

Abstract
Suprascapular nerve compression at the spinoglenoid notch can lead to posterior shoulder pain, muscle weakness, and longstanding muscle atrophy of the infraspinatus. Although rare, it is most commonly seen in overhead athletes and laborers who perform repetitive overhead activities. Early diagnosis requires a thorough history and physical examination including imaging, diagnostic injections, and electromyography to avoid a missed diagnosis. While a course of nonoperative treatment is most often prescribed, early surgical intervention may be prudent to avoid irreversible damage especially if a space occupying lesion is present. This article will describe the history, physical examination findings, diagnostic workup, and our surgical technique for arthroscopic decompression of the suprascapular nerve at the spinoglenoid notch through a simple posterior approach avoiding the subacromial space.
Keywords: Suprascapular nerve, spinoglenoid notch, arthroscopic decompression, posterior shoulder pain, infraspinatus atrophy, nerve release
Suprascapular neuropathy is a rare but not to be missed cause of shoulder pain accounting for 1%-2% of all shoulder pathologies.34 Suprascapular nerve entrapment may occur at the suprascapular notch due to compression by the transverse scapular ligament or at the spinoglenoid notch by the spinoglenoid ligament or a ganglion cyst6,21,22,24 (Fig. 1). While conservative treatment is usually the first line of management, a prolonged disease course can lead to weakness in external rotation and abduction with irreversible wasting of the infraspinatus muscle belly.28 The benefits of arthroscopic surgical decompression in lieu of open procedures have been established in the literature.10,12,16 The purpose of this article is to describe the senior author's technique for arthroscopic decompression of the suprascapular nerve at the spinoglenoid notch through a simple posterior approach avoiding the subacromial space, enabling a rapid return to activities of daily living and sport.
Figure 1.
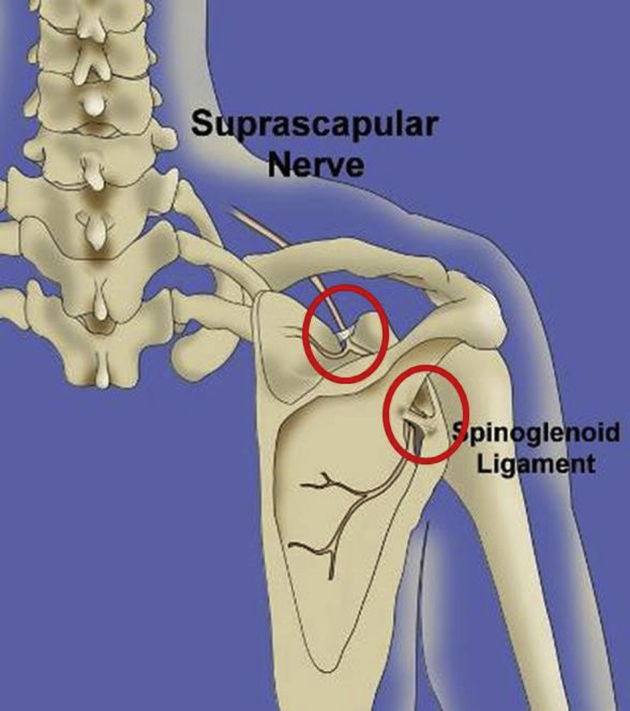
Right shoulder posterior view artwork demonstrating the 2 sites of compression of the suprascapular nerve.
Anatomy
The suprascapular nerve is a mixed sensory and motor nerve that classically arises from the upper trunk of the brachial plexus (C5-C6) at Erb's point; however, variations exist. The C4 nerve root has been shown to contribute to the suprascapular nerve in some cases and in approximately 6% of patients the suprascapular nerve is comprised of only the C5 ventral rami.25,32 At the suprascapular notch, the suprascapular nerve travels under the transverse scapular ligament. The suprascapular artery most commonly traverses over the transverse scapular ligament but may travel with the suprascapular nerve in rare instances.29 The nerve then travels laterally through the supraspinatus fossa, around the scapular spine, and under the spinoglenoid ligament before descending into the infraspinatus fossa.30 The suprascapular nerve then gives off several motor branches to the infraspinatus muscle belly (Fig. 2).
Figure 2.
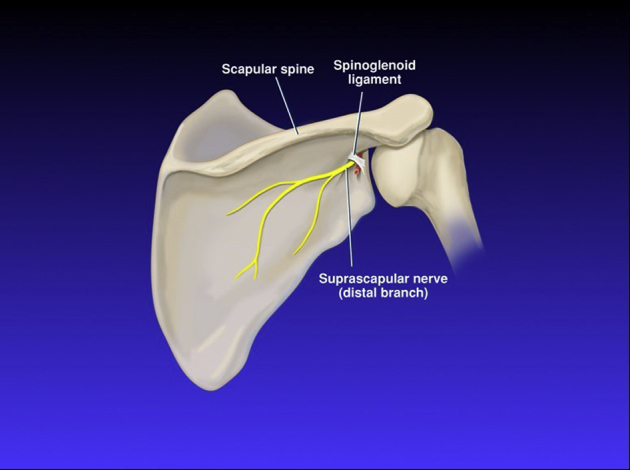
The suprascapular nerve descending into the infraspinatus fossa passing under the spinoglenoid ligament.
The spinoglenoid ligament runs from the scapular spine to the posterior glenoid. Previous research has positively identified the presence of the spinoglenoid ligament in 100% of specimens in cadaveric dissections.22 Two types of spinoglenoid ligaments have been described in the literature: a thin indistinct band of tissue (type I) and a well-formed ligament (type II).22 On gross examination, the spinoglenoid ligament has an irregular quadrangular shape, thinnest in its midportion and fanning out to its insertions superomedially and inferolaterally22 (Fig. 3). The inferolateral portion of the ligament has superficial layers that insert on the glenohumeral joint capsule and a deep layer that inserts at the glenoid neck. The distal branch of the suprascapular nerve, along with the suprascapular artery and vein, pass at the base of the scapular spine under the spinoglenoid ligament where compression occurs.
Figure 3.

The spinoglenoid ligament, quadrangular in shape, demonstrated in the posterior view of a right shoulder dissection. Note the distal branch of the suprascapular nerve is compressed.
Pathophysiology
Injury to the suprascapular nerve most commonly occurs at the suprascapular notch from compression by the transverse scapular ligament. However, compression at the spinoglenoid notch has also been well described. A stenotic notch and an ossified spinoglenoid ligament have been cited as causative factors of suprascapular neuropathy at the spinoglenoid notch.3,4 In overhead athletes, such as pitchers and volleyball players, repetitive traction and microtrauma have also been cited as causes of injury.8,13,14,21,22 When the arm is in a position of overhead external rotation, the spinoglenoid ligament tightens which can lead to compression of the suprascapular nerve.21 Compression of the suprascapular nerve by a soft tissue mass or ganglion cyst at the spinoglenoid ligament as a result of labral or capsule injury has also been described.18,20 Tears of the labrum or joint capsule may act as a one-way valve where synovial fluid is forced through tissues exiting the joint leading to the formation of a ganglion cyst.18 The relatively fixed position of the suprascapular nerve at the spinoglenoid ligament thus can lead to compression by formed ganglia or soft tissue mass. If a ganglion cyst is present, we choose to decompress the cyst posteriorly with meticulous dissection to remove the cyst stalk and the utilization of coagulation, no different than a ganglion cyst in the wrist, and not repair the labrum with excellent results and no recurrence of fluid accumulation.1,31 Labral repair alone will not lead to resolution of atrophy when present.
Indications/contraindications
The primary indications for arthroscopic decompression of the suprascapular nerve and the spinoglenoid notch are a prolonged course of symptoms, most commonly a chronic ache in the posterolateral aspect of the shoulder, and a failed minimum 6-month course of nonoperative treatment. Nonoperative treatment should include a period of rest and activity modification, and anti-inflammatory medication followed by a supervised physical therapy program. The focus of physical therapy is to preserve the normal physiologic range of motion of the shoulder and strengthen the shoulder girdle. Exercises include scapular stabilization, and resistive strength straining of the trapezius, rhomboids, and serratus musculature. When a space occupying lesion is present or there is visible atrophy of the infraspinatus, the course of nonoperative treatment should be minimal (maximum 3 months) to avoid irreversible damage to the infraspinatus.20
Compression at the spinoglenoid ligament is often insidious at onset with less severe symptoms compared to compression at the suprascapular notch. Therefore, a detailed history, physical examination, and diagnostic workup are essential to determine appropriate management. Patients often present with a chief complaint of a diffuse ache around the shoulder region with the pain most commonly localized to the region 4 cm medial to the posterolateral corner of acromion as well as the posterior aspect of the glenohumeral joint.23 These symptoms may be accompanied by complaints of catching, locking, or clicking, likely the result of a concomitant labral tear.23
Appreciable physical examination findings may include painful palpation at the spinoglenoid notch, visible atrophy of the infraspinatus muscle belly (Fig. 4), and shoulder external rotation and abduction weakness. This constellation of findings is often confused and attributed to a possible rotator cuff tear, wrongly so, which can be ruled out with advanced imaging. The cross-arm adduction test may reproduce the patient's symptoms with the arm extended and internally rotated. To perform the cross-arm adduction test, the shoulder is flexed to 90° with the elbow positioned in 90° of flexion. The examiner then gently horizontally adducts the arm toward the contralateral shoulder and assesses for provocation of symptoms. Pain may be present at the posterior shoulder and must be distinguished from pain localized to the acromioclavicular joint. Positive findings occur because of a small branch of the suprascapular nerve known to innervate the acromioclavicular joint.
Figure 4.

Clinical photograph of a right shoulder (posterior view) demonstrating severe atrophy of the infraspinatus in a 21-year-old female tennis player.
Radiographic examination should include an anteroposterior, axillary lateral, and the Y or supraspinatus outlet view. Findings on plain radiographs are often nonspecific but can assess for any fracture or minute trauma to the scapula, clavicle, coracoid, or glenoid neck. Magnetic resonance imaging can help to identify associated posterior-superior labral tears and ganglion cysts (Figs. 5 and 6). Ganglion cysts are often seen as a homogenous signal, low T1 intensity, high T2 intensity, and rim enhancement if contrast is used.9 Increased signal intensity on T2 fast spin echo imaging with fat saturation with a normal muscle mass of the infraspinatus muscle can indicate suprascapular nerve compression at the spinoglenoid notch. This finding may imply a subacute denervation of the nerve caused by neurogenic edema. Chronic denervation of the infraspinatus is best seen on T1 spin echo sequences with increased signal intensity within the muscle mass suggestive of muscle atrophy and fatty infiltration (Fig. 7). Ultrasound may aid in identifying ganglion cysts in the clinic as well as ganglion cyst aspiration in skilled hands, if felt appropriate.
Figure 5.

Coronal magnetic resonance image demonstrating a ganglion cyst displacing the suprascapular nerve at the spinoglenoid notch.
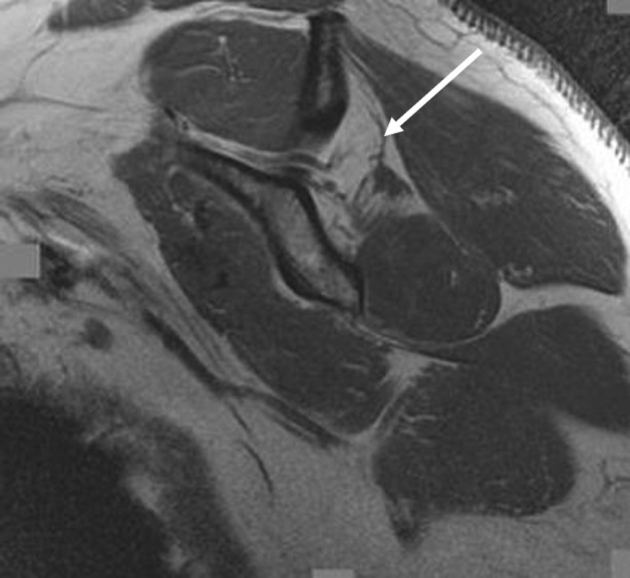
Figure 6.

Axial magnetic resonance image demonstrating a labral tear with associated ganglion cyst compressing the suprascapular nerve at the spinoglenoid notch.
Figure 7.
Sagittal oblique magnetic resonance image demonstrating isolated infraspinatus atrophy in a volleyball player. Note the course of the nerve in this T2-weighted image.
Diagnostic injections can also aid in making the correct diagnosis of suprascapular nerve entrapment at the spinoglenoid notch when atrophy of the infraspinatus is not present (Fig. 8). Administration of 10 cc of 1% lidocaine anesthetic injection approximately 4 cm medial to the posterolateral corner of the acromion and 1-2 cm inferior to the scapular spine may change the pain profile of the patient. Alleviation of the chronic ache in the posterior shoulder following the injection is a confirmatory finding. Additionally, if the cross-arm adduction test was positive prior to the injection, it should be repeated following the injection to assess for alleviation of symptoms.
Figure 8.

Lidocaine injection being administered at the spinoglenoid ligament, 4 cm medial to the posterolateral corner of the acromion.
Electromyography (EMG) and nerve conduction studies can help to discriminate points of compression of the suprascapular nerve at either the transverse scapular ligament or the spinoglenoid notch. When compression occurs at the spinoglenoid notch, the nerve shows decreased innervation of the infraspinatus muscle with normal innervation of the supraspinatus muscle. Motor distal latency and motor response amplitude at the supraspinatus and infraspinatus muscles are measured with stimulation at Erb's point. Latency greater than 3.3 milliseconds (range: 2.4-4.2 milliseconds) confirms compression at the spinoglenoid ligament.11 EMG recordings of the infraspinatus can be challenging as only 1 branch may be affected and the rest of the muscle intact. Multiple locations should be tested and caution should be used to avoid stimulation of other periscapular muscles that can lead to volume interference. An alternative procedure would be to use needle recordings to isolate these muscles. A negative finding by EMG does not rule out suprascapular nerve compression.
Technique
A posterior or subacromial approach can be used to release the suprascapular nerve at the spinoglenoid ligament (see Supplementary Video 1). Previous studies and descriptions have utilized the subacromial approach.10,16 The posterior approach will be described here as we believe the anatomy is best visualized with this approach and morbidity and postoperative recovery are simpler with faster return to activities of daily living and sport in patients with isolated compression of the suprascapular nerve at the spinoglenoid ligament.
Positioning and setup
The procedure is performed under general anesthesia. The patient may be placed in a lateral decubitus or a beach chair position with a bean bag and the arm placed at the side and draped free from the mid-sternum to the mid-posterior spine with complete access to the scapula. An examination under anesthesia is performed to assess shoulder range of motion and any signs of any concomitant shoulder instability or any other significant findings.
A posteromedial portal and posterolateral portal in the infraspinatus fossa are used (Fig. 9). The viewing portal is established 8 cm medial to the posterolateral corner of the acromion just inferior to the scapula spine and the working portal is established 4 cm medial to the posterolateral corner of the acromion just inferior to the scapula spine. We recommend the anesthesiologist maintain a systolic blood pressure slightly below 100 mm Hg and the pump pressure if used be maintained at 45 mm Hg to avoid any unnecessary swelling. This population of patients is young and often does not have any hypertension issues.
Figure 9.
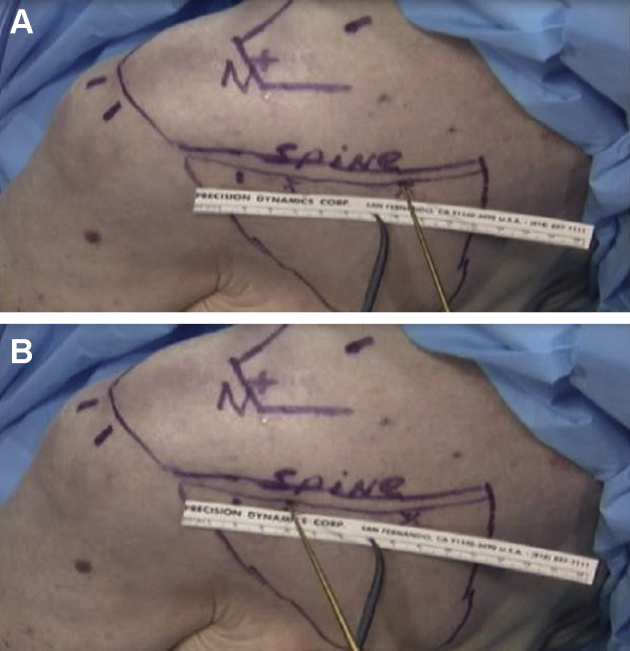
(A) Left shoulder, posterior view. The gold probe is pointing 8 cm medial to the posterolateral corner of the acromion. This portal is the viewing portal for the release of the spinoglenoid ligament with 30°arthroscope. (B) Clinical photograph of the posterior left shoulder. The gold probe is pointing 4 cm medial to the posterolateral corner of the acromion. This is the working portal for release of the spinoglenoid ligament. See Supplementary Video 1 for additional details.
Endoscopic releases of the suprascapular nerve
A blunt trocar is introduced into the viewing portal, directed toward the infraspinatus fossa (Fig. 10). The trocar is used to sweep the tissue under the spine of the scapula away. The trocar is then directed toward the working portal, passing the suprascapular nerve superiorly heading and falling into the spinoglenoid notch. To allow for adequate visualization, it is essential to ensure the trocar sweeps under the roof of the infraspinatus spine along its curvature.
Figure 10.

Left shoulder, posterior view. The trocar is introduced and the tip of the blunt trocar is used to palpate the spine of the scapula. The trocar is then moved inferiorly and gently swept to clear a space with the infraspinatus muscle posterior and the tip of the trocar on the infraspinatus fossa. The tip of the trocar is then moved laterally toward the working portal. The trocar sweeps the infraspinatus muscle as it is moved laterally and posteriorly to allow visualization of the spinoglenoid ligament. Please see Supplementary Video 1.
The arthroscope then replaces the trocar in the posteromedial viewing portal and the spinoglenoid ligament is first visualized hugging the spinoglenoid notch medially (Fig. 11). Identification of the various landmarks is now complete. Success with this procedure is achieved with visualization of the spine of the scapula to be maintained throughout the release of the ligament and decompression of the nerve.
Figure 11.

(A) Left shoulder, posterior view. The 30° arthroscope is introduced into the viewing portal located 8 cm medial to the posterolateral acromion. Please see Supplementary Video 1. (B) Left shoulder, posterior view. Note the relationship of the standard posterior intra-articular portal to the viewing and working portals for spinoglenoid ligament release.
Next, the trocar is introduced into the posterolateral working portal with the use of an 18-gauge spinal needle. The soft tissue is teased away laterally noting that the course of the suprascapular nerve is always on the medial side of the spinoglenoid notch (Fig. 12). With the suction turned off, a small radius, nonaggressive shaver or radiofrequency wand can now be used to clear the remaining tissue and, more specifically, the spinoglenoid ligament off the spine of the scapula (Fig. 13). The ligament located laterally can be resected by staying on the spine of the scapula to avoid bleeding while maintaining visualization of the suprascapular nerve located medially. The ligament can be followed to its insertion at the glenohumeral joint to confirm and visualize the complete resection of the ligament. The released suprascapular nerve and artery can be seen hugging tightly as it wraps around the notch and heads medially giving its 2-4 muscular branches to the infraspinatus muscle. The blunt tip trocar can be used to assess the mobility and adequate release of the suprascapular nerve (Fig. 14).
Figure 12.

Intraoperative photograph of the same left shoulder showing perineural fat with the trocar left teasing the spinoglenoid ligament off the suprascapular nerve. Partially detached spinoglenoid ligament, type 2.
Figure 13.

(A) The arthroscope and shaver are now moved into the appropriate spinoglenoid portals for decompression of the suprascapular nerve at the spinoglenoid notch. (B) Intraoperative photograph of the same left shoulder, posterior view. The shaver has taken off the spinoglenoid ligament directly off the spine of the scapula. All work is being completed lateral to the suprascapular nerve.
Figure 14.

(A) The suprascapular nerve seen medially with the suprascapular artery and the probe holding back the released spinoglenoid ligament. (B) The decompressed suprascapular nerve is now freed and fully mobile as it exits the spinoglenoid notch.
Anatomic variations at the spinoglenoid notch, such as the presence of a ganglion cyst or a bifid suprascapular nerve, should always be noted (Fig. 15). Decompression of the ganglion and excision of the stalk can be easily completed with a posterior approach. It is important to understand that the ganglion root is often headed toward the posterior inferior quadrant of the glenohumeral joint.
Figure 15.

(A) Left shoulder, posterior view with the arrow pointing to the suprascapular nerve heading medially. The bulging tissue to the left is a ganglion cyst that is not yet decompressed. (B) A bifid suprascapular nerve exiting the spinoglenoid notch. Note the tight compression in this anatomic variant.
Following successful release of the spinoglenoid ligament, the surgeon can, if necessary, proceed with any intra-articular or extra-articular work, as needed. Caution should always be exercised to protect the axillary nerve when performing intra-articular work from the 6 o'clock position. On completion and full inspection, all equipment is removed from the body and the portals are closed in routine manner.
Compression of the suprascapular nerve at the spinoglenoid ligament occurs posteriorly; therefore, we would recommend a direct posterior approach to release the nerve in a simplistic manner. Complications are rare with arthroscopic spinoglenoid ligament release. Meticulous attention is required during dissection and release to avoid iatrogenic injury to the suprascapular nerve, artery, and any surrounding vessels. While the posterior approach may be unfamiliar, taking down the rotator cuff as required in the subacromial approach may potentially cause more damage and prolongs recovery particularly for the throwing or overhead athlete. Additionally, the classic, open approach requires a deep wound in an area where a fair amount of bleeding occurs, minimal visibility, and a greater likelihood of incomplete resection of the spinoglenoid ligament.
Postoperative management
The patient is placed in a sling for comfort through postoperative day 7. If an isolated decompression of the suprascapular nerve was performed, the sling can be removed on postoperative day 7 and progressive range of motion exercises and return to all activities of daily living can be initiated. Full return to overhead activities can be expected by 4-6 weeks. However, if a concomitant labral or rotator cuff repair was performed, then standard, conservative rehabilitation principles for the respective procedures should be followed.
Discussion
While suprascapular nerve compression at the spinoglenoid notch is less common than at the suprascapular notch, early diagnosis and arthroscopic release of the spinoglenoid ligament can alleviate symptoms and prevent chronic infraspinatus muscle atrophy and unremitting pain with overhead activities. The described arthroscopic technique affords the ability to decompress any ganglion cysts as well as avoids muscular detachment as is necessitated in the open technique and the subacromial approach.
In the absence of a space occupying lesion, there is a general consensus to pursue a short course of nonoperative treatment before considering surgical intervention.1,20,23 Isolated, asymptomatic infraspinatus atrophy has been reported in overhead athletes such as volleyball and tennis players.7,8,33 Dominant-side infraspinatus atrophy may not always be associated with functional or performance deficits in these individuals. As they age, these athletes often realize the weakness deficit and chronic ache. Spontaneous reinnervation of the infraspinatus with nonoperative treatment is rare.7,27 In the symptomatic patient with or without a ganglion cyst, earlier surgical intervention is recommended to avoid irreversible damage. If symptomatic without infraspinatus atrophy, we also recommend surgical decompression after 6 months of failed conservative treatment.
Several case studies have been reported in the literature,2,5,17 although given the rare occurrence of isolated suprascapular nerve compression at the spinoglenoid notch, larger scale studies are limited. Mall et al reported on 29 shoulders with isolated compression at the spinoglenoid notch at a mean follow-up of 4.3 years after open decompression.15 Diagnosis was made based on clinical suspicion, physical examination, magnetic resonance imaging, and EMG. Of the 29 shoulders, all regained at least one full muscle strength grade in external rotation and 97% of shoulders exhibited a minimum of 4/5 strength at follow-up. Those with a ganglion cyst had a tendency to recover external rotation strength faster than those without a cyst with an average of 6 weeks.
Most recently, Nolte et al reported on the clinical outcomes after arthroscopic suprascapular nerve decompression in a cohort of patients with compression at either the suprascapular or spinoglenoid notch or both at a mean follow-up of 4.8 years.19 Fourteen patients underwent release of the transverse scapular ligament, 3 patients underwent release of the spinoglenoid ligament, and 2 patients underwent release at both the transverse scapular and spinoglenoid ligaments. A subacromial approach was used in all patients. The American Shoulder and Elbow Surgeons shoulder score, the Quick Disabilities of the Arm, Shoulder and Hand Score, Single Assessment Numeric Evaluation score, and the 12-Item Short Form Health Survey Physical Composite Scale, and external rotation strength significantly improved postoperatively, though the results were not presented by location of release. Similar findings were previously reported by Shah et al in 24 patients who underwent suprascapular nerve decompression at either the suprascapular or spinoglenoid notch.26 These authors identified symptom duration of less than 1 year, gradual onset of symptoms, nonworker's compensation cases, and male gender as predictors of good outcome (subjective shoulder values >70%).
Twenty patients (17 males, 3 females; average age 37.8 ± 14.7 years) have undergone suprascapular nerve release at the spinoglenoid notch using the described posterior approach at our institution at 5.5 ± 4.4 years follow-up. There were no complications or infections in any patient. All patients had complete resolution of posterior shoulder pain and exhibited restoration of external rotation strength to greater than 4 out of 5 on manual muscle testing. Patients returned to their preoperative sporting activities including weightlifting, tennis, baseball, swimming, and basketball as well as returned to work as overhead laborers without difficulty. Re-insufflation of the infraspinatus was not noted in 90% of patients at follow-up when atrophy was present.
Conclusion
Suprascapular nerve compression at the spinoglenoid notch occurs in overhead athletes and laborers. A thorough history and physical examination are paramount to ensure that correct diagnosis is not missed. The described technique has been successful in patients with or without EMG-proven compression, with or without visual atrophy in the infraspinatus fossa, and who have failed conservative treatment. This simple posterior technique allows the surgeon to address the pathology directly without involving any nonessential or essential muscular planes and allows the surgeon to address any intra-articular and extra-articular pathologies separately. The patient's pain profile often dramatically improves after surgery with resolution of symptoms by 6-9 weeks postoperatively. Restoration of the muscle mass of the infraspinatus is not always seen especially in patients with a protracted disease history; however, measurable improvements in external rotation strength are evidenced.
Disclaimers
Funding: No.
Conflicts of interest: The authors, their immediate families, and any research foundations with which they are affiliated have not received any financial payments or other benefits from any commercial entity related to the subject of this article.
Footnotes
Conflicts of interest: The authors, their immediate families, and any research foundations with which they are affiliated have not received any financial payments or other benefits from any commercial entity related to the subject of this article.
Institutional review board approval was not required for this technique article.
Supplementary data to this article can be found online at https://doi.org/10.1016/j.xrrt.2021.04.004.
Supplementary data
References
- 1.Abboud J.A., Silverberg D., Glaser D.L., Ramsey M.L., Williams G.R. Arthroscopy effectively treats ganglion cysts of the shoulder. Clin Orthop Relat Res. 2006;444:129–133. doi: 10.1097/01.blo.0000201155.44572.9b. [DOI] [PubMed] [Google Scholar]
- 2.Aiello I., Serra G., Traina G.C., Tugnoli V. Entrapment of the suprascapular nerve at the spinoglenoid notch. Ann Neurol. 1982;12:314–316. doi: 10.1002/ana.410120320. [DOI] [PubMed] [Google Scholar]
- 3.Bayramoglu A., Demiryurek D., Tuccar E., Erbil M., Aldur M.M., Tetik O., et al. Variations in anatomy at the suprascapular notch possibly causing suprascapular nerve entrapment: an anatomical study. Knee Surg Sports Traumatol Arthrosc. 2003;11:393–398. doi: 10.1007/s00167-003-0378-3. [DOI] [PubMed] [Google Scholar]
- 4.Bigliani L.U., Dalsey R.M., McCann P.D., April E.W. An anatomical study of the suprascapular nerve. Arthroscopy. 1990;6:301–305. doi: 10.1016/0749-8063(90)90060-q. [DOI] [PubMed] [Google Scholar]
- 5.Cummins C.A., Bowen M., Anderson K., Messer T. Suprascapular nerve entrapment at the spinoglenoid notch in a professional baseball pitcher. Am J Sports Med. 1999;27:810–812. doi: 10.1177/03635465990270062101. [DOI] [PubMed] [Google Scholar]
- 6.Cummins C.A., Messer T.M., Nuber G.W. Suprascapular nerve entrapment. J Bone Joint Surg Am. 2000;82:415–424. doi: 10.2106/00004623-200003000-00013. [DOI] [PubMed] [Google Scholar]
- 7.Ellenbecker T.S., Dines D.M., Renstrom P.A., Windler G.S. Visual observation of apparent infraspinatus muscle atrophy in male professional tennis players. Orthop J Sports Med. 2020;8 doi: 10.1177/2325967120958834. 2325967120958834. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Ferretti A., De Carli A., Fontana M. Injury of the suprascapular nerve at the spinoglenoid notch. The natural history of infraspinatus atrophy in volleyball players. Am J Sports Med. 1998;26:759–763. doi: 10.1177/03635465980260060401. [DOI] [PubMed] [Google Scholar]
- 9.Fritz R.C., Helms C.A., Steinbach L.S., Genant H.K. Suprascapular nerve entrapment: evaluation with MR imaging. Radiology. 1992;182:437–444. doi: 10.1148/radiology.182.2.1732962. [DOI] [PubMed] [Google Scholar]
- 10.Ghodadra N., Nho S.J., Verma N.N., Reiff S., Piasecki D.P., Provencher M.T., et al. Arthroscopic decompression of the suprascapular nerve at the spinoglenoid notch and suprascapular notch through the subacromial space. Arthroscopy. 2009;25:439–445. doi: 10.1016/j.arthro.2008.10.024. [DOI] [PubMed] [Google Scholar]
- 11.Khalili A.A. Neuromuscular electrodiagnostic studies in entrapment neuropathy of the suprascapular nerve. Orthop Rev. 1974;3:27–28. [Google Scholar]
- 12.Lafosse L., Piper K., Lanz U. Arthroscopic suprascapular nerve release: indications and technique. J Shoulder Elbow Surg. 2011;20:S9–S13. doi: 10.1016/j.jse.2010.12.003. [DOI] [PubMed] [Google Scholar]
- 13.Lajtai G., Pfirrmann C.W., Aitzetmuller G., Pirkl C., Gerber C., Jost B. The shoulders of professional beach volleyball players: high prevalence of infraspinatus muscle atrophy. Am J Sports Med. 2009;37:1375–1383. doi: 10.1177/0363546509333850. [DOI] [PubMed] [Google Scholar]
- 14.Lajtai G., Wieser K., Ofner M., Raimann G., Aitzetmuller G., Jost B. Electromyography and nerve conduction velocity for the evaluation of the infraspinatus muscle and the suprascapular nerve in professional beach volleyball players. Am J Sports Med. 2012;40:2303–2308. doi: 10.1177/0363546512455395. [DOI] [PubMed] [Google Scholar]
- 15.Mall N.A., Hammond J.E., Lenart B.A., Enriquez D.J., Twigg S.L., Nicholson G.P. Suprascapular nerve entrapment isolated to the spinoglenoid notch: surgical technique and results of open decompression. J Shoulder Elbow Surg. 2013;22:e1–e8. doi: 10.1016/j.jse.2013.03.009. [DOI] [PubMed] [Google Scholar]
- 16.Millett P.J., Barton R.S., Pacheco I.H., Gobezie R. Suprascapular nerve entrapment: technique for arthroscopic release. Tech Shoulder Elbow Surg. 2006;7:1–6. [Google Scholar]
- 17.Ming T.S., Min L.D., Andrew T.H. Unusual case of a volleyball athlete presenting with posterior shoulder pain and infraspinatus muscle wasting. J Orthop Case Rep. 2018;8:11–14. doi: 10.13107/jocr.2250-0685.1186. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Moore T.P., Fritts H.M., Quick D.C., Buss D.D. Suprascapular nerve entrapment caused by supraglenoid cyst compression. J Shoulder Elbow Surg. 1997;6:455–462. doi: 10.1016/s1058-2746(97)70053-3. [DOI] [PubMed] [Google Scholar]
- 19.Nolte P.C., Woolson T.E., Elrick B.P., Tross A.K., Horan M.P., Godin J.A., et al. Clinical outcomes of arthroscopic suprascapular nerve decompression for suprascapular neuropathy. Arthroscopy. 2021;37:499–507. doi: 10.1016/j.arthro.2020.10.020. [DOI] [PubMed] [Google Scholar]
- 20.Piatt B.E., Hawkins R.J., Fritz R.C., Ho C.P., Wolf E., Schickendantz M. Clinical evaluation and treatment of spinoglenoid notch ganglion cysts. J Shoulder Elbow Surg. 2002;11:600–604. doi: 10.1067/mse.2002.127094. [DOI] [PubMed] [Google Scholar]
- 21.Plancher K.D., Luke T.A., Peterson R.K., Yacoubian S.V. Posterior shoulder pain: a dynamic study of the spinoglenoid ligament and treatment with arthroscopic release of the scapular tunnel. Arthroscopy. 2007;23:991–998. doi: 10.1016/j.arthro.2007.03.098. [DOI] [PubMed] [Google Scholar]
- 22.Plancher K.D., Peterson R.K., Johnston J.C., Luke T.A. The spinoglenoid ligament. Anatomy, morphology, and histological findings. J Bone Joint Surg Am. 2005;87:361–365. doi: 10.2106/JBJS.C.01533. [DOI] [PubMed] [Google Scholar]
- 23.Plancher K.D., Petterson S.P. Posterior shoulder pain and arthroscopic decompression of the suprascapular nerve at the spinoglenoid notch. Oper Tech Sports Med. 2014;22:73–87. doi: 10.1053/j.otsm.2014.06.001. [DOI] [Google Scholar]
- 24.Post M., Mayer J. Suprascapular nerve entrapment. Diagnosis and treatment. Clin Orthop Relat Res. 1987:126–136. [PubMed] [Google Scholar]
- 25.Rengachary S.S., Burr D., Lucas S., Hassanein K.M., Mohn M.P., Matzke H. Suprascapular entrapment neuropathy: a clinical, anatomical, and comparative study. Part 2: anatomical study. Neurosurgery. 1979;5:447–451. doi: 10.1227/00006123-197910000-00007. [DOI] [PubMed] [Google Scholar]
- 26.Shah A.A., Butler R.B., Sung S.Y., Wells J.H., Higgins L.D., Warner J.J. Clinical outcomes of suprascapular nerve decompression. J Shoulder Elbow Surg. 2011;20:975–982. doi: 10.1016/j.jse.2010.10.032. [DOI] [PubMed] [Google Scholar]
- 27.Takagishi K., Saitoh A., Tonegawa M., Ikeda T., Itoman M. Isolated paralysis of the infraspinatus muscle. J Bone Joint Surg Br. 1994;76:584–587. [PubMed] [Google Scholar]
- 28.Thompson W.A., Kopell H.P. Peripheral entrapment neuropathies of the upper extremity. N Engl J Med. 1959;260:1261–1265. doi: 10.1056/NEJM195906182602503. [DOI] [PubMed] [Google Scholar]
- 29.Tubbs R.S., Smyth M.D., Salter G., Oakes W.J. Anomalous traversement of the suprascapular artery through the suprascapular notch: a possible mechanism for undiagnosed shoulder pain? Med Sci Monit. 2003;9:BR116–BR119. [PubMed] [Google Scholar]
- 30.Warner J.P., Krushell R.J., Masquelet A., Gerber C. Anatomy and relationships of the suprascapular nerve: anatomical constraints to mobilization of the supraspinatus and infraspinatus muscles in the management of massive rotator-cuff tears. J Bone Joint Surg Am. 1992;74:36–45. [PubMed] [Google Scholar]
- 31.Westerheide K.J., Dopirak R.M., Karzel R.P., Snyder S.J. Suprascapular nerve palsy secondary to spinoglenoid cysts: results of arthroscopic treatment. Arthroscopy. 2006;22:721–727. doi: 10.1016/j.arthro.2006.03.019. [DOI] [PubMed] [Google Scholar]
- 32.Yan J., Horiguchi M. The communicating branch of the 4th cervical nerve to the brachial plexus: the double constitution, anterior and posterior, of its fibers. Surg Radiol Anat. 2000;22:175–179. doi: 10.1007/s00276-000-0175-3. [DOI] [PubMed] [Google Scholar]
- 33.Young S.W., Dakic J., Stroia K., Nguyen M.L., Harris A.H., Safran M.R. High incidence of infraspinatus muscle atrophy in elite professional female tennis players. Am J Sports Med. 2015;43:1989–1993. doi: 10.1177/0363546515588177. [DOI] [PubMed] [Google Scholar]
- 34.Zehetgruber H., Noske H., Lang T., Wurnig C. Suprascapular nerve entrapment. A meta-analysis. Int Orthop. 2002;26:339–343. doi: 10.1007/s00264-002-0392-y. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.