

Abstract

Occupational injuries and illnesses are major risk factors for human health impacts worldwide, but they have not been consistently nor comprehensively considered in life cycle impact assessment (LCIA) methods. In this study, we quantified occupational health impacts as disability-adjusted life years (DALYs) for nonfatal injuries and illnesses in all US industries. We further applied an economic input–output model of the US economy to develop a new data set of characterization factors (CFs) that links direct and indirect occupational health impacts to product life cycle final demand. We found that the CF data set varies significantly by industry, ranging from 6.1 to 298 DALYs per billion dollars. About 20% of final demand in the US economic system contributes nearly 50% of the total impacts of occupational health, suggesting occupational health impacts are concentrated in a small portion of industries. To verify the feasibility of the CFs and demonstrate their importance, we included a case of an office chair. The occupational health impacts caused by nonfatal injuries and illnesses during the production of an office chair are of the same order of magnitude as those caused by chemical emissions across the chair’s life cycle, with 1.1 × 10–5 and 1.4 × 10–5 DALYs per chair, respectively. Results and data sets derived from this study support the integration of occupational health impacts with LCIA methods.
Keywords: work environment, life cycle impact assessment, disability-adjusted life years, economic input−output model
Short abstract
A system approach and new data set to characterize and evaluate occupational health impacts in work environments for improving the comprehensiveness of life cycle assessment methods.
Introduction
Life cycle assessment (LCA), a framework standardized by ISO 14040:2006,1 is commonly used to evaluate the potential life cycle environmental impacts of a product or service and is increasingly used to support environmental management decisions.2−4 Within LCA, life cycle impact assessment (LCIA) uses characterization factors to translate an inventory of physical inputs (e.g., freshwater used) and outputs (e.g., chemical emissions) into potential impact to human health, ecosystems, and natural resources. These characterization factors are generally developed by modeling underlying environmental mechanisms from cause (e.g., chemical emissions) to effects (e.g., carcinogenic effect on humans). From a human health perspective, LCIA generally focuses on environmental health impacts, i.e., impacts to the general population from environmental issues (e.g., chemical pollution, particulate matter formation, and climate change).5−7
The disability-adjusted life year (DALY) is often used in LCIA as an indicator of potential damage to human health. One DALY is equivalent to losing one year of healthy life due to premature death or living with a disease or disability.8 Weidema and Fantke estimated that a prominent LCIA method accounts for approximately 150 million DALYs (2012 reference year) attributed to environmental risks.9 As a comparison, the annual global burden attributed to behavioral, environmental, occupational, and metabolic risks is estimated to be more than 1 billion global DALYs. This indicates a substantial undercounting of human health impacts in LCA.9 For example, occupational risks, which account for approximately 70 million DALYs in 2019 (exceeding drug use, low physical activity, etc.),10 are not generally included in LCIA.
The minority of studies that include occupational health impacts in LCA used one of two methodological approaches. The first approach models the cause–effect chain for an occupational hazard, from worker exposure (e.g., chemical concentrations) to effects (e.g., dose–response relationships) and damage to workers (e.g., DALYs), similar to the approach generally used to assess environmental health impacts in LCIA.11−13 These studies tend to account for damage related to long-term exposures, for example, from indoor chronic chemical exposures14 to organic chemical exposures.15 The second approach estimates occupational health impacts based on incident data typically reported by workplaces and governments. These studies tend to quantify impact by summing relevant case statistics (e.g., fatalities, lost workdays)16−18 or by calculating damage (DALYs) using case statistics.19,20 This body of research has provided several case studies that include aspects of occupational health; however, it has not yet resulted in a standard approach or set of characterization factors for LCA.
We built on prior studies15,20,21 to develop a set of characterization factors for occupational health impacts from nonfatal injuries and illnesses. First, we extended the method developed by Scanlon et al.,20,21 which developed industry-level characterization factors for human health damage due to nonfatal injuries and illnesses per physical industry output (e.g., DALY per kg material produced) based on the number of incidents, age of workers at the time of the incident, the severity of the injury or illness, and duration of time lived with the outcome of the injury or illness. While that study provided characterization for industries included in a case study,20 we derived characterization factors for all US industries. In addition, our characterization factors instead relate damage to gross industry output and final demand, as was done by Kijko et al.,15,22 which derived hazard-based characterization factors in DALY/$ for long-term occupational exposure to organic chemicals based on measured concentration and labor hours for US manufacturing industries. This approach makes the characterization factors suitable for use in environmentally extended input–output (EEIO) models (e.g., USEEIO,23 CEDA24), which are commonly used in LCA. We then updated the LCA case study performed by Kijko et al.15 to include occupational health impacts from acute nonfatal injuries and illnesses.
Methods and Data Sources
Data Sources
We obtained incident data for nonfatal injuries and illnesses from 2014 to 2018 as reported to the US Bureau of Labor Statistics (BLS) via the Survey of Occupational Injuries and Illnesses (SOII).25 For each industry, we collected total number of cases and breakdown of cases by nature code, age stratum, and median days away from work. BLS codes industries according to the North American Industry Classification System (NAICS) and nature codes according to the BLS Occupational Injury and Illness Classification System (OIICS), which describe the principal physical characteristic of the injury or illness (e.g., sprain, fracture, burns).26 BLS estimates that more than 90% of reported cases are injuries from easily identifiable acute incidents, and the rest are illnesses from acute illnesses.27 While evidence suggests that SOII underestimates occupational injuries and illnesses (perhaps substantially),28 it is currently the most autoreactive data source for nonfatal occupational injuries and illnesses in the US.
To estimate DALYs, it was necessary to estimate the amount of healthy life lost from reported incidents. To do so, we obtained relevant data for health outcomes (sequelae) evaluated by World Health Organization (WHO) Global Burden of Disease (GBD) studies.29−32 This included the fraction of cases that result in short-term or lifelong health outcomes, severity weights for short-term and lifelong durations, and duration of time for short-term health outcomes (as available). GBD data and sources are listed in Supporting Information (SI) Tables S1–S3.
To convert annual DALYs into characterization factors, we obtained 2012 economic data from the US Environmentally Extended Input–Output (USEEIO) v2.0 model.23 This model was developed by the US Environmental Protection Agency (EPA) using economic data from the US Bureau of Economic Analysis (BEA).33 To derive industry-level characterization factors, we used the industry output vector from the USEEIO model.23 To use these characterization factors to estimate supply chain impacts, we used the direct requirement matrix (A) from the USEEIO model.23 Data and nomenclature of USEEIO used in this study are further explained in Tables S1 and S5, respectively.
Estimating Annual DALYs from Occupational Injuries and Illnesses
We used more recent data and a modified version of the method used by Scanlon et al.20,21 to estimate DALYs according to years lived with disability (YLD). YLD represents the diminished quality of life from living with a disability or disease, accounting for the severity of the disability or disease and duration of time lived with the disability or disease. One YLD is equal to one DALY. Four major modifications of our approach to estimating DALYs, as compared to Scanlon et al.’s approach, include (1) updating the severity weights with recent GBD reports34,35 and literature reference;32 (2) assuming the same severity weights for different age strata as most severity weights are the same across different age strata;21 (3) using the unisex life expectancy for each age strata, by taking the average life expectancy of males and females, as the difference of life expectancy between males and females for each age strata is not a critical determinant (only 3.2% age difference between males and females based on the WHO report);36 and (4) using three WHO age strata (age 15–44, 45–59, 60–80) for calculating the lifelong health impacts instead of five age strata (age <4, 5–14, 15–44, 45–59, 60–80) used in Scanlon et al.’s work,20 because there is no data for the age strata under the age of 14.
For each industry, BLS reported thirteen types of injuries and illnesses (represented as nature codes). To combine the BLS and GBD data, we first matched the BLS nature codes with the GBD health outcomes. For each of the injuries and illnesses, we assigned severity weights for short-term and lifelong health outcomes, and duration of time for short-term health outcomes, the fractions of cases that have short-term and lifelong health outcomes based on values published in GBD reports.32,34,35 Specific values used in this study with specific sources are provided in Tables S1–S4.
For each year (2014 to 2018) and each NAICS industry (n), we calculated annual YLD as the sum of YLD from short-term (ST) and lifelong (LL) health outcomes for all thirteen nature codes (c) (eq 1).
| 1 |
To calculate YLDn (eq 1), we estimated the occupational health damage for each industry from injuries and illnesses in nature code (c) with short-term health outcomes (YLDc,n,ST in eq 2) and lifelong health outcomes (YLDc,n,LL) in (eq 3).
| 2 |
| 3 |
where Ic,a,n represents different occupational injuries and illnesses (I) in nature code (c), age stratum (a), and industry (n) using the NAICS code (in cases). The BLS nonfatal injuries and illnesses data are categorized into eight age strata. The GBD health outcomes are categorized into five age strata. This made it necessary to overlay the BLS and GBD age strata and establish a single age strata classification (provided in Table S6) for our calculations.
The parameters fc,LL and fc,ST are the fraction of cases that result in short-term or lifelong health outcomes (unitless) for an injury or illness, regardless of industries. For each nature code, fc,ST and fc,LL sum to 1: fc,LL is 1 for nature codes with only lifelong impacts (e.g., amputations and tendonitis), fc,ST is 1 for nature codes with only short-term impacts (e.g., sprains, cuts, and bruises), and fc,ST and fc,LL are both nonzero for nature codes with both lifelong and short-term impacts (e.g., soreness, pain, and both heat and chemical burns).
The parameters Wc,ST and Wc,LL are the severity weights for short-term and lifelong (permanent) health outcomes, respectively, for nature codes (c) (unitless). Severity weights range from 0 to 1, where “0” indicates perfect health and “1” indicates death. Note that severity weights of nonfatal injuries or illnesses would never reach 1.
The parameter Dc,a,ST is the duration (in years) of health outcomes for injuries and illnesses in nature code (c) and age stratum (a) with short-term duration. For nature code with available duration data from GBD reports, we used those values directly. For nature codes with no available duration data from GBD, we used median days away from work reported in BLS as an estimate of the health outcome duration, which is a proxy method applied by Scanlon et al.24 Specific values of injury duration are provided in Tables S2 and S3. The parameter Dc,a,LL (in years) is the duration of health outcomes for injuries and illnesses in nature code (c) and age stratum (a) with lifelong health outcomes. We calculated Dc,a,LL by subtracting the average of the age strata from the unisex life expectancy according to the US Life Tables from National Vital Statistics Reports.37
Characterizing Characterization Factors (CFs) of Occupational Health Impacts
The nonfatal characterization factors or occupational risks are determined from the effective occurrence of occupational nonfatal illnesses and injuries and expressed as damage in DALYs per $ output or $ demand of the considered industry. Specifically, we calculated the direct impact factors (in DALYs/$output) and further calculated direct CFs (CFD, in DALYs/$demand) and supply chain CFs (CFSC, in DALYs/$demand). Direct impact factors are defined as occupational health impacts occurred in a specific industry corresponding to the total economic value of final goods and services (i.e., total output); direct CFs (CFD) are defined as the direct occupational health impacts occurred in a specific industry corresponding to the values of purchases made by final consumers (i.e., final demand). Supply chain CFs (CFSC) are defined as indirect occupational health impacts from supply chain on a specific industry. The sum of CFD and CFSC equals to CFtotal.
The equations to calculate these CFs are as follows (eqs 4–7). By convention, in the following equations, we represent vectors
using characters with an upper arrow, diagonal matrices with hat based
on a vector (e.g., ĝ), and represent matrices
with bold characters. An economic input–output (EIO) model
is needed to create CFD and CFSC from direct
impact factors. To this end, we utilized the YLDn calculated from eqs 1–3, which is  , standing as an n-dimensional
vector for n industries. We also constructed the
normalized conversion matrix (CONVnorm), interference
matrix (B), obtained direct requirement
matrix (A), and commodity production
vector (x⃗) from USEEIO v2.023 to first calculate CFtotal, and then separated
CFtotal into CFD and CFSC. The mathematical
formations of direct impact factors, CFD, CFSC, and CFtotal are provided in eqs 4–7; the detailed
calculations for obtaining eqs 4–7 are provided in the following
paragraphs.
, standing as an n-dimensional
vector for n industries. We also constructed the
normalized conversion matrix (CONVnorm), interference
matrix (B), obtained direct requirement
matrix (A), and commodity production
vector (x⃗) from USEEIO v2.023 to first calculate CFtotal, and then separated
CFtotal into CFD and CFSC. The mathematical
formations of direct impact factors, CFD, CFSC, and CFtotal are provided in eqs 4–7; the detailed
calculations for obtaining eqs 4–7 are provided in the following
paragraphs.
| 4 |
| 5 |
| 6 |
| 7 |
According to Leontief’s work,38 the commodity production vector x⃗ (in $ per functional unit) can be represented as a matrix constructed by (I – A)−1 and vector y⃗. x⃗ stands for the economic values (in $) for each industrial commodity of 397 industries needed for the production of a functional unit.
| 8 |
where (I – A)−1 is the Leontief inverse matrix and each column of the matrix represents the total production of different industries required to produce one dollar of that good, and the units of its rows are all in dollars ($/$). The vector y⃗ is the final demand vector for each good in the manufacturing stage in $ per good ($/functional unit).
The potential occupational health impacts of a product are not only from the production stage but also from across the supply chain represented by a broader economic system. To analyze product life cycle impacts covering all supply chains in an economic system, we constructed an interference matrix B (1/$) to connect CFD and IO analysis (i.e., indirect occupational health impacts). In this way, our equation becomes (eq 9)
| 9 |
where  represents the total CFs for occupational
health across all US industries.
represents the total CFs for occupational
health across all US industries.  represents
direct impacts across different
industries calculated in eq 1, which is an n-dimensional column vector where each element
corresponds to a YLD of an industry (YLDn).
represents
direct impacts across different
industries calculated in eq 1, which is an n-dimensional column vector where each element
corresponds to a YLD of an industry (YLDn).
Since the IO table uses the industry classification codes
(EIO
codes) from the US Bureau of Economic Analysis to classify different
industries and the NAICS codes were previously used to calculate  , the interference matrix B constructed in the study requires a transformation
matrix to convert the
, the interference matrix B constructed in the study requires a transformation
matrix to convert the  represented by the NAICS
codes into
represented by the NAICS
codes into  represented by EIO codes.
Due to the different
ways of dividing industries, multiple industries represented by 6-digit
NAICS codes need to be mapped into multiple industries represented
by EIO codes. In this study,
represented by EIO codes.
Due to the different
ways of dividing industries, multiple industries represented by 6-digit
NAICS codes need to be mapped into multiple industries represented
by EIO codes. In this study,  of corresponding industries
is also mapped
into multiple industries represented by EIO codes by the same mapping
in proportion to the total output of industries, and with this method,
a conversion matrix between NAICS (as rows, m NAICS
industries) and EIO (as columns, n BEA industries)
industries i and j can be constructed
consisting of convnormi,j elements of
a normalized conversion matrix CONVnorm that
is specified by the following equation (see Section S2.4 for details about this conversion)
of corresponding industries
is also mapped
into multiple industries represented by EIO codes by the same mapping
in proportion to the total output of industries, and with this method,
a conversion matrix between NAICS (as rows, m NAICS
industries) and EIO (as columns, n BEA industries)
industries i and j can be constructed
consisting of convnormi,j elements of
a normalized conversion matrix CONVnorm that
is specified by the following equation (see Section S2.4 for details about this conversion)
| 10 |
where convi,j is a binary parameter representing the mapping result between NAICS industry i and BEA industry j; if NAICS industry i belongs to BEA industry j, convi,j equals to 1, otherwise 0. This parameter comes directly from BEA data. gj is the total production in $ for the industry j in the BEA code. ∑k=1nconvi,k × gk represents the total production in $ for industry i in the NAICS code. It is worth mentioning that eq 10 indicates that one BEA industry might match multiple NAICS industries.
Afterward, we transformed the IO industry table into the IO commodity table based on a make matrix (V) from USEEIO v2.023 and included this transformation in the interference matrix B in the following equation (eq 11)
| 11 |
where  is
the inverse of the diagonal matrix of
the total output of the different industries in units of the inverse
of the dollar (1/$). V is a make matrix
with IO industries as rows and IO goods as columns, in which each
element vi,j represents
the total output of j commodity in i industry.
is
the inverse of the diagonal matrix of
the total output of the different industries in units of the inverse
of the dollar (1/$). V is a make matrix
with IO industries as rows and IO goods as columns, in which each
element vi,j represents
the total output of j commodity in i industry.  is
an inverse diagonal matrix based on
the total output of commodities in different industries (1/$).
is
an inverse diagonal matrix based on
the total output of commodities in different industries (1/$).
Case Study
To verify the feasibility of the developed CFs and demonstrate their importance, we expanded the case study performed by Kijko et al.15 to include our characterization factors to more fully compare occupational and environmental health impacts across a product’s life cycle. The functional unit (FU) is defined as the use of an office chair for 5 years. Data on material and energy consumptions are provided by Kijko et al.,15 and we used Monte Carlo simulation to quantify the uncertainty and provide 95% confidence intervals on results. The office chair for this case study is a fabric, wood, foam, and metal piece of furniture designed for breakrooms and informal meeting rooms. This study uses the human health impacts (e.g., chemical emissions affecting the general population) from the case study of Kijko et al.22 and compares the new occupational impacts with the previous findings to investigate the importance of including the occupational health impacts from a life cycle perspective. In our study, we assumed that US occupational injury rates apply throughout the supply chain, regardless of location.
Structural Path Analysis (SPA)
SPA is an important method to study the transfer influence and path relationship between different factors in the production supply chain and has been widely used in the analysis of IO models.39,40 We applied SPA to extract the individual supply chain pathways that contribute to the workplace occupational health impact for each production layer, using the Taylor expansion of the Leontief inverse matrix (see Section S2.5). By combining the input–output model with SPA, the main contributions along the supply chain paths leading to occupational impacts can be quantified.
Uncertainty and Sensitivity Analysis
We considered uncertainty in the duration and severity of each injury or illness. Specifically, the distribution of severity was collected from both James et al.32 and GBD reports.34,35 For the distribution of duration, no studies are reporting such information. To this end, we assumed uniform distributions for the duration of injuries by varying ±10% of mean values as lower and higher ends. The distributions of severity weights were assumed as log-normal distributions given that the data of severity weights from GBD are based on surveys.41 The specific type of distribution of severity and duration for the specific injury or illness is provided in Table S8. The standard deviation of log-normal distributions for each injury is calculated for short-term and lifelong injuries in the GBD report (Table S9). We conducted Monte Carlo simulations (1000 samples) for each of the 5 years of data and obtained 95% confidence intervals for each industry.
One major assumption in this study is the fraction of cases that result in short-term or lifelong health outcomes of certain injuries and illnesses (e.g., heat burns and pains) based on GBD reports29−32 and the study by Scanlon et al.21 that matched the BLS nature codes for the incident cases of nonfatal injuries and illnesses with GBD sequelae. Communicable illnesses were assigned as having short-term duration, noncommunicable illnesses were assigned as having lifelong duration, and injuries were assigned in accordance with GBD with some injuries having short-term durations, some having lifelong duration and several with a fraction assigned to each. After reviewing all of the fractions of cases that result in short-term or lifelong health outcomes used in Scanlon et al.’s study, we adjusted the fraction of “Soreness, pain” and “All other nature” and we have these noted in Table S4. Even detailed nature codes, such as those available in the US, provide ambiguous information for certain work-related injuries and illnesses. To evaluate whether the different fractions of short-term or lifelong duration assignments would impact the results (e.g., CFtotal ranking for different industries), we conducted a local sensitivity analysis by changing the fraction of lifelong health outcomes for each injury or illness by 10% (except for “Amputation” as we assumed its impact is always lifelong) and compared the results with the baseline. The values of fractions of short-term or lifelong cases are provided in Table S4.
Results and Discussion
Direct Impacts of Occupational Health Across Industries
To compare nonfatal injuries and illnesses among major industry groups, we investigated the reported cases and associated occupational health impacts (in DALYs/year) across the 404 US industries reported by the BEA. To facilitate the comparison of different industries, we aggregated 404 industries into 20 industry groups. Note that we took the average of the 5-year data with the number of cases and resulting DALYs for each year are provided in Section S3.3. Overall, the mix of nonfatal injuries and illnesses within each industry and the ranking across industries were relatively consistent. Our use of averages represents typical levels of workplace hazards (i.e., central tendency values). As shown in Figure 1, the total number of reported cases varies greatly among industry groups—this is mainly a function of the hazards inherent to the industries. For example, the industry group “Health care and social assistance” reports the largest number of cases (156,000 cases/year), while “Government” reports almost no cases. The main reason is that the workers in this industry group “Health care and social assistance” are at a high risk of injuries due to lifting and repetitive tasks, workplace aggression and violence, and exposure to infectious diseases and hazardous chemicals.42 The result also shows that the types of injuries represented are closely related to the characteristics of the industry itself. For example, the proportion of fractures and lacerations in “Manufacturing” is much higher than in other industries, while the service industry (e.g., retail trade, accommodation, food services) is characterized by sprains and strains. This is because “Manufacturing” has many physical hazards associated with work tasks such as cutting and handling, while the service industry has fewer types of hazards associated with work processes (e.g., office tasks), with a correspondingly lower risk of injuries and illnesses.43
Figure 1.

Cases of various injuries and risks of different injuries and illnesses in different industry groups. All 404 US industries are divided into 20 industry groups based on the US Bureau of Economic Analysis classification; injury risk (gray dots, bottom x-axis) is calculated as the ratio of the number of reported cases to the number of 1000 workers employed in that group. Note that not all industry groups can report this ratio due to missing data on the number of employees in some industry groups (e.g., Real estate and rental and lending).
Among the available data, the highest-risk industry group is “Transportation and warehousing” (gray dots in Figure 1). This high injury risk could be due to the frequent occurrence of traffic accidents and hazards in the process of moving goods in this industry group. There is no clear pattern between cases (bars) and their risks (gray dots). This variability is largely because injury risks are not only associated with cases but also dependent on the number of employees. Similar results are observed in the relationship between the number of cases and the health impacts (in DALYs/year) of occupational health, because the duration and severity of injuries and illnesses vary and so do their occupational health impacts. A related figure displaying the cases and health impacts can be found in Section S3.1 and Figure S2.
We further analyzed direct human health impacts of the entire US economy. Cell size in Figure 2 represents the values of the direct impacts coupled with demand (in DALYs/year) in a specific industry group or industry, while the color of each cell represents direct impact factors (DALYs/$output, darker colors indicating larger direct impacts). Figure 2 is a representation of this manuscript’s new data set of direct impact factors from all US industries. The full data set can be found in Section S5.1. The data show that “Accommodation and food services” and “Manufacturing” industry groups have the largest direct impacts in DALYs/year. This is because these industry groups have a high value of output (781 billion $ and 5765 billion $, respectively) and a large number of reported cases: close to 80,000 and 120,000, respectively.
Figure 2.
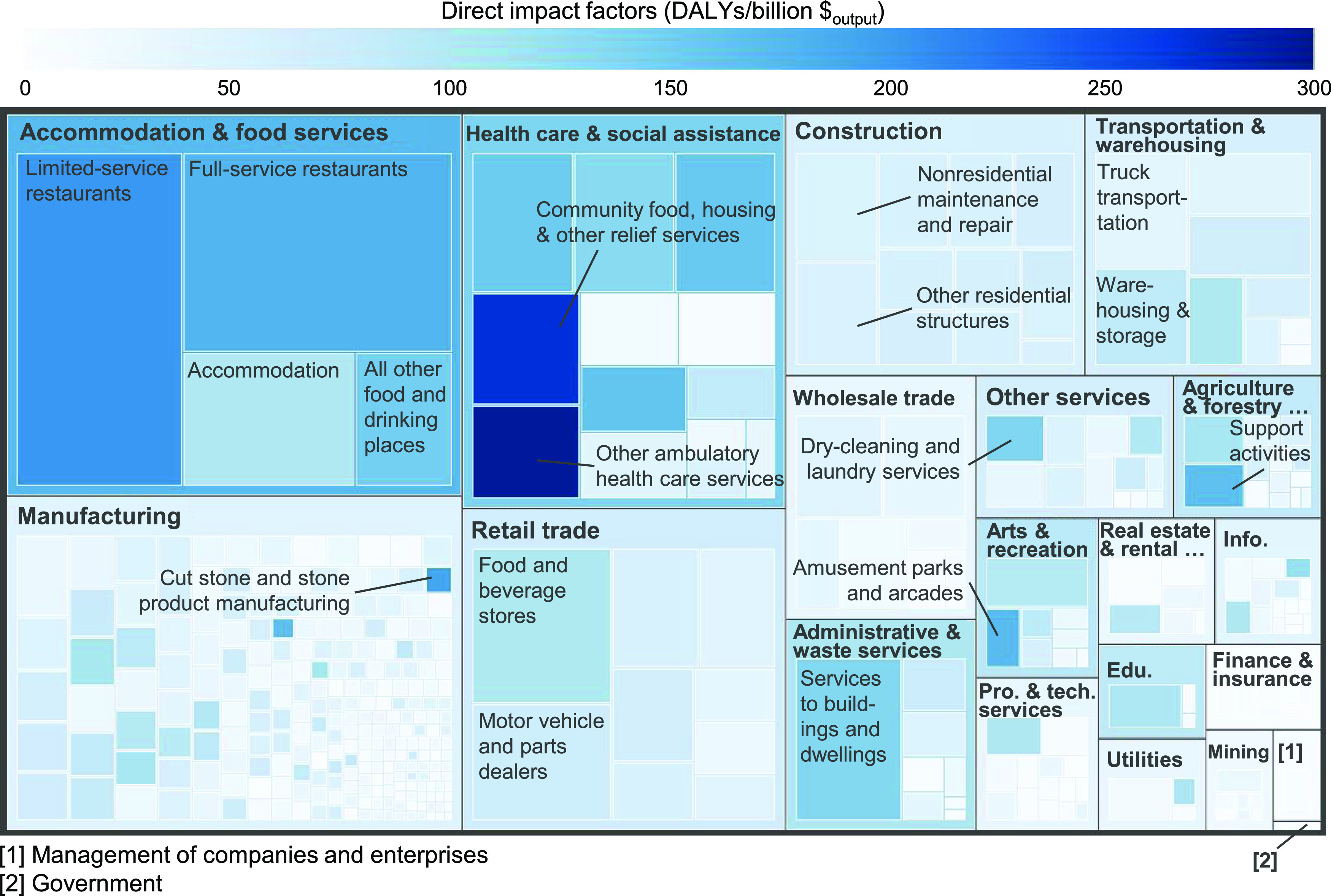
Direct impact factors in different industries. The size of the squares represent direct impacts for the industry; the shade of the color of the squares represents direct impact factors (the darker the color, the larger the direct impacts). Note that we used the total output as the denominator to calculate direct impact factors.
In terms of individual industries, “Other ambulatory health care services” and “Community food, housing, and other relief services” have the largest direct impact factors. Both have a high number of reported cases but low output because they are both social welfare industries. Tracing back from EIO codes to NAICS codes, we found that “Other ambulatory health care services” includes three industries (i.e., “Ambulance services”, “Blood and organ banks”, and “All other miscellaneous ambulatory health care services”). Their functions include engaging in ground or airborne patient transport and medical services, and engaging in the collection, storage, and distribution of blood and blood products and the storage and distribution of human organs and other ambulatory health care services, which are high-risk. This explanation can be supported by results from Dressner et al.44 who found out that private industry hospital workers have a higher incidence of injuries and illnesses than employees working in other industries by facing hazards related to lifting, moving, or otherwise physically interacting with patients.
The second largest direct impact factor is the “Community food, shelter, and other relief services, including reconstruction services” industry. The occupations in this industry have a relatively stable work environment but very high pressure of work.45 In addition, this industry also has a large number of reported cases (2249) and relatively low industrial output (42 billion $). Lawson and Masterson46 also confirmed that workers in these industries have a very high risk of getting hearing loss.
The direct impact factors and CFs developed in this study represent workplace safety standards, economic structures, and production technologies in the US. For other developed countries, such as Canada and the UK that have similar safety standards, economic structures, production technologies, and welfare,47 our CFs should be reasonable proxies; however, they may not be good proxies for developing countries. Our approach can be used to estimate similar quality CFs for countries (e.g., Japan,48 Australia49) that report injuries by injury type and industry, but the approach would result in lower resolution CFs for countries (e.g., European Union countries,50 Canada51) that report injuries by industry but without specific injury types. The approach would be challenging to apply in those countries with no or low-quality occupational injury reporting (e.g., Korea52). Additional information about the availability and characteristics of occupational injury databases in other countries is provided in Table S12.
Supply Chain Occupational Health Impacts in the US Economy
Figure 3 presents the direct CFs (CFD) and supply chain CFs (CFSC) in the work environment for all 397 US industries corresponding to the final demand of commodities provided in USEEIO.23 Note that CFD and CFSC refer to the CFs directly generated by the industry corresponding to the final demand of a commodity and the CFs across a supply chain (i.e., indirect), respectively. This figure further divides CFSC into producer and other industries: (1) CFSC outside producer industry—contributed by other industries that produce intermediate products for the industry—and (2) CFSC in producer industry—contributed by its own industry producing intermediate products for the industry itself. The height of each bar corresponds to the total CFs (i.e., CFtotal = CFD + CFSC) of the corresponding final demand of commodity. The area of each column is proportional to the total impacts (in DALYs/year) in industries starting with the highest CFtotal. The reason for using final demand instead of total output is that each industry has intermediate output used in other industries across supply chains (final demand = total output – intermediate output), which leads to double counting if using total output.19
Figure 3.

Characterization factors (CFs) for 397 US industries. Cumulative impact contribution represents the cumulative portion contributed by an industry to the total health impacts in US economic system. The width of the x-axis represents the final demand of an industry. The area is represented by the product of CFs in industries (y-axis) multiplied by the final demand (x-axis). Note that we used final demand (total output – intermediate output) as the denominator of the CFtotal to avoid double counting of intermediate output in supply chains. CFD = direct CFs; CFSC = supply chain CFs; and CFtotal = CFD + CFSC.
To investigate the distribution of occupational health impacts in the US industries, we note that the cumulative impact curve shows that about 20% of final demand in the US economy system contributes about 50% of the total impacts of occupational health. This finding suggests that occupational health impacts in US industries are concentrated in a small portion of industries. Among these industries, four of them have CFs exceeding 200 DALYs/billion $ (Section S3.2 and Figure S3 provide a more disaggregated view of the value of total impacts in all industries). Specifically, “Other ambulatory health care services” reaches 298 DALYs/billion $, followed by “Community food, housing, and other relief services, including reconstruction services” with 292.5 DALYs/billion $. They remain top 2 for either CFD or CFtotal, given that they have the relatively high health impacts (in DALYs/year) and small final demand (in $). This finding is also observed in Figure 2, which shows only the direct CFs (CFD in Figure 3). To track the contribution of CFtotal from supply chains, we applied structural path analysis (SPA) to find the contribution of the supply chain to the industries. Details about the SPA method are provided in Section S2.5. The major supply chain contributions of “Other ambulatory health care services” come from restaurants (5%) and housing (3%), while the major supply chain contributions of “Community food, housing, and other relief services, including reconstruction services” are recreation (4%) and education (3%).
Apart from the industries with the highest CFtotal in Figure 3, it is worth highlighting industries more commonly associated with the life cycle of products and processes, for example, petroleum refining and chemical manufacturing. In our analysis, we see the CFtotal of the “Petroleum refineries” is estimated as 16 DALYs/billion $. For the “Chemical manufacturing” industry group, it is a combination of 19 industries (e.g., Printing ink manufacturing, Biological product manufacturing). The CFtotal for the industry group ranges from 15 DALYs/billion $ to 53 DALYs/billion $. The industry with the highest CFtotal is “Printing ink manufacturing” (53 DALYs/billion $). The major contributions come from tendonitis and carpal tunnel syndrome, injuries resulting from long hours or ergonomically unsuitable work, or from exposures to a variety of hazardous and flammable chemicals and materials.53 We see that industries with the potential to release toxic chemicals are not as dangerous as expected. The CFtotal for both “Petroleum refineries” and “Chemical manufacturing” are much lower than that of the average of all industries (62 DALYs/billion $), which may indicate the success of safety protocols and risk management practices. However, these industries could have severe repercussions that considerably change the value of their CFs if an emergency event occurs during manufacturing or transportation, such as disaster accidentally releasing the toxic chemical (vinyl chloride) due to train derailment in Ohio, US.54
In general, the CFSC in the producer industry is much smaller than the other two components of the CFtotal. However, “Cheese production” has large CFSC in the producer industry with 63.9 DALYs/billion $. These impacts account for over 50% of the supply chain impacts, implying a large number of raw materials of the products are used as the products themselves. This is because cheese can be classified into natural and reconstituted, where natural cheeses are directly processed from dairy products and reconstituted cheeses are synthesized by melting several existing types of cheeses (e.g., ricotta cheese).55 The CFD of natural cheese is less than the CFSC, which is only 26.2 DALYs/billion $ because the cheese production process itself is relatively low risk. The high supply chain impacts, CFSC, mainly come from reconstituted cheeses. This might be because reconstituted cheeses with richer flavors and longer shelf life have become popular and production has increased significantly in recent years. And the contribution of dairy products to the reconstitution cheese comes not only from the process itself but also from its raw material (natural cheese). The SPA result shows that these contributions are mainly from the source of cheese production “Dairy farming and milk production” (38%), whose contribution exceeds the production process of the industry itself (16%).
This study also found that the range of CFD of occupational health in the work environment is from 2.8 × 10–3 to 283.1 DALY/billion $, while the range of CFSC is from 1.6 to 102.6 DALY/billion $ in US industries. The two CFs are of a similar order of magnitude, but the range of the supply chain CFs is smaller than that of the direct CFs. In addition, through uncertainty analysis, we found that coefficients of variation (CV) for CFtotal across industries range from 25 to 60%, which indicates that the CFs have high variability. This high variability mainly comes from the uncertain parameters (severity weights and durations), which suggests future efforts be invested in minimizing uncertainty from those parameters. For the sensitivity of the fraction of cases that result in short-term or lifelong health outcomes, we found that changing per percent of fraction of short-term and lifelong coefficient for different injuries or illnesses can result in up to 2% change on the CFs, as compared to baseline. More details can be found in Section S4.3. Among all injuries and illnesses, “Soreness, pain”; “Fractures”; and “All other nature” are the top three injuries most sensitive to results as their severity weight and cases are relatively high. However, the CFtotal ranking for different industries is similar in all scenarios. Therefore, this sensitivity analysis shows that the fraction of cases we used in this study that result in short-term or lifelong health outcomes would not change the major findings from this study.
Case Study
The case study illustrates how potential impacts of nonfatal injuries and illnesses are linked to the functional unit (FU) of a product life cycle and demonstrates the importance of occupational health impacts. To this end, this case study compares occupational health impacts with other potential sources of human health impacts:15 indoor emissions during the use stage, outdoor emissions during all life cycle processes, and chemical exposures in the work environment (Figure 4). The chemical exposures (worker chemical exposure) are estimates of long-term human health effects (e.g., cancers) based on hazards of the workplace that are unlikely to be reported in occupational health data. We assumed that US occupational injury rates apply throughout the supply chain for the office chair, regardless of location.
Figure 4.

Comparison of different types of human health impacts of an office chair due to its different life cycle processes, including impacts caused by chemical exposure to workers and users, toxic emissions to the general population, and fatal and nonfatal injuries and illnesses of workers. This study adds nonfatal injuries, split into lifelong and short-term (green), to previous work (gray).15 Error bars are labeled with 95% confidence intervals. FU = functional unit, i.e., the use of an office chair for 5 years in this case.
We used the Monte Carlo method to conduct the uncertainty analysis on the duration and severity of each lifelong and short-term injury and illness (see Section S4 for more details about parameters and distributions in the uncertainty analysis). Considering the median values of Monte Carlo simulations, Figure 4 shows that human health impacts from nonfatal injuries and illnesses were 9.6 × 10–6 DALYs/FU in the supply chain and 8.7 × 10–8 DALYs/FU in the production process, respectively. The worker chemical exposure (Kijko et al.15) is higher, 2.6 × 10–4 DALYs/FU. The sum of occupational health impacts from nonfatal injuries and illnesses is on the same magnitude of human health impacts due to general population exposure. Thus, both long-term health impacts due to worker chemical exposure and short-term injuries and illnesses are as large or larger than impacts in a typical LCA, underlining the need for occupational health impacts in LCA. Comparing health impacts of general population exposure (from Kijko et al.) with nonfatal injuries and illnesses, we found that nonfatal injuries and illnesses (1.8 × 10–5 DALYs) are of the same magnitude as general population exposure (1.4 × 10–5 DALYs). The latter is the only type of impact that a current, standard LCA of this case study would include. Through SPA, it is suggested that engineered wood products and foam products (except polystyrene) are the two main sources of occupational health impacts in the office chair life cycle. In addition, supply chain impacts are as important as the impacts directly related to the production itself.
Considering the split between long and short-term injuries, we found that the DALYs attributable to lifelong injuries and illnesses were much larger than those from short-term injuries and illnesses when tracing the contribution of lifelong and short-term injuries and illnesses to the final outcome separately (as shown in Figure 4). This finding is because the high severity and long duration of lifelong injuries and illnesses are not offset, in this example, by a higher frequency of short-term cases.
The findings from Kijko et al.15 have shown that the supply chain was responsible for the majority (97%) of the health impacts due to occupational chemical exposure. Among the supply chain, plastic manufacturing is the leading industry of occupational chemical exposure to workers for the use of an office chair’s life cycle. Through SPA in our study, we found that plastic (5%) is also one of the leading industries contributing to injuries and illnesses. Other leading industries include wood (30%) and foam (11%). Full SPA results are provided in Table S7. Through the case study, the results show that injuries caused by the hazards in the work environment should be an integral part of the calculation of the total impacts and should be considered to sum up with other categories to better characterize the total impacts of a product on human health. Overall, this case study evaluates occupational health impacts in work environments for improving the utility of LCIA methods. Our factors could be used to extend LCA-based processes and product design, such as Khan et al.,56 by efficiently including occupational illnesses and injuries.
Limitations and Outlook
The accurate recording of occupational injuries and illnesses is challenging, and this limitation cuts across any method that attempts to look at industry or economy-wide occupational impacts. For example, the BLS data used to account for the number, type, and duration of work-related nonfatal injuries and illnesses does not cover the entire US workforce, and fatal and nonfatal injuries can be underestimated by nearly 25% for a variety of reasons,57−59 including (1) not all industries are required to report injury data to the BLS, (2) employees conceal their industrial and commercial status for fear of dismissal, and (3) the underreporting due to the delay in time between when the work-related injuries or illnesses occur and when long-term effects are realized. Therefore, some authors19 contend that a correction factor of 1.5 should be given to adjust the underestimation of cases of nonfatal injuries and illnesses. We chose not to make these corrections for keeping the consistency of data from BLS and GBD reports. Beyond the reporting of injuries and illnesses, we recommended that future work includes an uncertainty analysis of information about the physical quantity of industry output and final demand from BEA.20
Our study develops a system approach and new data sets to characterize and evaluate occupational health impacts in work environments for improving the utility of life cycle assessment. Future occupational health studies can make advances in at least three areas. First, more rigorous analysis is needed for the fraction of cases that result in short-term or lifelong health outcomes of different nonfatal injuries and illnesses. To understand its impact on the estimate of health impacts to yield DALYs, further investigation on the fraction of cases that result in short-term or lifelong health outcomes should be made in the future. Second, occupational injury data reported to and compiled by BLS require further disaggregation. The classification (“All other nature”) that represents injuries and illnesses that are not otherwise classified into an existing classification is an important part of the occupational health impacts in the data used in the study. A more refined classification could more accurately quantify the occupational health impact of different industries. Third, the occupational health impacts should better represent the global supply chain for developing spatially explicit LCIA methods, given the fact that most supply chains are globalized and requires global databases representing multiple countries or regions.
Acknowledgments
S.L. and Z.H. received the support from the National Natural Science Foundation of China (72348004). P.F. was supported by the “(Safe and Efficient Chemistry by Design Safechem)” project funded by the Swedish Foundation for Strategic Environmental Research (grant no. DIA 2018/11). This work was also supported by the Global Life Cycle Impact Assessment Method (GLAM) group under the UN Environment Life Cycle Initiative. The authors appreciate Wesley W. Ingwersen for the help in applying the USEEIO model with NAICS data.
Data Availability Statement
All data sources supporting the results of this study can be found in the Supporting Information. Codes for calculating the characterization factors (CFs) are available on GitHub: https://github.com/ZhehanHuang/Occupational-health-calculation/
Supporting Information Available
The Supporting Information is available free of charge at https://pubs.acs.org/doi/10.1021/acs.est.3c00188.
Explanations on data source, allocation, nomenclature used, conversion from NAICE code to EIO code and structural path analysis; additional notes on direct and total impacts, and result variation between years; uncertainty and sensitivity analysis; terminologies; data sources; and developed CFs data sets (PDF)
The authors declare no competing financial interest.
Supplementary Material
References
- ISO . Environmental Management-Life Cycle Assessment-Principles and Framework, ISO 14040 international standard; International Organisation for Standardization, 2006.
- Lewandowska A.; Matuszak-Flejszman A.; Joachimiak K.; Ciroth A. Environmental life cycle assessment (LCA) as a tool for identification and assessment of environmental aspects in environmental management systems (EMS). Int. J. Life Cycle Assess. 2011, 16, 247–257. 10.1007/s11367-011-0252-3. [DOI] [Google Scholar]
- Li S.; Qin Y.; Subbiah J.; Dvorak B. Life cycle assessment of the U.S. beef processing through integrated hybrid approach. J. Cleaner Prod. 2020, 265, 121813 10.1016/j.jclepro.2020.121813. [DOI] [Google Scholar]
- Li S.; Zhilyaev S.; Gallagher D.; Subbiah J.; Dvorak B. Sustainability of safe foods: Joint environmental, economic and microbial load reduction assessment of antimicrobial systems in U.S. beef processing. Sci. Total Environ. 2019, 691, 252–262. 10.1016/j.scitotenv.2019.07.064. [DOI] [PubMed] [Google Scholar]
- Bare J.; Young D.; Qam S.; Hopton M.; Chief S.. Tool for the Reduction and Assessment of Chemical and other Environmental Impacts (TRACI); US Environmental Protection Agency: Washington, DC, USA, 2012.
- Huijbregts M. A. J.; Steinmann Z. J. N.; Elshout P. M. F.; Stam G.; Verones F.; Vieira M.; Zijp M.; Hollander A.; van Zelm R. ReCiPe2016: a harmonised life cycle impact assessment method at midpoint and endpoint level. Int. J. Life Cycle Assess. 2017, 22, 138–147. 10.1007/s11367-016-1246-y. [DOI] [Google Scholar]
- Jolliet O.; Margni M.; Charles R.; Humbert S.; Payet J.; Rebitzer G.; Rosenbaum R. IMPACT 2002+: A new life cycle impact assessment methodology. Int. J. Life Cycle Assess. 2003, 8, 324–330. 10.1007/BF02978505. [DOI] [Google Scholar]
- Murray C. J. L.; Lopez A. D.; World Health, O.; World, B.; Harvard School of Public, H. . The Global burden of disease: a comprehensive assessment of mortality and disability from diseases, injuries, and risk factors in 1990 and projected to 2020: summary; World Health Organization: Geneva, 1996.
- Weidema B. P.; Fantke P. Relating the Global Burden of Disease to Life Cycles. Procedia CIRP 2018, 69, 417–422. 10.1016/j.procir.2017.10.002. [DOI] [Google Scholar]
- Sharma R.; Abbasi-Kangevari M.; Abd-Rabu R.; Abidi H.; Abu-Gharbieh E.; Acuna J. M.; Adhikari S.; Advani S. M.; Afzal M. S.; Meybodi M. A.; Ahinkorah B. O.; Ahmad S.; Ahmadi A.; Ahmadi S.; Ahmed H.; Ahmed L. A.; Ahmed M. B.; Al Hamad H.; Alahdab F.; Alanezi F. M.; Alanzi T. M.; Alhalaiqa F. A. N.; Alimohamadi Y.; Alipour V.; Aljunid S. M.; Alkhayyat M.; Almustanyir S.; Al-Raddadi R. M.; Alvand S.; Alvis-Guzman N.; Amini S.; Ancuceanu R.; Anoushiravani A.; Anoushirvani A. A.; Ansari-Moghaddam A.; Arabloo J.; Aryannejad A.; Jafarabadi M. A.; Athari S. S.; Ausloos F.; Ausloos M.; Awedew A. F.; Awoke M. A.; Ayana T. M.; Azadnajafabad S.; Azami H.; Azangou-Khyavy M.; Jafari A. A.; Badiye A. D.; Bagherieh S.; Bahadory S.; Baig A. A.; Baker J. L.; Banach M.; Barrow A.; Berhie A. Y.; Besharat S.; Bhagat D. S.; Bhagavathula A. S.; Bhala N.; Bhattacharyya K.; Bhojaraja V. S.; Bibi S.; Bijani A.; Biondi A.; Bjørge T.; Bodicha B. B. A.; Braithwaite D.; Brenner H.; Calina D.; Cao C.; Cao Y.; Carreras G.; Carvalho F.; Cerin E.; Chakinala R. C.; Cho W. C. S.; Chu D.-T.; Conde J.; Costa V. M.; Cruz-Martins N.; Dadras O.; Dai X.; Dandona L.; Dandona R.; Danielewicz A.; Demeke F. M.; Demissie G. D.; Desai R.; Dhamnetiya D.; Dianatinasab M.; Diaz D.; Didehdar M.; Doaei S.; Doan L. P.; Dodangeh M.; Eghbalian F.; Ejeta D. D.; Ekholuenetale M.; Ekundayo T. C.; El Sayed I.; Elhadi M.; Enyew D. B.; Eyayu T.; Ezzeddini R.; Fakhradiyev I. R.; Farooque U.; Farrokhpour H.; Farzadfar F.; Fatehizadeh A.; Fattahi H.; Fattahi N.; Fereidoonnezhad M.; Fernandes E.; Fetensa G.; Filip I.; Fischer F.; Foroutan M.; Gaal P. A.; Gad M. M.; Gallus S.; Garg T.; Getachew T.; Ghamari S.-H.; Ghashghaee A.; Ghith N.; Gholamalizadeh M.; Navashenaq J. G.; Gizaw A. T.; Glasbey J. C.; Golechha M.; Goleij P.; Gonfa K. B.; Gorini G.; Guha A.; Gupta S.; Gupta V. B.; Gupta V. K.; Haddadi R.; Hafezi-Nejad N.; Haj-Mirzaian A.; Halwani R.; Haque S.; Hariri S.; Hasaballah A. I.; Hassanipour S.; Hay S. I.; Herteliu C.; Holla R.; Hosseini M.-S.; Hosseinzadeh M.; Hostiuc M.; Househ M.; Huang J.; Humayun A.; Iavicoli I.; Ilesanmi O. S.; Ilic I. M.; Ilic M. D.; Islami F.; Iwagami M.; Jahani M. A.; Jakovljevic M.; Javaheri T.; Jayawardena R.; Jebai R.; Jha R. P.; Joo T.; Joseph N.; Joukar F.; Jozwiak J. J.; Kabir A.; Kalhor R.; Kamath A.; Kapoor N.; Karaye I. M.; Karimi A.; Kauppila J. H.; Kazemi A.; Keykhaei M.; Khader Y. S.; Khajuria H.; Khalilov R.; Khanali J.; Khayamzadeh M.; Khodadost M.; Kim H.; Kim M. S.; Kisa A.; Kisa S.; Kolahi A.-A.; Koohestani H. R.; Kopec J. A.; Koteeswaran R.; Koyanagi A.; Krishnamoorthy Y.; Kumar G. A.; Kumar M.; Kumar V.; La Vecchia C.; Lami F. H.; Landires I.; Ledda C.; Lee S.-w.; Lee W.-C.; Lee Y. Y.; Leong E.; Li B.; Lim S. S.; Lobo S. W.; Loureiro J. A.; Lunevicius R.; Madadizadeh F.; Mahmoodpoor A.; Majeed A.; Malekpour M.-R.; Malekzadeh R.; Malik A. A.; Mansour-Ghanaei F.; Mantovani L. G.; Martorell M.; Masoudi S.; Mathur P.; Meena J. K.; Mehrabi Nasab E.; Mendoza W.; Mentis A.-F. A.; Mestrovic T.; Jonasson J.M.; Miazgowski B.; Miazgowski T.; Mijena G. F. W.; Mirmoeeni S.; Mirza-Aghazadeh-Attari M.; Mirzaei H.; Misra S.; Mohammad K. A.; Mohammadi E.; Mohammadi S.; Mohammadi S. M.; Mohammadian-Hafshejani A.; Mohammed S.; Mohammed T. A.; Moka N.; Mokdad A. H.; Mokhtari Z.; Molokhia M.; Momtazmanesh S.; Monasta L.; Moradi G.; Moradzadeh R.; Moraga P.; Morgado-da-Costa J.; Mubarik S.; Mulita F.; Naghavi M.; Naimzada M. D.; Nam H. S.; Natto Z. S.; Nayak B. P.; Nazari J.; Nazemalhosseini-Mojarad E.; Negoi I.; Nguyen C. T.; Nguyen S. H.; Noor N. M.; Noori M.; Noori S. M. A.; Nuñez-Samudio V.; Nzoputam C. I.; Oancea B.; Odukoya O. O.; Oguntade A. S.; Okati-Aliabad H.; Olagunju A. T.; Olagunju T. O.; Ong S.; Ostroff S. M.; Padron-Monedero A.; Pakzad R.; Pana A.; Pandey A.; Kan F. P.; Patel U. K.; Paudel U.; Pereira R. B.; Perumalsamy N.; Pestell R. G.; Piracha Z. Z.; Pollok R. C. G.; Pourshams A.; Pourtaheri N.; Prashant A.; Rabiee M.; Rabiee N.; Radfar A.; Rafiei S.; Rahman M.; Rahmani A. M.; Rahmanian V.; Rajai N.; Rajesh A.; Ramezani-Doroh V.; Ramezanzadeh K.; Ranabhat K.; Rashedi S.; Rashidi A.; Rashidi M.; Rashidi M.-M.; Rastegar M.; Rawaf D. L.; Rawaf S.; Rawassizadeh R.; Razeghinia M. S.; Renzaho A. M. N.; Rezaei N.; Rezaei N.; Rezaei S.; Rezaeian M.; Rezazadeh-Khadem S.; Roshandel G.; Saber-Ayad M. M.; Saberzadeh-Ardestani B.; Saddik B.; Sadeghi H.; Saeed U.; Sahebazzamani M.; Sahebkar A.; Farrokhi A. S.; Salimi A.; Salimzadeh H.; Samadi P.; Samaei M.; Samy A. M.; Sanabria J.; Santric-Milicevic M. M.; Saqib M. A. N.; Sarveazad A.; Sathian B.; Satpathy M.; Schneider I. J. C.; Šekerija M.; Sepanlou S. G.; Seylani A.; Sha F.; Shafiee S. M.; Shaghaghi Z.; Shahabi S.; Shaker E.; Sharifian M.; Sharifi-Rad J.; Sheikhbahaei S.; Shetty J. K.; Shirkoohi R.; Shobeiri P.; Malleshappa S. K. S.; Silva D. A. S.; Silva Julian G.; Singh A. D.; Singh J. A.; Siraj M. S.; Sivandzadeh G. R.; Skryabin V. Y.; Skryabina A. A.; Socea B.; Solmi M.; Soltani-Zangbar M. S.; Song S.; Szerencsés V.; Szócska M.; Tabarés-Seisdedos R.; Tabibian E.; Taheri M.; Abkenar Y. T.; Taherkhani A.; Talaat I. M.; Tan K.-K.; Tbakhi A.; Tesfaye B.; Tiyuri A.; Tollosa D. N.; Touvier M.; Tran B. X.; Tusa B. S.; Ullah I.; Ullah S.; Vacante M.; Tahbaz S. V.; Veroux M.; Vo B.; Vos T.; Wang C.; Westerman R.; Woldemariam M.; Jabbari S. H. Y.; Yang L.; Yazdanpanah F.; Yu C.; Yuce D.; Yunusa I.; Zadnik V.; Zahir M.; Zare I.; Zhang Z.-J.; Zoladl M. Global, regional, and national burden of colorectal cancer and its risk factors, 1990–2019: a systematic analysis for the Global Burden of Disease Study 2019. Lancet Gastroenterol. Hepatol. 2022, 7, 627–647. 10.1016/s2468-1253(22)00044-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Crettaz P.; Pennington D.; Rhomberg L.; Brand K.; Jolliet O. Assessing Human Health Response in Life Cycle Assessment Using ED10s and DALYs: Part 1—Cancer Effects. Risk Anal. 2002, 22, 931–946. 10.1111/1539-6924.00262. [DOI] [PubMed] [Google Scholar]
- McKone T. E.; Kyle A. D.; Jolliet O.; Olsen S. I.; Hauschild M. Dose-Response Modeling for Life Cycle Impact Assessment-Findings of the Portland Review Workshop. Int. J. Life Cycle Assess. 2006, 11, 137–140. 10.1065/lca2006.02.005. [DOI] [Google Scholar]
- Pennington D.; Crettaz P.; Tauxe A.; Rhomberg L.; Brand K.; Jolliet O. Assessing Human Health Response in Life Cycle Assessment Using ED10s and DALYs: Part 2—Noncancer Effects. Risk Anal. 2002, 22, 947–963. 10.1111/1539-6924.00263. [DOI] [PubMed] [Google Scholar]
- Hellweg S.; Demou E.; Bruzzi R.; Meijer A.; Rosenbaum R. K.; Huijbregts M. A. J.; McKone T. E. Integrating Human Indoor Air Pollutant Exposure within Life Cycle Impact Assessment. Environ. Sci. Technol. 2009, 43, 1670–1679. 10.1021/es8018176. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kijko G.; Jolliet O.; Margni M. Occupational Health Impacts Due to Exposure to Organic Chemicals over an Entire Product Life Cycle. Environ. Sci. Technol. 2016, 50, 13105–13114. 10.1021/acs.est.6b04434. [DOI] [PubMed] [Google Scholar]
- Hendrickson C. T.; Lave L. B.; Matthews H. S.. Environmental Life Cycle Assessment of Goods and Services: An Input-Output Approach (Occupational Safety Risks in an Input-Output Framework); Routledge, 2006; Chapter 15, p 274. [Google Scholar]
- Antonsson A.-B.; Carlsson H. The basis for a method to integrate work environment in life cycle assessments. J. Cleaner Prod. 1995, 3, 215–220. 10.1016/0959-6526(95)00083-6. [DOI] [Google Scholar]
- Li S.; Subbiah J.; Dvorak B. Environmental and occupational impacts from U.S. beef slaughtering are of same magnitude of beef foodborne illnesses on human health. Environ. Int. 2019, 129, 507–516. 10.1016/j.envint.2019.05.051. [DOI] [PubMed] [Google Scholar]
- Hofstetter P.; Norris G. A. Why and How Should We Assess Occupational Health Impacts in Integrated Product Policy?. Environ. Sci. Technol. 2003, 37, 2025–2035. 10.1021/es025838w. [DOI] [PubMed] [Google Scholar]
- Scanlon K. A.; Lloyd S. M.; Gray G. M.; Francis R. A.; LaPuma P. An Approach to Integrating Occupational Safety and Health into Life Cycle Assessment: Development and Application of Work Environment Characterization Factors. J. Ind. Ecol. 2015, 19, 27–37. 10.1111/jiec.12146. [DOI] [Google Scholar]
- Scanlon K. A.; Gray G. M.; Francis R. A.; Lloyd S. M.; LaPuma P. The work environment disability-adjusted life year for use with life cycle assessment: a methodological approach. Environ. Health 2013, 12, 21 10.1186/1476-069X-12-21. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kijko G.; Margni M.; Partovi-Nia V.; Doudrich G.; Jolliet O. Impact of Occupational Exposure to Chemicals in Life Cycle Assessment: A Novel Characterization Model Based on Measured Concentrations and Labor Hours. Environ. Sci. Technol. 2015, 49, 8741–8750. 10.1021/acs.est.5b00078. [DOI] [PubMed] [Google Scholar]
- Ingwersen W. W.; Li M.; Young B.; Vendries J.; Birney C. USEEIO v2.0, The US Environmentally-Extended Input-Output Model v2.0. Sci. Data 2022, 9, 194 10.1038/s41597-022-01293-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Suh S.Comprehensive Environmental Data Archive (CEDA) 3.0 User’s guide; Report, Leiden, The Netherlands, 2004.
- Survey of Occupational Injuries and Illnesses Data. https://www.bls.gov/iif/nonfatal-injuries-and-illnesses-tables.htm. (accessed November 08, 2022).
- BLS OSH Definitions. https://www.bls.gov/iif/definitions/occupational-safety-and-health-definitions.htm. (accessed October 30, 2022).
- Survey of Occupational Injuries and Illnesses: Overview. https://www.bls.gov/opub/hom/soii/. (accessed December 24, 2022).
- Rappin C. L.; Wuellner S. E.; Bonauto D. K. Employer reasons for failing to report eligible workers’ compensation claims in the BLS survey of occupational injuries and illnesses. Am. J. Ind. Med. 2016, 59, 343–356. 10.1002/ajim.22582. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Chen S.; Guo L.; Wang Z.; Mao W.; Ge Y.; Ying X.; Fang J.; Long Q.; Liu Q.; Xiang H.; Wu C.; Fu C.; Dong D.; Zhang J.; Sue J.; Tian L.; Wang L.; Zhou M.; Zhang M.; Qian M.; Liu W.; Jiang W.; Feng W.; Zeng X.; Ding X.; Lei X.; Tolhurst R.; Xu L.; Wang H.; Ziegeweid F.; Glenn S.; Ji J. S.; Story M.; Yamey G.; Tang S. Current situation and progress toward the 2030 health-related Sustainable Development Goals in China: A systematic analysis. PLoS Med. 2019, 16, e1002975 10.1371/journal.pmed.1002975. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Murray C. J.; Lopez A. D. Global and regional descriptive epidemiology of disability: incidence, prevalence, health expectancies and years lived with disability. Global Burden Dis. 1996, 1, 201–246. [Google Scholar]
- Salomon J. A.; Vos T.; Hogan D. R.; Gagnon M.; Naghavi M.; Mokdad A.; Begum N.; Shah R.; Karyana M.; Kosen S.; Farje M. R.; Moncada G.; Dutta A.; Sazawal S.; Dyer A.; Seiler J.; Aboyans V.; Baker L.; Baxter A.; Benjamin E. J.; Bhalla K.; Abdulhak A. B.; Blyth F.; Bourne R.; Braithwaite T.; Brooks P.; Brugha T. S.; Bryan-Hancock C.; Buchbinder R.; Burney P.; Calabria B.; Chen H.; Chugh S. S.; Cooley R.; Criqui M. H.; Cross M.; Dabhadkar K. C.; Dahodwala N.; Davis A.; Degenhardt L.; Díaz-Torné C.; Dorsey E. R.; Driscoll T.; Edmond K.; Elbaz A.; Ezzati M.; Feigin V.; Ferri C. P.; Flaxman A. D.; Flood L.; Fransen M.; Fuse K.; Gabbe B. J.; Gillum R. F.; Haagsma J.; Harrison J. E.; Havmoeller R.; Hay R. J.; Hel-Baqui A.; Hoek H. W.; Hoffman H.; Hogeland E.; Hoy D.; Jarvis D.; Jonas J. B.; Karthikeyan G.; Knowlton L. M.; Lathlean T.; Leasher J. L.; Lim S. S.; Lipshultz S. E.; Lopez A. D.; Lozano R.; Lyons R.; Malekzadeh R.; Marcenes W.; March L.; Margolis D. J.; McGill N.; McGrath J.; Mensah G. A.; Meyer A.-C.; Michaud C.; Moran A.; Mori R.; Murdoch M. E.; Naldi L.; Newton C. R.; Norman R.; Omer S. B.; Osborne R.; Pearce N.; Perez-Ruiz F.; Perico N.; Pesudovs K.; Phillips D.; Pourmalek F.; Prince M.; Rehm J. T.; Remuzzi G.; Richardson K.; Room R.; Saha S.; Sampson U.; Sanchez-Riera L.; Segui-Gomez M.; Shahraz S.; Shibuya K.; Singh D.; Sliwa K.; Smith E.; Soerjomataram I.; Steiner T.; Stolk W. A.; Stovner L. J.; Sudfeld C.; Taylor H. R.; Tleyjeh I. M.; van der Werf M. J.; Watson W. L.; Weatherall D. J.; Weintraub R.; Weisskopf M. G.; Whiteford H.; Wilkinson J. D.; Woolf A. D.; Zheng Z.-J.; Murray C. J. L. Common values in assessing health outcomes from disease and injury: disability weights measurement study for the Global Burden of Disease Study 2010. Lancet 2012, 380, 2129–2143. 10.1016/S0140-6736(12)61680-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Vos T.; Flaxman A. D.; Naghavi M.; Lozano R.; Michaud C.; Ezzati M.; Shibuya K.; Salomon J. A.; Abdalla S.; Aboyans V.; Abraham J.; Ackerman I.; Aggarwal R.; Ahn S. Y.; Ali M. K.; AlMazroa M. A.; Alvarado M.; Anderson H. R.; Anderson L. M.; Andrews K. G.; Atkinson C.; Baddour L. M.; Bahalim A. N.; Barker-Collo S.; Barrero L. H.; Bartels D. H.; Basáñez M.-G.; Baxter A.; Bell M. L.; Benjamin E. J.; Bennett D.; Bernabé E.; Bhalla K.; Bhandari B.; Bikbov B.; Abdulhak A. B.; Birbeck G.; Black J. A.; Blencowe H.; Blore J. D.; Blyth F.; Bolliger I.; Bonaventure A.; Boufous S.; Bourne R.; Boussinesq M.; Braithwaite T.; Brayne C.; Bridgett L.; Brooker S.; Brooks P.; Brugha T. S.; Bryan-Hancock C.; Bucello C.; Buchbinder R.; Buckle G.; Budke C. M.; Burch M.; Burney P.; Burstein R.; Calabria B.; Campbell B.; Canter C. E.; Carabin H.; Carapetis J.; Carmona L.; Cella C.; Charlson F.; Chen H.; Cheng A. T.-A.; Chou D.; Chugh S. S.; Coffeng L. E.; Colan S. D.; Colquhoun S.; Colson K. E.; Condon J.; Connor M. D.; Cooper L. T.; Corriere M.; Cortinovis M.; de Vaccaro K. C.; Couser W.; Cowie B. C.; Criqui M. H.; Cross M.; Dabhadkar K. C.; Dahiya M.; Dahodwala N.; Damsere-Derry J.; Danaei G.; Davis A.; De Leo D.; Degenhardt L.; Dellavalle R.; Delossantos A.; Denenberg J.; Derrett S.; Des Jarlais D. C.; Dharmaratne S. D.; Dherani M.; Diaz-Torne C.; Dolk H.; Dorsey E. R.; Driscoll T.; Duber H.; Ebel B.; Edmond K.; Elbaz A.; Ali S. E.; Erskine H.; Erwin P. J.; Espindola P.; Ewoigbokhan S. E.; Farzadfar F.; Feigin V.; Felson D. T.; Ferrari A.; Ferri C. P.; Fèvre E. M.; Finucane M. M.; Flaxman S.; Flood L.; Foreman K.; Forouzanfar M. H.; Fowkes F. G. R.; Franklin R.; Fransen M.; Freeman M. K.; Gabbe B. J.; Gabriel S. E.; Gakidou E.; Ganatra H. A.; Garcia B.; Gaspari F.; Gillum R. F.; Gmel G.; Gosselin R.; Grainger R.; Groeger J.; Guillemin F.; Gunnell D.; Gupta R.; Haagsma J.; Hagan H.; Halasa Y. A.; Hall W.; Haring D.; Haro J. M.; Harrison J. E.; Havmoeller R.; Hay R. J.; Higashi H.; Hill C.; Hoen B.; Hoffman H.; Hotez P. J.; Hoy D.; Huang J. J.; Ibeanusi S. E.; Jacobsen K. H.; James S. L.; Jarvis D.; Jasrasaria R.; Jayaraman S.; Johns N.; Jonas J. B.; Karthikeyan G.; Kassebaum N.; Kawakami N.; Keren A.; Khoo J.-P.; King C. H.; Knowlton L. M.; Kobusingye O.; Koranteng A.; Krishnamurthi R.; Lalloo R.; Laslett L. L.; Lathlean T.; Leasher J. L.; Lee Y. Y.; Leigh J.; Lim S. S.; Limb E.; Lin J. K.; Lipnick M.; Lipshultz S. E.; Liu W.; Loane M.; Ohno S. L.; Lyons R.; Ma J.; Mabweijano J.; MacIntyre M. F.; Malekzadeh R.; Mallinger L.; Manivannan S.; Marcenes W.; March L.; Margolis D. J.; Marks G. B.; Marks R.; Matsumori A.; Matzopoulos R.; Mayosi B. M.; McAnulty J. H.; McDermott M. M.; McGill N.; McGrath J.; Medina-Mora M. E.; Meltzer M.; Memish Z. A.; Mensah G. A.; Merriman T. R.; Meyer A.-C.; Miglioli V.; Miller M.; Miller T. R.; Mitchell P. B.; Mocumbi A. O.; Moffitt T. E.; Mokdad A. A.; Monasta L.; Montico M.; Moradi-Lakeh M.; Moran A.; Morawska L.; Mori R.; Murdoch M. E.; Mwaniki M. K.; Naidoo K.; Nair M. N.; Naldi L.; Narayan K. M. V.; Nelson P. K.; Nelson R. G.; Nevitt M. C.; Newton C. R.; Nolte S.; Norman P.; Norman R.; O’Donnell M.; O’Hanlon S.; Olives C.; Omer S. B.; Ortblad K.; Osborne R.; Ozgediz D.; Page A.; Pahari B.; Pandian J. D.; Rivero A. P.; Patten S. B.; Pearce N.; Padilla R. P.; Perez-Ruiz F.; Perico N.; Pesudovs K.; Phillips D.; Phillips M. R.; Pierce K.; Pion S.; Polanczyk G. V.; Polinder S.; Pope C. A.; Popova S.; Porrini E.; Pourmalek F.; Prince M.; Pullan R. L.; Ramaiah K. D.; Ranganathan D.; Razavi H.; Regan M.; Rehm J. T.; Rein D. B.; Remuzzi G.; Richardson K.; Rivara F. P.; Roberts T.; Robinson C.; De Leòn F. R.; Ronfani L.; Room R.; Rosenfeld L. C.; Rushton L.; Sacco R. L.; Saha S.; Sampson U.; Sanchez-Riera L.; Sanman E.; Schwebel D. C.; Scott J. G.; Segui-Gomez M.; Shahraz S.; Shepard D. S.; Shin H.; Shivakoti R.; Silberberg D.; Singh D.; Singh G. M.; Singh J. A.; Singleton J.; Sleet D. A.; Sliwa K.; Smith E.; Smith J. L.; Stapelberg N. J. C.; Steer A.; Steiner T.; Stolk W. A.; Stovner L. J.; Sudfeld C.; Syed S.; Tamburlini G.; Tavakkoli M.; Taylor H. R.; Taylor J. A.; Taylor W. J.; Thomas B.; Thomson W. M.; Thurston G. D.; Tleyjeh I. M.; Tonelli M.; Towbin J. A.; Truelsen T.; Tsilimbaris M. K.; Ubeda C.; Undurraga E. A.; van der Werf M. J.; van Os J.; Vavilala M. S.; Venketasubramanian N.; Wang M.; Wang W.; Watt K.; Weatherall D. J.; Weinstock M. A.; Weintraub R.; Weisskopf M. G.; Weissman M. M.; White R. A.; Whiteford H.; Wiersma S. T.; Wilkinson J. D.; Williams H. C.; Williams S. R. M.; Witt E.; Wolfe F.; Woolf A. D.; Wulf S.; Yeh P.-H.; Zaidi A. K. M.; Zheng Z.-J.; Zonies D.; Lopez A. D.; Murray C. J. L. Years lived with disability (YLDs) for 1160 sequelae of 289 diseases and injuries 1990–2010: a systematic analysis for the Global Burden of Disease Study 2010. Lancet 2012, 380, 2163–2196. 10.1016/S0140-6736(12)61729-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Input-Output Accounts Data. https://www.bea.gov/industry/input-output-accounts-data. (accessed September 10, 2022).
- Global Burden of Disease Study 2017 (GBD 2017) Data Resources. https://ghdx.healthdata.org/gbd-2017. (accessed December 12, 2022).
- Salomon J. A.; Haagsma J. A.; Davis A.; de Noordhout C. M.; Polinder S.; Havelaar A. H.; Cassini A.; Devleesschauwer B.; Kretzschmar M.; Speybroeck N.; Murray C. J. L.; Vos T. Disability weights for the Global Burden of Disease 2013 study. Lancet Global Health 2015, 3, e712–e723. 10.1016/S2214-109X(15)00069-8. [DOI] [PubMed] [Google Scholar]
- World Health Organization . World Health Statistics, 2020.
- National Center for Health Statistics . United States Life Tables, 2019; National Vital Statistics Reports, 2021. [PubMed]
- Leontief W.; Leontief W. W.. Input-Output Economics; Oxford University Press, 1986. [Google Scholar]
- Xie R.; Yuanyuan Z.; Liming C. Structural path analysis and its applications: literature review. Nat. Accounting Rev. 2020, 2, 83–94. 10.3934/NAR.2020005. [DOI] [Google Scholar]
- Sai L.; Yafei W.; Ming X.; Tianzhu Z. Environmental input-output analysis in industrial ecology. Acta Ecol. Sin. 2016, 36, 7217–7227. [Google Scholar]
- Qin Y.; Suh S. What distribution function do life cycle inventories follow?. Int. J. Life Cycle Assess. 2017, 22, 1138–1145. 10.1007/s11367-016-1224-4. [DOI] [Google Scholar]
- Health care and social assistance. https://www.safeworkaustralia.gov.au/safety-topic/industry-and-business/health-care-and-social-assistance. (accessed September 25, 2022).
- Nenonen S. Fatal workplace accidents in outsourced operations in the manufacturing industry. Saf. Sci. 2011, 49, 1394–1403. 10.1016/j.ssci.2011.06.004. [DOI] [Google Scholar]
- Dressner M. A.Hospital workers: an assessment of occupational injuries and illnesses. Monthly Labor Review, U.S. Bureau of Labor Statistics, June 2017; 10.21916/mlr.2017.17. [DOI] [Google Scholar]
- Hsiao C. J.; Cherry D. K.; Beatty P. C.; Rechtsteiner E. A.. National Ambulatory Medical Care Survey: 2007 Summary 27; National Health Statistics Reports, 2010. [PubMed]
- Lawson S. M.; Masterson E. A. Hearing Loss Among Health Care and Social Assistance Workers: A NIOSH Study. Hear. J. 2019, 72, 12 10.1097/01.HJ.0000552750.89735.6d. [DOI] [Google Scholar]
- Greer S. L. How Does Decentralisation Affect the Welfare State? Territorial Politics and the Welfare State in the UK and US. J. Soc. Policy 2010, 39, 181–201. 10.1017/S0047279409990407. [DOI] [Google Scholar]
- OSH Statistics in Japan. https://www.jisha.or.jp/english/statistics/index.html. (accessed March 11, 2023).
- Work-related injuries. https://www.safeworkaustralia.gov.au/data-and-research/work-related-injuries. (accessed March 11, 2023).
- Accidents at wor-k statistics. https://ec.europa.eu/eurostat/statistics-explained/index.php?title=Accidents_at_work_statistics#:%E2%88%BC:text=Standardised%20incidence%20rates%20only%20cover,employed%20(see%20Figure%204). (accessed March 11, 2023).
- Reports and publications: Occupational health and safety. https://www.canada.ca/en/employment-social-development/services/health-safety/reports.html. (accessed March 11, 2023).
- Occupational Injuries and Illnesses Statistics - as of February 2012. https://kosha.or.kr/english/news/whatsNew.do?mode=view&articleNo=55074&article.offset=0&articleLimit=10&srSearchVal=injuries&srSearchKey=article_title. (accessed March 11, 2023).
- Othman N.; Lerk L. L.; Chelliapan S.; Mohammad R.; Nasri N. S. Safety and Health Issues During Printing Ink Production Process. Int. J. Civil Eng. Technol. 2017, 8, 942–954. [Google Scholar]
- Revealed: the US is averaging one chemical accident every two days. https://www.theguardian.com/us-news/2023/feb/25/revealed-us-chemical-accidents-one-every-two-days-average. (accessed March 11, 2023).
- Vagnoni E.; Franca A.; Porqueddu C.; Duce P. Environmental profile of Sardinian sheep milk cheese supply chain: A comparison between two contrasting dairy systems. J. Cleaner Prod. 2017, 165, 1078–1089. 10.1016/j.jclepro.2017.07.115. [DOI] [Google Scholar]
- Khan F. I.; Natrajan B. R.; Revathi P. GreenPro: a new methodology for cleaner and greener process design. J. Loss Prev. Process Ind. 2001, 14, 307–328. 10.1016/S0950-4230(00)00047-4. [DOI] [Google Scholar]
- Azaroff L. S.; Levenstein C.; Wegman D. H. Occupational Injury and Illness Surveillance: Conceptual Filters Explain Underreporting. Am. J. Public Health 2002, 92, 1421–1429. 10.2105/AJPH.92.9.1421. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Leigh J. P.; Marcin J. P.; Miller T. R. An Estimate of the U.S. Government’s Undercount of Nonfatal Occupational Injuries. J. Occup. Environ. Med. 2004, 46, 10–18. 10.1097/01.jom.0000105909.66435.53. [DOI] [PubMed] [Google Scholar]
- Nestoriak N.; Pierce B. Comparing workers’ compensation claims with establishments’ responses to the SOII. Mon. Labor Rev. 2009, 132, 57. [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Data Availability Statement
All data sources supporting the results of this study can be found in the Supporting Information. Codes for calculating the characterization factors (CFs) are available on GitHub: https://github.com/ZhehanHuang/Occupational-health-calculation/