done in accordance with the ethical standards of the responsible committee on human experimentation (institutional or regional) and with the Helsinki Declaration of 1975, as revised in 2000.[23] Ethical approval was sought from the institution’s ethical review board. A self-administered questionnaire was used to collect the data after informed consent for participation was obtained. The participants included were patients who presented for assessment of their teeth where endodontic treatment (RCT) was planned. The questionnaire included sociodemographics, the eight questions of the IDAF-4C assessing the core fear, and other questions. The other questions (12) asked, assessed the reasons for possible rejection of the procedure. The IDAF-4C core fear module measures the four components of DA and fear and contains two items about each component: physiological, behavioural, cognitive, and emotional. The eight items have five possible responses to each question, ranging from “disagree” (score = 1) to “strongly agree” (score = 5). The total score was calculated by getting the average of the scores of the participants and grouped into low or moderate (<2.5), moderate or high (2.5–3.5), and high to extreme (>3.5). The other questions to assess reasons for rejection had a Yes or No response. The 12 questions were validated and were found acceptable (Cronbach’s alpha- 0.74).
Statistical analysis
Data collected were analysed with IBM Statistical Package for the Social Sciences (SPSS) software program for Windows, version 23.0 (IBM Corporation, Armonk, New York). Descriptive statistics were used; chi-square was used to test the association between categorical variables. Statistical significance was set at P ≤ 0.05.
Result
Thirty-one participants within the age range of 16 and 81 years, with a mean age of 38.16 ± 17.87 years, participated in the survey. The majority (17, 56.7%) of the patients were females. Pain was the reason (100%) for presentation, and most of the participants (22, 71%) were diagnosed with apical periodontitis. Only nine (29.03%) of the participants declined the treatment [Table 1]. Figures 1 and 2 show that the majority of those who refused the treatment did so due to fear of drilling (66.7 %, P = 0.014) and the cost of treatment (77.8%, P = 0.001).
Table 1.
Demographics of participants
| Sociodemographics | Frequency | Percent |
|---|---|---|
| Age group | N | % |
| <20 | 6 | 19.4 |
| 21–40 | 13 | 41.9 |
| 41–60 | 8 | 25.8 |
| >61 | 4 | 12.9 |
| Gender | ||
| Male | 14 | 45.2 |
| Female | 17 | 54.8 |
| Total | 31 | 100 |
| Educational status | ||
| Primary | 3 | 9.7 |
| Secondary | 5 | 16.1 |
| Tertiary | 20 | 64.5 |
| Others | 3 | 9.7 |
| Total | 31 | 100 |
| Diagnosis | ||
| Apical periodontitis | 22 | 71 |
| Irreversible pulpitis | 6 | 19.4 |
| Dentoalveolar abscess | 1 | 3.2 |
| Periapical abscess | 1 | 3.2 |
| Failed RCT | 1 | 3.2 |
| Total | 31 | 100 |
| Acceptance of RCT by patients | ||
| Yes | 22 | 71 |
| No | 9 | 29 |
Figure 1.
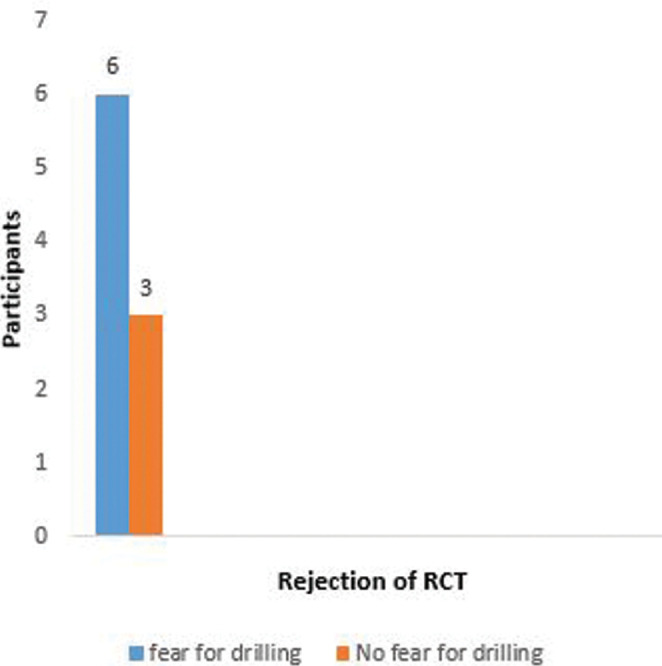
Fear of tooth drilling as a factor for rejection
Figure 2.

Cost of treatment as a factor for rejection of root canal treatment
Rejection of the endodontic treatment was, however not affected by past experience, the risk of taking multiple radiographs, and the number of hours or visits for the procedure. Though a lower proportion (10, 32.3%) of the participants claimed that they were fearful when visiting the dentist, most (6, 66.7%) of the participants in this group were those that rejected the treatment (P = 0.006) [Figure 3].
Figure 3.
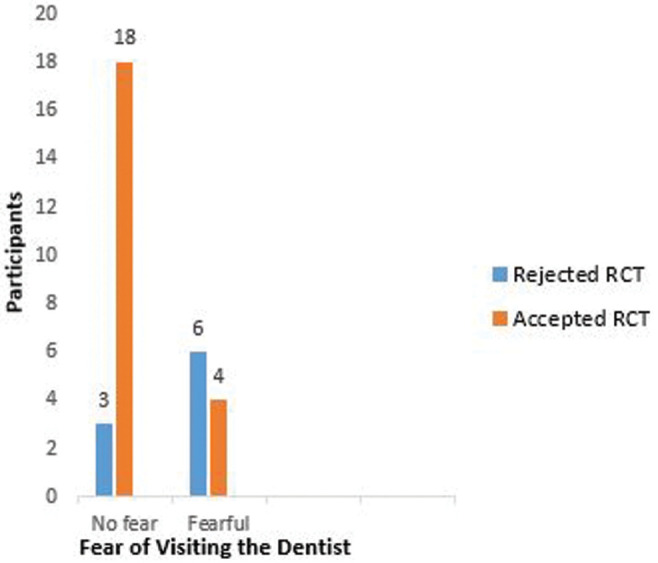
Fear of visiting the dentist as a reason for rejection of RCT
The majority of the participants (24, 77%) were in the low or moderate fear group, and the mean IDAF-4C of the participants was 1.86 ± 0.9 (standard deviation) [Figure 4]. However, more than half (56%) of the people that rejected the procedure fell into IDAF-4C of 2.5– >3.5 and this was statistically significant (P = 0.007) [Table 2]. The IDAF-4C level of fear correlated significantly with some of the reasons for the rejection of the treatment. These were the affordability of treatment, fear of drilling, and fear of injection (P = 0.041, 0.001, and 0.003, respectively).
Figure 4.
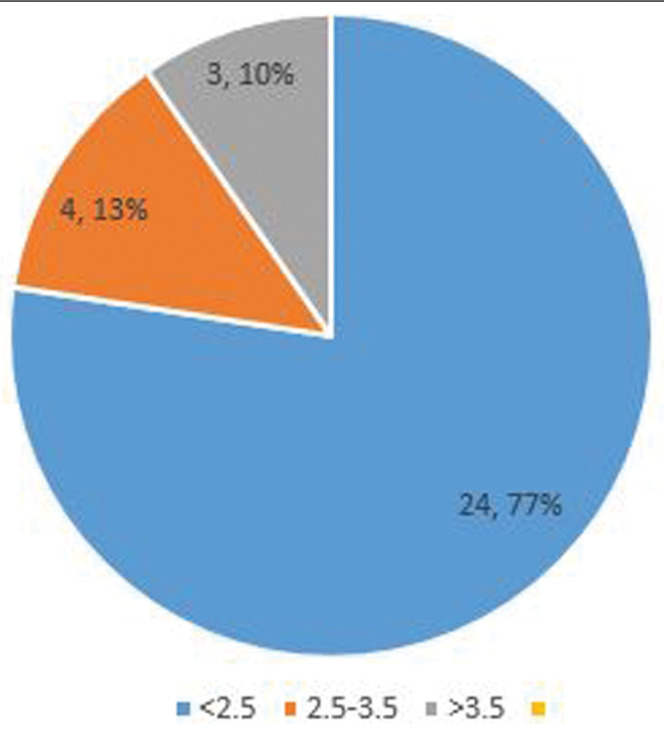
Classification of participants by IDAF-4C
Table 2.
Correlation of index of dental anxiety and fear (IDAF-4C) with acceptance of RCT and sociodemographics of participants
| IDAF-4C categories | ||||
|---|---|---|---|---|
|
| ||||
| <2.5 | 2.5–3.5 | >3.5 | Total | |
| Gender | ||||
| Male | 13 | 1 | 0 | 14 |
| Female | 11 | 3 | 3 | 17 |
| P = 0.14 | ||||
| Age | ||||
| <20 | 5 | 0 | 1 | 6 |
| 21–40 | 9 | 3 | 1 | 13 |
| 41–60 | 6 | 1 | 1 | 8 |
| >60 | 4 | 0 | 0 | 4 |
| P = 0.70 | ||||
| Education | ||||
| Primary | 3 | 0 | 0 | 3 |
| Secondary | 1 | 0 | 0 | 1 |
| Post-secondary | 4 | 0 | 0 | 4 |
| Tertiary | 15 | 4 | 1 | 20 |
| Others | 1 | 0 | 2 | 3 |
| P =0.063 | ||||
| Acceptance of RCT | ||||
| Yes | 20 | 0 | 2 | 22 |
| No | 4 | 2 | 3 | 9 |
| P =0.007* | ||||
*Significant P Value
Discussion
Root canal treatment is an alternative to the extraction of a tooth and its replacement on the arch when the tooth is restorable. Root canal treatment has over 90% success when all the necessary protocols are in place.[24] This pilot study looked at individuals’ rejection of the treatment and possible reasons for their choice.
The majority of the participants (71%) agreed to have RCT on their teeth in this study. This result could reflect an increase in awareness about the treatment. Also, in this study centre, the majority of RCT is done by resident doctors specialising in endodontics, which may increase patients’ confidence in the treatment as also reported by Alghofaily and Alsalleeh.[25] in their study.
Nevertheless, 9 (29%) of the participants declined RCT in this study. This was higher than the 4.09% reported by Sadasiva et al.,[26] and lower than 59% in a survey by the American Association of Endodontists.[25] However, one of the reasons for the rejection of RCT in this study was similar (cost of treatment) to the report of Sadasiva et al.[26] Globally, the cost of dental treatment tends to be expensive, particularly, when it involves conservative procedures such as RCT and prosthetic procedures such as tooth replacement with fixed partial dentures (bridges), and implants retained prosthesis.[27,28] For instance, high cost of conservative dental treatments has been reported in developing countries like Nigeria by previous studies.[29] Umanah et al.[30] reported low posterior teeth RCT which was possibly due to a decline of RCT on such teeth by patients. This decline was associated with financial constraints of the patient, as molar RCT is more expensive. Another reason given by the authors was low motivation on the side of the patient for the treatment. However, RCT with a definitive prosthetic restoration as the first line of treatment for a painful tooth that is restorable (either posterior or anterior teeth), is more cost-effective than extraction followed by replacement of the extracted tooth.[31] Therefore, patients’ education, explanation of the benefits, and cost-effectiveness of RCT versus extraction and replacement of the tooth may improve patients’ acceptance of the procedure.
Furthermore, the psyche of a patient may be affected by the procedure and/or a negative experience of the patient or that of a relative.[32] In concordance with this study, fear/anxiety was another factor presented by Sadaiva et al.,[26] among other reasons for patients’ rejection of RCT. The anxiety developed by individuals toward this procedure has been previously reported in many studies.[16,33,34] It has also been described as a factor that can affect the prognosis of the treatment.[35] Anxiety/fear of RCT may be reduced through psychotherapy after successfully identifying susceptible individuals.[36] The fear of drilling reported in this study has also been reported as a major cause of fear in endodontics.[15,37] Therefore, to plan appropriately and to provide an enabling and friendly environment for such individuals to accept the treatment, it is essential for dentists to identify the causes of fear for RCT and the individuals that may be predisposed to this.
Furthermore, in this study, the IDAF-4C fear assessment module correlated significantly with the reasons for rejection. This further validates the reports on the use of IDAF-4C as a reliable psychometric questionnaire for the assessment of fear among anxious dental patients.[20,21,22,38] However, this study reported no significant difference in IDAF-4C when age and gender were considered. This is similar to other studies[38,39] that have reported no difference in IDAF-4C based on the gender and age of the patients.
The possible pain associated with RCT is a major source of fear and should be a concern to the dentist.[40] The fear of pain in the treatment includes that, from local anaesthesia, and pain during and after the treatment. This is reflected in this study, as fear of pain from local anaesthetic injection correlated significantly with the anxiety and fear scale. Hence, dentists should endeavour to make the procedure as comfortable as possible, in other to gain the trust of the patients.[41] Furthermore, it is important to find solutions to alleviate the patient’s fear of the procedure besides motivating the patient towards receiving the treatment.
Also, there are many advances in the field of endodontics that have been developed towards improvement in diagnosis such as cone beam computed tomography (CBCT),[42] equipment/instrument, techniques,[43] and materials.[44] These advances have resulted in an overall increase in the success rate of the treatment.[45] Having such advances in place may reassure patients about the success of the treatment. In addition, patients should be encouraged to accept RCT, using evidence-based reports and educative videos on RCT, as suggested by the American Association of Endodontists.[46]
Though the study area is a resource-limited environment; it is essential to gradually develop toward the provision of a standard level of care that is comparable to that in the developed world. Therefore, dentists, healthcare providers, and policymakers should make available all that is necessary for the improvement of the health-related quality of life.
Limitation of study: This study was a cross-sectional pilot survey with small sample size and thus, may not be generalizable.
Conclusion
This study showed that some degree of fear and the cost of treatment were reasons for the rejection of RCT. It also showed that the level of fear in patients correlated with the rejection of the procedure. Hence, there is a need to seek further on how to make endodontic treatment comfortable and less fear-provoking in a resource-constrained clime. In addition, further studies with larger sample size can be conducted to give more insight on the factors that affect RCT rejection and how to address them.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- 1.Chugal NM, Clive JM, Spangberg LSW. Endodontic infection: Some biologic and treatment factors associated with outcome. Oral Surg, Oral Med, Oral Pathol, Oral Radiol and Endod. 2003(96):81–90. doi: 10.1016/s1079-2104(02)91703-8. [DOI] [PubMed] [Google Scholar]
- 2.Wali A, Siddiqui TM, Gul A, Khan A. Analysis of level of anxiety and fear before and after endodontic treatment. J Dent Oral Health. 2016(2):2–5. [Google Scholar]
- 3.Young GR, Parashos P, Messer HH. The principles of techniques for cleaning root canals. Aust Dent J. 2007;52:S52–63. doi: 10.1111/j.1834-7819.2007.tb00526.x. [DOI] [PubMed] [Google Scholar]
- 4.Alshathri N, Dada B, Alghofaili R, Altuwairqi D, Ghaida G, Alzabin A. The relationship between dental anxiety level and patients’ knowledge of the procedure. Int J Dent Oral Heal. 2017;3:92–102. [Google Scholar]
- 5.Peretz B, Moshonov J. Dental anxiety among patients undergoing endodontic treatment. JOE. 1998(24):435–7. doi: 10.1016/S0099-2399(98)80028-9. [DOI] [PubMed] [Google Scholar]
- 6.Kent GG, Blinkhorn AS. The Psychology of Dental Care. 2nd ed. Bristol: Wright; 1991. [Google Scholar]
- 7.Weiner AA, Sheehan DV. Differentiating anxiety panic disorders from psychologic dental anxiety. Dent Clin North Am. 1988(32):823–40. [PubMed] [Google Scholar]
- 8.Chen WJ, Carter A, Boschen M, Love RM, George R. Fear and anxiety pathways associated with root canal treatments amongst a population of east asian origin. Eur Endod J. 2020(1):2–5. doi: 10.14744/eej.2019.46338. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Bashiru BO, Omotola OE. Prevalence and determinants of dental anxiety among adult population in Benin City, Nigeria. Eur J Gen Dent. 2016(5):99–103. [Google Scholar]
- 10.Eitner S, Wichmann M, Paulsen A, Holst S. Dental anxiety: An epidemiological study on its clinical correlation and effects on oral health. J Oral Rehabil. 2006(33):588–93. doi: 10.1111/j.1365-2842.2005.01589.x. [DOI] [PubMed] [Google Scholar]
- 11.Armfield J, Slade G, Spencer A. Dental fear and adult oral health in Australia. Community Dentistry and Oral Epidemiology. 2009(37):220–30. doi: 10.1111/j.1600-0528.2009.00468.x. [DOI] [PubMed] [Google Scholar]
- 12.Beaton L, Freeman R, Humphris G. Why are people afraid of the dentist? Observations and explanations. Med Princ Pract. 2014;23:295–301. doi: 10.1159/000357223. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Acharya S. Factors affecting dental anxiety and beliefs in an Indian population. J Oral Rehabil. 2008(35):259–67. doi: 10.1111/j.1365-2842.2007.01777.x. [DOI] [PubMed] [Google Scholar]
- 14.Mohammed RB, Lalithamma T, Varma DM, Sudhakar KNV, Srinivas B, Krishnamraju PV, et al. Prevalence of dental anxiety and its relation to age and gender in coastal Andhra (Visakhapatnam) population, India. J Nat Sci Biol Med. 2014;5:409–14. doi: 10.4103/0976-9668.136210. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Udoye CI, Oginni AO, Oginni FO. Dental anxiety among patients undergoing various dental treatments in a Nigerian teaching hospital. J Contemp Dent Pract. 2005(6):91–8. [PubMed] [Google Scholar]
- 16.American Association of Endodontists: This Halloween, People More Scared of Root Canals Than Spiders, Snakes, Sharks Chicago, USA 2019. [Last accessed on 1 Jul 2022]. Available from: https://www.aae.org/specialty/communique/study-this-halloween-people-morescared-of-root-canals-than-spiders-snakes-sharks.
- 17.Melgaço-Costa J, Martins R, Ferreira E, Sobrinho A. Patients’ perceptions of endodontic treatment as part of public health services: A qualitative study. Int J Environ Res Public Health. 2016;13:450. doi: 10.3390/ijerph13050450. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Facco E, Zanette G, Manani G. Italian version of Corah’s dental anxiety scale: Normative data in patients undergoing oral surgery and relationship with the ASA physical status classification. Anesthesia Progress. 2008(55):109–15. doi: 10.2344/0003-3006-55.4.109. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Koleoso ON, Akhigbe KO. Prevalence of dental anxiety and the psychometric properties of modified dental anxiety scale in Nigeria. World J Dent. 2014(5):53–9. [Google Scholar]
- 20.Armfield JM. Development and psychometric evaluation of the index of dental anxiety and fear (IDAF-4C+) Psychol Assess. 2010(22):279–87. doi: 10.1037/a0018678. [DOI] [PubMed] [Google Scholar]
- 21.Alsanawi EA, Abusaris R, El-Metwally AA. Cross-cultural adaptation and validation of the Arabic version of the Index of Dental Anxiety and Fear (IDAF-4C) J Oral Sci. 2019;61:229–37. doi: 10.2334/josnusd.18-0097. [DOI] [PubMed] [Google Scholar]
- 22.Tolvanen M, Puijola K, Armfield JM, Lahti S. Translation and validation of the Finnish version of the Index of dental anxiety and fear (IDAF-4C+) among dental students. BMC Oral Health. 2017;17:85. doi: 10.1186/s12903-017-0375-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.World Medical Association Declaration of Helsinki. Ethical principles for medical research involving human subjects. JAMA. 2013;310:2191–4. doi: 10.1001/jama.2013.281053. [DOI] [PubMed] [Google Scholar]
- 24.Roda RS, Gettleman BH. Cohen's Pathway of the Pulp. 11th ed. Elsevier; 2016. Nonsurgical Retreatment; pp. 324–86. [Google Scholar]
- 25.Alghofaily M, Alsalleeh F. Levels of anxiety and fear related to non-surgical root canal treatment performed by endodontic residents and endodontists. Front Dent Med. 3:851834. [Google Scholar]
- 26.Sadasiva K, Rayar S, Senthilkumar K, Unnikrishnan M, Jayasimharaj U. Analyzing the reasons for patients opting-out from root canal treatment and preferring extraction in south Indian population: Prospective study. Int J Prosthodont Restor Dent. 2018(8):108–13. [Google Scholar]
- 27.Righolt AJ, Jevdjevic M, Marcenes W, Listl S. Global-,regional-,and country-level economic impacts of dental diseases in 2015. J Dent Res. 2018;97(5):501–7. doi: 10.1177/0022034517750572. [DOI] [PubMed] [Google Scholar]
- 28.Schwendicke F, Herbst SR. Health economic evaluation of endodontic therapies. Int Endod J. 2023(56):207–18. doi: 10.1111/iej.13757. [DOI] [PubMed] [Google Scholar]
- 29.Uguru N, Onwujekwe O, Chibuzo C, Uguru C, Ogu UU. Achieving universal health coverage in Nigeria: The dilemma of accessing dental care in Enugu state, Nigeria, a mixed methods study. Heliyon. 2021;7:e05977. doi: 10.1016/j.heliyon.2021.e05977. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Umanah AU, Osagbemiro BB, Arigbede AO. Pattern of demand for endodontic treatment by adult patients in Port-Harcourt, South-South Nigeria. J West Afr Coll Surg. 2012(2):12–23. [PMC free article] [PubMed] [Google Scholar]
- 31.Pennington MW, Vernazza CR, Shackley P, Armstrong NT, Whitworth JM, Steele JG. Evaluation of the cost effectiveness of root canal treatment using conventional approaches versus replacement with an implant. Int Endod J. 2009;42:874–83. doi: 10.1111/j.1365-2591.2009.01582.x. [DOI] [PubMed] [Google Scholar]
- 32.Carter AE, Carter G, George R. Pathways of fear and anxiety in endodontic patients. Int Endod J. 2015(48):528–32. doi: 10.1111/iej.12343. [DOI] [PubMed] [Google Scholar]
- 33.Perković I, Perić M, Knežević MR, Krmek SJ. The level of anxiety and pain perception of endodontic patients. Acta stomatol Croat. 2014(48):258–67. doi: 10.15644/asc47/4/3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Carter AE, Carter G, Boschen M, AlShwaimi E, George R. Ethnicity and pathways of fear in endodontics. J Endod. 2015;41:1437–40. doi: 10.1016/j.joen.2015.04.014. [DOI] [PubMed] [Google Scholar]
- 35.Murillo-Benitez M, Martin-Gonzalez J, Jimenez-Sanchez MC, Cabanillas-Balsera D, Velasco-Ortega E, Segura-Egea JJ. Association between dental anxiety and intraoperative pain during root canal treatment: A cross-sectional study. Int Endod J. 2020(53):447–54. doi: 10.1111/iej.13245. [DOI] [PubMed] [Google Scholar]
- 36.Appukuttan DP. Strategies to manage patients with dental anxiety and dental phobia: Literature review. Clin Cosmet Investig Dent. 2016(8):35–50. doi: 10.2147/CCIDE.S63626. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Kleinknecht RA, Thorndike RM, McGlynn FD, Harkavy J. Factor analysis of the dental fear survey with cross-validation. J Am Dent Assoc. 1984(108):59–61. doi: 10.14219/jada.archive.1984.0193. [DOI] [PubMed] [Google Scholar]
- 38.Svensson L, Hakeberg M, Wide U. Evaluating the validity of the index of dental anxiety and fear (IDAF-4C+) in adults with severe dental anxiety. Eur J Oral Sc. 2020;28:423–8. doi: 10.1111/eos.12731. [DOI] [PubMed] [Google Scholar]
- 39.Salgarello S, Garo ML, Paganelli C, Vita A, Salvadori M, Audino E. Translation and validation of Italian version of index of dental anxiety and fear (IDAF-4C+): A cross-sectional study. Dent J. 2021;9:149. doi: 10.3390/dj9120149. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Chandraweera L, Goh K, Lai-Tong J, Newby J, Abbott P. 2018. A survey of patients’ perceptions about, and their experiences of, root canal treatment. Aust Endod J. 2019;45:225–32. doi: 10.1111/aej.12312. [DOI] [PubMed] [Google Scholar]
- 41.Jacquot J. Trust in the dentist-patient relationship: a review. J Young Investig. 2005. Jun 1, [Last accessed on 1 Jul 2022]. Available from: https://www.jyi.org/2005-june/2005/6/8/trust-in-the-dentist-patient-relationshipa-review.
- 42.Venkatesh E, Elluru SV. Cone beam computed tomography: Basics and applications in dentistry. J Istanb Univ Fac Dent. 2017;51:S102–S121. doi: 10.17096/jiufd.00289. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Campbell F, Cunliffe J, Darcey J. Current technology in endodontic instrumentation: Advances in metallurgy and manufacture. British Dent J. 2021(231):49–57. doi: 10.1038/s41415-021-3170-1. [DOI] [PubMed] [Google Scholar]
- 44.Vishwanath V, Rao HM. Gutta-percha in endodontics: A comprehensive review of material science. J Conserv Dent. 2019(22):216–22. doi: 10.4103/JCD.JCD_420_18. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.Patel S, Brown J, Pimental T, Kelly R, Abella F, Durack C. Cone beam computed tomography in endodontics- A review of the literature. Int Endod J. 2019;52:1138–52. doi: 10.1111/iej.13115. [DOI] [PubMed] [Google Scholar]
- 46.Association of Endodontists. Videos to Educate Patient on Endodontics. American Association of Endodontists. [Last accessed on 11 Jun 2022]. Available from: https://www.aae.org/specialty/practice-management//managing-a-practice/practice-marketing/patient-professionalvideos.