

CASE REPORT
A 28-year-old man from Equatorial Guinea presented with debilitating fatigue, persistent shortness of breath for the past year, and notable episodes of hematochezia and melena for the past week. Laboratory workup indicated the presence of iron deficiency anemia as the sole significant finding. Colonoscopy revealed a diffuse area of mildly erythematous mucosa in the rectal-sigmoid colon (Figure 1). Biopsy revealed colonic mucosa with calcified parasitic eggs (Figure 1), initially read by pathology as morphologically suggestive of Schistosoma mansoni eggs and later confirmed to be Schistosoma intercalatum by gene sequencing. The patient was treated with praziquantel, resulting in improved symptoms, cessation of bleeding, and stabilization of hemoglobin levels. The endoscopic appearance of lesions was variable, ranging from granulomas to polyps to ulcerations.1,2 In a case review of 46 patients with colonic schistosomiasis, as many as 12 patients were initially misdiagnosed as ulcerative colitis, Crohn's disease, and ischemic colitis.3,4 It is of utmost importance to maintain a low threshold for conducting endoscopic biopsies in patients who are at risk of parasitic infections, particularly those caused by the Schistosoma species.
Figure 1.
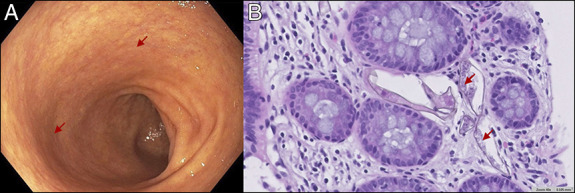
Diffuse area of mildly erythematous mucosa from 30 cm from the anal verge found in the rectal-sigmoid colon (A, arrows). Pathology showing multiple Schistosoma eggs (B, arrows).
DISCLOSURES
Author contributions: HE Lee: Made the most significant contribution to the case report in terms of drafting, data gathering, and revising the report. R. Abrol: Made significant contribution in revising and guiding the first author by gathering references and editing drafts. K. Humphrey and S. Qiu: Assisted with obtaining pathology, imaging, and explaining histologic findings. S. McLellan and SK Merwat: Helped with review of drafts and overall guidance. HE Lee is the article guarantor.
Financial disclosure: None to report.
Previous presentation: This case was presented at 13th Annual Quality and Research Forum at UTMB; April 2023; Galveston, TX.
Informed consent was obtained for this case report.
Contributor Information
Robinder Abrol, Email: rpabrol@utmb.edu.
Kyle Humphrey, Email: krhumphr@utmb.edu.
Suimin Qiu, Email: sqiu@utmb.edu.
Susan McLellan, Email: sumclell@utmb.edu.
Sheharyar K. Merwat, Email: skmerwat@utmb.edu.
REFERENCES
- 1.Bierman WF, Wetsteyn JC, van Gool T. Presentation and diagnosis of imported schistosomiasis: Relevance of eosinophilia, microscopy for ova, and serology. J Travel Med. 2005;12(1):9–13. [DOI] [PubMed] [Google Scholar]
- 2.Jusot JF, Simarro PP, De Muynck A. Schistosoma intercalatum bilharziasis: Clinical and epidemiological considerations. Med Trop (Mars). 1997;57(3):280–8. [PubMed] [Google Scholar]
- 3.Akere A, Oluwasola AO, Fakoya TO, Lawan A. Schistosomiasis presenting as colonic polypoid masses in a nigerian patient. Ann Ib Postgrad Med. 2017;15(1):61–4. [PMC free article] [PubMed] [Google Scholar]
- 4.Koulali H, Zazour A, Khannoussi W, Kharrasse G, Ismaili Z. Colonic schistosomiasis: A case report. World J Gastrointest Endosc. 2022;14(12):789–94. [DOI] [PMC free article] [PubMed] [Google Scholar]