

Abstract
目的
评估3种内镜下改良组织胶方案治疗孤立性胃静脉曲张的疗效。
方法
回顾性分析2008年1月–2019年12月就诊于北京地坛医院的孤立性胃静脉曲张患者73例,收集患者的临床资料,包括年龄、性别、病因、生化指标、Child-Pugh分级、自发性分流的类型、术前出血史、是否合并肝癌等指标。评价内镜下改良组织胶联合聚桂醇治疗、内镜下金属夹辅助组织胶联合聚桂醇治疗、内镜下金属夹和LOOP辅助组织胶联合聚桂醇治疗3种方法的异位栓塞率、生存率、再出血率、聚桂醇和组织胶治疗量、夹子数、治疗次数等临床治疗效果。
结果
患者的基线资料中Child-Pugh分级、术前有无血栓形成、是否合并肝癌在3种治疗方式间比较差异有统计学意义(P<0.05)。3种方法的异位栓塞率差异无统计学意义,但内镜下金属夹辅助组织胶联合聚桂醇治疗方案、内镜下金属夹和LOOP辅助组织胶联合聚桂醇治疗方案无异位栓塞发生。3种治疗方法的生存率、再出血率、聚桂醇和组织胶治疗量差异无统计学意义,但夹子数和1年内治疗次数差异有统计学意义(P<0.05)。
结论
内镜下金属夹辅助组织胶联合聚桂醇治疗、内镜下金属夹和LOOP辅助组织胶联合聚桂醇治疗,这2种改良内镜下组织胶治疗方案可减少孤立性胃静脉曲张患者1年内治疗次数。
Keywords: 孤立性胃静脉曲张, 内镜下治疗, 组织胶联合聚桂醇治疗, 金属夹, LOOP
Abstract
Objective
To evaluate the efficacy of three endoscopic therapies of isolated gastric varices (IGV) with modified tissue adhesive.
Methods
A retrospective analysis was conducted with the clinical data of 73 IGV patients who were treated between January 2008 and December 2019 at Beijing Ditan Hospital. Patient clinical data on age, sex, etiology, biochemistry findings, Child-Pugh classification, the type of spontaneous shunt, preoperative bleeding history, and the presence or absence of liver cancer were collected. The three therapies evaluated were endoscopic intravenous injection of tissue glue combined with lauromacrogol, endoscopic clip-assisted intravenous injection of tissue glue combined with lauromacrogol, and endoscopic clip and LOOP-assisted intravenous injection of tissue glue combined with lauromacrogol. Their respective clinical treatment outcomes, including ectopic embolism rate, survival rate, rebleeding rate, amount of lauromacrogol and tissue glue used, the number of endoscopic clips used, and the number of times of the procedure the patient underwent, were evaluated.
Results
In the patient baseline data, Child-Pugh grade, preoperative thrombus formation, and the presence or absence of liver cancer, showed significant difference between the three therapies (P<0.05). There was no significant difference in the rates of ectopic embolism among the three methods (P>0.05), but no ectopic embolism occurred after endoscopic clip-assisted intravenous injection of tissue glue combined with lauromacrogol, or after endoscopic clip and LOOP-assisted intravenous injection of tissue glue combined with lauromacrogol. There was no significant difference in the survival rate, the rebleeding rate, amount of lauromacrogol and tissue glue used for the three therapies, but there was significant difference in the number of endoscopic clips used and the number of times the procedure was conducted within one year (P<0.05).
Conclusion
The two endoscopic therapies of intravenous injection of modified tissue glue, one assisted by clip and the other assisted by clip and LOOP, can help reduce the number of procedures IGV patients undergo within one year.
Keywords: Isolated gastric varices, Endoscopic treatment, Intravenous injection of tissue glue combined with lauromacrogol, Clip, LOOP
食管胃静脉曲张破裂出血是肝硬化门脉高压最常见、最严重的并发症之一,死亡率高达33%[1-5]。尤其是伴有自发性分流的孤立性胃静脉曲张(isolated gastric varices, IGV),死亡率更高,可达45%~55%[6-10]。近年来内镜技术飞速发展,其操作简单、方便,成为国内外指南推荐的治疗IGV患者出血的一线治疗方案,但治疗过程中可并发致死率极高的肺栓塞、脑梗塞等异位栓塞[11-14]。本文通过总结3种不同的改良内镜下组织胶注射方法治疗IGV,探索内镜治疗的安全性和有效性,减少异位栓塞发生率,降低再出血率,从而提高生存率,为临床治疗提供更多的思路。
1. 资料与方法
1.1. 研究对象
收集2008年1月–2019年12月本院肝硬化伴有IGV患者共73例,随访时间至内镜治疗后1年,回顾性分析其完整临床资料。纳入标准:①明确诊断为肝硬化伴IGV的患者。②不能耐受非选择性β-受体阻断剂的患者。③首次治疗仅愿意接受内镜治疗方案的患者。④患者及家属同意行相关检查,并签署知情同意书,符合医学伦理学要求〔京地伦科字(2018)第(021)-01号〕。排除标准:①合并严重心肺原发疾病及肾功能不全、血液系统疾病等。②治疗过程中行球囊导管闭塞下逆行性静脉栓塞术(balloon-occluded retrograde transvenous obliteration, BRTO)、经颈静脉肝内门体静脉分流术(transjugular intrahepatic portosystemic shunt, TIPS)、外科手术及肝移植患者。③失访或临床资料不完整者。
经排除BRTO 1例、TIPS 1例、外科手术2例、肝移植1例、失访患者2例和临床资料不完整1例后,共纳入患者73例,其中采用内镜下改良组织胶联合聚桂醇治疗22例,采用内镜下金属夹辅助组织胶联合聚桂醇治疗30例,采用内镜下金属夹和LOOP辅助组织胶联合聚桂醇治疗21例。
1.2. 观察指标
基线资料包括性别、年龄、病因、血红蛋白(hemoglobin, HGB)水平、血小板(platelet, PLT)水平、丙氨酸氨基转移酶(alanine aminotransferase, ALT)、天门冬氨酸氨基转移酶(aspartate aminotransferase, AST)、人血白蛋白(albumin, ALB)、肌酐(creatinine, Cr)、国际标准化比值(international normalized ratio, INR)、凝血酶原时间(prothrombin time, PT)Child-Pugh分级、自发分流的类型(包括脾肾分流、胃肾分流和二者均有的混合型)、术前血栓情况、术前有无出血史(经胃镜检查明确诊断)和是否合并肝癌。疗效观察指标:主要指标为有无异位栓塞,次要指标包含生存率、再出血率、首次治疗聚桂醇量、首次治疗组织胶量、夹子数、1年治疗次数、1年聚桂醇总量、1年组织胶总量和术后血栓形成。
1.3. 治疗方案
内镜治疗前行腹部增强CT+门脉重建或门脉超声,评估是否合并自发性分流及分流类型。根据内镜下曲张静脉的大小,逐渐改进治疗方案,分为3组:
第1组(2008–2015年的入组患者)采用改良组织胶联合聚桂醇治疗,具体为“改良三明治法”混合物(2 mL聚桂醇+0.5 mL α-氰基丙烯酸正丁酯+2 mL盐水)分点多次注射治疗,每次每点注射均为前述4.5 mL混合物至曲张静脉实变。见图1。
图 1.
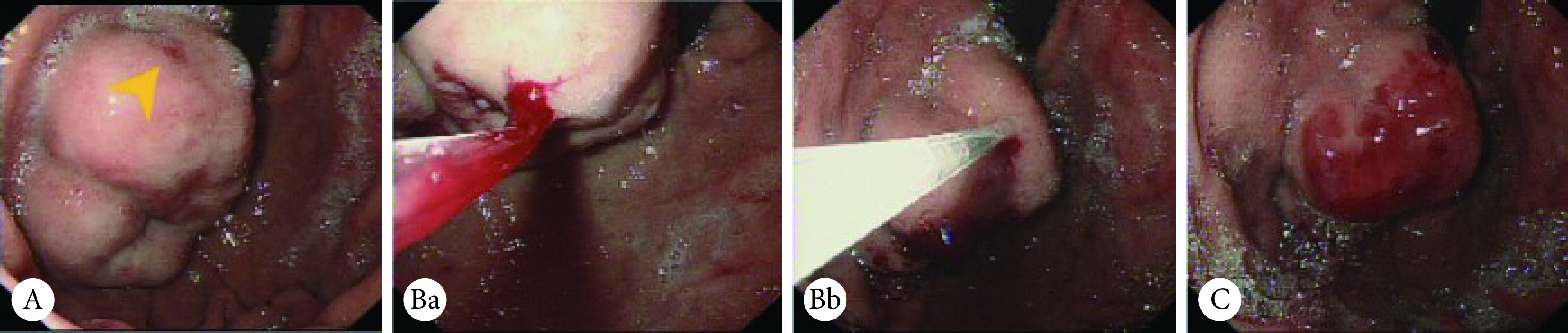
Cyanoacrylate mixture injection of "modified sandwich"
“改良三明治法”治疗图例
A: Before the endoscopic treatment and the erosion (yellow arrow); B: Cyanoacrylate mixture injection of “modified sandwich” (including 2 mL lauromacrogol, 0.5 mL cyanoacrylate and 2 mL sodium chloride in different positions; a: the position of injection to varix close to fundus; b: another position of injection to varix close to cardia); C: Complete the cyanoacrylate mixture injection of “modified sandwich”.
第2组(2016–2019年的入组患者,曲张静脉直径≤10 mm)采用金属夹辅助组织胶联合聚桂醇治疗,具体方法为金属夹(≥2枚)分别置于胃底曲张静脉的流入端与流出端,“改良三明治法”混合物注射于金属夹之间曲张静脉内,注射方法同文献[15]。见图2。
图 2.

Endoscopic clip-assisted cyanoacrylate mixture injection of "modified sandwich"
金属夹辅助“改良三明治法”治疗图例
A: Image taken before the endoscopic treatment and the erosion (yellow arrows); B: Endoscopic clip-assisted cyanoacrylate mixture injection of “modified sandwich” (a: a clip was fixed on the middle of the varix to obstruct partial blood flow, and then the second clip was fixed on the afferent branch to further block the flow; b: the “modified sandwich” cyanoacrylate mixture was injected into the vein between two clips; c: the cyanoacrylate mixture injection into afferent vein and efferent vein at different points separately was continued to block the blood flow thoroughly); C: Completion of the endoscopic clip-assisted cyanoacrylate mixture injection of “modified sandwich” therapy.
第3组(2018–2019年入组患者,曲张静脉团直径>10 mm)采用金属夹和LOOP辅助组织胶联合聚桂醇治疗,具体方法为金属夹(<2枚)辅助LOOP圈套曲张静脉团,分别于圈套的静脉团内、流入端、流出端分点注射“改良三明治法”混合物,注射方法同文献[16]。见图3。
图 3.

Endoscopic clip and LOOP-assisted cyanoacrylate mixture injection of "modified sandwich"
金属夹和LOOP辅助“改良三明治”法治疗图例
A: Image taken before the endoscopic treatment and the erosion (yellow arrow); B: Endoscopic clip and loop-assisted cyanoacrylate mixture injection of “modified sandwich” therapy (a: a clip fixed the LOOP on the fundus, and the LOOP encircled the varix; b: the LOOP was tightened up gradually to obstruct the partial blood flow; c: cyanoacrylate mixture of “modified sandwich” was injected into the circled vein to further break the blood flow, and cyanoacrylate injection into afferent vein and efferent vein at different points separately was continued to block the blood flow thoroughly); C: Completion of the endoscopic clip and LOOP-assisted cyanoacrylate mixture injection of “modified sandwich” therapy.
以上操作由具有10年以上治疗经验的专家按照《肝硬化门脉高压食管胃静脉曲张出血的防治指南》[17]进行规范化操作。
1.4. 随访
术后常规使用生长抑素降低门脉压力、质子泵抑制剂抑酸和抗菌药物治疗,术后1周复查胃镜、复查门脉CT重建或门脉超声,此后每3个月复查胃镜,必要时行重复治疗至曲张静脉消失、门脉超声至术后1年,若有胃静脉曲张再出血随时就诊。研究终点为出现异位栓塞或死亡。再出血标准:静脉曲张患者首次内镜治疗后,再次出现活动性出血,于24 h内血液动力学稳定状态下行胃镜检查明确其出血原因为胃静脉曲张破裂出血。
1.5. 统计学方法
正态分布的计量资料以
 表示,采用t检验进行组间比较;非正态分布的计量资料以中位数(四分位间距)表示,采用秩和检验、log-rank检验进行组间比较;计数资料采用χ2检验进行组间比较。P<0.05为差异有统计学意义。
表示,采用t检验进行组间比较;非正态分布的计量资料以中位数(四分位间距)表示,采用秩和检验、log-rank检验进行组间比较;计数资料采用χ2检验进行组间比较。P<0.05为差异有统计学意义。
2. 结果
纳入本研究的73例患者均为肝硬化患者,行内镜检查明确有IGV,年龄34~81岁,其中8例术前无上消化道出血,65例术前并发上消化道出血(65例中35例明确为IGV破裂出血,30例为原因不明上消化道出血)。73例患者中,乙肝肝硬化28例,丙肝肝硬化7例,酒精性肝硬化12例,自身免疫性肝病肝硬化10例,药物性肝硬化1例,不明原因所致肝硬化15例。
2.1. 基线资料比较
不同治疗方式的3组患者比较,性别、年龄、白蛋白、血红蛋白含量、血小板计数、凝血酶原时间、INR、ALT、AST和Cr、自发性分流类型和术前有无胃静脉曲张出血的发生方面差异无统计学意义。3组患者的Child-Pugh分级为A~B级,在Child-Pugh分级、术前有无血栓形成和是否合并肝癌等方面差异有统计学意义(P<0.05)。见表1。
表 1. Comparison of the baseline data of patients treated with three different endoscopic therapies.
3组不同治疗方式的基线资料比较
| Item | Group 1 (n=22) | Group 2 (n=30) | Group 3 (n=21) | t/H/χ2 | P |
| ALB: Albumin; HGB: Hemoglobin; PLT: Platelet; PT: Prothrombin time; INR: International normalized ratio; ALT: Alanine aminotransferase; AST: Aspartate aminotransferase; Cr: Creatinine. Group 1: Treated by only a cyanoacrylate mixture injection (including 2 mL lauromacrogol, 0.5 mL cyanoacrylate and 2 mL sodium chloride solution); Group 2: Treated by a cyanoacrylate mixture injection with the assistance of endoscopic clip; Group 3: Treated by a cyanoacrylate mixture injection with the assistance of endoscopic clip and LOOP. | |||||
Age/yr.,

|
56.27±13.70 | 60.23±9.81 | 59.86±9.53 | 0.919 | 0.404 |
ALB/(g/L),

|
32.77±6.48 | 33.64±7.99 | 30.46±5.03 | 1.380 | 0.258 |
HGB/(g/L),

|
83.17±23.08 | 89.67±24.89 | 84.95±19.15 | 0.572 | 0.567 |
| PLT/×109 L−1, median (P25, P75) | 77.20 (54.10, 133.50) | 85.50 (49.40, 130.25) | 94.00 (78.00, 132.50) | 1.238 | 0.538 |
| PT/s, median (P25, P75) | 12.80 (11.7, 16.13) | 13.65 (12.63, 15.70) | 14.50 (13.75, 18.30) | 5.210 | 0.740 |
| INR (median [P25, P75]) | 1.32 (1.08, 1.60) | 1.30 (1.17, 1.88) | 1.34 (1.24, 1.59) | 0.957 | 0.620 |
| ALT/(U/L), median (P25, P75) | 24.05 (9.98, 53.18) | 19.95 (12.38, 30.38) | 25.00 (20.35, 37.05) | 1.707 | 0.426 |
| AST/(U/L), median (P25, P75) | 22.45 (14.90, 48.65) | 22.65 (18.30, 31.40) | 29.00 (17.10, 42.60) | 0.590 | 0.744 |
| Cr/(μmol/L), median (P25, P75) | 58.50 (53.23, 67.83) | 66.45 (56.35, 83.18) | 69.40 (59.70, 76.55) | 2.681 | 0.262 |
| (Male/female)/case | 13/9 | 11/19 | 11/20 | 2.790 | 0.248 |
| (Child-Pugh A/B)/case | 10/9 | 25/5 | 11/10 | 7.234 | 0.027 |
| (Slpeno-renal/Gastro-renal/Compound shunt)/case | 8/7/7 | 8/12/10 | 3/8/10 | 5.178 | 0.521 |
| Thrombosis before therapy (yes/no)/case | 0/22 | 1/29 | 2/19 | 8.841 | 0.031 |
| Patient with hepatocellular carcinoma (yes/no)/case | 0/22 | 1/29 | 4/17 | 7.097 | 0.029 |
| Gastric varices hemorrhage before therapy (no/yes/unclear)/case | 5/12/5 | 2/16/12 | 1/7/13 | 9.365 | 0.053 |
2.2. 治疗指标比较
2.2.1. 主要指标
第1组患者中有2例发生异位栓塞,异位栓塞率为9.09%,其他2组患者中均无异位栓塞发生。3组间比较差异无统计学意义。见表2。
表 2. Comparison of the therapeutic indicators of the three different endoscopic therapies.
3组不同治疗方式的治疗指标比较
| Item | Group 1 (n=22) | Group 2 (n=30) | Group 3 (n=21) | χ2/H | P |
| Group 1, Group 2, Group 3: Denotes the same as those in table 1. * One case with liver cancer and portal thrombosis in group 2 and 4 cases with liver cancer and 2 cases with portal thrombosis in group 3 were excluded because liver cancer and portal thrombosis could increase the rebleeding rate. | |||||
| Rate of systemic embolism/case (%) | 2 (9.09) | 0 (0.00) | 0 (0.00) | 4.767 | 0.092 |
| Survival rate/case (%) | 20 (90.91) | 30 (100.00) | 20 (95.24) | 2.694 | 0.260 |
| Rate of post-therapeutic thrombosis/case (%) | 2 (9.09) | 1 (3.33) | 3 (14.29) | 1.966 | 0.369 |
| Rate of rebleeding/case (%)* | 9 (40.91) | 9 (31.03) | 4 (26.67) | 0.251 | 0.618 |
| Volume of cyanoacrylate at first time therapy/mL, median (P25, P75) | 2.75 (1.50, 4.13) | 4.00 (2.75, 4.50) | 3.00 (3.00, 5.00) | 4.046 | 0.132 |
| Volume of lauromacrogol atfirst time therapy/mL, median (P25, P75) | 12.50 (0.00, 20.00) | 10.00 (10.00, 20.00) | 10.00 (10.00, 10.00) | 1.564 | 0.457 |
| Clip number (median [P25, P75]) | 0.00 (0.00, 0.00) | 2.00 (2.00, 3.00) | 2.00 (1.00, 2.00) | 49.36 | 0.000 |
| Volume of cyanoacrylate in one year/mL, median (P25, P75) | 4.75 (3.00, 8.00) | 4.50 (3.00, 7.00) | 5.00 (3.00, 7.25) | 0.734 | 0.693 |
| Volume of lauromacrogol in one year/mL, median (P25, P75) | 20.00 (10.00, 46.63) | 10.00 (10.00, 20.00) | 20.00 (10.00, 50.00) | 5.250 | 0.072 |
| Therapeutic times in one year (median [P25, P75]) | 3.50 (2.00, 5.25) | 3.00 (2.00, 4.00) | 2.00 (2.00, 2.50) | 7.527 | 0.023 |
2.2.2. 次要指标
第1组患者中2例死于异位栓塞,生存率90.91%;第2组患者中无死亡发生,生存率100%;第3组患者中1例死于心源性猝死,生存率95.24%。3组间比较生存率差异无统计学意义。
由表2可见,3组间患者首次治疗聚桂醇量和组织胶量、1年聚桂醇总量和组织胶总量,及术后血栓形成方面差异亦无统计学意义,而夹子数和1年内治疗次数在3组间比较差异有统计学意义(P<0.05)。因患者术前有无血栓形成、是否合并肝癌方面对再出血的发生有影响,故剔除合并肝癌患者5例,合并术前血栓形成3例,其中1例患者既合并肝癌又有术前血栓。剩余患者肝功能为Child-pugh A~B级,组间比较基线资料差异无统计学意义。66例患者经3种不同治疗后进行再出血率比较:第1组22例患者中1年内有9例发生再出血,其再出血率为40.91%;第2组29例患者中1年发生再出血9例,其再出血率为31.03%;第3组15例患者中有4例发生再出血,其再出血率26.67%;差异无统计学意义。
3. 讨论
既往研究发现组织胶治疗IGV,组织胶可沿分流道随体循环流动至全身各重要脏器而出现栓塞,其发生与使用组织胶的剂量呈正相关[18-20]。因此,我们采用“改良三明治”法小剂量多点分次注射,减少组织胶用量,从而达到减少异位栓塞的发生。但在本研究的早期阶段,22例患者中仍有2例发生异位栓塞并死亡,考虑可能与操作者对分流道的血流方向判断不准确,操作手法不熟练有关。为准确判断分流方向,我们术前进行CT门脉重建或腹部超声检查,预评估分流情况后再行内镜下治疗。
MANATAKA等[21]和NI等[22]发现异位栓塞的发生可能与分流血流速度有更大的相关性。我们应用金属夹机械性夹闭血管,能有效阻断部分血流,降低血流速度,同时联合组织胶+聚桂醇治疗少量多点分次注射,从而达到减少异位栓塞发生的目的。自2016年以后本研究中采用此方法治疗30例患者过程中未再有异位栓塞发生。直径大于10 mm的孤立性胃底静脉曲张应用金属夹操作过程中易出现曲张静脉破裂出血,因此我们采用LOOP联合金属夹圈套结扎迂曲粗大静脉团的改良方式,在圈套的静脉团中注射组织胶+聚桂醇混合物,避免操作诱发大出血的风险,有效减慢血流,减少异位栓塞的发生。21例患者采用此方法治疗无异位栓塞发生。3种方法比较异位栓塞发生率差异无统计学意义,但考虑样本量较少,故有待扩大样本量进一步研究观察。
尽管患者在术前有无血栓形成、是否合并肝癌方面基线资料存在差异,但随访时间短,仅有1年,考虑二者对生存率影响不大,同时对组织胶和聚桂醇治疗及术后血栓形成影响亦不大,但对再出血的发生可能存在影响,因门脉血栓形成可进一步增加门脉压力,门脉压力与再出血呈正相关,可加重再出血的发生,故在比较3种方法治疗后再出血的情况时剔除合并这两个因素的病例。3种治疗方法在降低患者1年内再出血率、首次治疗应用组织胶+聚桂醇的量,以及1年组织胶+聚桂醇的总量方面无明显差异。但3组间在金属夹的使用数目和1年内治疗的次数方面,金属夹辅助组织胶联合聚桂醇治疗方案、金属夹和LOOP辅助组织胶联合聚桂醇治疗方案明显减少,由此推断患者住院费用可明显下降,大大减少了患者的经济负担。
本研究尚存不足之处,仅有2例患者组织胶治疗发生了异位栓塞,故未采用多因素回归分析发生异位栓塞的危险因素,下一步拟扩大样本量深入研究。此外,因在操作中易造成曲张静脉破裂大出血而死亡,如何合理地在这3种治疗方案中选择,依赖于内镜医师的经验,对操作者的技术要求较高。
综上所述,内镜下金属夹辅助组织胶联合聚桂醇治疗、内镜下金属夹和LOOP辅助组织胶联合聚桂醇治疗,这2种改良内镜下组织胶治疗方案可减少患者1年内治疗次数,发生异位栓塞的危险因素有待扩大样本量继续研究。
* * *
利益冲突 所有作者均声明不存在利益冲突
Funding Statement
北京市科技新星交叉项目(No. Z191100001119140)资助
Contributor Information
正琳 艾 (Zheng-lin AI), Email: aizhenglin@126.com.
坪 李 (Ping LI), Email: endolp@126.com.
References
- 1.TAYYEM O, BILAL M, SAMUEL R, et al Evaluation and management of variceal bleeding. Dis Mon. 2018;64(7):312–320. doi: 10.1016/j.disamonth.2018.02.001. [DOI] [PubMed] [Google Scholar]
- 2.LESMANA C R A, RAHARJO M, GANI R A Managing liver cirrhotic complications: Overview of esophageal and gastric varices. Clin Mol Hepatol. 2020;26(4):444–460. doi: 10.3350/cmh.2020.0022. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.DE F R. Portal hypertension Ⅶ. Proceedings of the Ⅶth Baveno consensus workshop: Personalized care in portal hypertension. New York, USA: Springer, 2022.
- 4.NORTHUP P C, GARCIA-PAGAN J C, GARCIA-TSAO G, et al Vascular liver disorder, portal vein thrombosis, and procedural bleeding in patients with liver disease: 2020 practice guidance by the American association for the study of liver disease. Hepatolgoy. 2021;73(1):366–413. doi: 10.1002/hep.31646. [DOI] [PubMed] [Google Scholar]
- 5.IBRAHIM M, MOSTAFA I, DEVIERE J New developments in managing variceal bleeding. Gastroenterology. 2018;154(7):1964–1969. doi: 10.1053/j.gastro.2018.02.023. [DOI] [PubMed] [Google Scholar]
- 6.JAKAB S S, GARCIA T G Screening and surveillance of varices in patients with cirrhosis. Clin Gastroenterol Hepatol. 2019;17(1):26–29. doi: 10.1016/j.cgh.2018.03.012. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.LUO X, XIANG T, WU J, et al Endoscopic cyanoacrylate injection versus balloon-occluded retrograde transvenous obliteration for prevention of gastric variceal bleeding: A randomized controlled trial. Hepatology. 2021;74(4):2074–2084. doi: 10.1002/hep.31718. [DOI] [PubMed] [Google Scholar]
- 8.LESMANA C R A, KALISTA K F, SANDRA S, et al Clinical significance of isolated gastric varices in liver cirrhotic patients: A single-referral-centre retrospective cohort study. JGH Open. 2019;4(3):511–518. doi: 10.1002/jgh3.12292. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.DE G A, RAUTOU P E, SCHOUTEN J, et al Porto-sinusoidal vascular disease: Proposal and description of a novel entity. Lancet Gastroenterol Hepatol. 2019;4(5):399–411. doi: 10.1016/S2468-1253(19)30047-0. [DOI] [PubMed] [Google Scholar]
- 10.ALKHAZRAJI A, CURRY M P The current knowledge about the therapeutic use of endoscopic sclerotherapy and endoscopic tissue adhesives in variceal bleeding. Expert Rev Gastroenterol Hepatol. 2019;13(9):893–897. doi: 10.1080/17474124.2019.1652092. [DOI] [PubMed] [Google Scholar]
- 11.IRISAWA A, SHIBUKAWA G, HOSHI K, et al Endoscopic ultrasound-guided coil deployment with sclerotherapy for isolated gastric varices: Case series of feasibility, safety, and long-term follow-up. Dig Endosc. 2020;32(7):1100–1104. doi: 10.1111/den.13666. [DOI] [PubMed] [Google Scholar]
- 12.LEE H A, CHANG J M, GOH H G, et al Prognosis of patients with gastric variceal bleeding after endoscopic variceal obturation according to the type of varices. Eur J Gastroenterol Hepatol. 2019;31(2):211–217. doi: 10.1097/MEG.0000000000001271. [DOI] [PubMed] [Google Scholar]
- 13.LI H, YE D, LI P, et al. Endoscopic clipping prior to GVO vs GVO in IGV1 bleeding: A multicenter retrospective clinical trial. Endosc Int Open. 2019;7(11):E1365–E1370. doi: 10.1055/a-0902-4384. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.DE F R, BOSCH J, GARCIA-TSAO G, et al Baveno Ⅶ-Renewing consensus in portal hypertension. J Hepatol. 2022;76(4):959–974. doi: 10.1016/j.jhep.2021.12.022. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.马佳丽, 陈旭, 洪珊, 等 金属夹联合组织胶注射治疗胃静脉曲张伴自发性门体分流的临床研究(含视频) 中华消化内镜杂志. 2020;37(2):111–114. doi: 10.3760/cma.j.issn.1007-5232.2020.02.007. [DOI] [Google Scholar]
- 16.AI Z L, LI P Loop combined endoscopic clip and cyanoacrylate injection to treat severe gastric varices with spleno-renal shunt. VideoGIE. 2020;5(12):652–654. doi: 10.1016/j.vgie.2020.07.020. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.中华医学会肝病学分会, 中华医学会消化病学分会, 中华医学会内镜学分会 肝硬化门静脉高压食管胃静脉曲张出血的防治指南. 临床肝胆病杂志. 2016;32(2):203–219. doi: 10.3969/j.issn.1001-5256.2016.02.002. [DOI] [Google Scholar]
- 18.ALBAWARDY B, GOROSPE E C, SALEEM A, et al Outcomes and predictors of rebleeding after 2-octyl cyanoacrylate injection in acute gastric variceal hemorrhage. J Clin Gastroenterol. 2016;50(6):458–463. doi: 10.1097/MCG.0000000000000487. [DOI] [PubMed] [Google Scholar]
- 19.SINGH V, SINGH R, BHALLA A, et al Cyanoacrylate therapy for the treatment of gastric varices a new method. J Dig Dis. 2016;17(6):392–398. doi: 10.1111/1751-2980.12351. [DOI] [PubMed] [Google Scholar]
- 20.王芳, 刘仕倩, 曾西, 等 食管胃底静脉曲张伴自发性分流血管栓塞治疗的研究进展. 胃肠病学和肝病学杂志. 2018;27(3):346–350. doi: 10.3969/j.issn.1006-5709.2018.03.024. [DOI] [Google Scholar]
- 21.MANATAKA A, AUGOUSTAKI A, KOUROUMALIS E A, et al Portal vein thrombosis in cirosis: Diagnosis, natural history, and therapeutic challenges. Ann Gastroenterol. 2018;31(3):315–329. doi: 10.20524/aog.2018.0245. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.NI Z, CHEN H, TANG S, et al. The efficacy and the safety of prophylactic -butyl-2-cyanoacrylate injection for gastric varices using a modified injection technique. Surg Laparosc Endosc Percutan Tech, 2016, 26(4): e85−e90[2021-07-26]. https://journals.lww.com/surgical-laparoscopy/Fulltext/2016/08000/The_Efficacy_and_the_Safety_of_Prophylactic.21.aspx. doi: 10.1097/SLE.0000000000000296.