

Abstract
Introduction The surgical management of jugulotympanic paragangliomas has remained challenging. They are the second most common type of tumor of the temporal bone after acoustic neuroma. It has been noticed by the authors that the jugulotympanic paragangliomas may have extensions to the epitympanum and aditus in addition to the mesotympanum and hypotympanum. The modified technique could be an alternative to the conventional facial recess technique for complete removal of the tumors.
Objective To highlight the modified surgical technique for the surgical treatment of jugulotympanic paragangliomas.
Methods This is a retrospective review of 34 cases of jugulotympanic paragangliomas treated in a tertiary center with respect to clinical presentation, diagnosis, and surgical treatment. Tinnitus and hearing loss were predominant symptoms. A modified technique of postauricular transcanal posterior tympanectomy with extended hypotympanic access was performed in 29 patients. Only two cases were operated with a classical transcanal approach. A canal wall down the mastoidectomy was required in three patients.
Results The patients operated on with the modified technique had complete excision evident by absence of any lesion in computed tomography and the disappearance of tinnitus. However, two patients had recurrence of symptoms and presence of tumor in the follow-up period. These two patients underwent revision surgery. None of the patients required postoperative radiotherapy or gamma knife therapy.
Conclusions Jugulotympanic paragangliomas can be effectively managed with the modified technique to ensure complete removal of the lesions. This technique has not been reported earlier in the literature.
Keywords: Glomus tympanicum, Surgical approach, modified surgical technique
Introduction
Tympanic paragangliomas typically arise from the middle ear without involvement of the jugular bulb or jugular foramen. They have a propensity to extend along the path of least resistance to the epitympanum, hypotympanum, and Eustachian tube, or to expand into the mastoid and external auditory canal. A reddish mass behind the tympanic membrane with tinnitus along with conductive loss is the most common presentation. They are benign and slow growing but produce disabling symptoms for which patients seek intervention. Rosenwasser, 1 in 1945, was the first to report a carotid body tumor of the middle ear and mastoid. The preferred term for middle ear paraganglioma is jugulotympanic paraganglioma. They are the second most common type of temporal bone tumor after acoustic neuroma. The female-to-male ratio is usually 4:1. Usually, high-resolution computed tomography is used to study the extent of the tumor and eventual surgical planning.
Jugulotympanic paragangliomas, as per the Glasscock Jackson classification, are of 4 types. I - limited to promontory, II - filling the middle ear space, III - filling the middle ear space and extending to mastoid, and IV - from the mastoid to fill the external auditory canal and may extend anteriorly to the carotid artery. 2 3 Type-I tumors can be safely excised with the transcanal approach. Type-II and -III jugulotympanic paragangliomas have been conventionally excised with the facial recess approach. Tumors with grade-IV extension require standard canal wall mastoidectomy. The facial recess approach, with its extension, was described to gain access to remove the tumor from the retrotympanum and hypotympanic region. 4 However, there is restriction in tumor visualization due to limited exposure to the tumor with increased chances of bleeding. The objective of the present paper is to highlight our experience with a modified technique called postauricular transcanal posterior tympanectomy for type-II and -III tumors. This technique is a head-on approach for excision of the tumor.
Methods and Materials
This is a retrospective review of 34 cases of jugulotympanic paraganglioma treated in a tertiary center between the period from 2009 to 2019. An approval of the institutional ethics committee was obtained for the retrospective review of the cases. These patients underwent surgical excision of the tumor using the modified technique. All the cases were operated by the senior surgeon (N. K. P.). The cases of jugulotympanic paraganglioma were reviewed by analyzing the files and charts with regard to clinical presentation, diagnosis, and surgical management. Pulsatile tinnitus and hearing loss were the predominant symptoms. The tumors were classified according to Glasscock and Jackson. 3 The patients were divided into three subgroups according to surgical procedure performed. Group 1 included patients with type-1 tumors who underwent excision strictly via transcanal approach ( n = 2). Group 2 patients underwent surgery by the modified technique for type-II and -III tumors ( n = 29). Group 3 tumors underwent modified radical mastoidectomy for type-IV tumors ( n = 3). ( Table 1 )
Table 1. Showing the Surgical approaches for Glomus Tympanicum.
| Surgical approach based on extent of tumor. |
| ➢ Type I Transcanal excision |
| ➢ Type II–III Facial recess or extended facial recess |
| ➢ Modified - Postaural posterior tympanectomy approach |
| ➢ Type IV may require a canal wall up mastoidectomy approach |
Brief Overview of the Surgical Steps
Video 1 Video of the surgical procedure
The procedure was performed under general anesthesia. The patient was positioned supine, with the head rotated to the opposite side. After sterile draping, a surgical microscope was placed on the opposite of where the surgeon was. The skin was infiltrated with 2% lignocaine with 1:200,000 adrenaline in the postauricualr region and in the external auditory canal following the Plester technique. A postaural Wilde incision was made, and a large Palva flap elevated in addition to harvesting the temporalis facia. The external auditory canal was entered by making a horizontal incision at the level of the beginning of the bony canal. The tympanomeatal flap was elevated from 12° clock to the 6° clock position till the sulcus tymapanicus and annulus dissected out. The tympanomeatal flap was secured using an aluminum foil, which was held in place with the help of corrugated drain and a mastoid rertractor. The postauricular approach and anterior based periosteal flap enable the surgeon to have additional exposure. ( Fig. 1 )
Fig. 1.
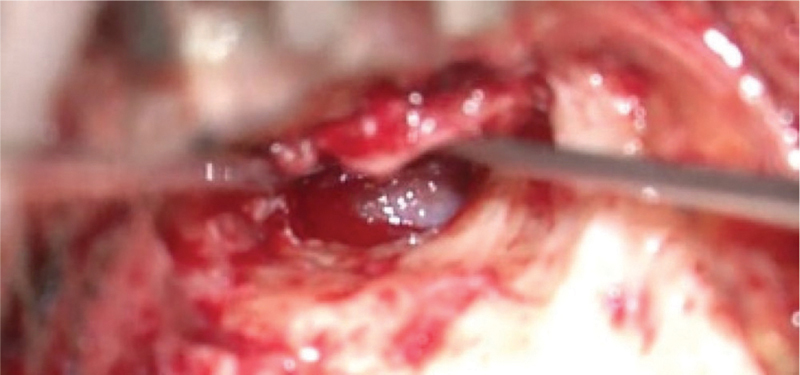
Edited showing the tumor after elevation of the tympanomeatal flap.
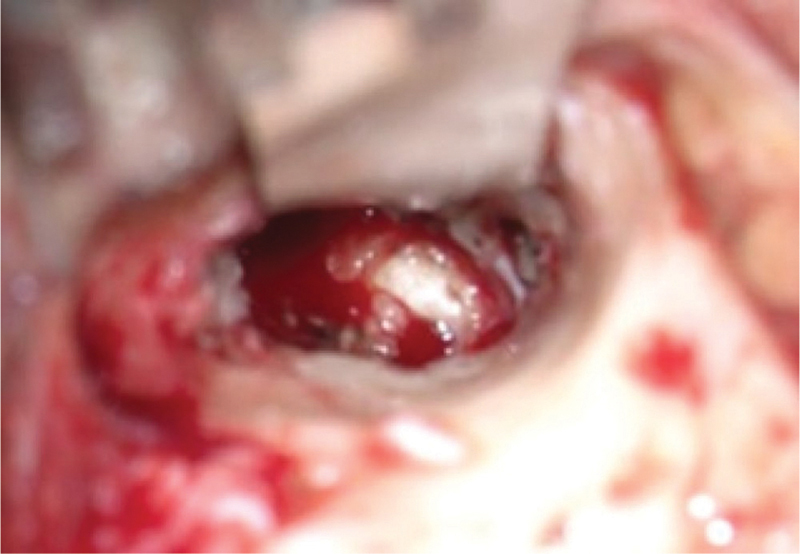
The extent and margin of the tumor were examined all around. The drilling commenced in the posterosuperior region of the external auditory canal and the outer attic wall to expose the ossicles. Fig. 2 The tumor could then be easily dissected around the ossicles, thus preserving the hearing. Thereafter, the drilling was performed judiciously in the posteroinferior part as the facial nerve runs lateral to the tympanic annulus in this region. The hypotympanic air cells were then exposed, and the tumor was delineated all around. Once the tumor margins were clearly delineated, a bipolar cautery was used to control the feeding vessels. Fig. 3 This shrinks the primary lesion sufficiently and provides hemostasis. The devascularized lesion was, thereafter, dissected from the promontory by a sharp dissection. Fig. 4 . At times, the residual bleeding from the bony channels on the promontory could be effectively controlled by oxidized cellulose (Surgicel - Ethicon Inc., Somerville, NJ, USA). Fig. 5 . The surgical video of the procedure is enclosed ( video 1 ).
Fig. 2.

Edited showing the drilling in the posterosuperior region of the external auditory canal.
Fig. 3.
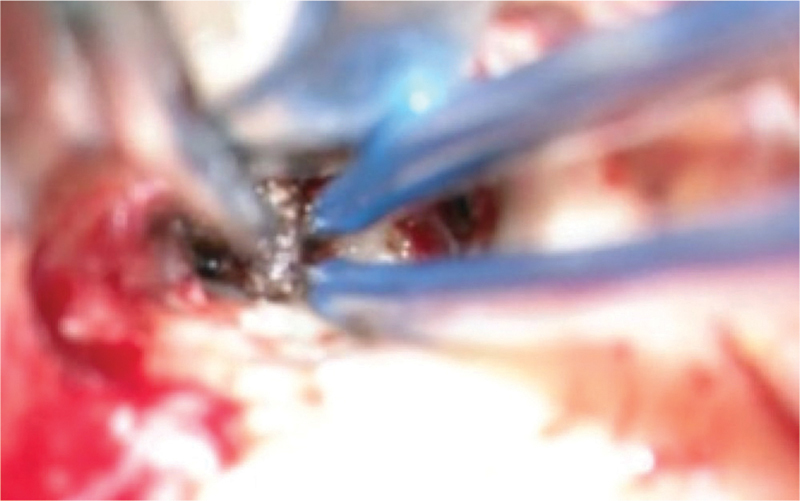
Edited showing the application of the bipolar diathermy for shrinking the tumor.
Fig. 4.

Edited showing the dissection of the lesion from the promontory. The incudostapedial joint and stapedius tendon are seen.
Fig. 5.
Edited showing the ossicular chain, stapedius tendon and round window niche after tumor removal.
If the tumor extended medial to the ossicles, the incus was dislocated from the stapes and removed to gain access. Tympanoplasty was performed, and the canal was packed with medicated gel film. The patients were alerted regarding the possibility of bleeding, hearing loss, facial nerve paralysis, taste disturbance, and tympanic membrane perforation. The follow-up protocol consisted of a computed tomography of the temporal bone with contrast at the end of 3 months to rule out any recurrence of the tumor. Those with persistent symptoms of tinnitus underwent computed tomography after 6 months
Results
A total number of 34 jugulotympanic paragangliomas were operated. Out of 34 patients, 8 were male and 26 were female. The modified technique was used in 29 patients. Only two cases were operated on with a classical transcanal approach. Canal wall down mastoidectomy was required in three cases. All the cases were successfully operated. Only 2 cases (2/29) had recurrence with return of tinnitus and conductive hearing loss. A computerized tomography scan confirmed the presence of tumor in the middle ear. Revision surgery in the two patients resulted in complete removal of the lesion. None of the patients required postoperative gamma knife therapy or radiotherapy.
Two patients had tympanic membrane perforation, for which they underwent repair of the tympanic membrane.
None of the patients had bleeding, facial paralysis, or taste disturbances.
All the patients had resolution of tinnitus after surgery. That is indicative of the completeness of tumor excision. A repeat computerized scan also confirmed the removal of the tumor. ( Fig. 6 a and b )
Fig. 6.

( a ) Edited computerized scan in axial plane showing the soft tissue opacity in the middle ear surrounding the ossicles. ( b ) edited post operative scan in axial plane showing the complete disappearance of the lesion
Hearing results: The hearing results are shown in Table 2 . There was a significant difference in the hearing thresholds after surgery. The postoperative improvement was around 19%.
Table 2. Showing the hearing thresholds before and after surgical excision. ( n = 29) .
| Hearing threshold | Preoperative | Postoperative | P -value |
|---|---|---|---|
| 49.52 ± 17.22 dB | 40.53 ± 17.34 dB | 0.001 * |
P -value is derived using the Wilcoxon test
statistical significance ( p < 0.05)
Discussion
It was Guild, in 1941, who described glomic tissue for vascularized tissue in the middle ear over the promontory and jugular bulb. 5 The glomus tympanicum tumors are typically located in the mesotympanum over the promontory, with propensity to expand into the mastoid and external auditory canal. The patients typically present with hearing loss and tinnitus. There can be otalgia, and vagal or hypoglossal palsy due to the mass effect on the surrounding structures. A complete excision is ensured by identifying the entire margin of tumor extension.
The management of jugulotympanic paragangliomas stand divided with the current standard of care. Surgical management of glomus tympanicum depends upon the stage of the tumor. Tumors strictly over the promontory are generally approached by the transcanal route. Recently, endoscopes have also been used for small tumors, with excellent results. 6 Endoscopic ear surgery has also revolutionized transcanal surgery for these lesions. Pollak et al. 6 described a removal of tympanic paraganglioma exclusively with endoscopes. Endoscopic ear surgery enhances visualization to ensure complete removal of smaller lesions. Mohammed et al. 7 also reported a case of endoscopic excision of tympanic paraganglioma. Endoscopic ear surgery, thus, could be a good tool for smaller lesions. Endoscopes enable the surgeon to have three-dimensional anatomy of the middle ear cleft. However, for larger lesions, a transcanal endoscopy may not be feasible for complete extirpation of the lesion.
A facial recess approach can still be used when the computerized tomography localizes it in the mesotympanum. Traditionally, the removal of type-II or type-III tumors is accomplished through the extended facial recess approach described by House and Glascock. 4 The extended facial recess is a time tested and safe approach for the management of tympanic paragangliomas. The approach preserves the posterior canal wall and is supposed to provide exposure through a facial recess approach. The advantages of this approach are clear demarcation of the entire course of vertical segment of the facial nerve prior to handling of the tumor, thus ensuring safety. Occasionally, one of the limitations of the facial recess approach could be the presence of continuous oozing at the time of surgery. This may prompt the surgeon to remove the canal wall or resort to canal wall mastoidectomy for tumor removal.
We have, therefore, modified our technique in glomus tympanicum class II and III, in which we use the postauricular transcanal posterior tympanectomy approach, the surgical steps of which have already been described. Our technique obviates the need to convert to a canal wall mastoidectomy in cases of imminent difficulty with the facial recess approach. This approach gives a head-on approach in addition to wide and adequate exposure to dissect tumor from the attic, mesotympanum, and hypotympanum.
The tumors extending into the hypotympanum are approached by extended hypotympanic access by drilling the anteroinferior canal wall. A wider access also ensures easy maneuverability of the bipolar cautery forceps used for dissection and making the tumor avascular. This results in complete excision of the tumor. ( Figs. 1 and 2 ). Some surgeons advocate the use of fiber-based laser system, which allows for accurate delivery of laser pulses to the tumor margins, thus being useful for tumor dissection. In our opinion, a microbipolar forceps is quite convenient to use.
The extension of glomus tympanicum to the hypotympanum is a difficult issue. The transcanal approach may have to be combined with endoscopic assisted visualization. Some of them may require mastoidectomy with retrofacial hypotympanotomy. Our technique also facilitates a hypotympanum approach, as described by Shambaugh 8 or Farrior. 9 The hypotympanic access is achieved by removing the inferior part of the posterior bony external auditory canal. 10 The surgeon must exercise caution here to avoid injury to the mastoid (vertical segment) of the facial nerve. Our technique (PT 2 ) is, therefore, unique in providing wide exposure of the mesotympanum, epitympanum, and hypotympanum for achieving complete excision of the tumor. This surgical procedure is safe and provides better anterior and inferior dissection of tumor without compromising the visualization of the tumor margins. Another advantage of our approach is a wider canal for adequate postoperative examination. The ossicular chain and tympanic membrane repair can also be done with satisfactory outcomes. These added advantages make this technique an ideal approach for removal of glomus tympanicum tumors. This technique of removal of jugulotympanic paragangliomas has not been reported earlier in the literature.
We came across only two cases who had recurrence in 2 years of follow-up. Both patients required revision surgery. None of the patients had any tympanic membrane perforation or cholesteatoma. No patient required gamma knife therapy.
Conclusions
A complete surgical removal is the treatment of choice in tympanic paragangliomas. The preoperative imaging allows for exact localization of the tumor and surgical planning. The modified technique of the postauricular transcanal posterior tympanectomy approach, nicknamed PT 2 , is ideally suited for types II and III glomus tympanicum tumors. This technique provides an adequate exposure for complete excision of jugulotympanic paragangliomas.
Funding Statement
Funding The author(s) received no financial support for the research.
Conflict of Interests The authors have no conflict of interests to declare.
Institute Ethics Committee Protocol No/Reference no NK/6313/study/636
References
- 1.Rossenwasser H. Carotid body tumor of the middle ear and mastoid. Arch Otolaryngol. 1945;41:64–67. [Google Scholar]
- 2.Oldring D, Fisch U. Glomus tumors of the temporal region: surgical therapy. Am J Otol. 1979;1(01):7–18. [PubMed] [Google Scholar]
- 3.Jackson C G, Glasscock M E, III, Harris P F. Glomus Tumors. Diagnosis, classification, and management of large lesions. Arch Otolaryngol. 1982;108(07):401–410. doi: 10.1001/archotol.1982.00790550005002. [DOI] [PubMed] [Google Scholar]
- 4.House W F, Glasscock M E., III Glomus tympanicum tumors. Arch Otolaryngol. 1968;87(05):550–554. doi: 10.1001/archotol.1968.00760060552023. [DOI] [PubMed] [Google Scholar]
- 5.Guild S R. A hitherto unrecognized structure- the Glomus jugularis. Man Anat. Rec. 1941;70:28. [Google Scholar]
- 6.Pollak N, Soni R S. Endoscopic excision of a tympanic paraganglioma: Training the next generation of ear surgeons. World J Otorhinolaryngol Head Neck Surg. 2017;3(03):160–162. doi: 10.1016/j.wjorl.2017.08.002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Mohammed A AS, Ahmed H S, Abdullah M AM, Badr-El-Dine M MK. Transcanal endoscopic excision of tympanic paraganglioma, a report of our surgical technique. The Egyptian J Neck Surgery Otorhinolaryngology. 2020;6(01):1–9. [Google Scholar]
- 8.Shambaugh G E., Jr Surgical approach for so-called glomus jugulare tumors of the middle ear. Laryngoscope. 1955;65(04):185–198. doi: 10.1288/00005537-195504000-00001. [DOI] [PubMed] [Google Scholar]
- 9.Farrior J B. Glomus tumors. Postauricular hypotympanotomy and hypotympanoplasty. Arch Otolaryngol. 1967;86(04):367–373. doi: 10.1001/archotol.1967.00760050369003. [DOI] [PubMed] [Google Scholar]
- 10.Jethanamest D. Tympanic paraganglioma. Resection techniques. Operation Techniques in Otolaryngology. 2016;27:15–19. [Google Scholar]