

Abstract
Purpose:
Compare occurrence of self-inflicted injuries among transgender and gender diverse (TGD) youth to that of their cisgender peers while accounting for mental health diagnoses.
Methods:
Review of electronic health records from three integrated health care systems identified 1087 transfeminine and 1431 transmasculine adolescents and young adults. Poisson regression was used to calculate prevalence ratios comparing the proportion of TGD participants with at least one self-inflicted injury (a surrogate for suicide attempt) before index date (first evidence of TGD status) to the corresponding proportions in presumed cisgender male and female referents matched on age, race/ethnicity and health plan. Interactions between gender identities and mental health diagnoses were assessed on multiplicative and additive scales.
Results:
In cisgender persons, self-inflicted injuries were concentrated among those with multiple mental health diagnoses. In contrast, the prevalence of self-inflicted injuries among TGD adolescents and young adults was high even in the absence of mental health diagnoses. Results were consistent with positive additive interaction and negative multiplicative interaction.
Conclusions:
Universal suicide prevention efforts for all youth, including those with no mental health diagnoses, and more intensive suicide prevention efforts for TGD adolescents and young adults and those with at least one mental health diagnosis are warranted.
Keywords: transgender, suicide, disparities
Introduction
Suicide is one of the top ten leading causes of death in the US, and the second leading cause of death among adolescents and young adults.1,2 It is also well documented that transgender and gender diverse (TGD) youth (i.e., those whose gender identity does not align with their assigned natal sex) experience especially high rates of suicide attempts and suicidal ideation, relative to cisgender youth.3–8 The high rates of suicidality in TGD youth are attributable to many factors. Some of those factors are identified in the broader population, including a range of mental health diagnoses such as mood disorders, substance use disorders, depression, and anxiety, among others.9–11 Yet, TGD people and especially TGD youth may also experience unique risk factors such as minority stress, internalized transphobia, gender-based victimization, a history of abuse, and lack of social support.6,12–15 These observations underscore the need to better understand the interplay of mental health conditions with TGD identities as they relate to suicidality.
Motivated by these considerations, the current study uses data from a large health system-based cohort to examine the association between TGD identities and self-inflicted injury, a surrogate for suicide attempts, while considering concurrent mental health diagnoses. The primary aim of the current analysis is to estimate the prevalence of self-inflicted injury among TGD and cisgender youth with and without common mental health diagnoses as well as across categories defined by the total number of mental health diagnoses. The secondary aim was to assess the statistical interaction between TGD identities and mental health diagnoses on both multiplicative and additive scales.
Methods
Data
Data for this analysis come from the Study of Transition, Outcomes, and Gender (STRONG) cohort. The cohort includes individuals from three participating Kaiser Permanente health systems in Georgia, Northern California, and Southern California. TGD individuals seeking care between January 1, 2006 and December 31, 2014 at these health systems were identified using a multistep approach. Briefly, an initial electronic health record (EHR) identification of TGD cohort candidates was conducted using relevant International Classification of Diseases Ninth Edition (ICD-9) codes (e.g., 302.6 – “gender identity disorder in children”) and an automated search of relevant keywords (e.g., “transgender”) in the free text clinical notes. Eligibility for inclusion was validated based on assessment of keyword-containing text excerpts, using two independent reviewers with disagreements adjudicated by expert review. Each TGD individual was then characterized as transfeminine (TF) or transmasculine (TM). Up to 10 cisgender male (CM) and 10 cisgender female (CF) referents were matched to each TGD person on age (based on 5-year groups for adults and 2-year groups for children and adolescents), race/ethnicity, site, and membership year at the index date, and the minimum number of cisgender referents was 7.16 Cisgender status was inferred by the absence of meeting the criteria for inclusion in the TGD cohort. Index date was defined based on the first evidence of TGD status and the same date was assigned as index date for the matched referents. A full description of cohort establishment has been published elsewhere.17 Data from several sources, including ICD-9 and ICD-10 codes for mental health diagnoses and other conditions, disease registries, health care utilization and pharmacy records, were integrated to create a comprehensive record of health and health care experiences in both TGD and matched cisgender cohorts. The cohort ascertainment and data collection were coordinated by Emory University, and all activities were reviewed and approved by the institutional review boards of the participating institutions with exemption of informed consent.
Measures
Self-inflicted injury, a surrogate for suicide attempts, any time before the index date was captured using two groups of ICD-9 and ICD-10 codes in EMRs for self-inflicted injury using a previously validated approach.18 Codes captured self-inflicted injuries and poisonings and possible self-inflicted injuries (Supplemental Table 1).19 Examining the time before index state is important (i.e., before evidence of TGD status is documented), as it represents a critical time period where suicide risk may be heightened among TGD persons.4 Further, after TGD status is documented in the health care setting, individuals may receive gender-affirming services (e.g., hormone therapy), which have been linked with suicidality outcomes,20 and it is beyond the scope of this study to examine the effects of said services.
Mental health diagnoses (anxiety disorder, attention deficit disorders, autism spectrum disorders, bipolar spectrum disorders, conduct/disruptive disorder, depressive disorders, personality disorders, substance abuse disorders) ever before index date were identified using ICD codes based on the Mental Health Research Network’s guidelines.21 Schizophrenia spectrum disorder, other psychoses, dementia, and eating disorders were categorized as “other diagnoses” due to sparse counts.
Statistical analysis
To focus on TGD adolescents and young adults, the present analysis was restricted to STRONG cohort participants from 13 to 26 years of age. The prevalence of mental health diagnoses and self-inflicted injury any time before index was determined for the TF and TM cohorts and the corresponding CM and CF reference groups. Prevalence ratios (PRs) compared the prevalence of self-inflicted injury before index date among TGD cohort members to reference male and female cohort members. PRs and 95% confidence intervals (CIs) were estimated using conditional Poisson regression and a robust variance estimator, accounting for the matched-cohort design, stratified by presence or absence of each individual mental health diagnosis and number of mental health diagnoses (0, 1–2, 3+). The presence of multiplicative interaction reflecting heterogeneity of PR estimates across strata was assessed using Wald chi-square tests for individual mental health diagnoses and a Wald test for joint interaction parameters for number of mental health diagnoses.
As interaction is scale-dependent, both additive and multiplicative interactionsa were assessed, as is considered best practice.22 Although measures of multiplicative interaction are most typically reported, measures of additive interaction incorporate background prevalence and are, thus, often considered to have more public health relevance in terms of identifying groups that may especially benefit from prevention measures.22 Both multiplicative and additive statistical interaction between TGD identities and mental health diagnoses were examined by comparing prevalence estimates in six groups of participants: 1) cisgender (CF or CM) with 0 mental health diagnoses (reference category), 2) cisgender with 1–2 diagnoses, 3) cisgender with 3+ diagnoses, 4) TGD (TM or TF) with 0 diagnoses, 5) TGD with 1–2 diagnoses and 6) TGD with 3+ diagnoses. This approach allowed comparing the observed PRs for self-inflicted injury to those expected in the absence of additive or multiplicative interaction between TGD identities and mental health diagnoses. Additive interaction was evaluated by calculating the relative excess risk due to interaction (RERI) a measure that quantifies departure from additivity using ratio estimates of association.23 Multiplicative interaction was evaluated by calculating the multiplicative interaction ratio (MIR), which quantifies departure from multiplicativity. Given the cross-sectional design of this study, the RERI and MIR are approximated using prevalence instead of risk. For TM and TF participants and the corresponding cisgender referents, we graphically depict the distributions of the total number of mental health diagnoses (0, 1–2, and 3+) and the percent of participants with documented selfinflicted injury within each group.
Two separate sensitivity analyses were conducted when examining associations between gender identity and number of mental health diagnoses with self-inflicted injury: (1) the outcome was restricted to self-inflicted injuries associated with an in-patient hospital visit (2) analyses were restricted to TGD participants without a recorded gender dysphoria diagnosis, as individuals with a gender dysphoria diagnosis are more likely to have received supportive services. P-values less than 0.05 were considered statistically significant. All analyses were conducted in SAS 9.4 and STATA 16.1.
Results
The final study population included 2,518 TGD youth, aged 13 to 26 years, matched with 24,544 CM and 24,617 CF referents (Table 1). Of the 2,518 TGD participants, 43% were TF (n = 1087) and 57% were TM (n = 1431). Most participants were 18 to 26 years old. Among TF youth, 46% were non-Hispanic white, 25% were Hispanic, and 9.5% were non-Hispanic Black. Among TM youth the proportions of non-Hispanic white, Hispanic, and non-Hispanic Black were 52%, 23% and 9.4%, respectively.
Table 1.
Demographic characteristics and prevalence of mental health diagnoses and self-inflicted injury among TGD and cisgender youth included in the STRONG cohort
| Participant Characteristics | TF cohort | CM referents | CF referents | TM cohort | CM referents | CF referents |
|---|---|---|---|---|---|---|
| n (%) | n (%) | n (%) | n (%) | n (%) | n (%) | |
|
| ||||||
| Age | ||||||
| 13–17 | 358 (33) | 3505 (33) | 3496 (33) | 595 (42) | 5822 (42) | 5836 (42) |
| 18–26 | 729 (67) | 7081 (67) | 7133 (67) | 836 (58) | 8136 (58) | 8152 (58) |
| Race/ethnicity | ||||||
| Non-Hispanic White | 502 (46) | 4866 (46) | 4903 (46) | 739 (52) | 7169 (51) | 7195 (51) |
| Non-Hispanic Black | 103 (9.5) | 998 (9.4) | 1008 (9.5) | 134 (9.4) | 1311 (9.4) | 1314 (9.4) |
| Hispanic | 273 (25) | 2673 (25) | 2679 (25) | 325 (23) | 3178 (23) | 3185 (23) |
| Other | 111 (10) | 1087 (10) | 1092 (10) | 129 (9.0) | 1272 (9.1) | 1275 (9.1) |
| Unknown | 98 (9.0) | 962 (9.1) | 947 (8.9) | 104 (7.3) | 1028 (7.4) | 1019 (7.3) |
| Kaiser Permanente site | ||||||
| Northern California | 600 (55) | 5857 (55) | 5878 (55) | 833 (58) | 8152 (58) | 8173 (58) |
| Southern California | 453 (42) | 4393 (41) | 4414 (42) | 559 (39) | 5422 (39) | 5430 (39) |
| Georgia | 34 (3.1) | 336 (3.2) | 337 (3.2) | 39 (2.7) | 384 (2.8) | 385 (2.8) |
| Self-inflicted injury | 81 (7.5) | 122 (1.2) | 198 (1.9) | 164 (11) | 175 (1.3) | 284 (2.0) |
| Mental health diagnoses | ||||||
| Anxiety disorders | 336 (31) | 1009 (9.5) | 1440 (14) | 447 (31) | 1335 (9.6) | 1920 (14) |
| Attention deficit disorders | 196 (18) | 1031 (9.7) | 473 (4.5) | 162 (11) | 1531 (11) | 590 (4.2) |
| Autism spectrum disorders | 53 (4.9) | 142 (1.3) | 30 (0.3) | 38 (2.7) | 203 (1.5) | 52 (0.4) |
| Bipolar spectrum disorders | 61 (5.6) | 139 (1.3) | 145 (1.4) | 90 (6.3) | 149 (1.1) | 190 (1.4) |
| Conduct/Disruptive disorder | 95 (8.7) | 421 (4.0) | 222 (2.1) | 79 (5.5) | 626 (4.5) | 291 (2.1) |
| Depressive disorders | 409 (38) | 1181 (11) | 1730 (16) | 631 (44) | 1525 (11) | 2229 (16) |
| Personality disorders | 33 (3) | 41 (0.4) | 84 (0.8) | 64 (4.5) | 61 (0.4) | 119 (0.9) |
| Substance abuse disorders | 115 (11) | 714 (6.7) | 497 (4.7) | 130 (9.1) | 905 (6.5) | 617 (4.4) |
| Other diagnosesa | 96 (8.8) | 141 (1.3) | 266 (2.5) | 126 (8.8) | 201 (1.4) | 358 (2.6) |
|
| ||||||
| Total numbers | 1087 | 10586 | 10629 | 1431 | 13958 | 13988 |
TM = transmasculine; TF= transfeminine; CF = cisgender female; CM = cisgender male
Other diagnoses includes schizophrenia spectrum disorder, other psychoses, dementia, and eating disorders.
Among TF cohort members, 7.5% (n = 81) had at least one identified episode of self-inflicted injury at any time before the index date. The corresponding percent among TM participants was 11% (n=164) and ≤2% among all cisgender referent groups. The three most prevalent mental health diagnoses among TGD youth were depressive disorders (38% for TF and 44% for TM), anxiety disorders (31% for both groups), and attention deficit disorders (18% for TF and 11% for TM). All mental health diagnoses were more common among TGD youth than CM and CF youth. Among those with a self-inflicted injury, 84% of TF members, 70% of their CM referents, and 73% of their CF had at least one mental health diagnosis (data not shown). Among those with a self-inflicted injury, 87% of TM members, 63% of their CM referents, and 71% of their CF referents had at least one mental health diagnosis (data not shown).
The PR for self-inflicted injury comparing TF youth to cisgender reference groups was consistently less pronounced among those who had a particular mental health diagnosis compared to those who did not have that mental health diagnosis (Table 2). The same pattern was observed in the analyses comparing TM participants to either cisgender cohort (Table 3). The heterogeneity of results was especially pronounced in all analyses comparing PR estimates among participants with and without bipolar spectrum disorders (Table 2–3). Other notable interactions were present in the analyses stratified by depressive disorders (TF vs. either reference group and TM vs. CF), conduct/disruptive disorder (TF vs. CF and TM vs. CF), and attention deficit disorder (TM vs. CF).
Table 2.
Associations between gender identity and self-inflicted injury stratified by presence of individual mental health diagnoses among TF and matched cisgender youth included in the STRONG cohort
| Mental health diagnoses | Transfeminine youth | Cisgender male referents | Cisgender female referents | TF cohort vs. CM referents | TF cohort vs. CF referents | |||
|---|---|---|---|---|---|---|---|---|
| # of events/total | % | # of events/total | % | # of events/total | % | PR (95% CI) | PR (95% CI) | |
|
| ||||||||
| Anxiety disordersc | ||||||||
| Yes | 44/336 | 13% | 36/1009 | 3.6% | 80/1440 | 5.6% | 3.4 (2.0, 5.7) | 2.1 (1.4, 3.2) |
| No | 37/751 | 4.9% | 86/9577 | 0.9% | 118/9189 | 1.3% | 5.7 (3.8, 8.4) | 3.9 (2.7, 5.7) |
| Attention deficit disorders | ||||||||
| Yes | 26/196 | 13% | 39/1031 | 3.8% | 27/473 | 5.7% | 4.0 (2.1, 7.5) | 2.2 (1.2, 4.0) |
| No | 55/891 | 6.2% | 83/9555 | 0.9% | 171/10156 | 1.7% | 7.0 (5.0, 9.9) | 3.8 (2.8, 5.2) |
| Autism spectrum disorders | ||||||||
| Yes | 5/53 | 9.4% | 3/142 | 2.1% | 3/30 | 10% | 3.8 (0.9, 15.4) | 0.9 (0.2, 4.1) |
| No | 76/1034 | 7.4% | 119/10444 | 1.1% | 195/10599 | 1.8% | 6.6 (5.0, 8.8) | 4.1 (3.1, 5.3) |
| Bipolar spectrum disordersb,c | ||||||||
| Yes | 13/61 | 21% | 15/139 | 11% | 32/145 | 22% | 1.4 (0.6, 3.5) | 0.7 (0.3, 2.0) |
| No | 68/1026 | 6.6% | 107/10447 | 1.0% | 166/10484 | 1.6% | 6.7 (5.0, 9.1) | 4.2 (3.2, 5.5) |
| Conduct/Disruptive disorderc | ||||||||
| Yes | 21/95 | 22% | 27/421 | 6.4% | 28/222 | 13% | 5.2 (2.1, 13.3) | 1.5 (0.7, 3.2) |
| No | 60/992 | 6.0% | 95/10165 | 0.9% | 170/10407 | 1.6% | 6.3 (4.6, 8.6) | 3.8 (2.9, 5.1) |
| Depressive disordersb,c | ||||||||
| Yes | 56/409 | 14% | 63/1181 | 5.3% | 128/1730 | 7.4% | 2.6 (1.7, 4.0) | 1.5 (1.0, 2.1) |
| No | 25/678 | 3.7% | 59/9405 | 0.6% | 70/8899 | 0.8% | 5.9 (3.7, 9.4) | 5.2 (3.3, 8.3) |
| Personality disordersc | ||||||||
| Yes | 12/33 | 36% | 5/41 | 12% | 24/84 | 29% | 2.5 (0.5, 12.3) | 0.9 (0.2, 3.1) |
| No | 69/1054 | 6.5% | 117/10545 | 1.1% | 174/10545 | 1.7% | 6.0 (4.5, 8.0) | 4.0 (3.0, 5.2) |
| Substance abuse disorders | ||||||||
| Yes | 31/115 | 27% | 41/714 | 5.7% | 54/497 | 11% | 4.7 (2.6, 8.6) | 2.5 (1.4, 4.4) |
| No | 50/972 | 5.1% | 81/9872 | 0.8% | 144/10132 | 1.4% | 6.2 (4.4, 8.9) | 3.6 (2.6, 5.0) |
| Other diagnosesd | ||||||||
| Yes | 20/96 | 21% | 8/141 | 5.7% | 31/266 | 12% | 5.2 (1.8, 14.9) | 1.7 (0.8, 3.6) |
| No | 61/991 | 6.2% | 114/10445 | 1.1% | 167/10363 | 1.6% | 5.5 (4.0, 7.5) | 3.8 (2.9, 5.1) |
PR = adjusted prevalence ratio, CI = confidence interval; TF = transfeminine; CF = cisgender female; CM = cisgender male
Each PR compares the prevalence of self-inflicted injury among TF participants and matched cisgender participants by presence of individual mental health diagnoses
Wald chi-square test for the product term between transgender status and mental health diagnosis had a p-value <.05 for transfeminine vs. reference male comparison
Wald chi-square test for the product term between transgender status and mental health diagnosis had a p-value <.05 for transfeminine vs. reference female comparison
Other diagnoses includes schizophrenia spectrum disorder, other psychoses, dementia, and eating disorders
Table 3.
Associations between gender identity and self-inflicted injury stratified by presence of individual mental health diagnoses among TM and cisgender youth included in the STRONG cohort
| Mental health diagnoses | Transfeminine youth | Cisgender male referents | Cisgender female referents | TM cohort vs. CM referents | TM cohort vs. CF referents | |||
|---|---|---|---|---|---|---|---|---|
| # of events/total | % | # of events/total | % | # of events/total | % | PR (95% CI) | PR (95% CI) | |
|
| ||||||||
| Anxiety disorders | ||||||||
| Yes | 88/447 | 20% | 46/1335 | 3.4% | 111/1920 | 5.8% | 5.2 (3.4, 7.8) | 3.3 (2.4, 4.6) |
| No | 76/984 | 7.7% | 129/12623 | 1.0% | 173/12068 | 1.4% | 7.8 (5.8, 10.4) | 5.3 (4.0, 6.9) |
| Attention deficit disordersc | ||||||||
| Yes | 33/162 | 20% | 50/1531 | 3.3% | 41/590 | 6.9% | 6.7 (3.8, 11.8) | 2.8 (1.6, 4.8) |
| No | 131/1269 | 10% | 125/12427 | 1.0% | 243/13398 | 1.8% | 10.2 (8.0, 12.9) | 5.8 (4.7, 7.1) |
| Autism spectrum disorders | ||||||||
| Yes | 8/38 | 21% | 8/203 | 3.9% | 2/53 | 3.8% | 4.3 (1.3, 14.1) | 4.4 (0.8, 24.2) |
| No | 156/1393 | 11% | 167/13755 | 1.2% | 282/13936 | 2.0% | 9.3 (7.6, 11.5) | 5.6 (4.6, 6.7) |
| Bipolar spectrum disordersb,c | ||||||||
| Yes | 31/90 | 34% | 16/149 | 11% | 35/190 | 18% | 2.5 (1.2, 5.3) | 2.3 (1.1, 4.9) |
| No | 133/1341 | 9.9% | 159/13809 | 1.2% | 249/13798 | 1.8% | 8.8 (7.0, 11) | 5.4 (4.4, 6.6) |
| Conduct/Disruptive disorderc | ||||||||
| Yes | 26/79 | 33% | 33/626 | 5.3% | 38/291 | 13% | -e | 2.5 (1.3, 4.9) |
| No | 138/1352 | 10% | 142/13332 | 1.1% | 246/13697 | 1.8% | -e | 5.7 (4.6, 7.0) |
| Depressive disordersc | ||||||||
| Yes | 134/631 | 21% | 73/1525 | 4.8% | 181/2229 | 8.1% | 4.3 (3.2, 5.9) | 2.3 (1.8, 3.0) |
| No | 30/800 | 3.8% | 102/12433 | 0.8% | 103/11759 | 0.9% | 4.7 (3.1, 7.0) | 4.4 (2.9, 6.6) |
| Personality disordersc | ||||||||
| Yes | 24/64 | 38% | 9/61 | 15% | 29/119 | 24% | 4.4 (1.4, 13.4) | 2.1 (0.9, 5.2) |
| No | 140/1367 | 10% | 166/13897 | 1.2% | 255/13869 | 1.8% | 8.4 (6.8, 10.4) | 5.5 (4.5, 6.7) |
| Substance abuse disorders | ||||||||
| Yes | 47/130 | 36% | 55/905 | 6.1% | 72/617 | 12% | 5.8 (3.2, 10.5) | 3.5 (2.0, 6.1) |
| No | 117/1301 | 9% | 120/13053 | 0.9% | 212/13371 | 1.6% | 9.8 (7.7, 12.5) | 5.6 (4.5, 7.0 |
| Other diagnosesb,c,d | ||||||||
| Yes | 30/126 | 24% | 15/201 | 7.5% | 47/358 | 13% | 2.9 (1.3, 6.4) | 1.7 (1.0, 3.0) |
| No | 134/1305 | 10% | 160/13757 | 1.2% | 237/13630 | 1.7% | 9.0 (7.2, 11.2) | 5.9 (4.8, 7.2) |
PR = prevalence ratio, CI = confidence interval; TM = transmasculine; CF = cisgender female; CM = cisgender male
compares the prevalence of self-inflicted injury among TM participants and matched cisgender participants by presence of individual mental health diagnoses
Wald chi-square test for the product term between transgender status and mental health diagnosis had a p-value <.05 for transmasculine vs. reference male comparison
Wald chi-square test for the product term between transgender status and mental health diagnosis had a p-value <.05 for transmasculine vs. reference female comparison
Other diagnoses includes schizophrenia spectrum disorder, other psychoses, dementia, and eating disorders
Model did not converge.
Additive interaction between TGD identities and number of mental health diagnoses was evident when comparing prevalence of self-inflicted injuries across six groups (Tables 4 and 5). For example, compared to CM youths with no mental health diagnoses (reference group) the PR for CM with 3+ diagnoses (PRA-B+) was 19.6. Relative to the same reference group, the corresponding PR for TF youth with 0 diagnoses (PRA+B−) was 5.5. In the absence of additive interaction, the expected PR comparing the same reference group to TF youth with 3+ diagnoses (PRA+B+) would be 24.0, but the observed PR was much higher at 43.4. This resulted in the RERI estimate of 19.4. As shown in Tables 4 and 5, all comparisons suggested positive additive interaction. A corresponding comparison of observed PRA-B+ estimates to those expected on the multiplicative scale showed that in all instances the MIR values were less than 1.0, except for two comparisons. The magnitude of negative multiplicative interaction appeared to increase (as evidenced in greater departure of MIR from 1.0) with increasing number of mental health diagnoses.
Table 4.
Associations between gender identity and number of mental health diagnoses with self-inflicted injury using a common referent approach among TF and matched cisgender youth included in the STRONG cohort
| TF and CM cohort | TF and CF cohort | |||||
|---|---|---|---|---|---|---|
| # of events/total | % | PR (95% CI) | # of events/total | % | PR (95% CI) | |
|
| ||||||
| Cisgender, 0 diagnoses | 36/7965 | 0.5 % | ref | 53/7889 | 0.7 % | ref |
| Cisgender, 1–2 diagnoses | 39/2048 | 1.9 % | 4.3 (2.7, 6.7) | 76/2214 | 3.4 % | 5.8 (4.0, 8.3) |
| Cisgender, 3+ diagnoses | 47/573 | 8.2 % | 19.6 (11.9, 32.3) | 69/526 | 13 % | 21.7 (14.4, 32.6) |
| TF, 0 diagnoses | 13/512 | 2.5 % | 5.5 (2.9, 10.4) | 13/512 | 2.5 % | 4.8 (2.6, 8.8) |
| TF, 1–2 diagnoses | 28/354 | 7.9 % | 17.6 (10.2, 30.5) | 28/354 | 7.9 % | 9.7 (5.9, 15.9) |
| TF, 3+ diagnoses | 40/221 | 18 % | 43.4 (24.7, 76.3) | 40/221 | 18 % | 27.4 (17.4, 42.9) |
|
| ||||||
| Magnitude of additive interaction (RERI)a between TF status and 1–2 mental health diagnoses | 8.9 (observed PR=17.6, expected PR=8.7) | 0.2 (observed PR=9.7, expected PR =9.5) | ||||
| Magnitude of additive interaction (RERI)a between TF status and 3+ mental health diagnoses | 19.4 (observed PR=43.4, expected PR=24.0) | 1.9 (observed PR=27.4, expected PR=25.4) | ||||
| Magnitude of multiplicative interaction (MIR)a between TF status and 1–2 mental health diagnoses | 0.8 (observed PR=17.6, expected PR=23.3) | 0.4 (observed PR=9.7, expected PR=27.5) | ||||
| Magnitude of multiplicative interaction (MIR)a between TF status and 3+ mental health diagnoses | 0.4 (observed PR=43.4, expected PR=107.3) | 0.3 (observed PR=27.4, expected PR=102.9) | ||||
PR = prevalence ratio; CI = confidence interval; TF = transfeminine; CF = cisgender female; CM = cisgender male; RERI = relative excess risk due to interaction; MIR=multiplicative interaction ratio
Value obtained from a model, which accounts for matched study design; minor differences may appear due to rounding.
Table 5.
Associations between gender identity and number of mental health diagnoses with self-inflicted injury using a common referent approach among TM and matched cisgender youth included in the STRONG cohort
| TF and CM cohort | TF and CF cohort | |||||
|---|---|---|---|---|---|---|
| # of events/total | % | PR (95% CI) | # of events/total | % | PR (95% CI) | |
|
| ||||||
| Cisgender, 0 diagnoses | 64/10363 | 0.6% | ref | 83/10386 | 0.8% | ref |
| Cisgender, 1–2 diagnoses | 62/2822 | 2.2% | 3.5 (2.5, 5.1) | 99/2912 | 3.4% | 4.8 (3.5, 6.5) |
| 49/773 | 6.3% | 102/690 | 15% | 22.7 (16.2, 31.8) | ||
| Cisgender, 3+ diagnoses | 9.9 (6.6, 14.8) | |||||
| TM, 0 diagnoses | 21/666 | 3.2% | 5.2 (3.2, 8.5) | 21/666 | 3.2% | 3.8 (2.4, 6.2) |
| 69/492 | 14% | 21.1 (14.4, 31.0) | 69/492 | 14% | 19.6 (13.7, 28.1) | |
| TM, 1–2 diagnoses | ||||||
| TM, 3+ diagnoses | 74/273 | 27% | 46.6 (30.6, 70.9) | 74/273 | 27% | 35.5 (23.6, 53.5) |
|
| ||||||
| Magnitude of additive interaction (RERI)a between TF status and 1–2 mental health diagnoses | 13.4 (observed PR=21.1, expected PR=7.8) | 10.0 (observed PR=19.6, expected PR=7.6) | ||||
| Magnitude of additive interaction (RERI)a between TF status and 3+ mental health diagnoses | 32.5 (observed PR=46.6, expected PR=14.1) | 10.0 (observed PR=35.5, expected PR=25.6) | ||||
| Magnitude of multiplicative interaction (MIR)a between TF status and 1–2 mental health diagnoses | 1.1 (observed PR=21.1, expected PR=18.4) | 1.1 (observed PR=19.6, expected PR=18.3) | ||||
| Magnitude of multiplicative interaction (MIR)a between TF status and 3+ mental health diagnoses | 0.9 (observed PR=46.6, expected PR=51.8) | 0.4 (observed PR=35.5, expecte PR=87.2) | ||||
PR = prevalence ratio; CI = confidence interval; TM – transmasculine; CF = cisgender female; CM = cisgender male; RERI = relative excess risk due to interaction; MIR=multiplicative interaction ratio
Values obtained from a model, which accounts for matched study design; minor differences may appear due to rounding.
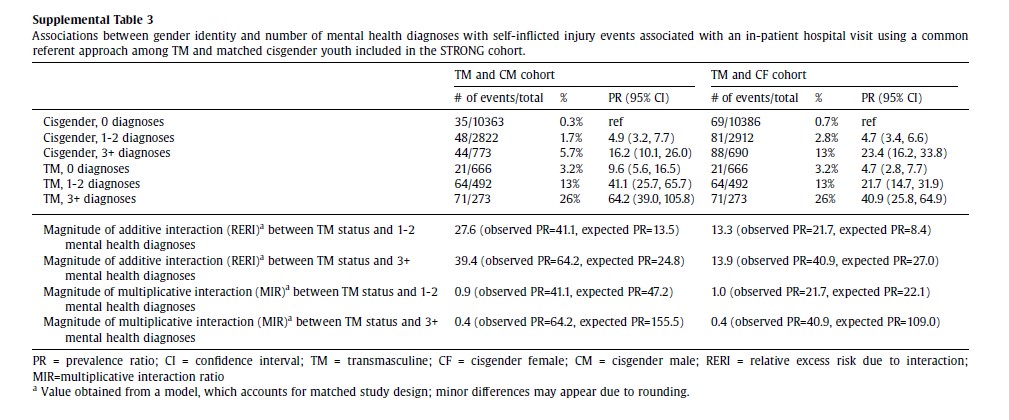
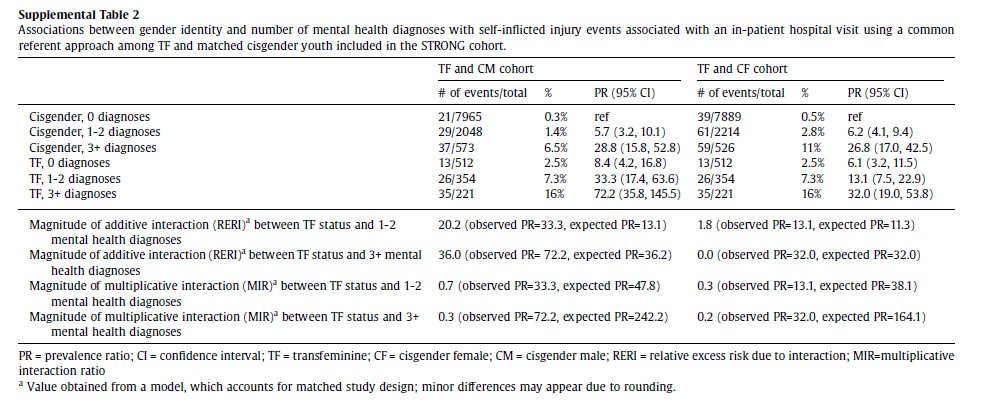
When examining self-inflicted injuries associated with a hospital visit, findings remained consistent and suggestive of positive additive interaction for the majority of comparisons and negative multiplicative interaction (Supplemental Tables 2 and 3). Additionally, restricting analyses to only include TGD participants without a diagnosis of gender dysphoria also did not meaningfully change findings, although some of the estimates were less precise due to sparse numbers (Supplemental Tables 4 and 5).
Consistent with negative multiplicative interaction, the PR estimates for self-inflicted injury comparing TGD youth and cisgender youth attenuated as the number of mental health diagnoses increased (Supplemental Table 6). For example, comparing TF youth to CM referents, the prevalence ratio for self-inflicted injury was 5.5 (95% CI: 2.9, 10.4) among those with no mental health diagnoses, 4.2 (95% CI: 2.4, 7.3) among those with 1–2 mental health diagnoses, and 2.2 (95% CI: 1.3, 3.8) among those with 3+ mental health diagnoses.
Discussion
This study documents gender identity-related differences in self-inflicted injury and a high prevalence of mental health diagnoses among TGD adolescents and young adults, corroborating findings from previous reports.3–7,24–29 TGD adolescents and young adults were more likely to have a self-inflicted injury, various mental health diagnoses, and multiple mental health diagnoses than their cisgender peers. Analysis of multiplicative interaction demonstrated that ratios of self-inflicted injury prevalence in TGD versus cisgender youth was far more pronounced in the absence of mental health diagnoses indicating a negative multiplicative interaction in most analyses. When the same data were examined on the additive scale, we observed a substantial positive interaction between TGD identities and mental health diagnoses in most analyses. Taken together these results serve as a reminder that interaction is scale dependent.22 Unlike measures of multiplicative interaction, measures of additive interaction account for the background prevalence of self-inflicted injury (i.e., among those with 0 mental health diagnoses) among cisgender youth, which was relatively low (less than 1%). Consequently, associations between the number of mental health diagnoses and suicidality may appear “stronger” or “weaker” in TGD vs. cisgender youth, depending on the scale. Our approach to assessing additive interaction relies on ratio measures. It is also possible to examine additive interaction by comparing prevalence differences; however, to our knowledge, this cannot be readily accomplished using these conditional models.
The differences in the prevalence of mental health diagnoses and the observed additive interaction between TGD status and mental health morbidity may help inform intervention strategies. Among cisgender adolescents and young adults, roughly three quarters (>74%) had 0 mental health diagnoses and contributed about approximately one-quarter of all self-inflicted injuries. Moreover, in all groups, a notable proportion of self-inflicted injuries were among those who had no mental health diagnoses, although the problem appeared to be more pronounced in the TGD group. These findings provide additional support for the American Academy of Pediatrics recommendation of universal suicide screening among all youth ages 12 and above.30 More frequent screening and intensive suicide prevention interventions may be needed for youth with at least one mental health diagnosis and especially among those who identify as TGD.
Further, many studies have focused on possible minority stressors and their link to suicidality among TGD persons.12–15 A robust body of literature has found that TGD youth are more likely to experience various types of victimization.3,31 A recent analysis of Youth Risk Behavior Survey data provided evidence of a syndemic model in which socio-structural factors (e.g., housing insecurity) was associated with co-occurrence of substance use and depressive symptoms among TGD youth, which, in turn, were associated with increased odds of suicidal ideation, plans, and attempts.32 Additionally, measures of structural stigma (e.g., discriminatory policies) have also been associated with poorer outcomes among transgender populations.12,33 Future research may benefit from considering the complex interplay between policy, chronic and acute life stressors, mental health conditions, and suicide outcomes among TGD youth.
Important characteristics of this study include the use of de-identified EHR-based data, and a well-defined sampling frame within three large community-based health plans. These methodological features ensured inclusion of all eligible individuals without a need for subject opt-in and offered an opportunity to match each TGD participant to cisgender referents with the same demographic characteristics, from the same geographic areas, and enrolled in the same health systems.34
As the use of EHR population-based studies to research health issues among TGD populations has increased, careful consideration of how gender identities and examined outcomes are measured is needed.35 Perhaps the most notable limitation of this study is the use of self-inflicted injury diagnoses as a surrogate for suicide attempts. It is likely that some of the self-inflicted injuries were not attempted suicides. It is worth pointing out, however, that when the data were restricted to presumably more serious events associated with inpatient hospitalization encounters, the results remained the same. Conversely, not all suicide attempts in the study population were documented in the EHR and a more complete ascertainment of these events would require patient or parent reporting, which was beyond the scope of the current study. Our results may be influenced by the differences in the available data points prior to the index date. We have addressed this issue in our previous publication by adjusting for the total number of visits, and by using two time-windows: ever before index date and 6 months before index date.4 The results were generally the same, although some of the associations were stronger when the data were limited to the preceding six months. As the goal of the present paper was to assess interaction between TGD status and mental health morbidity in relation to self-inflicted injuries, the main outcome of interest and the mental health diagnoses were ascertained during the same time interval for each participant. TGD people enrolled in integrated health care systems represent a group of persons with health insurance that may not be representative of the TGD population with limited access to care. On the other hand, the STRONG cohort does include persons enrolled in Medicaid plans, ensuring at least some representation of individuals with lower socioeconomic position.17 Further, eligible TGD cohort members were seeking care at participating health care systems between 2006 and 2014 and recent experiences of TGD youth may differ. This study used a cross-sectional design to characterize history of self-inflicted injury and mental health diagnoses among TGD youth at the time they first disclosed their gender identity to health providers and temporality cannot be inferred. It was beyond the scope of the present analysis to examine how gender-affirming or mental health services, which are often delivered after the index date, affected subsequent risk of self-inflicted injuries. Longitudinal data indicate that past history of suicide attempt is one of the most important predictors of future events in this population.19 Thus, from the clinical practice perspective, these data support the need for thorough and immediate evaluation of TGD youth as soon as they present for care.
In summary, our findings indicate that the interaction between TGD identity and mental health diagnoses is evident and its direction is scale-dependent. These observations underscore the importance of routine self-harm and suicide risk screening among all youth and perhaps more intensive suicide prevention efforts among those identifying as TGD or gender-questioning, especially those with at least one mental health diagnosis. Such efforts would be complemented by programs and policies that enhance individual, relationship, community, societal factors identified as protective among transgender youth (e.g., social support, access to organizational resources).36
Supplementary Material
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Funding:
The sources of financial support for this work include Contract AD-12–11-4532 from the Patient Centered Outcome Research Institute, Grant R21HD076387 from the Eunice Kennedy Shriver National Institute of Child Health and Human Development, and Grant R01AG066956 from the National Institute of Aging.
Abbreviations:
- TGD
transgender and gender diverse
- EHR
electronic health record
- TM
transmasculine
- TF
transfeminine
- CF
cisgender female
- CM
cisgender male
- ICD
International Classification of Diseases
- PR
prevalence ratio
- CI
confidence interval
- RERI
relative excess risk due to interaction
- STRONG
Study of Transition, Outcomes, and Gender
Footnotes
Footnotes
The general formula for RERI reflecting additive interaction between two factors A and B is written out as: ; where PRA+B+ , PRA+B−, and PRA-B+ are the observed prevalence ratios for persons with both factors A and B relative to the same reference category that includes persons with neither factor. RERI can also be viewed as the difference between the observed PRA+B+ and its expected value on the additive scale. A positive RERI suggests a greater than additive association and a negative RERI suggests a less than additive association. The multiplicative interaction ratio (MIR) is the ratio of the observed PRA+B+ and its expected value on the multiplicative scale. This multiplicative interaction ratio (MIR) is calculated as . A MIR value of >1 is interpreted as positive multiplicative interaction, and a value of <1 it is interpreted as negative multiplicative interaction. In the present analyses, factors A and B denote TGD identities and the number of mental health diagnoses, respectively. In the present analyses, factors A and B denote TGD identities and the number of mental health diagnoses, respectively.
Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
References
- 1.Martinez-Ales G, Hernandez-Calle D, Khauli N, Keyes KM. Why Are Suicide Rates Increasing in the United States? Towards a Multilevel Reimagination of Suicide Prevention. In: Baca-Garcia E, ed. Behavioral Neurobiology of Suicide and Self Harm. Current Topics in Behavioral Neurosciences. Springer International Publishing; 2020:1–23. doi: 10.1007/7854_2020_158 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Hedegaard H, Curtin SC, Warner M. Suicide Rates in the United States Continue to Increase. NCHS Data Brief. 2018;(309):1–8. [PubMed] [Google Scholar]
- 3.Johns MM, Lowry R, Andrzejewski J, et al. Transgender identity and experiences of violence victimization, substance use, suicide risk, and sexual risk behaviors among high school students—19 states and large urban school districts, 2017. Morb Mortal Wkly Rep. 2019;68(3):67. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Becerra-Culqui TA, Liu Y, Nash R, et al. Mental health of transgender and gender nonconforming youth compared with their peers. Pediatrics. 2018;141(5). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Wichaidit W, Assanangkornchai S, Chongsuvivatwong V. Disparities in behavioral health and experience of violence between cisgender and transgender Thai adolescents. PloS One. 2021;16(5):e0252520. doi: 10.1371/journal.pone.0252520 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Vance SRJ, Boyer CB, Glidden DV, Sevelius J. Mental Health and Psychosocial Risk and Protective Factors Among Black and Latinx Transgender Youth Compared With Peers. JAMA Netw Open. 2021;4(3):e213256. doi: 10.1001/jamanetworkopen.2021.3256 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Toomey RB, Syvertsen AK, Shramko M. Transgender adolescent suicide behavior. Pediatrics. 2018;142(4). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Office of the Surgeon General (US), National Action Alliance for Suicide Prevention (US). 2012 National Strategy for Suicide Prevention: Goals and Objectives for Action: A Report of the U.S. Surgeon General and of the National Action Alliance for Suicide Prevention. US Department of Health & Human Services (US); 2012. Accessed October 23, 2021. http://www.ncbi.nlm.nih.gov/books/NBK109917/ [PubMed] [Google Scholar]
- 9.Mustanski B, Liu RT. A longitudinal study of predictors of suicide attempts among lesbian, gay, bisexual, and transgender youth. Arch Sex Behav. 2013;42(3):437–448. [DOI] [PubMed] [Google Scholar]
- 10.Brent DA, Perper JA, Moritz G, et al. Psychiatric risk factors for adolescent suicide: a case-control study. J Am Acad Child Adolesc Psychiatry. 1993;32(3):521–529. doi: 10.1097/00004583-199305000-00006 [DOI] [PubMed] [Google Scholar]
- 11.Mental disorders and comorbidity in suicide. Am J Psychiatry. 1993;150(6):935–940. doi: 10.1176/ajp.150.6.935 [DOI] [PubMed] [Google Scholar]
- 12.Perez-Brumer A, Hatzenbuehler ML, Oldenburg CE, Bockting W. Individual-and structural-level risk factors for suicide attempts among transgender adults. Behav Med. 2015;41(3):164–171. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Goldblum P, Testa RJ, Pflum S, Hendricks ML, Bradford J, Bongar B. The relationship between gender-based victimization and suicide attempts in transgender people. Prof Psychol Res Pract. 2012;43(5):468. [Google Scholar]
- 14.Leon K, O’Bryan J, Wolf-Gould C, Turell SC, Gadomski A. Prevalence and Risk Factors for Nonsuicidal Self-Injury in Transgender and Gender-Expansive Youth at a Rural Gender Wellness Clinic. Transgender Health. 2021;6(1):43–50. doi: 10.1089/trgh.2020.0031 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Lefevor GT, Boyd-Rogers CC, Sprague BM, Janis RA. Health disparities between genderqueer, transgender, and cisgender individuals: An extension of minority stress theory. J Couns Psychol. 2019;66(4):385–395. doi: 10.1037/cou0000339 [DOI] [PubMed] [Google Scholar]
- 16.Getahun D, Nash R, Flanders WD, et al. Cross-sex hormones and acute cardiovascular events in transgender persons: a cohort study. Ann Intern Med. 2018;169(4):205–213. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Quinn VP, Nash R, Hunkeler E, et al. Cohort profile: Study of Transition, Outcomes and Gender (STRONG) to assess health status of transgender people. BMJ Open. 2017;7(12):e018121. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Rossom RC, Coleman KJ, Ahmedani BK, et al. Suicidal ideation reported on the PHQ9 and risk of suicidal behavior across age groups. J Affect Disord. 2017;215:77–84. doi: 10.1016/j.jad.2017.03.037 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Mak J, Shires DA, Zhang Q, et al. Suicide attempts among a cohort of transgender and gender diverse people. Am J Prev Med. 2020;59(4):570–577. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Green AE, DeChants JP, Price MN, Davis CK. Association of Gender-Affirming Hormone Therapy With Depression, Thoughts of Suicide, and Attempted Suicide Among Transgender and Nonbinary Youth. J Adolesc Health. 2022;70(4):643–649. doi: 10.1016/j.jadohealth.2021.10.036 [DOI] [PubMed] [Google Scholar]
- 21.Mental Health Research Network’s Diagnosis Codes. Published online May 27, 2021. Accessed July 13, 2021. https://github.com/MHResearchNetwork/Diagnosis-Codes
- 22.VanderWeele TJ, Knol MJ. A Tutorial on Interaction. Epidemiol Methods. 2014;3(1):33–72. doi: 10.1515/em-2013-0005 [DOI] [Google Scholar]
- 23.Richardson DB, Kaufman JS. Estimation of the Relative Excess Risk Due to Interaction and Associated Confidence Bounds. Am J Epidemiol. 2009;169(6):756–760. doi: 10.1093/aje/kwn411 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Reisner SL, Biello KB, White Hughto JM, et al. Psychiatric Diagnoses and Comorbidities in a Diverse, Multicity Cohort of Young Transgender Women. JAMA Pediatr. 2016;170(5):481–486. doi: 10.1001/jamapediatrics.2016.0067 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Reisner SL, Vetters R, Leclerc M, et al. Mental health of transgender youth in care at an adolescent urban community health center: a matched retrospective cohort study. J Adolesc Health Off Publ Soc Adolesc Med. 2015;56(3):274–279. doi: 10.1016/j.jadohealth.2014.10.264 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Olson J, Schrager SM, Belzer M, Simons LK, Clark LF. Baseline Physiologic and Psychosocial Characteristics of Transgender Youth Seeking Care for Gender Dysphoria. J Adolesc Health Off Publ Soc Adolesc Med. 2015;57(4):374–380. doi: 10.1016/j.jadohealth.2015.04.027 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Coulter RWS, Blosnich JR, Bukowski LA, Herrick AL, Siconolfi DE, Stall RD. Differences in Alcohol Use and Alcohol-Related Problems between Transgender- and Nontransgender-identified Young Adults. Drug Alcohol Depend. 2015;154:251–259. doi: 10.1016/j.drugalcdep.2015.07.006 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Warrier V, Greenberg DM, Weir E, et al. Elevated rates of autism, other neurodevelopmental and psychiatric diagnoses, and autistic traits in transgender and gender-diverse individuals. Nat Commun. 2020;11(1):3959. doi: 10.1038/s41467-020-17794-1 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Mitchell HK, Keim G, Apple DE, et al. Prevalence of gender dysphoria and suicidality and self-harm in a national database of paediatric inpatients in the USA: a population-based, serial cross-sectional study. Lancet Child Adolesc Health. 2022;6(12):876–884. doi: 10.1016/S2352-4642(22)00280-2 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.American Academy of Pediatrics,. Screening for Suicide Risk in Clinical Practice. Accessed October 17, 2022. http://www.aap.org/en/patient-care/blueprint-for-youth-suicide-prevention/strategies-for-clinical-settings-for-youth-suicide-prevention/screening-for-suicide-risk-in-clinical-practice/
- 31.Peitzmeier SM, Malik M, Kattari SK, et al. Intimate Partner Violence in Transgender Populations: Systematic Review and Meta-analysis of Prevalence and Correlates. 10.2105/AJPH.2020.305774. doi: 10.2105/AJPH.2020.305774 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Lett E, Abrams MP, Moberg E, Benson GP, Perlson JE. Syndemic relationship of depressive symptoms, substance use, and suicidality in transgender youth: a cross-sectional study using the US youth risk behavior surveillance system. Soc Psychiatry Psychiatr Epidemiol. Published online 2022:1–12. [DOI] [PubMed] [Google Scholar]
- 33.Bränström R, Pachankis JE. Country-level structural stigma, identity concealment, and day-to-day discrimination as determinants of transgender people’s life satisfaction. Soc Psychiatry Psychiatr Epidemiol. 2021;56:1537–1545. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Hashemi L, Zhang Q, Getahun D, et al. Longitudinal Changes in Liver Enzyme Levels Among Transgender People Receiving Gender Affirming Hormone Therapy. J Sex Med. 2021;18(9):1662–1675. doi: 10.1016/j.jsxm.2021.06.011 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Kronk CA, Everhart AR, Ashley F, et al. Transgender data collection in the electronic health record: Current concepts and issues. J Am Med Inform Assoc JAMIA. 2022;29(2):271–284. doi: 10.1093/jamia/ocab136 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Johns MM, Beltran O, Armstrong HL, Jayne PE, Barrios LC. Protective factors among transgender and gender variant youth: A systematic review by socioecological level. J Prim Prev. 2018;39:263–301. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.