

Abstract
A shortage of physiotherapist (PT) manpower is a barrier for providing better rehabilitation service in Hong Kong. Quality training can benefit patients with better recovery, on the contrary, insufficient training may cause a longer length of stay, readmission, and thus the burden of healthcare system. The estimated cost for PT services in Hospital Authority was HK$7.0 Billion in 2020. A novel Danish robot with a 7-joint robotic arm became popular in Denmark and Germany in the last two years. The robot is designed for lower limb patient rehabilitation. It can enhance the mobility of patients. Based on the experience of a university hospital in Denmark, this robotic rehabilitation was well accepted by both patients and PTs. Function-wise, the robot provides many clinical benefits to patients, especially stroke ones. A physiotherapist’s time can be saved when the robot is being used. The cost-effectiveness of ROBERT is better than PT performing repetitive exercises for lower limbs. The robot potentially provides a cost-effective solution to the Hong Kong healthcare system.
Keywords: Robot, ROBERT, stroke, rehabilitation, length of stay, effectiveness
Background
Physiotherapists (PTs) diagnose and assess injured patients in physical means. Their role is exceptionally essential to stroke rehabilitation. Daras et al. stated that with additional physical activities during Length of Stay (LOS), patients can have better functional independence during discharge and thus lower the readmission opportunity.1 A long LOS of stroke patients results in hospital bed occupation in the Hong Kong Hospital Authority (HA) hospitals. To meet the stroke rehabilitation goals, a guideline from the Royal College of Physicians of United Kingdom recommended that exercise intensity should accumulate to at least 45 min every day.2 Slade et al. conducted a single-blinded research to examine the effect of intensity of physiotherapy upon LOS for 126 stroke patients. The control group received 59 min exercise daily while the Quality Improved (QI) group received 77 min. The mean LOS for all patients was 84.6 days, but the QI group resulted in 14 days LOS (or 16.5%) shorter than the control group with statistical significance.3 Many bedridden patients, who suffer from muscle wasting, are susceptible to increase fall risk. Improved post-stroke patient physical condition enhances mobility and reduces opportunity of complications, e.g., falls and pressure injury. On the contrary, poor physical condition would prolong LOS and increase the potential of readmission in future, which lead to burdening of the healthcare system.
Concern: Burden in Hong Kong Physiotherapy
To the best of our knowledge about acute stroke case number in Hong Kong, there were about 16,900 cases annually between year 1999 and 2007 including new and recurrent cases, which was from Prof. J. Woo’s research team articles.4,5 The mean LOS of 1,111 stroke patients in Kowloon Hospital was 36.6 days.6 The HA Annual Report 2020–2021 showed that the cost for acute or convalescent in-patient service was HK$ 7,240 per patient day.7 With a direct calculation with the above figures, the estimated cost paid by HA for stroke in-patients was HK$ 4.48 billion in 2020.
Apart from post-stroke rehabilitation, PTs also treat other physically injured patients. They served about 1.2 million and 3.0 million PT patient attendances out- and in-patients, respectively, in HA hospitals in 2020.8 The average session cost for specialist outpatient attendance among HA hospitals was HK$1,660.7 Assuming the cost of the PT inpatient service is the same as that of outpatient, the estimated cost for PT service in 2020 in HA was close to HK$7.0 billion. The expenditure on Physiotherapy treatments is considerable. An effective and efficient rehabilitation helps HA save costs and reduce the economic burden.
Cause: PT Manpower Shortage
According to the HA Annual Report 2020–2021, there were 1,248 PTs in HA.7 With a calculation of an ideal case that all 1,248 PTs performing exercise at full throttle, 9 h a day, Monday to Saturday, to 4.2 million in-/out-patient attendances. On average, every attendance receives around 0.72 h or 43.2 min per session by PT. In reality, PTs have to spend time on administration, treatment record documentation, research works, etc. No PT can perform exercise non-stopped for 9 h a day. Some exercises are performed by assistants inevitably. Are the treatments similar in quality? Are PT session durations sufficient in quantity?
Shortage of PT is the major barrier leading PT not being able to provide quality exercise to patients. The Standard dated on 19 June 2017 reported that “The projection done for the government indicated that Hong Kong could see a shortage of 933 physiotherapists by 2030. But two unions and a pressure group from the physiotherapy sector said yesterday the figure is a serious underestimation.9” Currently, there are 3,950 registered practicing PTs on the registration list of the Hong Kong Physiotherapists Board. Among them, about 2,700 PTs are in private practice whereas 1,250 PTs are in HA. Considering the aging population in Hong Kong, physiotherapy is facing a severe manpower shortage issue.
Solution: Robot Therapy
In 2013, Kwok and Ma foresaw that rehabilitation training would be robot-driven in future. Robots can provide more exercises to patients with minimum PT manpower. It saves PT time and assists PTs gather treatment parameters to prepare a tailor-made training.10 Lum et al. and Hug et al. recognised that robot provides a cost-effective means for stroke patients to maintain mobility.11,12 Few criteria were mentioned by Lum et al. to choose a successful Robot therapy system, i.e., the device
-
(1)
must provide quantifiable, functional benefits to patients,
-
(2)
should improve the efficiency of therapists’ current practice,
-
(3)
should be affordable,
-
(4)
should not increase the cost of health care.11
A novel robotic device — ROBERT
Bertelsen et al. shared their experience of a pilot test in geriatric wards of Odense University Hospital with a Danish robot called ROBERT (Life Science Robotics, Aalborg, Denmark). The research employed the passive mobilization of the robot to treat 13 elderly patients. Bertelsen et al. concluded that the pilot test was well accepted by patients, relatives, and staff.13 The system overview is as shown in Fig. 1.
Fig. 1.
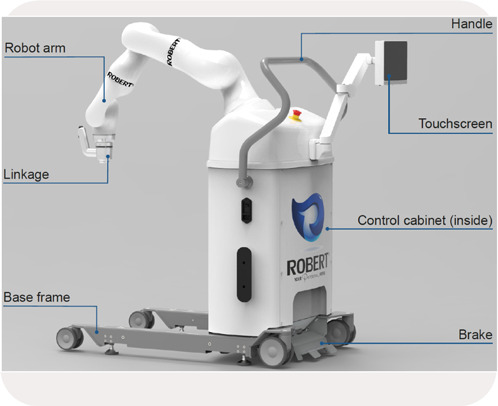
ROBERT system overview.
ROBERT Technical Capabilities
The Danish robot is designed for performing lower limb exercises with a 7-joint robotic arm technology which allows a wide range of movement. The robot can lift an injured leg of maximum 11 kg which is equivalent to a patient body mass of approximately of 160 kg. The PT can move the impaired leg with little effort because the weight of the leg is compensated. With the excellent movement feasibility of the robotic arm, one PT alone can perform Proprioceptive Neuromuscular Facilitation training easily.
There is no built-in program in the robot. It only replicates the exercise path performed by PT. The robot is a tireless workhorse to allow up to 999 repetitions for one exercise. Four exercises can be recorded in one go. The quality of exercise is the same as PT. Repetitive exercises are beneficial to neuroplasticity rewiring. After the PT performs the first cycle of exercise, and hereafter, the robot will start replicating the exercise in certain cycles without any support from the PT. Then, the PT can treat another patient or do some documentation work. The PT efficiency is improved.
Ho et al. mentioned that rehabilitation process should start as early as possible to avoid spasticity.14 The novel robot is good for many stages of lower limb rehabilitation. It allows passive or active mode. Patients in poor condition can be trained in passive mode that the robot brings the impaired leg to move. After the leg gains power, patients can be trained in active mode. The starting point and ending point are set. With no restriction on path, the patient can move his/her leg to reach the destination autonomously, which is good for motor control and learning. There are 10 levels of resistive force for active training. A healthy adult feels hard when the resistive force reaches level 7 or above. The resistive force and number of cycles from the active exercise can form a treatment evolution graph. Thus, a better individualized treatment can be prepared. The robot allows treatment in supine, prone, lateral or sitting positions. This serves bedridden or wheelchair patients. Furthermore, the Danish robot is complementary to exoskeleton devices. Prior to being trained with a walking device, patients can be trained with ROBERT for hip flexion to attain a large extent and for dorsal/plantar orientations (Dorsiflexion 20∘ — Plantar flexion 70 to strengthen their ankles. These improvements would make a walking exercise session more efficient.
The robot is equipped with emergency buttons: One was installed on the control cabinet and one is held by the patient. For safety precaution, the device will automatically stop moving if the patient’s leg is against the movement of the robotic arm, e.g., spasticity or cramp.
The device is mobile with four wheels and weighs 165 kg. It can be moved between wards or stayed in outpatient department. It is equipped with a built-in battery of 30-min power capacity to enable the robot to be powered on during transportation. This saves users four minutes for system rebooting and self-calibration. The device is ready for treatment when it arrives at the bedside of the next patient.
The setup interfaces for PTs are intuitive. That leads the setup quick and learning curve short. A 10-inch touch screen is installed on a swingable holder. During training, the screen is swung close to the patient. The software can be displayed in Chinese or some other popular European languages and the visual is aided by graph presentation. Patients are able to understand the training progress easily.
Bertelsen et al. gave feedback in their pilot test of using ROBERT that about 10–15 min were spent on setup including moving furniture to make space in the ward and attaching the velcro-sheet fixture to the training leg.13 This problem will happen in Hong Kong as well. However, after the setup, patients can be trained uninterruptedly for the rest of the session.
Although other robotic therapy machines are capable to perform the exercises robotically, a PT is required to operate them. There is no manpower saving. However, the ROBERT frees up the PT to help another patient or do other work after the setup. It truly optimizes PT’s precious time.
Cost Effectiveness Analysis
Here is a brief cost-effectiveness analysis between ROBERT and PT and its details are shown in Table 1.
Table 1.
Cost-effectiveness analysis among ROBERT and PT.
| (All currencies are in HK$) | ROBERT | Physiotherapist |
|---|---|---|
| COST | ||
| a. Therapist salary | — | $63,000 |
| b. Daily working hours | 5.25 | 9.00 |
| c. Monthly working days | 26 | 26 |
| d. Machine cost | $1,509,200.00 | — |
| e. Annual maintenance fee | $50,000.00 | — |
| f. Number of year with annual maintenance [Expected Operating Hour/(b x c x 12)hour/year] — Warranty years | 5 (2-year warranty) | — |
| g. Total machine cost [] | $1,759,200.00 | — |
| h. Total hourly cost | $175.92 | $269.23 |
| EFFECTIVENESS | one eff. unit | one eff. unit |
| RESULT | ||
| Cost effectiveness | $175.92/eff. unit | $269.23/eff. unit |
Cost: (1) The robot: The reference price of ROBERT in June 2022 was HK$1,509,200.00 with 10,000 h expected lifetime. The average hourly operating cost is HK$175.92; whereas
(2) The PT: 2022 salary report of Physiotherapists in Hong Kong stated that a mean salary of PT is HK$63,000.00.15 Thus, the hourly salary of PT is HK$269.23.
Effectiveness: The effectiveness of ROBERT and PT is the same because the robot replicates what PT performs. Either effectiveness result is defined as “one eff. unit”.
Cost-Effectiveness Analysis: Dividing the Cost by the Effectiveness for each group, the cost per one eff. unit is calculated.
Cost
A larger value in cost-effectiveness comparison indicates higher cost be paid to obtain the same result.
The cost-effectiveness analysis result showed that employing Danish robot to perform repetitive exercises for lower limbs is less costly than the equivalent performed by PT. Its cost-effectiveness is HK$175.92/one eff. unit; whereas that of PT is HK$269.23/one eff. unit. Although the capital cost of the robotic system is high, its average hourly operating cost is just one-tenth of the cost for one specialty outpatient session in HA hospitals.7
Discussion
Due to a shortage of clinicians, the Hong Kong healthcare system unavoidably considers robots to assist in maintaining or enhancing service quality. The healthcare system is progressing into the robotic era. A Robot-Assisted Gait Training device — Lokomat — was awarded in April 2022 for Kowloon East Cluster. There are a wide variety of evaluations of its effectiveness in locomotor training. van Nunen et al. concluded that there was no significant difference between Lokomat and the conventional training,16 while Duncan et al. showed a better effectiveness ratio of 2.33 than PT did.17 Based on the result from Duncan et al. and the amount of HK$ 1,950,000 on the contract award notice webpage, the cost-effectiveness of Lokomat was translated to about HK$210.55/one eff. unit in locomotor training versus that of PT is HK$269.23/one eff. unit manually.
Robotic treatment with ROBERT fulfils Lum et al.’s criteria of choosing a Robot therapy system. It clinically benefits the patients, especially stroke patients. Therapists’ efficiency will be improved. Its average cost is less than HK$200 per operating hour. It potentially helps reduce the economic burden by reducing LOS and lowering the readmission rate.
Updated on the end of 2021, there have been 13 systems in clinical use, mainly in neurology centres in Denmark and Germany. This technology is innovative and swiftly accepted. Throughout the world, hundreds of patients are treated with it on a daily basis.
Conclusion
The Danish robot benefits patients, PT, and HA quantitatively and qualitatively. It improves patients’ condition, increases patient numbers, releases PT shortage stress, shortens bed occupancy time, and reduces the economic burden. That the robot performs repetitive exercises for lower limbs is less costly than the equivalent performed by PT. ROBERT potentially would be another cost-effective solution for HA.
Conflict of Interest
The author is an employee of a distributor company of ROBERT.
Author Contributions
The author conducted the conception and design of the study, drafted this paper and performed revision of the final version of this paper.
References
- 1. Daras LC, Deutsch A, Ingber MJ, Hefele JG, Perloff J. Inpatient rehabilitation facilities’ hospital readmission rates for medicare beneficiaries treated following a stroke. Top Stroke Rehabil 2021;28(1):61–71. [DOI] [PubMed] [Google Scholar]
- 2. Hancock N, Kilbride C, McGregor L. Physiotherapy concise guide for stroke 2016. Royal College of Physicians, United Kingdom, 2016, www.strokeaudit.org/guideline.
- 3. Slade A, Tennant A, Chamberlain A. A randomised controlled trial to determine the effect of intensity of therapy upon length of stay in a neurological rehabilitation setting. J Rehabil Med 2002;34:260–66. [DOI] [PubMed] [Google Scholar]
- 4. Woo J, Ho SC, Goggins W, Chau PH, Lo SV. Stroke incidence and mortality trends in Hong Kong: Implications for public health education efforts and health resource utilization. Hong Kong Med J 2014;20(S3):S24–9. [PubMed] [Google Scholar]
- 5. Chau PH, Woo J, Goggins W, Tse Y, Chan K, Lo SV, et al. Trends in stroke incidence in Hong Kong differ by stroke subtype. Cerebrovasc Dis 2011;31:138–46. [DOI] [PubMed] [Google Scholar]
- 6. Fung ML. Stroke Rehabilitation: Predicting inpatient length of stay and discharge placement. Hong Kong J Occup Ther 2004;14:3–11. [Google Scholar]
- 7. Hospital Authority Annual Report 2020-2021 Appendixes 8 & 11. Available at https://www.ha.org.hk/haho/ho/cc/HA_Annual_Report_2020-21_en.pdf.
- 8. Hospital Authority Statistical Report 2020-2021; Cluster Reports. Available at https://www3.ha.org.hk/data/HAStatistics/StatisticalReport/2020-2021.
- 9. Shortage of physios sparks warning. The Standard, 19 Jun 2017. Available at https://www.thestandard.com.hk/section-news/section/4/184119/Shortage-of-physios-sparks-.warning#:∼:textA%20manpower%20shortage%20projection%20on%20the%20physiotherapy%20sector,see%20a%20shortage%20of%20933%20physiotherapists%20by%202030.
- 10. Kwok T, Ma E. Clinical applications of technology in rehabilitation. The Hong Kong Med Dairy 2013;18(7):21–2. [Google Scholar]
- 11. Lum P, Reinkensmeyer D, Mahoney R, Rymer WZ, Burgar C. Robotic devices for movement therapy after stroke: Current status and challenges to clinical acceptance. Top Stroke Rehabil 2002;8(4):40–53. [DOI] [PubMed] [Google Scholar]
- 12. Hug A, Spingler T, Hensel C, Fichtner S, Daniel T, Heutehaus L, et al. Goal attainment in mobility after acute rehabilitation of mobility-restricting paralysis syndromes with regard to the ambulatory therapeutic level of participation NeuroMoves. A German national multicenter observational cohort study. BMC Neurol 2021;21(149):1–13. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13. Bertelsen AS, Storm A, Minet L, Ryg J. Use of robot technology in passive mobilization of acute hospitalized geriatric medicine patients: A pilot test and feasibility study. Pilot Feasibility Stud 2020;6(1):1–9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14. Ho L, Ngan PS. Spasticity. News Bull. Hong Kong Physiother. Assoc 2019;23(4):1. [Google Scholar]
- 15. Average Salary of Hong Kong Physiotherapists at year 2022. Available at http://www.salaryexplorer.com/salary-survey.php?loc97&loctype1&job916&jobtype3.
- 16. van Nunen MPM, Gerrits KHL, Konijnenbelt M, Janssen TWJ, de Haan A. Recovery of walking ability using a robotic device in subacute stroke patients: A randomized controlled study. Disabil Rehabil Assist Technol 2014;10(2):141–8. [DOI] [PubMed] [Google Scholar]
- 17. Duncan PW, Sullivan KJ, Behrman AL, Azen SP, Wu SS, Nadeau SE, Dobkin BH, Rose DK, Tilson JK. Protocol for the locomotor experience applied post-stroke (LEAPS) trial: A randomized controlled trial. BMC Neurol 2007;7:39–62. [DOI] [PMC free article] [PubMed] [Google Scholar]