

Introduction
Anomalous aortic origin of the coronary artery (AAOCA) is a rare congenital disease in which the coronary artery originates from a single opening or 2 independent openings of the same aortic sinus. It may be related to sudden cardiac death (SCD), and myocardial ischemia is considered the potential cause of SCD associated with AAOCA (1). Therefore, the early diagnosis and hemodynamic assessment of AAOCA are critical for reducing the risk of cardiac death. Presently, computed tomography angiography (CTA) and invasive coronary angiography (ICA) are commonly used to evaluate the anatomical morphology of AAOCA, but these are not useful for the hemodynamic detection of AAOCA (2). Fractional flow reserve derived from CTA (FFR-CT), a specific application in ischemia with coronary arteries, can noninvasively explore the hemodynamic changes in a patient with AAOCA and determine the relative benefit of therapeutic interventions (3,4).
Here, we report a patient with AAOCA who presented with postexercise syncope and acute myocardial infarction (AMI). We evaluated the hemodynamics of abnormal coronary artery detected using FFR-CT.
Case presentation
An 18-year-old male patient was sent to the emergency department due to sudden chest pain, progressive dyspnea, and dizziness while running. His lungs were covered with massive wet rales. The systolic blood pressure was 70 mmHg, and the heart rate was 110 bpm. The electrocardiogram revealed a sinus rhythm, a high and sharp T wave in leads V1–V6, an elevated ST-segment in lead augmented vector left (aVL) a depressed ST-segment in leads II and III, and augmented vector foot (aVF). Echocardiography revealed a segmental wall motion abnormality (especially in the inferior posterior wall) and an ejection fraction (EF) of 51%. Laboratory findings were as follows: creatinine kinase (CK), 8,444 U/L (38–174 U/L); creatinine kinase MB (CK-MB), 612 U/L (0–25 U/L); and cardiac troponin l (cTnI), 4.19 ng/mL (<0.04 ng/mL).
The patient had no previous history of the disease or a family history of cardiovascular disease or SCD. He had previously experienced difficulty in breathing after exercise.
A chest X-ray of the patient showed acute pulmonary edema. The left main coronary artery (LM) ran abnormally between the anterior wall of the aorta and the outflow tract of the right ventricle, causing severe compression of the LM. ICA showed up to 90% stenosis of the opening of the LM (Figure 1), while the left anterior descending artery (LAD), the left circumflex artery (LCX), and the right coronary artery (RCA) were normal. CTA with 3D volume-rendering reconstruction confirmed that the LM originated from the anterior wall of the aorta (between the right and the left sinus) (Figure 2).
Figure 1.

ICA examination. Severe stenosis was detected at the origin of the LM opening (arrows). ICA, invasive coronary angiography; LM, left main coronary artery.
Figure 2.

Axial view (A) and 3D volume-rendering image (B) of CTA showing the starting point and the course of the LM (arrow) relative to the AO and the PA. LM, left main coronary artery; LAD, left anterior descending artery; LA, left atrium; PA, pulmonary artery; AO, aorta; CTA, computed tomography angiography.
We used a deep learning based FFR-CT technique, which can accurately detect coronary artery ischemia (5). Since the reconstruction of LM showed severe stenosis and failed to match with the FFR-CT analysis, the imported image was not successful; thus, we measured the FFR values of the 3 branches. Taking the LAD, LCX and RCA within 2 cm of the opening as the measuring point, we found that the FFR of the LAD, LCX, and RCA was 0.75, 0.72, and 0.96, respectively (Figure 3).
Figure 3.
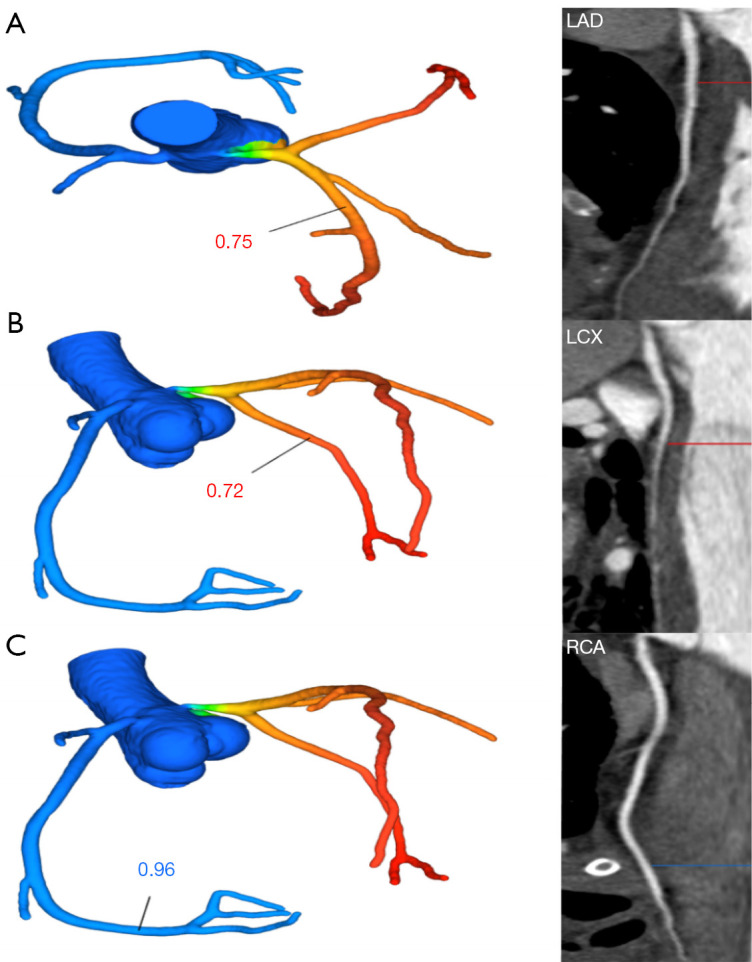
According to the CTA images, the FFR-CT values of the LAD and LCX caused by the stenosis of the LM were 0.75 and 0.72, respectively, and the FFR-CT value of the RCA was 0.96. LAD, left anterior descending artery; LCX, left circumflex artery; RCA, right coronary artery; CTA, computed tomography angiography; FFR-CT, fractional flow reserve derived from computed tomography angiography.
The patient’s condition continued to worsen after symptomatic treatment. The patient died of heart failure 1 week later.
All procedures performed in this study were conducted in accordance with the Declaration of Helsinki (as revised in 2013) and were approved by the Human Subjects Review Committee at Beijing Anzhen Hospital, Capital Medical University, Beijing, China (No. 2013007X). Written informed consent was obtained from the patient for publication of this case report and accompanying images. A copy of the written consent is available for review by the editorial office of this journal.
Discussion
AAOCA is a rare congenital cardiac condition. The varied clinical manifestations range from typical chest pain to syncope and cardiac arrest, which could cause malignant cardiovascular events. In this case, the patient eventually died of cardiac insufficiency due to myocardial ischemia, indicating the great value of hemodynamic detection with FFR-CT.
Although the gold standard for evaluating the hemodynamic significance of coronary artery is FFR (6), its invasiveness and high-cost limit is more widespread use in clinical practice. The DISCOVER-FLOW (Diagnosis of Ischemia-Causing Stenoses Obtained Via Noninvasive Fractional Flow Reserve), DeFACTO (Determination of Fractional Flow Reserve by Anatomic Computed Tomographic Angiography, and NXT (Analysis of Coronary Blood Flow Using CT Angiography: Next Steps) trials have confirmed that FFR-CT has good consistency with FFR in the detection of ischemic disease in the coronary artery (7-9). In patients with AAOCA, the indication of ischemia by FFR remains an important tool for guiding clinical decision-making. A study showed that conservative treatment may be justifiable in adult patients in the presence of normal FFR and nonsuspicious symptoms despite the presence of an inter-arterial course and/or slit-like orifice (10). Adjedj et al. retrospectively enrolled 54 patients with AAOCA, and they found that AAOCA was associated with a moderate hemodynamic decrease of FFR-CT values from 1.0 at the ostium to 0.90±0.10 downstream the ectopic course and 0.82±0.11 distally (11). We applied FFR-CT to the presently discussed patient with AAOCA to further confirm the hemodynamic manifestations of AAOCA with cardiac death in addition to morphology. In this case of AAOCA with cardiac death, the FFR-CT of the LAD and LCX was consistent with stenosis of the LM, with the FFR-CT being <0.8, which might have caused the corresponding ischemic symptoms.
Patients presenting with symptoms such as myocardial ischemia need surgical treatment as soon as possible. Surgical repair is usually safe, but adverse events such as restenosis may occur, and long-term monitoring is essential (12,13). Furthermore, FFR-CT may potentially serve as a noninvasive detection method in those patients with severe cardiac insufficiency.
Conclusions
FFR-CT is an essential tool for evaluating the hemodynamics of patients with AAOCA. It can reduce the incidence of SCD and guide clinical decision-making and prognosis evaluation in these patients. Moreover, young patients with coronary heart disease-like symptoms should be suspected of AAOCA, and intervention should be provided as early as possible to avoid the risk of SCD.
Supplementary
The article’s supplementary files as
Acknowledgments
Funding: This study was supported by grants from the National Natural Science Foundation of China (No. U1908211) and the Capital’s Funds for Health Improvement and Research Foundation of China (No. 2020-1-1052).
Ethical Statement: The authors are accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. All procedures performed in this study were in accordance with the Declaration of Helsinki (as revised in 2013) and were approved by the Human Subjects Review Committee at Beijing Anzhen Hospital, Capital Medical University, Beijing, China (No. 2013007X). Written informed consent was obtained from the patient for publication of this case report and accompanying images. A copy of the written consent is available for review by the editorial office of this journal.
Footnotes
Conflicts of Interest: All authors have completed the ICMJE uniform disclosure form (available at https://qims.amegroups.com/article/view/10.21037/qims-22-1447/coif). LX reports that this study was supported by grants from the National Natural Science Foundation of China (No. U1908211) and the Capital’s Funds for Health Improvement and Research Foundation of China (No. 2020-1-1052). ZS serves as an unpaid associate editor of Quantitative Imaging in Medicine and Surgery. The other authors have no conflicts of interest to declare.
References
- 1.Taylor AJ, Rogan KM, Virmani R. Sudden cardiac death associated with isolated congenital coronary artery anomalies. J Am Coll Cardiol 1992;20:640-7. 10.1016/0735-1097(92)90019-J [DOI] [PubMed] [Google Scholar]
- 2.Meijboom WB, Van Mieghem CA, van Pelt N, Weustink A, Pugliese F, Mollet NR, Boersma E, Regar E, van Geuns RJ, de Jaegere PJ, Serruys PW, Krestin GP, de Feyter PJ. Comprehensive assessment of coronary artery stenoses: computed tomography coronary angiography versus conventional coronary angiography and correlation with fractional flow reserve in patients with stable angina. J Am Coll Cardiol 2008;52:636-43. 10.1016/j.jacc.2008.05.024 [DOI] [PubMed] [Google Scholar]
- 3.Taylor CA, Fonte TA, Min JK. Computational fluid dynamics applied to cardiac computed tomography for noninvasive quantification of fractional flow reserve: scientific basis. J Am Coll Cardiol 2013;61:2233-41. 10.1016/j.jacc.2012.11.083 [DOI] [PubMed] [Google Scholar]
- 4.Tang CX, Lu MJ, Schoepf JU, Tesche C, Bauer M, Nance J, Griffith P, Lu GM, Zhang LJ. Coronary Computed Tomography Angiography-Derived Fractional Flow Reserve in Patients with Anomalous Origin of the Right Coronary Artery from the Left Coronary Sinus. Korean J Radiol 2020;21:192-202. 10.3348/kjr.2019.0230 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Wang ZQ, Zhou YJ, Zhao YX, Shi DM, Liu YY, Liu W, Liu XL, Li YP. Diagnostic accuracy of a deep learning approach to calculate FFR from coronary CT angiography. J Geriatr Cardiol 2019;16:42-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Pijls NH, De Bruyne B, Peels K, Van Der Voort PH, Bonnier HJ, Bartunek J, Koolen JJ, Koolen JJ. Measurement of fractional flow reserve to assess the functional severity of coronary-artery stenoses. N Engl J Med 1996;334:1703-8. 10.1056/NEJM199606273342604 [DOI] [PubMed] [Google Scholar]
- 7.Koo BK, Erglis A, Doh JH, Daniels DV, Jegere S, Kim HS, Dunning A, DeFrance T, Lansky A, Leipsic J, Min JK. Diagnosis of ischemia-causing coronary stenoses by noninvasive fractional flow reserve computed from coronary computed tomographic angiograms. Results from the prospective multicenter DISCOVER-FLOW (Diagnosis of Ischemia-Causing Stenoses Obtained Via Noninvasive Fractional Flow Reserve) study. J Am Coll Cardiol 2011;58:1989-97. 10.1016/j.jacc.2011.06.066 [DOI] [PubMed] [Google Scholar]
- 8.Nakazato R, Park HB, Berman DS, Gransar H, Koo BK, Erglis A, Lin FY, Dunning AM, Budoff MJ, Malpeso J, Leipsic J, Min JK. Noninvasive fractional flow reserve derived from computed tomography angiography for coronary lesions of intermediate stenosis severity: results from the DeFACTO study. Circ Cardiovasc Imaging 2013;6:881-9. 10.1161/CIRCIMAGING.113.000297 [DOI] [PubMed] [Google Scholar]
- 9.Nørgaard BL, Leipsic J, Gaur S, Seneviratne S, Ko BS, Ito H, et al. Diagnostic performance of noninvasive fractional flow reserve derived from coronary computed tomography angiography in suspected coronary artery disease: the NXT trial (Analysis of Coronary Blood Flow Using CT Angiography: Next Steps). J Am Coll Cardiol 2014;63:1145-55. 10.1016/j.jacc.2013.11.043 [DOI] [PubMed] [Google Scholar]
- 10.Driesen BW, Warmerdam EG, Sieswerda GT, Schoof PH, Meijboom FJ, Haas F, Stella PR, Kraaijeveld AO, Evens FCM, Doevendans PAFM, Krings GJ, van Dijk APJ, Voskuil M. Anomalous coronary artery originating from the opposite sinus of Valsalva (ACAOS), fractional flow reserve- and intravascular ultrasound-guided management in adult patients. Catheter Cardiovasc Interv 2018;92:68-75. 10.1002/ccd.27578 [DOI] [PubMed] [Google Scholar]
- 11.Adjedj J, Hyafil F, Halna du Fretay X, Dupouy P, Juliard JM, Ou P, Laissy JP, Muller O, Wijns W, Aubry P; . Physiological Evaluation of Anomalous Aortic Origin of a Coronary Artery Using Computed Tomography-Derived Fractional Flow Reserve. J Am Heart Assoc 2021;10:e018593. 10.1161/JAHA.120.018593 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Nees SN, Flyer JN, Chelliah A, Dayton JD, Touchette L, Kalfa D, Chai PJ, Bacha EA, Anderson BR. Patients with anomalous aortic origin of the coronary artery remain at risk after surgical repair. J Thorac Cardiovasc Surg 2018;155:2554-2564.e3. 10.1016/j.jtcvs.2017.12.134 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Brothers JA, Frommelt MA, Jaquiss RDB, Myerburg RJ, Fraser CD, Jr, Tweddell JS. Expert consensus guidelines: Anomalous aortic origin of a coronary artery. J Thorac Cardiovasc Surg 2017;153:1440-57. 10.1016/j.jtcvs.2016.06.066 [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
The article’s supplementary files as