

Abstract
Introduction: Complete healing of a gingivectomy wound usually takes between one and two months. To speed up this process, different topical medications have been reported. In addition, there are different studies assessing the efficacy of low-level laser therapy (LLLT) in terms of wound healing and pain relief subsequent to gingivectomy, yielding inconsistent outcomes. In the present study, we systematically reviewed the existing evidence in the literature to resolve the given conflicts.
Methods: We searched for the studies published from inception to 1 April 2023 in Embase, PubMed, and Scopus databases without language limitation by the use of appropriate keywords. We included randomized or non-randomized clinical trial studies that appraised the efficacy of LLLT in pain reduction and wound healing in adult patients who underwent gingivectomy. We pooled the continuous data concerning the pain visual analogue scale and the healing index extracted from the individual studies to provide a standardized mean difference (SMD) with a 95% confidence interval (CI), using a random-effects model.
Results: Out of 188 sources initially captured from the database search, six studies were ultimately included. Regarding wound healing, the LLLT group exhibited a significantly higher mean value of the healing index compared to the control group on days 3 (SMD, 0.93; 95% CI, 0.39 to 1.47) and 7 (SMD, 1.03; 95% CI, 0.49 to 1.57) post-surgery. Also, significant differences were noted in the postoperative pain reduction between the two groups on days 3 (SMD, -2.00; 95% CI, -2.48 to -1.51) and 7 (SMD, -2.44; 95% CI, -4.66 to -0.22) post-surgery.
Conclusion: According to the present systematic review, LLLT could potentially be an efficient adjunctive treatment after gingivectomy for wound healing acceleration and patient pain alleviation.
Keywords: Low-level laser therapy, Gingivectomy, Pain management, Wound healing, Systematic review
Introduction
Gingivectomy refers to a common surgical procedure in which the gum tissue (gingiva) is removed. The potential indications for gingivectomy mainly include the elimination of gingival enlargements, suprabony pockets, and gingival enlargements.1,2 Complete healing of a gingivectomy wound usually takes 4-6 weeks.3,4 To speed up this process, different topical medicaments, antibiotics, or amino acids have been mentioned5,6; also, low-level laser therapy (LLLT) has recently been proposed as another option for this aim.1,5
During the last decades, medical and dental professionals have utilized lasers as an adjunct to conventional therapies.7,8 The mechanism of LLLT is mainly based on photobiomodulation or biostimulation, leading to irritating cellular metabolism and proliferation.9,10 Over recent years, LLLT has been shown effective in the postoperative pain relief and wound healing process in dental practice, such as periodontology11,12; however, LLLT has not been widely used in dental practice because of insufficient clinical trial data.
There are different studies assessing the effect of LLLT on wound healing and pain reduction following gingivectomy with various findings1,3,13; no comprehensive study has yet been done to provide responsive results. Therefore, in the current study, we aimed to carry out a systematic review and meta-analysis of the existing data on the clinical effectiveness of LLLT in patients who underwent gingivectomy. Our findings would help clinicians better manage the patients undergoing gingivectomy by utilizing LLLT.
Methods
Information Sources and Search Strategy
The current study was presented in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) guideline.14 We searched for the literature published from inception to 1 April 2023 in the databases of Embase, PubMed, and Scopus, without language restrictions, using the following keywords: gingiva OR gingivectomy OR gingivoplasty AND laser therapy OR low-level laser therapy OR low-level light therapy OR LLLT. The search was limited to the Title/Abstract. We also scrutinized the reference lists of the retrieved eligible articles by hand searching to capture other sources.
Inclusion and Exclusion Criteria
We included randomized or non-randomized clinical trial studies that examined the efficacy of LLLT in reducing pain and promoting wound healing in patients who underwent gingivectomy. We defined the following selection criteria according to the PICO model:
Population: Adult subjects (aged ≥ 18 years old) undergoing gingivectomy
Intervention: LLLT (without limitations in any irradiation parameters)
Comparison: Placebo or active comparator
Outcomes: Wound healing and/or Pain reduction
Review articles, case reports, editorials, and letters to the editors were not eligible for the present study. Duplicate publications were excluded. We also excluded surveys with unextractable data on the study outcome. Finally, we considered the studies without available full text ineligible for inclusion.
Study Selection and Data Extraction
We transferred the records primarily obtained from the electronic database search to the reference management software (EndNote Xx8.1, Thomson Reuters, Stamford, Connecticut, USA). Duplicate results were then excluded. In the next step, we independently screened the titles and abstracts of the remaining papers for eligibility by means of the pre-designed suitability form. Next, we appraised the relevant reports in a full-text format. Any discrepancies were resolved by consensus. We finally extracted the following information from the eligible studies onto a Microsoft Excel spreadsheet (Microsoft Corporation): first author’s name, publication year, study location (country), study design, irradiation parameters (type, wavelength, power, energy, mode), number of subjects, study outcomes. We recorded the continuous data (mean and standard deviation) on postoperative pain measured by the visual analogue scale (VAS) and wound healing measured by the healing index (HI) for both LLLT and control groups, where available. We used Google Translate for translating the non-English reports, where necessary.
Risk of Bias Assessment
We appraised the quality of the enrolled surveys by the use of the revised Cochrane risk-of-bias tool for randomized trials (RoB 2),15 and the results were plotted by the robvistool(https://mcguinlu.shinyapps.io/robvis/). The RoB 2 tool evaluates the likelihood of a bias in a study across five different domains. These domains include the process of randomization, the deviations from the intended interventions, the missing data related to the outcome, the method used to measure the outcome, and the selection of the reported result. There are three levels of quality for each domain: ‘low risk’, ‘some concerns’, and ‘high risk’.
Statistical Analysis
We pooled the continuous data concerning the VAS and HI extracted from the individual studies to provide the standardized mean difference (SMD) with a 95% confidence interval (CI), using a random-effects model. The analysis was performed on the data obtained on the third and seventh days after the gingivectomy. The I-squared statistic test was used to explore the heterogeneity between the surveys, which can range from 0% to 100%, with significant values considered at P < 0.10. Forest plots were generated to show the summary results. STATA software (StataCorp, College Station, TX, USA) was utilized to conduct all statistical analyses.
Results
Search Results and Study Selection
A total of 188 citations were initially yielded from the databases searched; 176 articles were excluded due to duplication or unsuitability. Out of the remaining 14 papers, eight were excluded at the full-text screening stage. After conducting a rigorous screening process, a total of six eligible studies were included in this review1,3,4,13,16,17 The flow of the search strategy and result information is illustrated as per the PRISMA diagram in Figure 1.
Figure 1.
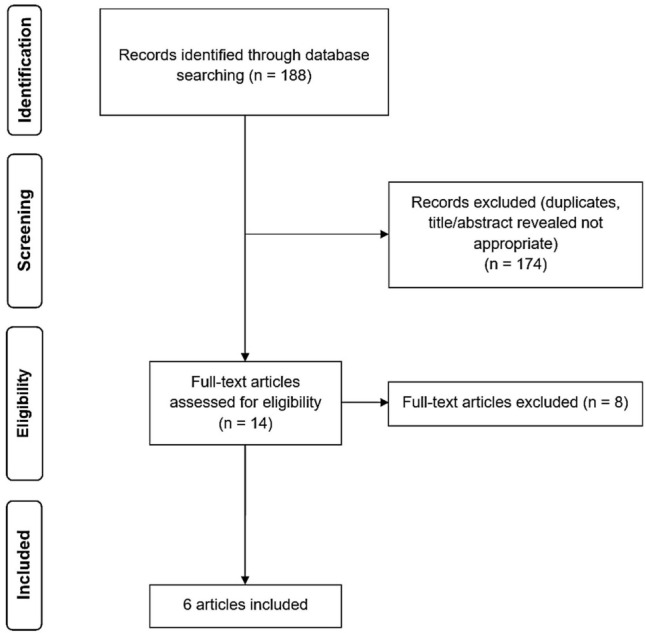
PRISMA Flow Diagram
Study Characteristics
Out of six eligible studies included in this review, five were randomized clinical trials (RCTs), and one was a non-RCT. In addition, there were three studies from India, one from Brazil, one from Saudi Arabia, and one from Turkey. All articles were written in English. They got published between 2006 and 2020. Table 1 summarizes the basic information of the articles included in this systematic review. The results of the quality assessment were reported for all of the included studies in Figure 2.
Table 1. Baseline Information of the Studies Included in the Systematic Review .
| Study | Country | Study Design | Number of Subjects | Intervention and Comparator | Irradiation Parameters | Outcomes |
| Amorim et al, 200616 | Brazil | Non-RCT | 20 patients with periodontal disease | One side of the operated area received LLLT, while the other did not. | Type: Diode laser; Wavelength: 685 nm; Power: 50 mW; Energy: 4 J/cm2; Mode: Continuous | The biometrical evaluation demonstrated a significant improvement in wound healing for the laser group at 21 and 28 days postoperatively. Clinical evaluation showed better repair for the laser group, mainly after the third day of the gingivectomy. |
| Kohale et al, 20181 | India | RCT | 40 patients with gingival enlargement in the maxillary and mandibular anterior region | One side of the operated area received LLLT, while the other did not. | Type: Diode laser; Wavelength: 940 nm; Power: 100 mW; Energy: 4 J/cm2; Mode: Continuous | LLLT-applied sites showed significantly lower stained areas (indicating improved healing) in comparison with the controls on the 7th and 30th days of the gingivectomy. |
| Lingamaneni et al, 20193 | India | RCT | 10 patients with inflammatory gingival enlargement | One side of the operated area received LLLT, while the other did not. | Type: Diode laser; Wavelength: 810 nm; Power: NA; Energy: NA; Mode: Continuous | No statistically significant difference was observed between the two groups in the surface epithelialization on the third and seventh postoperative days. However, highly significant differences were observed on the 14th day of the gingivectomy. |
| Madi and Mahmoud, 202013 | Saudi Arabia | RCT | 20 patients with inflammatory gingival enlargement | 10 patients received postoperative LLLT, and 10 patients did not. | Type: Diode laser; Wavelength: 660 nm; Power: 50 mW; Energy: 4 J/cm2; Mode: Continuous | The laser-treated group showed significant improvement in the healing score at days 5, 7, and 14 after the gingivectomy, and in the visual analogue scale score at days 3, 5, and 7 after the surgery, versus the control group. |
| Ozcelik et al, 200817 | Turkey | RCT | 20 patients with inflammatory gingival hyperplasias | One side of the operated area received LLLT, while the other did not. | Type: Diode laser; Wavelength: 588 nm; Power: 120 mW; Energy: 4 J/cm2; Mode: Continuous | LLLT-applied sites had significantly lower stained areas (indicating improved healing) than the controls on the third, seventh, and 15th days of the surgery. |
| Reddy et al, 20194 | India | RCT | 30 Patients with suprabony pockets and gingival enlargement | 10 patients received LLLT, 10 patients received hyaluronic acid, and 10 patients received herbal gel | Type: Diode laser; Wavelength: 940 nm; Power: 50 mW; Energy: 4 J/cm2; Mode: Continuous | The plaque index, gingival index, and gingival enlargement index (GEI) showed good improvement postoperatively within the groups, which was statistically significant. However, the GEI pertaining only to the laser group showed significant changes in an intergroup comparison. Moreover, the pain perception analyzed by the visual analogue score was the least, and histologically, the amount of mature collagen fibers laid down was higher in the laser group. |
RCT, randomized clinical trial; LLLT, low-level laser therapy
Figure 2.

Risk of Bias Assessment for the Individual Domains (A) and Studies (B)
Main Findings
In the study by Amorim et al,16 20 patients with bilateral involvement of premolar teeth in both the maxillary and mandibular regions were included. Following a gingivectomy procedure, one side of the mouth was subjected to LLLT intervention, while the other side did not receive any treatment (control). According to the biometrical assessment, the intervention group showed substantial improvements in wound healing within both 21 and 28 days after the surgery. Furthermore, the laser group showed better repair based on the clinical evaluation, mainly after the third day.
Madi and Mahmoud13 randomly allocated 20 patients with inflammatory gingival enlargement who underwent gingivectomy to two groups (ten patients received postoperative LLLT and ten did not). Follow-up investigation on the 5th, 7th, and 14th days of the surgery demonstrated that the healing score was significantly improved in the laser group in comparison to the control group. In addition, the intervention group exhibited a significant improvement in the VAS score than the control group on days 3, 5, and 7 of the surgery.
The study by Ozcelik et al17 was carried out on 20 cases who underwent gingivectomy and gingivoplasty. After the operations, one side of the surgery randomly received the laser, and the other side did not. The authors examined the surface area of the stained gingiva by utilizing image-analyzing software. According to the results, LLLT resulted in significantly reduced stained areas in the treated sites versus the controls at 3, 7, and 15 days post-surgery.
In the study by Reddy et al,4 30 patients indicated for gingivectomy were equally divided into three groups receiving LLLT, hyaluronic acid, or herbal gel after the surgery. The findings demonstrated that the laser group had superior clinical and histological results compared to the other two groups at six weeks of the surgery.
Kolahe et al1 studied 40 patients with gingival enlargement. One side of the surgical site was randomly subjected to LLLT (intervention); in contrast, the other side did not receive the laser (control). The assessment of the stained areas showed a statistically significant decrease in the stained area in the sites that received the laser versus the controls at 7 and 30 days after the surgery.
Finally, in the study by Lingamaneni et al,3 which was performed on ten patients, one side of the operated area received LLLT, while the other did not. The soft tissue healing was examined by a healing index immediately after the surgery and on the third day, one week, and two weeks postoperatively. No significant difference was identified in the surface epithelialization between the two groups at 3 and 7 days after the gingivectomy, but significant differences were seen at 14 days of the surgery.
Meta-Analysis
Regarding wound healing, two studies compared HI data between LLLT and control groups.1,3 The results indicated a significantly higher mean value of HI in the LLLT group than in the control group on days 3 (SMD, 0.93; 95% CI, 0.39 to 1.47; I-squared = 0.0%, P = 0.322) and 7 (SMD, 1.03; 95% CI, 0.49 to 1.57; I-squared = 0.0%, P = 0.463) post-surgery (Figure 3).
Figure 3.

Forest Plots of Wound Healing (Healing Index) Between Low-Level Laser Therapy and Control Groups on Days 3 and 7 Post-surgery
There were two studies that compared postoperative pain intensities between LLLT and control groups by using the VAS.1,13 According to the analyses, significant differences were observed between the two groups on days 3 (SMD, -2.00; 95% CI, -2.48 to -1.51; I-squared = 0.0%, P = 0.478) and 7 (SMD, -2.44; 95% CI, -4.66 to -0.22; I-squared = 94.9%, P < 0.001) post-surgery (Figure 4).
Figure 4.

Forest Plots of Pain Reduction (Visual Analogue Scale) Between Low-Level Laser Therapy and Control Groups on Days 3 and 7 Post-surgery
Discussion
The healing process of a gingivectomy wound is a slow phenomenon taken by secondary intention, taking between one and two months for complete epithelialization and connective tissue maturation.18,19 In addition to conventional treatments, LLLT has been reported as adjunctive therapy to accelerate this process and improve patient satisfaction. So far, a number of clinical studies have endeavored to quantify the efficiency of LLLT in promoting wound healing and pain relief in patients who underwent gingivectomy, and they have reported contradictory results.4,16,17 In the present study, we systematically reviewed the available evidence on this topic in different scientific databases to resolve the given conflicts.
After screening many articles, we finally included six eligible clinical trials. According to the meta-analysis results, LLLT efficiently reduced postoperative pain and improved wound healing on days 3 and 7 of the surgery. Lingamaneni et al3 also reported that the healing signs were significantly observed on the 14th day of gingivectomy in operated areas receiving LLLT versus those not. Reddy et al4 also stated that LLLT was associated with better clinical and histological outcomes than hyaluronic acid and herbal gel.
Zhao et al11 conducted a meta-analysis to investigate the impact of LLLT on decreasing the pain and healing the wound after periodontal surgery. The authors reported that LLLT was beneficial in reducing pain on day 3 (but not day 7) after the surgery. They also found that LLLT could accelerate the re-epithelialization and wound healing on day 14 (but not day 21) postoperatively. Contrary to Zhao and colleagues’ review, we focused on gingivectomy. Also, we included more studies than that review and conducted a meta-analysis on postoperative pain reduction and wound healing following gingivectomy.
There are also meta-analyses exploring the potential impacts of LLLT on the clinical outcomes of the patients who underwent other oro-dental surgeries. Domah et al20 reported that the use of LLLT effectively decreases the swelling following the mandibular third molar extraction compared to a placebo. On the other hand, it has not been observed to have a significant impact on reducing postoperative pain and trismus. Seyyedi et al21 reported in their review article that LLLT has the potential to be a beneficial instrument in oral surgeries due to its ability to speed up the healing of wounds and alleviate pain during the operation, which is consistent with our results. Finally, Ebrahimi et al22 reported that LLLT could be a useful technique in enhancing the healing process of secondary intention wounds.
The trials included in the present review study utilized diode lasers with wavelengths of 588 nm, 660 nm, 685 nm, 810 nm, and 940 nm and power of 50 mW, 100 mW, and 120 mW to conduct LLLT following gingivectomy. These variations might cause differences in the findings seen in the included studies. In general, the efficacy of LLLT can be influenced by various laser parameters such as fluency, irradiation, and beam profile.23 When administering LLLT, it is important to consider the biphasic response, which outlines the ideal light dose-response. This response curve includes three phases based on the laser doses. The first phase is characterized by an inadequate amount of energy, which fails to meet the minimum threshold required for a response. The second phase, on the other hand, involves the application of an adequate amount of energy, which surpasses the threshold, resulting in biostimulation. Finally, the third phase highlights that if an excessive amount of energy is applied, bioinhibition will occur instead of stimulation. Generally, LLLT is performed in a 400-980 nm wavelength and 1-500 mW power by using different types of light sources, such as gallium arsenide, ruby, helium-neon, and diode.1,24
Wound healing promotion by LLLT can be done by different mechanisms, which include25-28:
Increase in the reactive oxygen species, affecting the intercellular homeostasis of the cells proliferation
Influencing the microcirculation and altering capillary hydrostatic pressure, leading to a decrease in the edema
Increasing the human keratinocytes motility and accelerating the epithelialization process
Enhancing the proliferation of the fibroblast and synthesis of the matrix
Increasing neovascularization
A limitation of the present systematic review and meta-analysis was the various irradiation parameters and different scales for patients’ outcomes used in the individual studies, potentially leading to differences in the information and restricting us from pooling more data and providing more substantial evidence on postoperative pain reduction and wound healing. Therefore, it is suggested to carry out more homogenous randomized placebo-controlled clinical trials in the future.
Conclusion
According to the present systematic review, LLLT could potentially be an efficient adjunctive treatment after gingivectomy to promote wound healing and reduce patient discomfort. However, further studies with larger sample sizes and placebo/active comparators must be done to provide more robust evidence.
Authors’ Contribution
Conceptualization: Farida Abesi, Nahid Derikvand.
Data curation: Farida Abesi, Nahid Derikvand.
Investigation: Farida Abesi, Nahid Derikvand.
Formal analysis: Farida Abesi.
Methodology: Farida Abesi.
Project administration: Farida Abesi.
Resources: Farida Abesi.
Supervision: Farida Abesi.
Validation: Farida Abesi, Nahid Derikvand.
Visualization: Farida Abesi, Nahid Derikvand.
Writing–original draft: Farida Abesi, Nahid Derikvand.
Writing–review & editing: Farida Abesi, Nahid Derikvand.
Competing Interests
The authors declare that they have no conflict of interest.
Ethical Approval
Not applicable.
Please cite this article as follows: Abesi F, Derikvand N. Efficacy of low-level laser therapy in wound healing and pain reduction after gingivectomy: a systematic review and meta-analysis. J Lasers Med Sci. 2023;14:e17. doi:10.34172/jlms.2023.17.
References
- 1.Kohale BR, Agrawal AA, Raut CP. Effect of low-level laser therapy on wound healing and patients’ response after scalpel gingivectomy: a randomized clinical split-mouth study. J Indian Soc Periodontol. 2018;22(5):419–26. doi: 10.4103/jisp.jisp_239_18. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2. Jepsen K, Sculean A, Jepsen S. Complications and treatment errors involving periodontal tissues related to orthodontic therapy. Periodontol 2000. 2023. 10.1111/prd.12484. [DOI] [PubMed]
- 3.Lingamaneni S, Mandadi LR, Pathakota KR. Assessment of healing following low-level laser irradiation after gingivectomy operations using a novel soft tissue healing index: a randomized, double-blind, split-mouth clinical pilot study. J Indian Soc Periodontol. 2019;23(1):53–7. doi: 10.4103/jisp.jisp_226_18. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Reddy SP, Koduganti RR, Panthula VR, Surya Prasanna J, Gireddy H, Dasari R, et al. Efficacy of low-level laser therapy, hyaluronic acid gel, and herbal gel as adjunctive tools in gingivectomy wound healing: a randomized comparative clinical and histological study. Cureus. 2019;11(12):e6438. doi: 10.7759/cureus.6438. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Lafzi A, Kadkhodazadeh M, Mojahedi SM, Amid R, Shidfar S, Baghani MT. The clinical evaluation of the effects of low-level laser therapy on the donor and recipient sites of the free gingival graft: a case series. J Lasers Med Sci. 2019;10(4):355–60. doi: 10.15171/jlms.2019.58. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6. Amaliya A, Budhirahardjo I, Hendiani I. Histological examination of lemongrass resorbable dressing on gingival healing after gingivectomy in rats. Eur J Dent. 2022. 10.1055/s-0042-1748197. [DOI] [PMC free article] [PubMed]
- 7.Arjmand B, Khodadost M, Jahani Sherafat S, Rezaei Tavirani M, Ahmadi N, Hamzeloo Moghadam M, et al. Low-level laser therapy: potential and complications. J Lasers Med Sci. 2021;12:e42. doi: 10.34172/jlms.2021.42. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Luke AM, Mathew S, Altawash MM, Madan BM. Lasers: a review with their applications in oral medicine. J Lasers Med Sci. 2019;10(4):324–9. doi: 10.15171/jlms.2019.52. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Carneiro AMP, Barros APO, de Oliveira RP, de Paula BLF, Silva AM, de Melo Alencar C, et al. The effect of photobiomodulation using low-level laser therapy on tooth sensitivity after dental bleaching: a systematic review. Lasers Med Sci. 2022;37(7):2791–804. doi: 10.1007/s10103-022-03578-0. [DOI] [PubMed] [Google Scholar]
- 10.Dompe C, Moncrieff L, Matys J, Grzech-Leśniak K, Kocherova I, Bryja A, et al. Photobiomodulation-underlying mechanism and clinical applications. J Clin Med. 2020;9(6):1724. doi: 10.3390/jcm9061724. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Zhao H, Hu J, Zhao L. The effect of low-level laser therapy as an adjunct to periodontal surgery in the management of postoperative pain and wound healing: a systematic review and meta-analysis. Lasers Med Sci. 2021;36(1):175–87. doi: 10.1007/s10103-020-03072-5. [DOI] [PubMed] [Google Scholar]
- 12.Varma SR, AlShayeb M, Narayanan J, Abuhijleh E, Hadi A, Jaber M, et al. Applications of lasers in refractory periodontitis: a narrative review. J Int Soc Prev Community Dent. 2020;10(4):384–93. doi: 10.4103/jispcd.JISPCD_241_20. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Madi M, Mahmoud MM. The evaluation of healing effect of low-level laser treatment following gingivectomy. Beni Suef Univ J Basic Appl Sci. 2020;9(1):25. doi: 10.1186/s43088-020-00053-z. [DOI] [Google Scholar]
- 14.Moher D, Liberati A, Tetzlaff J, Altman DG. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLoS Med. 2009;6(7):e1000097. doi: 10.1371/journal.pmed.1000097. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Sterne JAC, Savović J, Page MJ, Elbers RG, Blencowe NS, Boutron I, et al. RoB 2: a revised tool for assessing risk of bias in randomised trials. BMJ. 2019;366:l4898. doi: 10.1136/bmj.l4898. [DOI] [PubMed] [Google Scholar]
- 16.Amorim JC, de Sousa GR, de Barros Silveira L, Prates RA, Pinotti M, Ribeiro MS. Clinical study of the gingiva healing after gingivectomy and low-level laser therapy. Photomed Laser Surg. 2006;24(5):588–94. doi: 10.1089/pho.2006.24.588. [DOI] [PubMed] [Google Scholar]
- 17.Ozcelik O, Cenk Haytac M, Kunin A, Seydaoglu G. Improved wound healing by low-level laser irradiation after gingivectomy operations: a controlled clinical pilot study. J Clin Periodontol. 2008;35(3):250–4. doi: 10.1111/j.1600-051X.2007.01194.x. [DOI] [PubMed] [Google Scholar]
- 18.Aoki A, Mizutani K, Schwarz F, Sculean A, Yukna RA, Takasaki AA, et al. Periodontal and peri-implant wound healing following laser therapy. Periodontol 2000. 2015;68(1):217–69. doi: 10.1111/prd.12080. [DOI] [PubMed] [Google Scholar]
- 19.Rosa DS, Aranha AC, Eduardo Cde P, Aoki A. Esthetic treatment of gingival melanin hyperpigmentation with Er:YAG laser: short-term clinical observations and patient follow-up. J Periodontol. 2007;78(10):2018–25. doi: 10.1902/jop.2007.070041. [DOI] [PubMed] [Google Scholar]
- 20. Domah F, Shah R, Nurmatov UB, Tagiyeva N. The use of low-level laser therapy to reduce postoperative morbidity after third molar surgery: a systematic review and meta-analysis. J Oral Maxillofac Surg 2021;79(2):313.e1-313.e19. 10.1016/j.joms.2020.09.018. [DOI] [PubMed]
- 21.Seyyedi SA, Taram S, Heydari M, Valizadeh R. Efficacy of low-level laser therapy in oral mucosal surgical wound healing: a systematic review and meta-analysis. Explor Med. 2022;3(5):451–60. doi: 10.37349/emed.2022.00106. [DOI] [Google Scholar]
- 22.Ebrahimi P, Hadilou M, Naserneysari F, Dolatabadi A, Tarzemany R, Vahed N, et al. Effect of photobiomodulation in secondary intention gingival wound healing-a systematic review and meta-analysis. BMC Oral Health. 2021;21(1):258. doi: 10.1186/s12903-021-01611-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Hosseinpour S, Tunér J, Fekrazad R. Photobiomodulation in oral surgery: a review. Photobiomodul Photomed Laser Surg. 2019;37(12):814–25. doi: 10.1089/photob.2019.4712. [DOI] [PubMed] [Google Scholar]
- 24.Dalirsani Z, Ghazi N, Delavarian Z, Pakfetrat A, Esmaily H, Davaji M, et al. Effects of diode low-level laser therapy on healing of tooth extraction sockets: a histopathological study in diabetic rats. Lasers Med Sci. 2021;36(7):1527–34. doi: 10.1007/s10103-021-03270-9. [DOI] [PubMed] [Google Scholar]
- 25.Migliario M, Sabbatini M, Mortellaro C, Renò F. Near infrared low-level laser therapy and cell proliferation: the emerging role of redox sensitive signal transduction pathways. J Biophotonics. 2018;11(11):e201800025. doi: 10.1002/jbio.201800025. [DOI] [PubMed] [Google Scholar]
- 26.Lins RD, Dantas EM, Lucena KC, Catão MH, Granville-Garcia AF, Carvalho Neto LG. Biostimulation effects of low-power laser in the repair process. An Bras Dermatol. 2010;85(6):849–55. doi: 10.1590/s0365-05962010000600011. [DOI] [PubMed] [Google Scholar]
- 27.Chawla K, Lamba AK, Tandon S, Faraz F, Gaba V. Effect of low-level laser therapy on wound healing after depigmentation procedure: a clinical study. J Indian Soc Periodontol. 2016;20(2):184–8. doi: 10.4103/0972-124x.176393. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Pansani TN, Basso FG, Turrioni AP, Soares DG, Hebling J, de Souza Costa CA. Effects of low-level laser therapy and epidermal growth factor on the activities of gingival fibroblasts obtained from young or elderly individuals. Lasers Med Sci. 2017;32(1):45–52. doi: 10.1007/s10103-016-2081-x. [DOI] [PubMed] [Google Scholar]