

Abstract
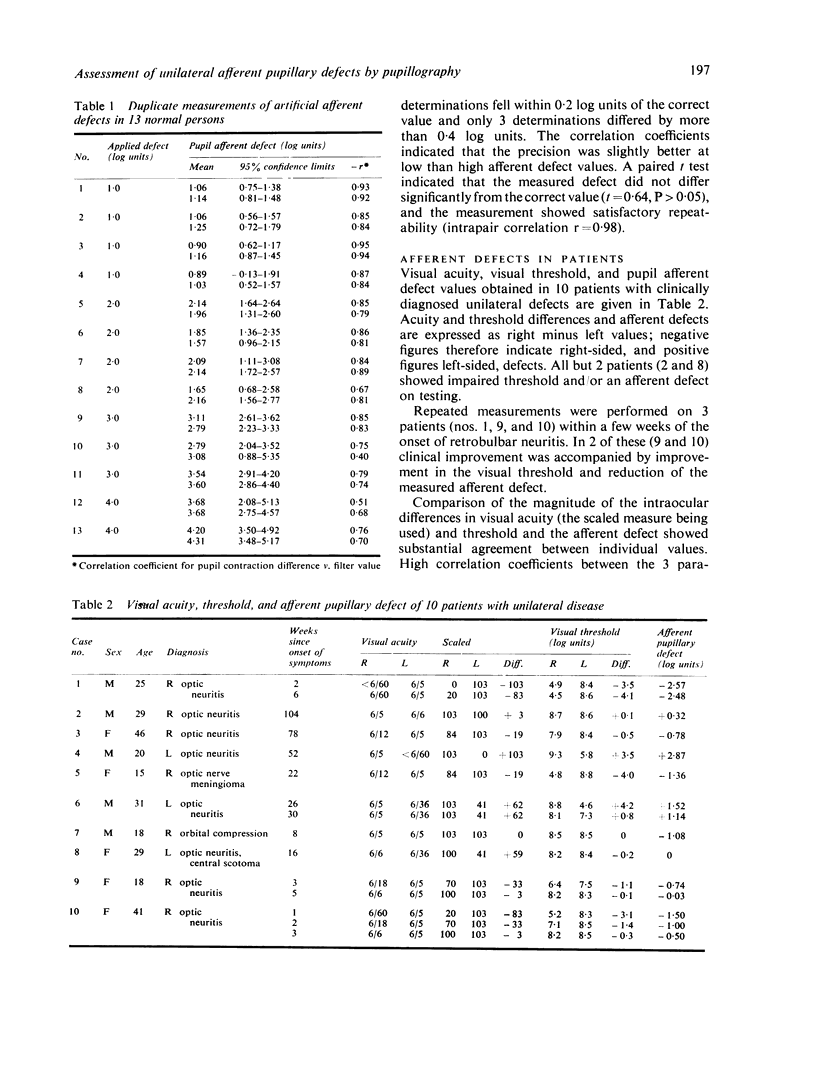
A pupillographic technique, an adaptation of the swinging light test, is described for the measurement of unilateral afferent pupillary defects. In normal persons it yielded accurate, reproducible estimates of the magnitude of artificial afferent defects made with neutral filters of 1 to 4 log units density. In 15 studies on 8 patients with unilateral optic neuritis and 2 with unilateral compressive lesions the measured afferent pupillary defects correlated closely with both visual acuity and visual threshold deficits. Measurement of the pupillary defect underestimated severe degrees of impairment revealed by visual threshold determination. Discrepancies between pupillary defect and visual acuity were observed in the 2 patients with compressive lesions and in 1 patient who had a central scotoma 4 months after an attack of optic neuritis.
Full text
PDF
Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Asselman P., Chadwick D. W., Marsden D. C. Visual evoked responses in the diagnosis and management of patients suspected of multiple sclerosis. Brain. 1975 Jun;98(2):261–282. doi: 10.1093/brain/98.2.261. [DOI] [PubMed] [Google Scholar]
- HARRIS H., KALMUS H. The measurement of taste sensitivity to phenylthiourea. Ann Eugen. 1949 Oct;15(1):24–31. doi: 10.1111/j.1469-1809.1949.tb02419.x. [DOI] [PubMed] [Google Scholar]
- Halliday A. M., McDonald W. I., Mushin J. Delayed visual evoked response in optic neuritis. Lancet. 1972 May 6;1(7758):982–985. doi: 10.1016/s0140-6736(72)91155-5. [DOI] [PubMed] [Google Scholar]
- Halliday A. M., McDonald W. I., Mushin J. Visual evoked response in diagnosis of multiple sclerosis. Br Med J. 1973 Dec 15;4(5893):661–664. doi: 10.1136/bmj.4.5893.661. [DOI] [PMC free article] [PubMed] [Google Scholar]
- LEVATIN P. Pupillary escape in disease of the retina or optic nerve. Arch Ophthalmol. 1959 Nov;62:768–779. doi: 10.1001/archopht.1959.04220050030005. [DOI] [PubMed] [Google Scholar]
- LOWENSTEIN O. Alternating contraction anisocoria; a pupillary syndrome of the anterior midbrain. AMA Arch Neurol Psychiatry. 1954 Dec;72(6):742–757. [PubMed] [Google Scholar]
- LOWENSTEIN O. Clinical pupillary symptoms in lesions of the optic nerve, optic chiasm, and optic tract. AMA Arch Ophthalmol. 1954 Sep;52(3):385–403. doi: 10.1001/archopht.1954.00920050387006. [DOI] [PubMed] [Google Scholar]
- Rushton D. Use of the Pulfrich pendulum for detecting abnormal delay in the visual pathway in multiple sclerosis. Brain. 1975 Jun;98(2):283–296. doi: 10.1093/brain/98.2.283. [DOI] [PubMed] [Google Scholar]
- Thompson H. S. Afferent pupillary defects. Pupillary findings associated with defects of the afferent arm of the pupillary light reflex arc. Am J Ophthalmol. 1966 Nov;62(5):860–873. [PubMed] [Google Scholar]