

Abstract
Introduction and importance
Paget's disease of the nipple is a rare form of ductal carcinoma in situ. It is often associated with an underlying breast cancer or, more rarely, may be isolated with no associated breast neoplasm.
Presentation of case
We report the case of a patient with extensive Paget's disease of the nipple without associated breast lesions, treated by mastectomy with coverage by a dorsalis major flap.
Clinical discussion
The association of Paget's disease of the nipple with breast cancer is the most frequent situation, requiring a complete radiological work-up of the breast. The diagnosis is confirmed by anatomopathological examination combined with immunohistochemistry, the treatment of Paget's disease of the nipple remains controversial, with conservative or radical treatment depending on the extent of the disease and the presence or absence of associated breast cancer.
Conclusion
Paget's disease of the nipple is a rare form of breast cancer. Treatment relies mainly on surgery, which can be either conservative or radical.
Keywords: Paget's disease, Nipple, Breast cancers, Mastectomy, Carcinoma in situ
Highlights
-
•
Paget's disease of the nipple is a rare form of ductal carcinoma in situ, in which adenocarcinoma-like cells infiltrate the epidermis of the nipple-areolar region.
-
•
it is often associated with underlying breast cancer in more than 80% of cases or more rarely be isolated without breast neoplasm
-
•
Diagnosis is confirmed by pathological examination associated with immunohistochemistry
-
•
The treatment of Paget's disease remains controversial between mastectomy and conservative treatment
1. Introduction
Paget's disease of the nipple is a rare form of ductal carcinoma in situ. It corresponds to infiltration of the epidermis of the nipple-areolar region by adenocarcinoma-like cells. It accounts for 1–3 % of breast tumours and is often associated with an underlying breast cancer in over 80 % of cases or, more rarely, may be isolated without breast neoplasm. Paget's disease should be suspected in the presence of any persis0074ent unilateral lesion of the nipple, and only anatomopathological examination combined with immunohistochemistry can confirm the diagnosis. Imaging, based on ultrasound mammography and magnetic resonance imaging (MRI), is of fundamental importance in the search for underlying cancer, which will enable management to be adapted and prognosis to be established. We report a case of extensive Paget's disease of the nipple of atypical clinical presentation, with no underlying neoplasm, which posed a management problem. All our work has been reported in accordance with the SCARE criteria and guidelines (8).
2. Clinical observation
A 68-year-old female patient with no personal or family history of breast cancer, menopausal for 14 years and no menopausal hormone therapy, presented with a pruritic erythematous lesion of the right nipple that had been evolving for over two years and was resistant to topical treatments. Clinical examination revealed an erythematous, desquamative lesion with circular pearly margins covering the entire right breast, extending beyond the infra-mammary fold, with complete disappearance of the nipple-areolar plate (Fig. 1) and no palpable nodules. The left breast was unremarkable. Mammography was not possible on the right and showed no abnormality in the contralateral breast. However, ultrasound exploration was difficult in the face of the skin lesion, showing diffuse infiltration of the right breast (Fig. 2), with no solid or cystic lesion in either breast, and a right axillary adenopathy measuring 17 mm. The ultrasound-mammography pair was classified as ACR BI-RADS O on the right and BI-RADS 1 on the left. A breast MRI was performed, showing a retracted right breast with significant thickening and skin enhancement, associated with homolateral axillary adenopathies with no underlying parenchymal tumor process, and a left retroareolar ductal ectasia, with no other suspicious abnormalities detectable (Fig. 3). Skin biopsy was consistent with Paget's disease of the nipple, and cytopuncture of the adenopathy revealed no carcinomatous cells.
Fig. 1.

Clinical aspect of the right breast.
Fig. 2.
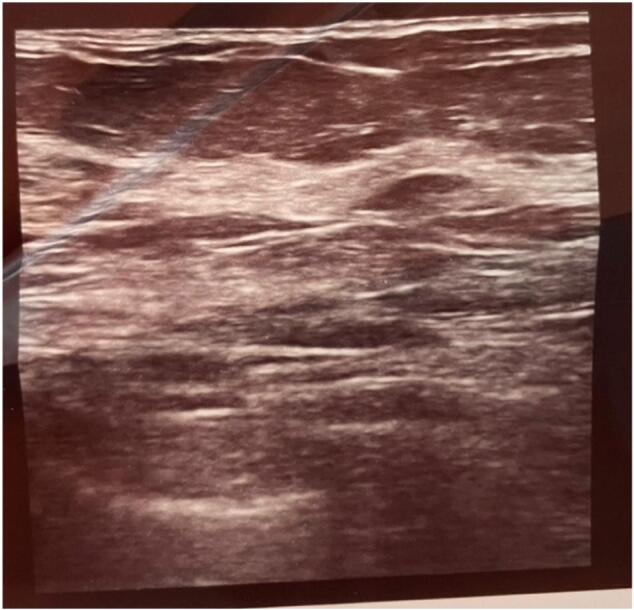
Ultrasound appearance of the right breast.
Fig. 3.
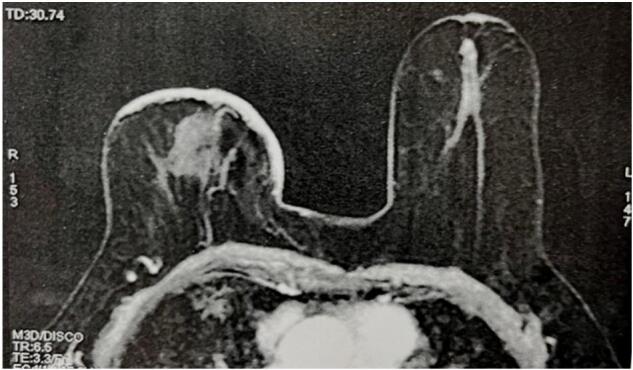
Appearance of right breast on MRI.
The patient underwent a wide right mastectomy (Fig. 4) with sentinel lymph node technique and, given the significant skin deficit, a homolateral greater dorsalis flap was used to cover the defect (Fig. 5). Pathological examination of the mastectomy specimen confirmed extensive Paget's disease of the nipple with no underlying breast lesion, while sentinel lymph node sampling revealed two nodes free of metastatic proliferation.
Fig. 4.

Intraoperative picture of mastectomy.
Fig. 5.

Intraoperative image of mastectomy and latissimus dorsi flap.
3. Discussion
Histologically, Paget's disease corresponds to invasion of the nipple epidermis by lesions of ductal carcinoma in situ, with the presence of so-called Paget's cells in the epidermis (large cells with clear cytoplasm, large irregular hyperchromatic nuclei, seat of mitosis). Two mechanisms have been suggested: migration of Paget cells from an underlying carcinoma, or transformation of nipple keratinocytes independently of any associated breast pathology (3).
Clinically, it manifests as erythematous and eczematous eruptions on the nipple and areola, the extent of which varies according to the age of the lesions. At an advanced stage, it may extend to the entire surface of the breast, with destruction of the entire nipple-areolar plate (5).
The association of Paget's disease of the nipple with breast cancer is the most frequent situation, requiring a complete radiological work-up of the breast (breast ultrasound, mammography and at least breast MRI) in search of an underlying breast lesion, in order to adapt therapeutic management and establish a prognosis (1).
Diagnosis is confirmed by anatomopathological examination combined with immunohistochemistry. Paget's cells express low-molecular-weight cytokeratins, including cytokeratin 7 (CK7), with a sensitivity close to 100 %, helping to confirm the diagnosis (4).
The treatment of Paget's disease remains controversial, with mastectomy long considered the gold standard due to its potential multifocality (3). However, given the low sensitivity of clinical examination and mammography/ultrasound for the detection of underlying breast carcinomas, and their multifocal or multicentric nature, treatment of Paget's disease should be discussed on a case-by-case basis within the framework of a multidisciplinary consultation meeting (2).
In our case, Paget's disease of the nipple was very extensive, so there was no room for conservative treatment, but we had a problem with coverage, so we proceeded with a dorsalis major flap (6).
Our case illustrates, by its clinical and histological originality, the difficulties of diagnostic and therapeutic management that can be encountered in Paget's disease in relation to diagnostic delay; imposing that any persistent anomaly of the nipple must be the subject of a specialized consultation with possibly a skin biopsy (7).
4. Conclusion
Paget's disease of the nipple is a rare entity among breast cancers, often associated with an underlying breast cancer, which needs to be evaluated in order to adjust the therapeutic strategy and determine the prognosis.
The diagnosis is clinically suspected in the presence of a persistent nipple-areolar plaque lesion and confirmed by histology and immunohistochemistry.
Treatment is essentially based on surgery, which may be conservative or radical, depending on the presence or absence of associated cancer and the extent of Paget's disease.
Ethical approval
I declare on my honour that this work has been exempted from ethical approval by my institution, as the dissemination of research results does not allow specific individuals to be identified.
Sources of funding
We have no sources of funding.
CRediT authorship contribution statement
BENCHERIFI Younes: writing the paper and Corresponding author.
BOUSADA Zakaria writing the paper.
NOURI Meriem: writing the paper.
BENHESSOU Mustapha: correction of the paper.
ENNACHIT Simohamed: correction of the paper.
EL KARROUMI Mohammed: correction of the paper.
Guarantor
Dr. Bencherifi Younes.
Registration of research studies
Researchregistry9309.
Provenance and peer review
Not commissioned, externally peer-reviewed.
Consent
Written informed consent was obtained from the patient for publication of this case report and accompanying images. A copy of the written consent is available for review by the Editor-in-Chief of this journal on request.
Declaration of competing interest
The authors declare that they have no conflict of interest.
References
- 1.Ashikari R., Park K., Huvos A.G., Urban J.A. Paget’s disease of the breast. Cancer. 1970;26:680–685. doi: 10.1002/1097-0142(197009)26:3<680::aid-cncr2820260329>3.0.co;2-p. [DOI] [PubMed] [Google Scholar]
- 2.C. Beltrana,∗ , V. Orlandini a , J. Stokkermans-Dubois a , B. Vergier b, J.-M. Fauchier c , M.-S. Doutrea , M. Beylot-Barry Pigmented Paget's disease of the breast. [DOI] [PubMed]
- 3.D. Geffroya, ∗ , I. Doutriaux-Dumoulins a , C. Labbe-Devilliers a , P. Meingana , S. Houdebinea , C. et al Paget's disease of the nipple and differential diagnosis. [DOI] [PubMed]
- 4.Ines Mkhinini ∗ , Ridha Fatnassi , Wassim Saidi , Wadhah Mansouri , Ines Rebhi , Sabrine Kraiem , Houcem Ragmoun Paget's disease of the nipple.
- 5.Léa Manse, Martine BOISSERIE-LACROIX * Nipple Paget's disease.
- 6.Mitchell S., Lachica R., Barry Randall M., Beech D. Paget’s disease of the breast areola mimicking cutaneous melanoma. Breast J. 2006;2:233–236. doi: 10.1111/j.1075-122X.2006.00247.x. [DOI] [PubMed] [Google Scholar]
- 7.Saoussane Kharmoum1,&, Rabie Rahhal Paget's disease of the nipple.
- 8.Agha R.A., Franchi T., Sohrabi C., Mathew G., for the SCARE Group The SCARE 2020 Guideline: updating consensus Surgical CAse REport (SCARE) guidelines. Int. J. Surg. 2020;(84):226–230. doi: 10.1016/j.ijsu.2020.10.034. [DOI] [PubMed] [Google Scholar]