

Introduction
Virtual Reality (VR) is a technology that intends to create an artificial experience of immersion and presence via head-mounted display and head-tracking presentations of visual and auditory stimuli. During the past decades, there has been an increasing number of experimental studies and clinical trials examining VR as a potential non-pharmacological adjuvant in the medical context including treating both acute and chronic pain[19; 38]. Evidence from limited data-based studies have supported that VR shows promise for reducing inpatient pain and mitigating opioid usage[24; 33]. However, preliminary studies show that VR might reduce pain or facilitate physical therapy after acute traumatic injuries but are limited by lack of appropriate controls and/or small sample sizes[18; 26; 35], leaving VR efficacy and generalizability remaining uncertain. We are not aware of any study evaluating the use of VR for pain reduction in patients hospitalized with acute TBI, despite a relatively robust literature supporting VR-enhanced rehabilitation for motor and cognitive recovery after admissions for TBI.[3] Given that 2.5 million patients present to emergency departments yearly for TBI, and that headache pain from TBI is persistent and associated with chronic opioid use, it is surprising that patients with TBI have not been included in prior studies[34]. To address these gaps, we designed a randomized within-subjects study of VR for pain reduction in patients with acute traumatic injuries, including TBI. Moreover, we included two active controls to determine how immersive VR would effectively reduce pain in the acute traumatic injury population beyond placebo responses. We hypothesized that VR could reduce pain in the acute inpatient setting following traumatic injury.
Methods
Design
The study design and protocol have been previously published[11]. Briefly, we conducted a randomized, within-subjects, crossover clinical trial comparing the effects of an immersive VR environment against two control interventions. One control consisted of identical content to the immersive VR environment presented on a non-immersive, electronic tablet to control for immersion effects. The other control consisted of use of the VR headset without content to control for external sensory deprivation and placebo effects.
The study was conducted from October 2020 to January 2022 in a dedicated trauma hospital and was approved by the Local Institutional Review Board (Prot. #HP-00090603) and conducted in accordance with the Declaration of Helsinki for human research. All patients provided written and verbal informed consent to participate in the study. The study was also registered at ClinicalTrials.gov (NCT04356963). Data are available by request to the corresponding author.
Study Population
Patients 18 years of age and above with a Glasgow Coma Scale of 15, hospitalized for a traumatic injury, who reported at least moderate pain (numeric rating scale (NRS) for pain of at least three out of 10) within 24 hours of enrollment were enrolled in this study. We initially planned to only include TBIs, but we expanded the eligibility to all traumatic injuries due to slow enrollment. Moreover, patients were expected to remain hospitalized for at least 12 hours following enrollment to complete the study protocol. We excluded patients who could not consent for themselves, who had a medical history of seizure or a known intolerance to VR (usually reported as motion-sickness), who were pregnant, and who were non-English speaking.
Protocol
Patients engaged in three different 20 min sessions run by research coordinators and spaced a minimum of 4 hours apart, including 1) a commercially available, immersive VR environment, theBlu (WEVR, Inc, Venice, California, USA) delivered via Oculus Rift (Oculus VR, Irvine, California, USA) headset, 2) a non-immersive two-dimensional mimic delivered via a tablet computer, and 3) a VR control session delivered via a content-less Oculus Rift headset. We refer to those conditions as VR Blu, Tablet Blu, and VR Blank. theBlue scenario, which has been used in previous studies to induce relaxation and a sense of presence, simulates a dynamic encounter with a coral reef surrounded by aquatic wildlife to a soundtrack of calming music[21]. The three sessions were run by research coordinators and spaced a minimum of 4 hours apart. The intervention order was counterbalanced using a randomized sequence generator. During the consent process, participants were told that each session was aimed at reducing their pain as follows: “After the questionnaires, you will receive further instructions on how to use the virtual reality or tablet-based system. You will experience three sessions aimed at reducing your pain. One session will be a virtual reality-based immersive experience. Another session will be the same as the virtual reality-based experience but presented on a tablet computer instead of the virtual reality headset. In the third session, you will wear the virtual reality headset, but no content will be displayed”. We did not specifically ask participants what they did during their time in the VR Blank condition although they were encouraged to close their eyes and relax.
Immediately before and after each session, patients rated their clinical pain intensity via a NRS ranging from 0 (no pain) to 10 (worst possible pain)[20]. Headache pain severity specifically was also assessed by the same NRS, which has been previously validated in multiple headache syndromes [39; 42]. To assess anxiety, patients completed the six—item short-form of the Spielberger State-Trait Anxiety Inventory (STAI)[22] before and after each condition.
Potential side-effects of VR were measured before and after each session, including neck pain, nausea, dizziness, and light sensitivity according to a NRS ranging from 0 (no symptom) to 10 (worst possible symptom)[27; 41]. Before and immediately after each session, we also collected vital sign measurements (blood pressure and heart rate), and pupillary maximum constriction velocity. Additionally, the electrocardiogram (ECG) was recorded 15 minutes before the beginning of each session as baseline and was continuously recorded during the 20 minutes intervention to assess heart rate variabilities relevant to VR related effects. At the conclusion of all sessions, patients completed a questionnaire regarding their level of engagement and perceptions of effectiveness of each condition to assess patients-oriented outcomes.
The primary treatment team was blinded to the session order and prescribed pain therapeutics independent from the research team. We recorded opioid dosage and administration times.
Outcomes
The primary outcome was reduction in overall pain severity for VR sessions compared with controls, as measured by the change in the pain NRS rating before vs. after each interventional session. Secondary outcomes included changes in headache pain, anxiety, patient-reported engagement and perceived effectiveness, as well as autonomic measurements (i.e., pupillary maximum constriction velocity and heart rate variability).
We evaluated opioid consumption as an exploratory outcome due to the complex interactions of patient-, provider-, and systems-factors that drive it[13; 23]. We monitored the medication administration record for all opioid usage that we converted to morphine milligram equivalents (MME). Within our trauma units, when opioids are prescribed by convention they are usually prescribed as needed every four hours. We compared the pre- vs. post-intervention doses of opioids received in morphine equivalents among conditions.
Autonomic Measures
Systolic blood pressure, diastolic blood pressure, and heart rate were assessed before and after each condition by using an automated blood pressure cuff leveled at the right atrium and telemetry, respectively.
Heart rate variability was assessed using an ECG recording from standard five lead telemetry. Normally distributed R-R intervals provided evidence of good quality ECG signals and we used the Z-test to remove segments of low quality (R-R interval outliers). Heart rate variability was obtained following standard measures[1]. We examined both time-domain indices including normal-to-normal (NN) means and heart rate, as well as frequency domain indices low frequency (LF) power and high frequency (HF) power. We split the ECG waveforms of each experiment condition into pre-session and intra-session periods. A pre-session period was defined as 25 minutes of recording before the start of an experimental condition, while an intra-session period was the period of the experimental condition from the start time to the end time (about 20 minutes). Afterwards, a rolling 5-minute window was applied to both pre-session and intra-session periods to generate heart rate variability indices, resulting in 4 epochs for each condition. To ensure adequate time for any physiological effects to be realized, we chose the last three pre-session and intrasession epochs for analysis. Time domain heart rate variability indices, NN means and heart rate, as well as frequency domain indices LF and HF power were extracted using the PhysioNet Cardiovascular Signal Toolbox. Decreasing heart-rate variability indices are associated with sympathetic nervous system activity, while increasing indices are associated with parasympathetic nervous system activity.
A purer measure of parasympathetic nervous system activity was also obtained by collecting the maximum constriction velocity as measured by the NPi-200 Pupillometer (NeurOptics, Irvine, CA). The maximum constriction velocity for each pupil is directly reported by the pupillometer. We measured the right eye before and after each condition given that both eyes constrict in an equal manner [4]. The difference scores of maximum constriction velocity values before and after each condition were calculated to compare constriction velocity changes among the three conditions. Faster maximum constriction velocities represent increased parasympathetic nervous system activity, as pupillary constriction occurs independent from sympathetic innervation [15].
Side-Effects
We accounted for the safety and feasibility of immersive VR for patients with acute traumatic injury including TBI by assessing for changes in neck pain, nausea, dizziness, light sensitivity, and clinical seizures and comparing those changes with the baseline and among the three conditions.
Engagement and Perceived Effectiveness
Immediately after each session patients completed the Brockmeyer Gaming Engagement Questionnaire, a validated measure of engagement in video game playing that encompasses absorption, flow, presence, and immersion.[5] Patients were instructed to complete the questionnaire based on their engagement in the session that they just completed. At the end of the study, patients rated how effective each condition was in reducing pain on a Likert scale of 0 (not at all effective) to 5 (very effective).
Statistical Analyses
Power calculation and sample size.
We enrolled 60 patients, projecting a study dropout of 30%, leaving us with 42 patients to give us an 80% likelihood to detect a treatment difference at a one-sided 0.05 significance level in our primary analysis of pain reduction[9; 10]. Prior work suggests that a 33% pain intensity difference or a 3-point difference on a 0–10 pain NRS is an appropriate surrogate for a patient-determined clinically important response [36].
Missing data
Among the 60 enrolled patients, one did not complete any of the three experimental conditions, resulting in 59 patients entering the final analysis. The remaining 11 patients who did not finish the whole study but completed at least one experimental condition were included in the analysis (Figure 1). The missing data for the primary outcome (pain rating changes) for the three experimental conditions ranged between 6.7% (for VR Blu and VR blank) to 8.5% (for Tablet Blu) with the missing data pattern randomly distributed (Little’s MCAR test: chi-square=4.72, p=0.581). To retain most of the study patients in the analysis, we adopted the linear mixed-effects model (LMM) analysis given its superiority in handling missing values.
Figure 1: Enrollment flow chart.
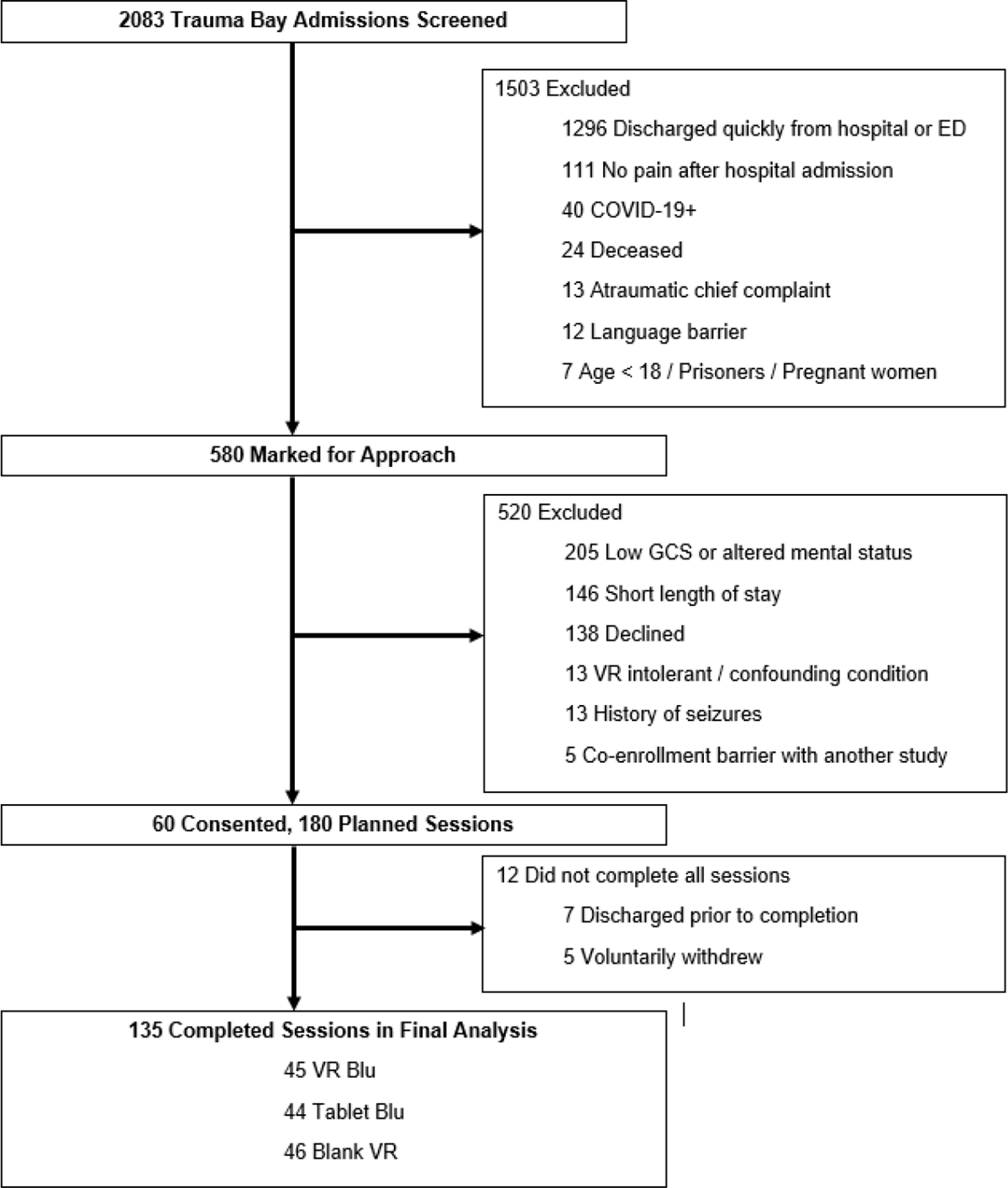
After screening 2083 patients admitted to our trauma resuscitation unit, we enrolled 60 patients in the study.
Primary and Secondary Analyses
We used descriptive statistics to characterize study patients In terms of the analyses related to primary and secondary outcomes, we used LMMs to analyze the differences between the ratings over time to allow for missing data expected in a trauma population[28]. For each LMM, we treated the three treatment conditions (VR Blu vs. Tablet Blu vs. VR Blank) as the fixed factors to examine if the three conditions would differ in changes in pain intensity, headache, anxiety, objective autonomic measurement of body response (I.e., blood pressure, heart rate, heart rate variability, and pupil maximum constriction velocity), as well as potential side effects. We controlled analyses for experimental sequence, demographic variables such as age, sex, race, clinical variables baseline pain severity, and injury severity score. Pair-wise comparisons were conducted wherever a main effect of the intervention conditions was found.
In terms of heart rate variability, LMMs were built to determine the main effect of the three experimental conditions (VR Blu vs. Tablet Blu vs. VR Blank) on the heart rate variability indices (NN mean, heartbeats rate, LF and HF power). For each LMM, experimental conditions were set as the fixed factor. The three epochs of each condition were set as repeated measures. We also controlled for baseline level of heart rate variability (i.e., pre-session recordings), age, sex, race, and experimental sequence in the LMMs.
Finally, we compared opioid consumptions among the three treatment conditions within the VR Blu responders and non-responders using separate LMMs, respectively.
Pair-wise comparisons were applied to a significance of one-tailed p-value of .05 because we hypothesized VR Blu condition would result in greater improvement in clinical outcomes as compared to the Table Blu and VR Blank conditions based on our previous results [7]. Given the proof-of-concept nature of the study, Least Significance Difference (LSD) adjustment was applied for multiple comparisons. SPSS version 27 (IBM) was used to perform all the analyses.
Results
We enrolled sixty patients. Seven patients were discharged from the hospital prior to completion of the study and five patients withdrew from the study due to disinterest without specific complaint, leaving 48 patients that completed the entire protocol (Figure 1). The patients were mostly men (42/60, 70%) with a median age of 53 years (IQR 38–63). One third (20/60) of the patients had TBIs (Table 1). The median baseline pain score was 5.0 (IQR 4.0–7.0).
Table 1:
Patient Characteristics
| Characteristic | N = 60 | |
|---|---|---|
| Age, median (IQR) | 53 (38–63) | |
| Female | 18 (30) | |
| Race | ||
| White | 37 (61.6) | |
| Black | 19 (31.6) | |
| Asian | 2 (3.3) | |
| Native Hawaiian / Pacific Islander | 1 (1.6) | |
| Other | 1 (1.6) | |
| Injury (AIS > 0) | ||
| Head | 29 (48) | |
| Head w/ Traumatic Brain Injury | 20 (33) | |
| Face | 20 (33) | |
| Neck | 8 (13) | |
| Thoracic | 26 (43) | |
| Abdominal | 29 (48) | |
| Spine | 15 (25) | |
| Upper Extremity | 28 (42) | |
| Lower Extremity | 35 (58) | |
| Traumatic Brain Injury | ||
| Intracranial hemorrhage | 13 (65) | |
| Subdural hematoma | 10 (50) | |
| Subarachnoid hemorrhage | 8 (40) | |
| Epidural hematoma | 1 (5) | |
| Cause of Injury | ||
| Fall | 23 (38) | |
| Motor Vehicle Collision | 17 (28) | |
| Gunshot Wound | 7 (12) | |
| Stabbing | 5 (8) | |
| Motorcycle Collision | 4 (7) | |
| Pedestrian Struck | 3 (5) | |
| Assault | 1 (2) | |
| Past Medical History | ||
| Depression | 18 (30) | |
| Anxiety | 16 (27) | |
| Chronic Pain | 13 (22) | |
| Alcohol Abuse | 13 (22) | |
| Positive Toxicology Screen | 32 (53) | |
| Health Insurance | ||
| Private | 39 (66) | |
| Medicare | 16 (26) | |
| Medicaid | 5 (8) | |
| Length of Stay, median (IQR) days | 7 (4–10) | |
Abbreviations: AIS, Abbreviated Injury Scale
Data are presented as number (%) unless otherwise specified.
Pain Reduction
Controlling for the experimental sequence, age, sex, race, baseline pain severity, and injury severity, there was a significant main effect of the experimental conditions on pain intensity (F2,75.43 = 3.32, p = .042) (Figure 2). Pair-wise comparisons applying LSD adjustment indicated that pain reduction by VR Blu was significantly greater as compared to Tablet Blu (−0.92 vs. −0.16, one-tailed p = .043) but pain reduction by VR Blu was not different as compared to VR Blank (one-tailed p = .243). Moreover, pain reductions induced by VR Blank (mean = −1.24, sem = 0.33) were also significantly greater than Tablet Blu (mean = −0.16, sem = 0.29, LSD adjusted one-tailed p = .008).
Figure 2: Reduction in pain severity by intervention.
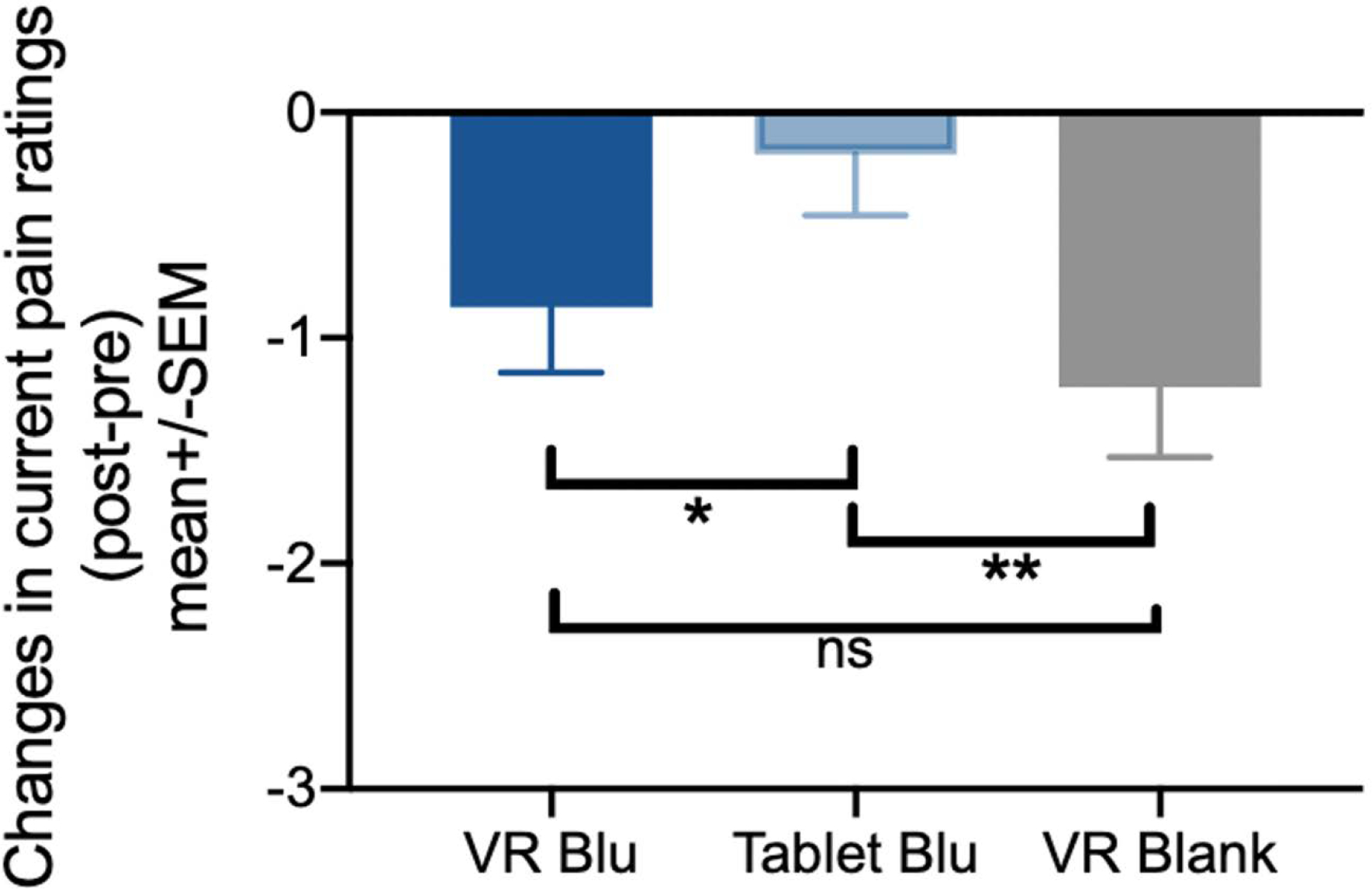
Controlling for the experimental sequence, age, sex, race, baseline pain severity, as well as the level of injury severity, there was a significant main effect of the experimental conditions on the current pain intensity changes (F1,75.43=3.32, p=.042). That is, pain reductions induced by Tablet Blu condition (mean=−0.16, sem=0.29) were significantly lower than VR Blank condition (mean=−1.24, sem=0.33, one-tailed p=.008) and significantly lower than VR Blu condition (mean=−0.92, sem=0.33, one-tailed p=.043).
VR Blu induced analgesic effects were then calculated as the continuous delta-scores of post-VR minus pre-VR pain intensity ratings. Bivariate correlations indicated that no significant relationship between VR Blu induced analgesic effects and baseline pain intensity (Pearson r = −.13, one-tailed p = .199) as well as non-significant relationship between VR Blu induced analgesia and trauma injury severity (Pearson r = .119, one-tailed p = .205).
Age, sex and race did not influence the results related to pain reductions induced by VR Blu condition as revealed by non-significant multivariate regression controlling for baseline pain and injury severity (age: beta = −.23, one-tailed p = .111; sex: beta = −.09, one-tailed p = .299; White vs. non-White race: beta = −.53, one-tailed p = .300).
Headache Pain Reduction
Among patients with TBI, VR Blu did not significantly reduce headache pain more than the other conditions (F1,18.21=.051, p = .951). Among patients without TBI, VR Blu induced greater reductions in headache pain compared to VR Blank (mean difference = .717, 95% CI 0.089–1.344, one-tailed p = .013) but non-significant headache reduction compared to Tablet Blu (mean difference = .133, 95% CI −0.787–1.054, one-tailed p = .386).
Opioid Use
The main effect of the three conditions on opioid consumption was not significant (F1,73.89 = 0.13, p = .876). Fourteen patients (29%) had pain reduced by at least three points on the 11-point NRS after VR Blu, defining them as VR Blu responders. Subgroup analyses within VR Blu responders and non-responders indicated a marginal significant main effect of the three conditions within the VR Blu responders (F2,8.00=3.88, p = .066). That is, VR Blu responders had significant reductions in opioid intake following VR Blu compared to Tablet Blu (LSD adjusted one-tailed p = .012) but not after VR Blank condition (one-tailed p = .063) (Figure 3). No such effects were observed within the VR Blu non-responders (F2,55.46=1.58, p = .218).
Figure 3: Changes in opioid intake among VR Blu responders by intervention.
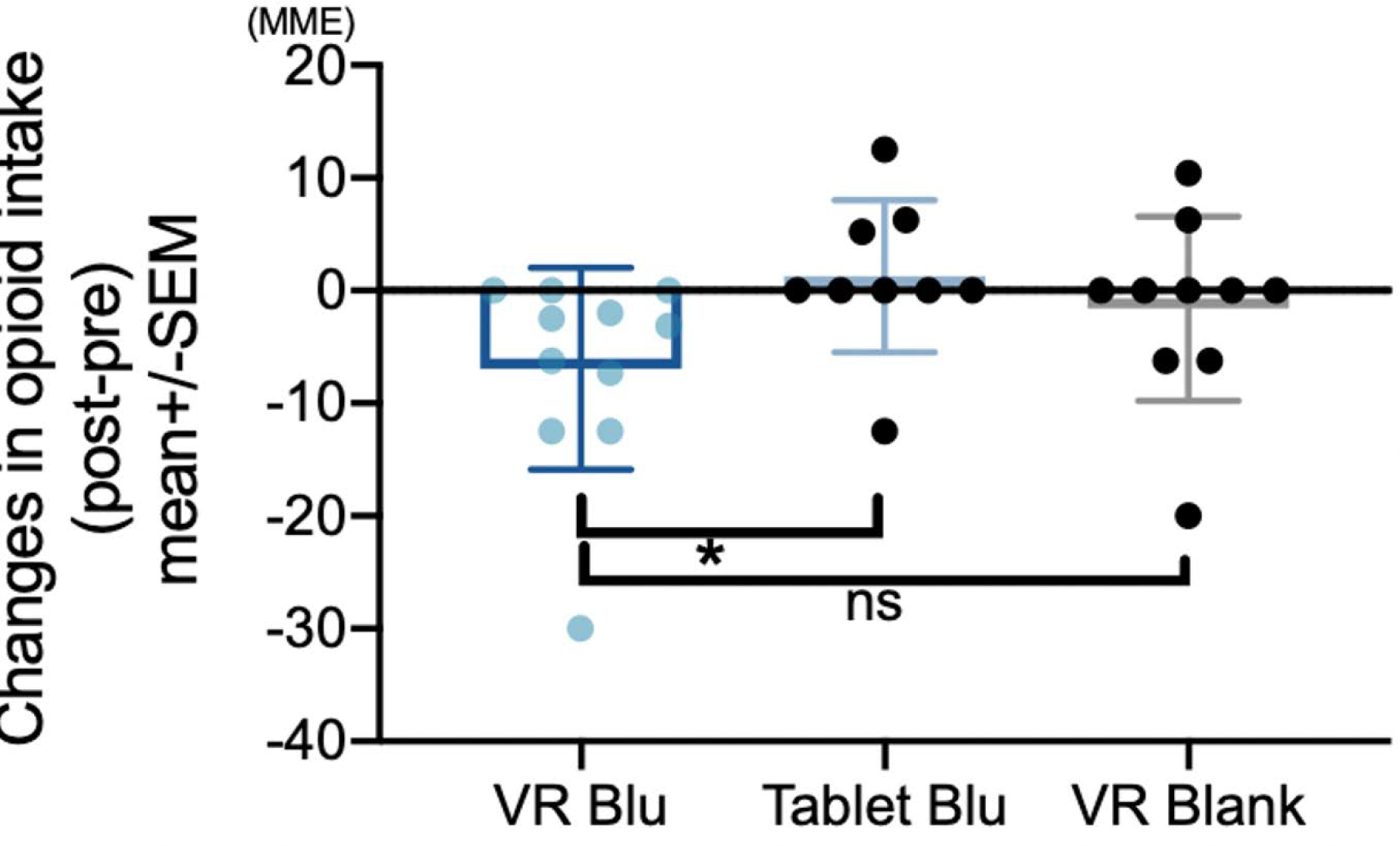
There were 14 VR Blu Responders, defined as patients that had a 3-point on greater pain reduction from VR Blu. VR Blu responders had significantly more reductions in opioid intake (measured in morphine equivalents) in the four hours following VR Blu compared to Tablet Blu (one-tailed p < .012) but not after VR Blank condition (one-tailed p < .063).
Anxiety
There was no significant effect of the experimental condition on patient anxiety changes as measured by the short-form STAI (F1,77.48 = 1.66, p = .198).
Autonomic Measures
There were no significant effects of condition on changes in systolic blood pressure (F2,61.93 = 1.13, p = .330) or heart rate (F2,70.22=1.98, p=.146) after controlling for experimental sequence, age, sex, race, baseline pain severity, and injury severity. We observed a significant main effect of the three VR conditions on diastolic blood pressure (F2,70.68 = 3.38, p = .004) where VR Blu induced a significant decrease in diastolic blood pressure as compared to VR Blank condition (LSD adjusted one-tailed p = .050) but no different from the Tablet Blu (LSD adjusted one-tailed p = .102). Moreover, decreasing of diastolic blood pressure induced by Tablet Blu was significantly greater than the VR Blank condition (LSD adjusted one-tailed p = .012). In addition, there was a significant main effect of the VR conditions on pupillary maximum constriction velocity (F2,61.41 = 3.50, p = .038). Pairwise comparisons indicated that VR Blu increased maximal constriction velocity, a measure of parasympathetic nervous system activity, more than VR Blank (LSD adjusted one-tailed p = .006) but not different than the Tablet Blu (LSD adjusted one-tailed p = .059, Figure 4). Tablet Blu and VR Blank did not significantly differ in maximal constriction velocity (LSD adjusted one-tailed p = .081).
Figure 4: Change in pupillary maximum constriction velocity by intervention.
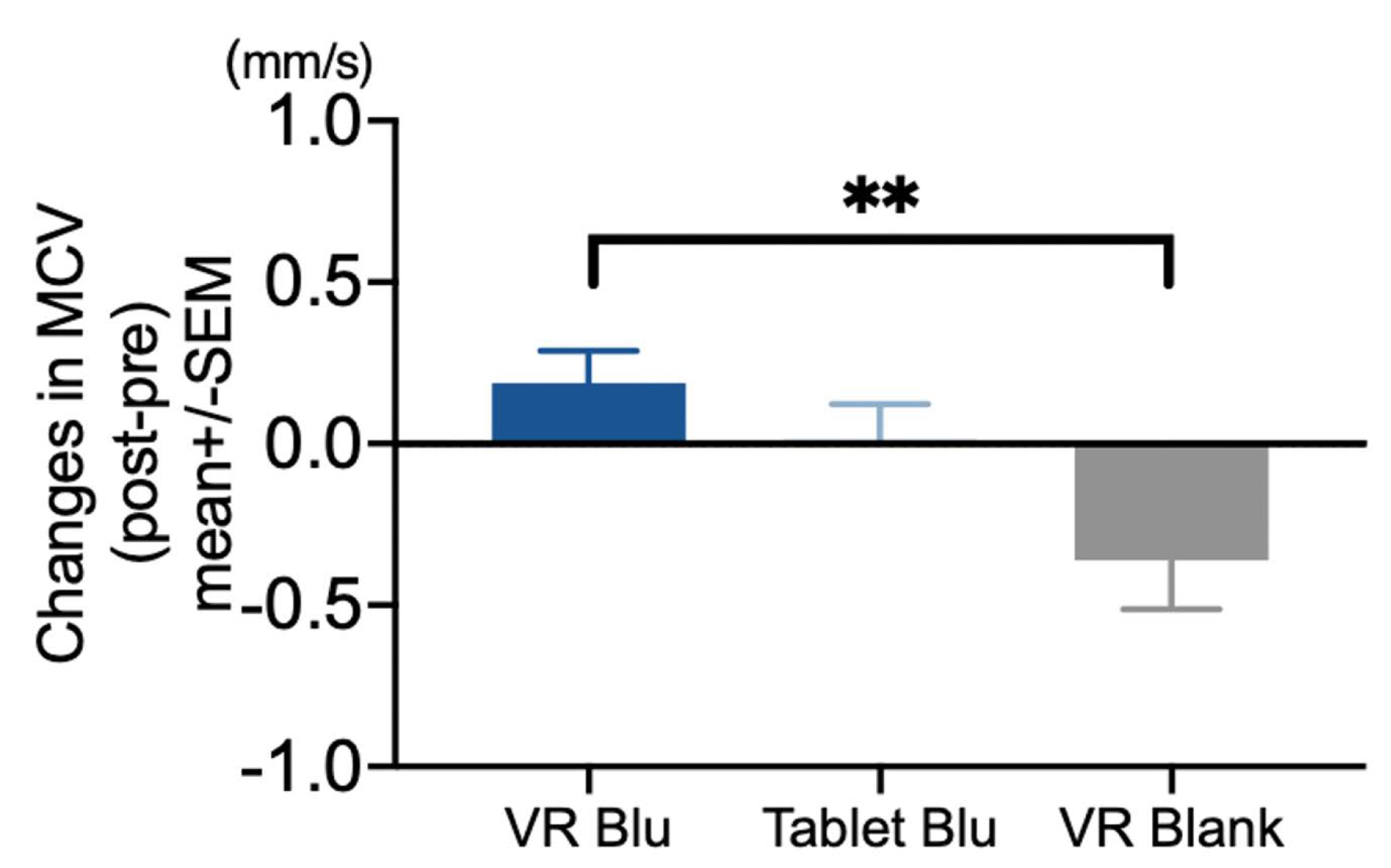
Controlling for the experimental sequences, age, sex, race, baseline pain severity and injury severity, the main effect of the three experimental conditions on maximum constriction velocity was significant (F1,61.41=3.50, p=.038), whereas VR Blu condition induced a significant greater increase in maximum constriction velocity than the VR Blank condition (one-tailed p=.006).
Results from heart rate variability indicated that VR Blu slowed the heart rate (F2,57.31=3.61, p = .033, mean=348.82 beats/5mins, SEM=4.23) more than VR Blank did (mean=361.83 beats/5mins, SEM=3.07, one-tailed p=.008), adjusting for baseline variabilities and controlling for age, sex, race, as well as the sequence of experimental conditions (Figure 5A). No significant differences were observed in heart rate between VR Blu and Tablet Blu (LSD adjusted one-tailed p = .316), or VR blank and Tablet Blu (LSD adjusted one-tailed p = 0.051). Moreover, we observed a significant main effect of the experimental condition on the NN mean index (F2,55.511 = 7.87, p < .001). Both VR Blu (mean = 874.64 ms, SEM = 15.36 ms) and VR Blank (mean = 867.64 ms, SEM = 10.37 ms) induced greater NN mean compared to the tablet Blu condition (mean = 834.78 ms, SEM = 1.93 ms, one-tailed p = .008 and .003, respectively), suggesting greater levels of parasympathetic activity induced by both VR conditions (Figure 5B). No main effect of the three experimental conditions on frequency domain indices LF power (F2,29.33 = 1.19, p = .320) and HF power (F2,57.52 = .69, p = .505) were found.
Figure 5: Changes in Heart Rate Variability by Intervention.
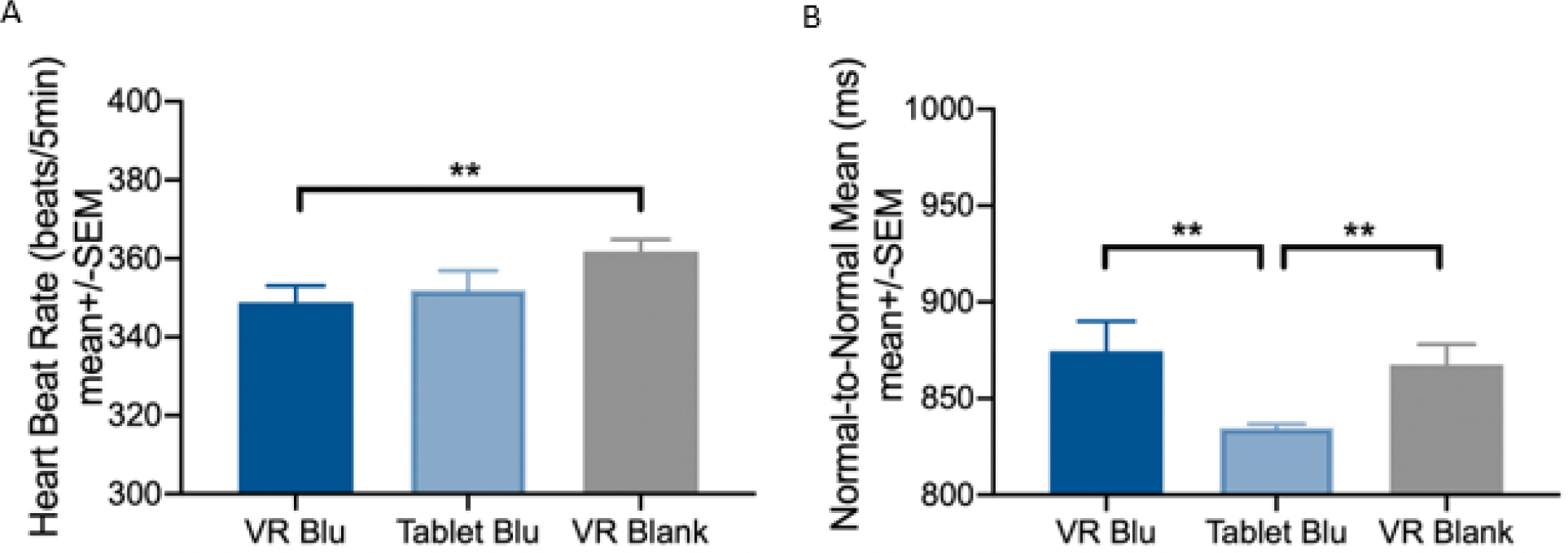
(A) VR Blu slowed down the heartbeat rate more than VR Blank condition did. (B) Both VR Blue and VR Blank conditions induced greater normal-to-normal means compared to Tablet Blu condition. All results adjusted for baseline heartbeat rate and controlled for age, sex, race and experimental sequences
Side-Effects
Compared to the baseline and across conditions, there were no significant worsening of neck pain (F2,83.50 = 0.696, p = .501), nausea (F2,46.559 = 0.707, p = .498), dizziness (F2,89.820 = 0.330, p = .720), or light-sensitivity (F2,90.602 = 1.330, p = .270). The results were unchanged in the subset of patients with TBI. No patients had a seizure or reported motion sickness associated with any interventions.
Patient Engagement and Perception
There was a significant main effect of the three conditions on Brockmyer Gaming Engagement (F2,76.54 = 20.00, p < .001). Pairwise comparison applying LSD adjustment indicated that patients were significantly more engaged in VR Blu compared to Tablet Blu or VR Blank (mean 52.31 (SEM 2.04) vs. 38.02 (SEM 2.30) vs. 35.91 (SEM 2.25), both one-tailed p < .001). Engagement was not significantly associated with VR Blu induced pain relief (Pearson r = .074, one-tailed p = .300), but did correlate with increased pain reduction across all conditions (Pearson r = .15, one-tailed p = .029) There was a significant main effect of the VR conditions on patients’ perception of effectiveness (F2,66.84 = 16.28, p < .001). Patients perceived VR Blu as more effective than VR Blank (one-tailed p < .001) and Tablet Blu (one-tailed p = .007) (Figure 6) in reducing their clinical pain.
Figure 6: Perceived Effectiveness of Interventions.
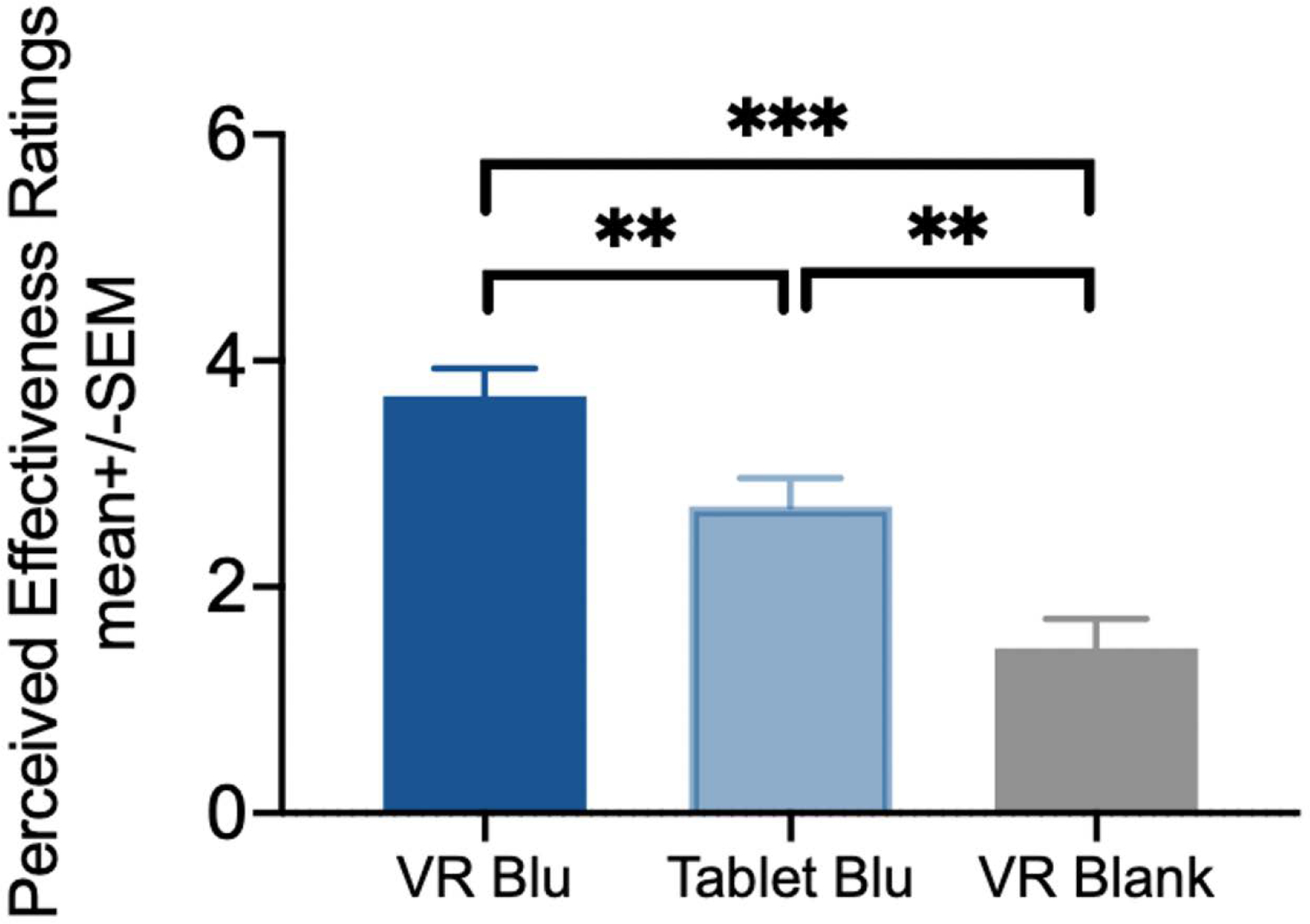
Controlling for the experimental sequences, age, sex, race, baseline pain severity and injury severity, the main effect of the three experimental conditions on perceived effectiveness (measured on a Likert scale from 0 (not at all effective) to 5 (very effective)) was significant (F1,65.73=16.24, p<0.001). The self-reported perceived effectiveness in pain reduction was the highest for the VR Blu condition (mean=3.63, sem=0.23) compared to both Tablet Blu (mean=2.68, sem=0.23, p=0.005) and VR Blank conditions (mean=1.52, sem=0.29, p<0.001), where Tablet Blu condition had greater perceived effectiveness than the VR blank condition (p=0.003).
Discussion
In this randomized within-subjects proof-of-concept study of patients hospitalized with acute traumatic injuries, including TBI, we found that adjunctive VR-delivered intervention (VR Blu and VR Blank) surpassed the tablet-delivered benefit in reducing clinical pain, after controlling for demographics, baseline pain severity, and injury severity. No condition had a significant effect on anxiety. VR Blu, but not VR Blank, led to an increase in pupillary maximum constriction velocity and heart rate variability as measured by NN mean and heart rate, suggesting increased parasympathetic activity induced by VR Blu. While both the VR Blu and the VR Blank conditions decreased pain compared to Tablet Blu, study patients perceived that VR Blu was more effective than Tablet Blu, which they perceived as more effective than VR Blank. Patients who benefited from the VR Blu intervention used less opioids following the intervention than in the hours preceding the VR Blu condition but not after Tablet Blu or VR Blank, suggesting that successful pain reduction with VR may potentially reduce inpatient opioid needs. In terms of safety, we did not find any side effects related to VR in this population such as nausea, photophobia, and dizziness indicating potential for therapeutic clinical use of VR-delivered interventions.
Our study builds on prior work demonstrating efficacy of VR interventions for acute clinical pain, which has mostly focused on burn and wound care[30], as well as periprocedural pain[6]. The few studies focused on VR analgesia for acute traumatic pain have been limited by small sample size or lack of controls, limitations shared by studies of VR for other acute pain etiologies[16; 18; 26; 35]. More robust studies of VR for administration of behavioral therapy for chronic pain have led to FDA approval for that indication[8; 14]. A recent, properly powered, randomized-controlled trial of VR hypnosis for acute traumatic pain, in contrast, found no analgesic benefits[40].
Our study differs from that study in several important ways. First, we included patients with TBI (compared to only long-bone fractures and intra-abdominal injury requiring surgical repair). Second, we used a within-subjects design to increase power. Third, we only studied VR distraction as opposed to VR hypnosis. In addition, we used more modern VR technology, our controls differed, we evaluated pain immediately before and after each session (as opposed to averages over the hospital stay), and as a proof-of-concept study our analyses were less rigorous in controlling for multiple comparisons. It is possible that VR analgesia is effective in pain reduction but either it was not administered frequently enough, or its effect was not durable enough to affect pain scores averaged over the entire hospitalization in the other trial. Further work is necessary to explore the dosing and durability of VR intervention benefits for acute traumatic pain in inpatients.
Surprisingly, both the VR Blu and VR Blank conditions relieved pain significantly. A recent paper found that in healthy controls more immersive environments increased analgesia in a thermal pain stimulus paradigm[17]. The effect of presence or engagement on VR-induced pain reduction may be different in trauma inpatients compared to healthy controls. The VR Blank per se is not immersive. We did, however, measure engagement, which was significantly higher in the VR Blu condition. Engagement positively correlated with pain reduction, albeit weakly. We posit that VR Blank may have reduced pain intensity through ritual placebo effects by merely wearing the VR headset [19]. In fact, it is possible that both VR conditions benefited from a placebo effect and future studies should test to which extent there is an effect beyond placebo. An alternative explanation is that wearing the VR headset reduced noxious visual and auditory stimuli from the hospital environment, explaining the pain reduction in both VR Blu and VR Blank compared to the tablet.[29]. In the future, a no-intervention intervention would help disentangle placebo versus VR headset-derived benefits. Patients perceived the VR Blu as more effective than the tablet control in line with the results. However, they perceived the VR Blank as inferior, and this may be due to the lack of VR content and therefore engagement. Beyond pain, others have reported effects of interventions on patient-reported measures that are distinct and independent from objective physiological measures[39].
Nonetheless, we found objective physiological evidence of the effect of the immersive VR intervention on the autonomic nervous system responses. Indeed, VR Blu increased pupillary maximum constriction velocity and heart rate variability, suggesting increased parasympathetic activation [32]. This result echoed those from a previous study where VR induced an increase in parasympathetic nervous activation that is paralleled with a gain in experimental heat pain tolerance [7]. In fact, the autonomic nervous system may interact with descending pain modulation pathway given that brain areas of pain matrix (e.g., middle cingulate cortex, anterior cingulate cortex, insular cortex, hypothalamus, amygdala, and periaqueductal gray) also contribute to autonomic responses [2]. It is plausible that VR triggers a re-balancing of sympathetic and parasympathetic nervous homeostasis that could optimize with the endogenous descending pain modulatory system [37] mitigating pain experience. The immersive VR Blu may affect sensory pathways and ultimately activate parasympathetic responses that decrease pain unpleasantness, while the sensory deprivation of the VR Blank condition may significantly reduce pain but have less effects on perception of effectiveness [31]. An important aspect of this study is the difference in the results measured by the subjective ratings and the physiological measures. If we would have considered only the subjective measure of pain, VR Blu and VR Blank similar results would have prevented us from understanding part of the observed benefits. Without such measures we may not have been able to discern meaningful differences between the VR Blu and VR Blank environments. The physiological measures gave an appreciation of the VR Blu condition in line with a previous study [8] where the vagal activation characterized the VR Blu as compared to several control conditions. Our results highlight the importance of incorporating physiologic measures in future studies when testing immersive VR environments. We note that our analysis of physiologic measures did not account for multiple comparisons, warranting cautious interpretation.
Our study has some limitations and strengths. Very few patients with TBI met inclusion criteria. Expected hospital length of stay is usually quite short in mild TBI and patients with more severe TBI would not be able to engage with the content. Thus, while we initially hoped to only enroll patients with TBI, we opened enrollment to patients with other traumatic injuries and we were underpowered to detect significant effects in the subset of patients with TBI. We did, however, include some patients with (mild) acute TBI, a group in whom VR has been studied very little. Mild TBI causes headache, light sensitivity, nausea, and dizziness that persists over 12 months following injury[25]. We were concerned that VR may have carried a risk of exacerbating these symptoms, but it was reassuring that VR Blu did not worsen any of these symptoms compared to the other conditions. Mild TBI may also have increased risk of seizure but no patient seized as a result of participating in the study. Early traumatic seizures are unlikely to be photosensitive and recent expert consensus is that VR technology does not raise seizure concerns[12]. Furthermore, we note that there were no safety concerns at all in our entire cohort of inpatients with traumatic injuries. We do not appreciate any compelling reason to exclude patients with traumatic injuries from future trials of VR environments, for pain reduction, physical rehabilitation, or other purposes.
In addition, the intervals between conditions were quite short to improve feasibility of study completion based on brief anticipated length of stay. This limited our ability to evaluate effects on opioid use and duration of VR intervention effect. This was necessary, however, in order to include control conditions, which are often lacking from VR studies. Future studies may consider focusing on VR interventions in the outpatient setting to facilitate study of duration of the effect and dosing of VR interventions along with influences on opioid reduction. Finally, the sample size limited out ability to account for multiple comparisons; thus, our findings should be interpreted cautiously.
Conclusions
Adjunctive VR interventions to reduce clinical pain in in-patients with acute traumatic injuries, including TBI, is safe and may have modest yet tangible analgesic effects through increased parasympathetic nervous system activation and engagement perceived as beneficial. Future studies of VR in acute traumatic injuries may need to extend to outpatient settings to study long-term effects of VR-based interventions, given generally short hospital lengths of stay.
Acknowledgments
We acknowledge the support of the University of Maryland, Baltimore, Institute for Clinical & Translational Research (ICTR), the National Center for Advancing Translational Sciences (NCATS) Clinical Translational Science Award (CTSA) grant number 1UL1TR003098, and the National Center for Complementary and Integrative Health (R01 AT011347–01A1, LC). The funding source had no involvement in this work.
Footnotes
Conflicts of Interest
L.C. received in the past 3 years research grants from the US National Institutes of Health, and honoraria for lecturing, payment for expert testimony, consulting fees from Chiesi, Averitas, Shionogi and Patient-Centered Outcomes Research Institute, and royalties for a didactical book. N.A.M. has received honoraria for Continuing Medical Education (Grand Rounds, Review Papers, Tweetorials) and serves on the editorial board for Neurology. The other authors have no conflicts of interest to report.
References
- [1].Heart rate variability. Standards of measurement, physiological interpretation, and clinical use. Task Force of the European Society of Cardiology and the North American Society of Pacing and Electrophysiology. Eur Heart J 1996;17(3):354–381. [PubMed] [Google Scholar]
- [2].Arslan D, Çevik IÜ. Interactions between the painful disorders and the autonomic nervous system. Agri 2022;34:155–165. [DOI] [PubMed] [Google Scholar]
- [3].Aulisio MC, Han DY, Glueck AC. Virtual reality gaming as a neurorehabilitation tool for brain injuries in adults: A systematic review. Brain Inj 2020;34(10):1322–1330. [DOI] [PubMed] [Google Scholar]
- [4].Broadway DC. How to test for a relative afferent pupillary defect (RAPD). Community Eye Health 2012;25(79–80):58. [PMC free article] [PubMed] [Google Scholar]
- [5].Brockmyer JH, Fox CM, Curtiss KA, McBroom E, Burkhart KM, Pidruzny JN. The development of the Gaming Engagement Questionnaire: a measure of engagement in video game-playing. Journal of Experimental Social Psychology 2009;45:624–634. [Google Scholar]
- [6].Chuan A, Zhou JJ, Hou RM, Stevens CJ, Bogdanovych A. Virtual reality for acute and chronic pain management in adult patients: a narrative review. Anaesthesia 2021;76(5):695–704. [DOI] [PubMed] [Google Scholar]
- [7].Colloca L, Raghuraman N, Wang Y, Akintola T, Brawn-Cinani B, Colloca G, Kier C, Varshney A, Murthi S. Virtual reality: physiological and behavioral mechanisms to increase individual pain tolerance limits. Pain 2020;161(9):2010–2021. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [8].Darnall BD, Krishnamurthy P, Tsuei J, Minor JD. Self-Administered Skills-Based Virtual Reality Intervention for Chronic Pain: Randomized Controlled Pilot Study. JMIR Form Res 2020;4(7):e17293. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [9].Dharmarajan S, Lee JY, Izem R. Sample size estimation for case-crossover studies. Stat Med 2019;38(6):956–968. [DOI] [PubMed] [Google Scholar]
- [10].Dupont WD. Power calculations for matched case-control studies. Biometrics 1988;44(4):1157–1168. [PubMed] [Google Scholar]
- [11].Felix RB, Rao A, Khalid M, Wang Y, Colloca L, Murthi SB, Morris NA. Adjunctive virtual reality pain relief following traumatic injury: protocol for a randomised within-subjects clinical trial. BMJ Open 2021;11(11):e056030. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [12].Fisher RS, Acharya JN, Baumer FM, French JA, Parisi P, Solodar JH, Szaflarski JP, Thio LL, Tolchin B, Wilkins AJ, Kasteleijn-Nolst Trenité D. Visually sensitive seizures: An updated review by the Epilepsy Foundation. Epilepsia 2022;63(4):739–768. [DOI] [PubMed] [Google Scholar]
- [13].Flanagan CD, Wysong EF, Ramey JS, Vallier HA. Understanding the Opioid Epidemic: Factors Predictive of Inpatient and Postdischarge Prescription Opioid Use After Orthopaedic Trauma. J Orthop Trauma 2018;32(10):e408–e414. [DOI] [PubMed] [Google Scholar]
- [14].Garcia LM, Birckhead BJ, Krishnamurthy P, Sackman J, Mackey IG, Louis RG, Salmasi V, Maddox T, Darnall BD. An 8-Week Self-Administered At-Home Behavioral Skills-Based Virtual Reality Program for Chronic Low Back Pain: Double-Blind, Randomized, Placebo-Controlled Trial Conducted During COVID-19. J Med Internet Res 2021;23(2):e26292. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [15].Hall CA, Chilcott RP. Eyeing up the Future of the Pupillary Light Reflex in Neurodiagnostics. Diagnostics (Basel) 2018;8(1). [DOI] [PMC free article] [PubMed] [Google Scholar]
- [16].Hile GB, Cook AM. Treatment of headache in aneurysmal subarachnoid hemorrhage: Multimodal approach. Interdisciplinary Neurosurgery 2021;22:100857. [Google Scholar]
- [17].Hoffman HG. Interacting with virtual objects via embodied avatar hands reduces pain intensity and diverts attention. Sci Rep 2021;11(1):10672. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [18].Hoffman HG, Patterson DR, Soltani M, Teeley A, Miller W, Sharar SR. Virtual reality pain control during physical therapy range of motion exercises for a patient with multiple blunt force trauma injuries. Cyberpsychol Behav 2009;12(1):47–49. [DOI] [PubMed] [Google Scholar]
- [19].Honzel E, Murthi S, Brawn-Cinani B, Colloca G, Kier C, Varshney A, Colloca L. Virtual reality, music, and pain: developing the premise for an interdisciplinary approach to pain management. Pain 2019;160(9):1909–1919. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [20].Jensen MP, Karoly P, Braver S. The measurement of clinical pain intensity: a comparison of six methods. Pain 1986;27(1):117–126. [DOI] [PubMed] [Google Scholar]
- [21].Liszio S, Graf L, Masuch M. The relaxing effect of virtual nature: immersive technology provides relief in acute stress situations. Annual Review of Cybertherapy and Telemedicine 2018;16:87–93. [Google Scholar]
- [22].Marteau TM, Bekker H. The development of a six-item short-form of the state scale of the Spielberger State-Trait Anxiety Inventory (STAI). Br J Clin Psychol 1992;31(3):301–306. [DOI] [PubMed] [Google Scholar]
- [23].Mazurenko O, Andraka-Christou BT, Bair MJ, Kara AY, Harle CA. Clinical perspectives on hospitals’ role in the opioid epidemic. BMC Health Serv Res 2020;20(1):521. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [24].Mosadeghi S, Reid MW, Martinez B, Rosen BT, Spiegel BM. Feasibility of an Immersive Virtual Reality Intervention for Hospitalized Patients: An Observational Cohort Study. JMIR Ment Health 2016;3(2):e28. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [25].Nelson LD, Temkin NR, Dikmen S, Barber J, Giacino JT, Yuh E, Levin HS, McCrea MA, Stein MB, Mukherjee P, Okonkwo DO, Diaz-Arrastia R, Manley GT, Adeoye O, Badjatia N, Boase K, Bodien Y, Bullock MR, Chesnut R, Corrigan JD, Crawford K, Duhaime AC, Ellenbogen R, Feeser VR, Ferguson A, Foreman B, Gardner R, Gaudette E, Gonzalez L, Gopinath S, Gullapalli R, Hemphill JC, Hotz G, Jain S, Korley F, Kramer J, Kreitzer N, Lindsell C, Machamer J, Madden C, Martin A, McAllister T, Merchant R, Noel F, Palacios E, Perl D, Puccio A, Rabinowitz M, Robertson CS, Rosand J, Sander A, Satris G, Schnyer D, Seabury S, Sherer M, Taylor S, Toga A, Valadka A, Vassar MJ, Vespa P, Wang K, Yue JK, Zafonte R, Investigators at T-T, MIS. Recovery After Mild Traumatic Brain Injury in Patients Presenting to US Level I Trauma Centers: A Transforming Research and Clinical Knowledge in Traumatic Brain Injury (TRACK-TBI) Study. JAMA Neurol 2019. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [26].Patterson DR, Jensen MP, Wiechman SA, Sharar SR. Virtual reality hypnosis for pain associated with recovery from physical trauma. Int J Clin Exp Hypn 2010;58(3):288–300. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [27].Rice T, Mancinelli C, Utzman R, Cassis A, Wetmore S. Reliability of the Numeric Dizziness Scale for the Quantification of Dizziness. West Virginia Medical Journal 2018;114(3):30–35. [Google Scholar]
- [28].Ringham BM, Kreidler SM, Muller KE, Glueck DH. Multivariate test power approximations for balanced linear mixed models in studies with missing data. Stat Med 2016;35(17):2921–2937. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [29].Russo AF, Recober A. Unanswered questions in headache: so what is photophobia, anyway? Headache 2013;53(10):1677–1678. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [30].Scapin S, Echevarria-Guanilo ME, Boeira Fuculo Junior PR, Goncalves N, Rocha PK, Coimbra R. Virtual Reality in the treatment of burn patients: A systematic review. Burns 2018;44(6):1403–1416. [DOI] [PubMed] [Google Scholar]
- [31].Stilwell P, Hudon A, Meldrum K, Pagé MG, Wideman TH. What is Pain-Related Suffering? Conceptual Critiques, Key Attributes, and Outstanding Questions. J Pain 2022;23(5):729–738. [DOI] [PubMed] [Google Scholar]
- [32].Sztajzel J Heart rate variability: a noninvasive electrocardiographic method to measure the autonomic nervous system. Swiss Med Wkly 2004;134(35–36):514–522. [DOI] [PubMed] [Google Scholar]
- [33].Tashjian VC, Mosadeghi S, Howard AR, Lopez M, Dupuy T, Reid M, Martinez B, Ahmed S, Dailey F, Robbins K, Rosen B, Fuller G, Danovitch I, IsHak W, Spiegel B. Virtual Reality for Management of Pain in Hospitalized Patients: Results of a Controlled Trial. JMIR Ment Health 2017;4(1):e9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [34].Taylor CA, Bell JM, Breiding MJ, Xu L. Traumatic Brain Injury-Related Emergency Department Visits, Hospitalizations, and Deaths - United States, 2007 and 2013. MMWR Surveill Summ 2017;66(9):1–16. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [35].Teeley AM, Soltani M, Wiechman SA, Jensen MP, Sharar SR, Patterson DR. Virtual reality hypnosis pain control in the treatment of multiple fractures: a case series. Am J Clin Hypn 2012;54(3):184–194. [DOI] [PubMed] [Google Scholar]
- [36].ten Klooster PM, Drossaers-Bakker KW, Taal E, van de Laar MA. Patient-perceived satisfactory improvement (PPSI): interpreting meaningful change in pain from the patient’s perspective. Pain 2006;121(1–2):151–157. [DOI] [PubMed] [Google Scholar]
- [37].Tracey I, Mantyh PW. The cerebral signature for pain perception and its modulation. Neuron 2007;55(3):377–391. [DOI] [PubMed] [Google Scholar]
- [38].Trost Z, France C, Anam M, Shum C. Virtual reality approaches to pain: toward a state of the science. Pain 2021;162(2):325–331. [DOI] [PubMed] [Google Scholar]
- [39].Wechsler ME, Kelley JM, Boyd IO, Dutile S, Marigowda G, Kirsch I, Israel E, Kaptchuk TJ. Active albuterol or placebo, sham acupuncture, or no intervention in asthma. N Engl J Med 2011;365(2):119–126. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [40].Wiechman SA, Jensen MP, Sharar SR, Barber JK, Soltani M, Patterson DR. The Impact of Virtual Reality Hypnosis on Pain and Anxiety Caused by Trauma: Lessons Learned from a Clinical Trial. Int J Clin Exp Hypn 2022;70(2):156–173. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [41].Wikström L, Nilsson M, Broström A, Eriksson K. Patients’ self-reported nausea: Validation of the Numerical Rating Scale and of a daily summary of repeated Numerical Rating Scale scores. J Clin Nurs 2019;28(5–6):959–968. [DOI] [PubMed] [Google Scholar]
- [42].Young IA, Dunning J, Butts R, Cleland JA, Fernández-de-Las-Peñas C. Psychometric properties of the Numeric Pain Rating Scale and Neck Disability Index in patients with cervicogenic headache. Cephalalgia 2019;39(1):44–51. [DOI] [PubMed] [Google Scholar]