

Abstract
Propose
The purpose of this study was to assess whether the implementation of a "dual trigger" approach, utilizing gonadotropin-releasing hormone agonist (GnRHa) and human chorionic gonadotropin (hCG) in the GnRH antagonist protocol for in vitro fertilization (IVF), leads to improved pregnancy outcomes compared to the conventional hCG trigger alone. Previous meta-analyses have not provided sufficient evidence to support the superiority of the dual trigger over the hCG trigger in fresh or frozen embryo transfer cycles. Thus, a systematic review and meta-analysis of randomized trials were conducted to provide a comprehensive evaluation of the impact of the dual trigger on pregnancy outcomes in fresh or frozen embryo transfer cycles.
Method
A systematic review and meta-analysis of randomised controlled trials (RCTs) were conducted. We searched the Medline and Embase databases for articles up to 2023 by using search terms: “dual trigger,” “GnRHa,” “hCG,” “IVF.” Eligible RCTs comparing the dual trigger with the hCG trigger were included. The primary outcome was the live birth rate (LBR) per cycle. The secondary outcomes were the number of oocytes retrieved, number of mature oocytes retrieved, implantation rate, biochemical pregnancy rate, CPR, miscarriage rate and ovarian hyperstimulation syndrome (OHSS) rate per started cycle We compared the oocyte maturation and pregnancy outcomes in the dual trigger and hCG trigger groups. In patients undergoing fresh embryo transfer (ET) and frozen–thawed ET, we also conducted a subgroup analysis to evaluate whether dual trigger improves the clinical pregnancy rate (CPR).
Results
We included 10 randomised studies, with 825 participants in the dual trigger group and 813 in the hCG trigger group.
Compared with the hCG trigger, dual trigger was associated with a significant increase in the LBR per cycle (odds ratio (OR) = 1.61[1.16, 2.25]), number of oocytes retrieved (mean difference [MD] = 1.05 [0.43, 1.68]), number of mature oocytes retrieved (MD = 0.82 [0. 84, 1.16]), and CPR (OR = 1.48 [1.08, 2.01]). Subgroup analyses revealed that dual trigger was associated with a significantly increased CPR in patients who received fresh ET (OR = 1.68 [1.14, 2.48]). By contrast, the dual trigger was not associated with an increased CPR in the patient group with frozen–thawed ET (OR = 1.15 [0.64, 2.08]).
Conclusion
The dual trigger was associated with a significantly higher number of retrieved oocytes, number of mature oocytes, CPR, and LBR in IVF than the hCG trigger. The beneficial effect for fresh ET cycles compared with frozen–thawed ET might be associated with increased endometrial receptivity.
Relevance
After dual trigger, delaying ET due to the concern of endometrial receptivity might not be needed.
Keywords: Dual trigger, GnRH agonist, hCG, Randomised trials, Systematic review, Meta-analysis
Introduction
In vitro fertilization (IVF) and intracytoplasmic sperm injection (ICSI) are assisted reproductive technology (ART) procedures that involve controlled ovarian hyperstimulation, oocyte retrieval before ovulation, and oocyte insemination.
The gonadotropin-releasing hormone (GnRH) antagonist protocol is widely used during controlled ovarian hyperstimulation (COH) for IVF. GnRH antagonists competitively block GnRH receptors, causing gonadotropin suppression and preventing a premature luteinizing hormone (LH) surge. The advantages of the GnRH antagonist protocol over GnRH agonist (GnRHa) protocols (i.e. long protocol) include the absence of a flare-up effect, rapid decline in LH and follicle-stimulating hormone (FSH) levels, lower gonadotropin dose, and shorter duration of ovulation stimulation [1–3].
In a spontaneous ovulatory cycle, the mid-cycle LH surge induces oocyte maturation and triggers ovulation. In ART, final oocyte maturation can be triggered using human chorionic gonadotropin (hCG), the GnRHa, or their combination (‘dual’ or ‘double’ trigger). Exogenous hCG has been used to trigger final oocyte maturation since the mid-1970s because its biological activity is similar to that of LH. Oocytes respond to the LH surge by resuming meiosis and processing through synchronised maturation of the nucleus and cytoplasm [4]. hCG acts on the receptor shared with LH (i.e. LH and chorionic gonadotropin receptor [LH/CG receptor]), serving as a surrogate to the naturally occurring LH surge [5].
Final oocyte maturation can also be stimulated using one or multiple doses of a GnRHa. GnRHa induces a surge of FSH and LH, resembling the preovulatory gonadotropin surge in natural cycles. Both animal and human studies have indicated that FSH plays a role in ovulation and oocyte maturation by stimulating the expansion of cumulus cells surrounding the oocyte and inducing the formation of LH receptors on luteinised granulosa cells [6, 7]. By coordinating the resumption of oocyte meiosis, FSH eventually increases the number of metaphase II (MII) oocytes [6, 7]. However, compared with the traditional hCG trigger, using a GnRHa alone induces a shorter LH surge, resulting in luteal-phase dysfunction [8], which required intensive luteal phase support to improve pregnancy outcomes.
The dual trigger involves the concurrent administration of a GnRHa and hCG. Initially proposed by Shapiro et al. (2011) [9], it combines the advantages of hCG and GnRHa triggers. Despite the increasing evidence of its superiority over an hCG-only trigger [10, 11], systemic reviews and meta-analyses of randomized studies have provided controversial results [12–15]. Ding et al. found that while the dual trigger was not associated with an increased number of oocytes or mature oocytes retrieved, it could significantly improve the pregnancy rate [15]. Zhang et al. concluded that despite dual trigger was associated with a significant increased number of retrieved oocytes or mature oocytes compared with hCG trigger, there was no significant difference between the pregnancy rate in the two groups [12]. The study by Hu et al. included eight randomized trials published before 2020 indicated that the dual trigger is associated with significant increases in the total number of oocytes retrieved, the number of mature oocytes retrieved, clinical pregnancy rate, and live birth rate [14]. Because newer randomized trials on this topic have since been conducted [2, 3], we performed a systematic review and meta-analysis to compare the effects of dual and HCG triggers. We also performed a subgroup analysis to evaluate the effect of the dual trigger on the clinical pregnancy rate after fresh embryo transfer (ET) and frozen–thawed ET.
Materials and methods
Eligibility criteria
Only randomized studies in English comparing the effect of dual trigger with hCG trigger for final oocyte maturation were included. Case reports, observational studies, retrospective cohort studies, review articles, conference abstracts, and study protocols were excluded.
Information sources
Two authors (LHH and YHL) independently searched the Medline and Embase databases for randomized studies published before April 2023.
Search strategy
The search keywords included ‘in vitro fertilization,’ ‘intracytoplasmic sperm injection,’ ‘GnRH agonist,’ ‘hCG,’ ‘dual trigger,’ and ‘randomized trials.’ References from the articles assessed for eligibility were manually screened to identify other potentially relevant articles.
Selection process
The titles and abstracts of the studies considered for inclusion were independently screened by the two authors (LHH and YHL), and ineligible articles were excluded. No automation tool was used. The full texts of the eligible studies were reviewed to determine their eligibility. Discussions or consultations with a third author (THL) resolved disagreements regarding study inclusion.
The two authors (LHH and YHL) independently also extracted data from the included articles for analysis.
Data items
The primary outcome was the live birth rate per cycle. The live birth rate was defined as the number of deliveries resulting in at least one live birth, expressed per cycle.
The secondary outcomes were the number of oocytes retrieved, number of mature oocytes (i.e. MII oocytes) retrieved, implantation rate, biochemical pregnancy rate, clinical pregnancy rate, miscarriage rate, and ovarian hyperstimulation syndrome (OHSS) rate per started cycle. The biochemical pregnancy rate per cycle was calculated as the number of patients with beta hCG detection in the serum or urine divided by the total number of started cycles. The clinical pregnancy rate per cycle was calculated as the number of patients with ultrasonographic visualization of one or more gestational sacs or definitive clinical signs of pregnancy divided by the total number of started cycles. The implantation rate per cycle was determined as the number of gestational sacs observed divided by the number of embryos transferred in each started cycle. The miscarriage rate was calculated as the number of cases with spontaneous loss of intrauterine pregnancy prior to 22 completed weeks of gestational age divided by the total number of started cycles. OHSS was defined as a systemic response from ovarian stimulation interventions characterised by a broad spectrum of severe clinical symptoms and biochemical abnormalities [16].
Data were extracted for the outcomes reported in each study. If the information was unclear or the measurements of results were incompatible with our study outcome, the data were omitted.
Study risk-of-bias assessment
Quality assessments for the 10 included studies were conducted by the two authors (LHH and YHL). We assessed the risk of bias according to Version 1 of the Cochrane risk-of-bias tool for randomized trials (RoB 1.0).
Effect measures
The effects of continuous results expressed as mean and standard deviation were measured by estimating the mean difference with 95% confidence interval. The effects of dichotomous data were measured by calculating the odds ratio.
Synthesis methods
We used Review Manager (Review Manager (RevMan) [Computer program]. Version 5.4. The Cochrane Collaboration, 2020. Available at revman.cochrane.org) to analyze the extracted data from the included studies. The inverse variance model was used to combine the results for the meta-analyses.
When no significant heterogeneity (I2 < 50%) was noted, a fixed-effects model was used for the meta-analysis; when substantial heterogeneity (I2 > 50%) was observed, a random-effect model was used for the meta-analysis.
Statistical significance was set at P ≤ 0.05.
Reporting bias assessment
A funnel plot was used to evaluate the publication bias for the primary outcome.
Certainty assessment
Two reviewers assessed the confidence of evidence across the outcomes by using the Grading of Recommendations Assessment, Development and Evaluation (GRADE) system. The GRADE approach classifies the certainty of evidence into one of four grades: high, moderate, low, and very low.
Results
Study selection
After the initial search, the duplicate entries were removed. The titles and abstracts of the remaining 364 studies were screened. Eventually, the full texts of 11 eligible articles were retrieved for screening, and 10 studies were included [2, 3, 8, 17–23] (Fig. 1).
Fig. 1.

PRIZMA diagram
We excluded the 2019 study by Hass et al. [24], which was included in a recent meta-analysis [14]. That study used a 'double trigger' instead of a dual trigger. Unlike the dual trigger, in which two agents are given concomitantly, the double trigger involves the administration of the GnRHa and hCG at 40 and 34 h, respectively, prior to oocyte retrieval.
Study characteristics
The 10 included trials were published between 2008 and 2022 and included 76,332 women each. The total number of participants was 1643, with 825 in the dual trigger group and 818 in the hCG trigger group.
All but two trials (Schachter et al. (2008), Decleer et al. (2014), Kim et al. (2014), Mahajan et al. (2016), Eftekhar et al. (2017), Alleyassin et al. (2018), Ali et al. (2020), Haas et al. (2020)) enrolled patients with an expected normal ovarian response. Factors indicating a normal ovarian response include younger age (range: 18–42 years), optimal body mass index (BMI; range: 18.0–30.0 kg/m2, categorized as normal to overweight), and laboratory test results for antral follicle count (AFC), FSH, and anti-Mullerian hormone (AMH) being within the reference range. Among these studies, one study excluded patients with poor ovarian reserve [23], one excluded patients with polycystic ovarian syndrome (PCOS) [18], one excluded patients with a lack of oocytes aspirated in the previous cycle [17], and one excluded patients with an increased risk of OHSS [20]. The remaining two studies included specific groups of patients. One study enrolled poor responders defined by Bologna criteria [2]. The other study included advanced-aged women (aged ≥ 35 years), some of which were predicted as poor responders according to the Bologna criteria. Therefore, subgroup analysis was conducted on the results of these two studies to evaluate the effect of dual trigger in comparison with hCG trigger. Table 1 summarizes the studies' inclusion and exclusion criteria.
Table 1.
The design of the included studies
| Study | Year | Study method | Method of randomization | Blinding | ART method | Inclusion criteria | Exclusion criteria | Intervention group protocol | Comparison group protocol |
|---|---|---|---|---|---|---|---|---|---|
| Schachter | 2008 | Prospective, randomized | Random number tables | Clinicians and IVF laboratory staff were blinded to treatment groups | IVF | Infertile patients needing IVF-ET who had failed at least 1 previous IVF-ET cycle on the GnRH agonist long protocol | Lack of oocytes aspirated in the previous cycle, BMI > 30 kg/m2 or < 18 kg/m2 | Triptorelin 0.2 mg + hCG 5000 U | hCG 5000 U |
| Decleer | 2014 | Prospective, randomized, controlled | Computer- generated random number list | The statistician who performed the statistical analysis was blinded | IVF/ICSI, fresh or frozen ET | Tubal or male infertility, BMI < 32 kg/m2, age ≤ 38 years, absence of major endocrinological pathology, 1–3rd IVF cycle | Azoospermia, female uterine abnormalities and major endocrinological disorders (e.g., PCOS); ovarian endometriotic cysts | Triptorelin acetate 0.2 mg (Gonapeptyl) + hCG 5000 IU | hCG 5000 IU |
| Kim | 2014 | Prospective, randomized | Sealed envelopes and computer-generated list |
The patients were not blinded The clinicians managing the cases were not blinded Lack of blinding of the investigators |
IVF or ICSI, Fresh ET | Infertile patients who were in good health, with normal thyroid, hepatic, and renal function | PCOS, metabolic disorders as hypothyroidism, DM, abnormal liver function | Decapeptyl 0.1 mg + recombinant hCG (Ovidrel) 250 μg | Recombinant hCG 250 μg + placebo |
| Mahajan | 2016 | Prospective, randomized | Simple randomization using sequentially numbered sealed envelopes | Unclear about the physicians. “The envelope was opened by our head nurse.” | IVF/ ICSI | Women aged 24–43 years with AMH < 4 ng/mL and AFC < 12 per ovary | High responders: AMH > 4 ng/mL and AFC/ovary > 12 to avoid OHSS risk with the hCG trigger | Leuprolide 1 mg + hCG 5000 IU | hCG 10,000 IU |
| Eftekhar | 2017 | Single-blinded, randomized, controlled | Randomization table | The physicians were blinded | IVF/ICSI, fresh ET | Normal responders aged ≤ 42 years and 18 < BMI < 30 kg/m2 | Presence of endocrine disorders such as DM, hyperprolactinemia, thyroid disorders, congenital adrenal hyperplasia, Cushing syndrome, PCOS, congenital uterine anomalies disorders, repeated implantation failure, day-3 FSH concentration ≥ 10 IU/L or AMH ≤ 1 ng/mL, and azoospermia | Triptorelin 0.2 mg + hCG 6500 IU | hCG 6500 IU |
| Alleyassin | 2018 | Randomized | Balanced block randomization technique and sealed envelopes | The researcher in charge of measuring the outcomes were blinded. The statistical analyzer was blinded | IVF/ICSI | Women aged 18–40 years, having a BMI between 18 and 35 kg/m2, day 3 FSH < 10 and regular menstrual cycles of 25–35 days, being candidate for IVF for any reasons such as unexplained infertility, tubal factor, and ovulation dysfunctions or mild male factor infertility | Day 3 FSH > 10, AMH < 1.1 ng/mL, being high risk of OHSS (> 16 follicles in the last ultrasound before the final oocyte induction), endocrine disorders such as DM, hyperprolactinemia, thyroid dysfunction, congenital adrenal hyperplasia, Cushing syndrome, PCOS, an anomaly confirmed using HSG or hysteroscopy in the uteri, severe male factor (azoospermia needed TESE or PESA), and history and signs of OHSS | Triptorelin 0.2 mg + hCG 5000 IU | hCG 10,000 IU |
| Ali | 2020 | Open-label, randomized, controlled | Computer-generated random table and sealed envelopes | Not mentioned | IVF/ICSI, fresh or frozen ET | Normal responders in GnRH antagonist ICSI cycles | Women aged > 40 years, azoospermia, and AMH < 1 ng /mL | Leuprolide acetate 1 mg + recombinant hCG 250 μg | 250 μg recombinant hCG |
| Haas | 2020 | Double-blind, randomized, controlled | Sealed envelope |
The patients were blinded The nurses, physicians and embryologists were all blinded |
IVF, fresh or frozen ET | Women aged 18–41 years, with BMI of 18–35 kg/m2, AMH > 1 ng/mL, AFC 6–20, and FSH < 20 IU/l undergoing one of their first 3 IVF cycle attempts | Poor ovarian reserve (AMH < 1 ng/mL), high risk of OHSS, BMI > 35 kg/m2, or moderate to severe endometriosis | Suprefact 0.5 mg + hCG 10000 IU (Pregnyl) | hCG (Pregnyl) 10000 IU + placebo |
| Maged | 2021 | Open-label, randomized, controlled | Automated Web-based randomization system | Open label, not blinded | IVF + fresh ET | Poor responders (1) age ≥ 40 years or presence of other risk factors for poor response (2) poor response in a previous cycle with production of ≤ 3 oocytes after stimulation with a conventional stimulation protocol (3) low ovarian reserve test AFC 5–7, or AMH 0.5–1.1 ng/mL | Ovarian cysts, endometriosis, hydrosalpinx, and endocrinologic disorders such as hyperprolactinemia, thyroid disorders, or adrenal disorders | Triptorelin 0.2 mg + hCG 10000 units | hCG 10000 units |
| Zhou | 2022 | Open-label, randomized, controlled | Random number table | Open-label, not blinded | IVF or ICSI, fresh or frozen ET | Advanced-age women (aged ≥ 35 years) | PCOS, hydrosalpinx, ovarian endometrioma, abnormal uterus or uterine cavity (adenomyosis, uterine malformations, endometrial polyps and intrauterine adhesions) or chromosome abnormalities (in either of the couple), patients who were at high risk of OHSS (E2 > 18,000 pmol/L and > 20 follicles with diameter > 10 mm on the trigger day), who underwent remedial ICSI after fertilisation failure, or who underwent preimplantation genetic test | Triptorelin 0.2 mg + hCG 2000 IU | hCG 6000 IU |
AFC antral follicle count, AMH: anti-Mullerian hormone, ART Assisted reproductive technologies, BMI body mass index, DM diabetes mellitus, E2 Estradiol, ET embryo transfer, FSH follicle-stimulating hormone, HSG hysterosalpingography, ICSI intracytoplasmic sperm injection, IVF-ET in vitro fertilization–embryo transfer, PESA percutaneous epididymal sperm aspiration, PCOS polycystic ovarian syndrome, TESE testicular sperm extraction
All studies used a GnRH antagonist for pituitary downregulation. After enrolment, the patients were randomized to receive either the dual trigger (intervention group) or hCG trigger (control group). In the dual trigger group, the patients received both the GnRHa (0.1–0.2 mg triptorelin, 1 mg leuprolide, or 0.5 mg buserelin) and hCG for final oocyte maturation. Seven studies used an equal hCG dose in the dual trigger and control groups, whereas the other three trials halved the hCG dose in the dual trigger group [3, 20, 21]. The design of each study is summarized in Table 1.
Risk of bias in studies
Figures 2, 3 and 4 display the assessment for risk of bias and a high risk of bias was noted in some studies.
Fig. 2.

Meta-analysis of studies reporting the following outcomes. A Number of retrieved oocytes; B Number of mature oocytes retrieved; C Biochemical pregnancy rate per cycle; D Clinical pregnancy rate per cycle; E Implantation rate per cycle; F Miscarriage rate per cycle; G Live birth rate per cycle
Fig. 3.

Subgroup analysis for clinical pregnancy rate after fresh ET and frozen–thawed ET. A Clinical pregnancy rate after fresh ET. B Clinical pregnancy rate after frozen–thawed ET
Fig. 4.
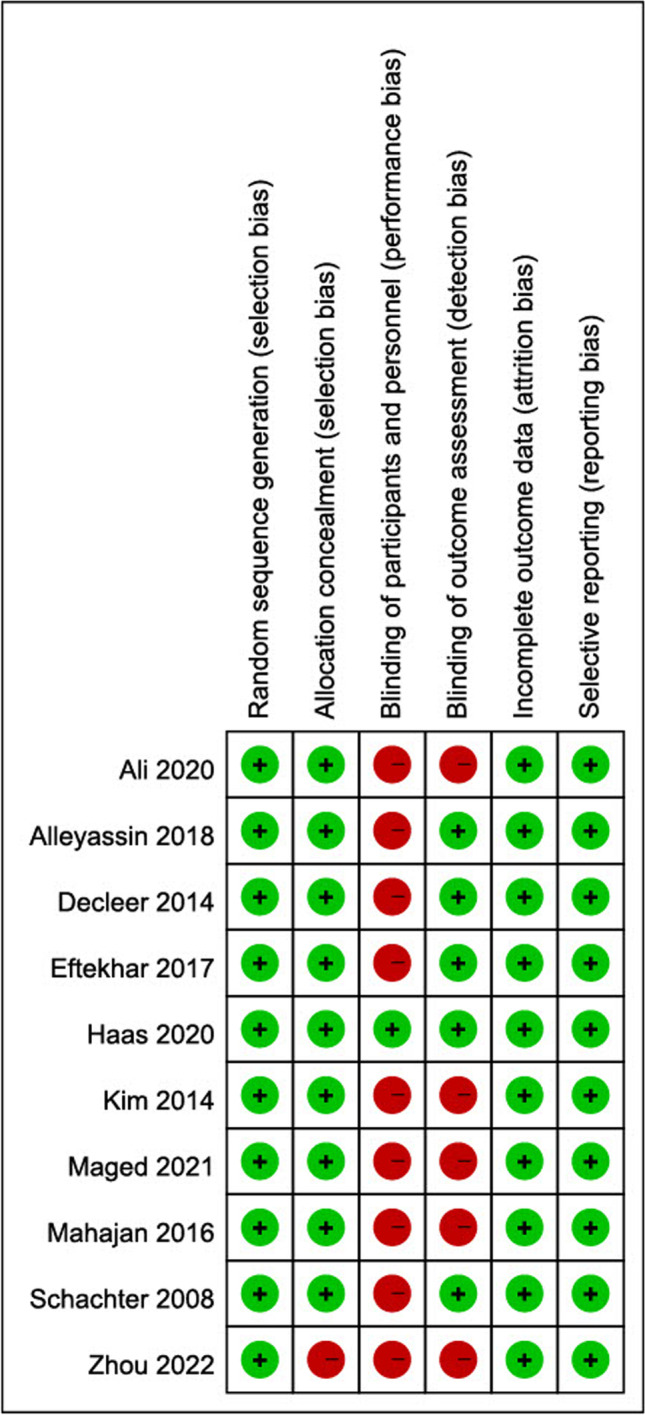
Results of the risk-of-bias analysis
Results of individual studies
The live birth rate was reported in four studies. The funnel plot indicated no publication bias for the primary outcome (Fig. 5.)
Fig. 5.

Funnel plot of the included studies for live birth rate
Results of the syntheses
Outcomes (Table 2 summarized the outcomes reported in each study).
Table 2.
Outcomes of the included studies
| Study | Year | Primary outcome | Outcomes reported | Outcomes not reported |
|---|---|---|---|---|
| Schachter | 2008 | Not mentioned | Total number of oocytes, implantation rate, clinical pregnancy rate per started cycle and per transfer, and miscarriage rate | Biochemical pregnancy rate, number of mature oocytes, live birth rate, and OHSS rate |
| Decleer | 2014 | Number of MII oocytes | Number of mature oocytes, total number of oocytes, implantation rate, clinical pregnancy rate, and OHSS rate | Biochemical pregnancy rate, miscarriage rate, and live birth rate |
| Kim | 2014 | Number of MII oocytes | Number of mature oocytes, total number of oocytes, miscarriage rate, clinical pregnancy per cycle, implantation rate, live birth rate, and OHSS rate | Biochemical pregnancy rate |
| Mahajan | 2016 | Number of mature oocytes; usable embryos | Number of mature oocytes, total number of oocytes, 2PN zygotes, and usable embryos | Chemical pregnancy rate, clinical pregnancy rate, miscarriage rate, implantation rate, live birth rate, and OHSS rate |
| Eftekhar | 2017 | Clinical pregnancy rate | Number of mature oocytes, total number of oocytes, clinical pregnancy rate, and miscarriage rate | Live birth rate and OHSS rate |
| Alleyassin | 2018, | Number of MII oocytes, clinical pregnancy, abortion, and implantation rates per cycle | MII oocytes number, biochemical/ clinical pregnancy, miscarriage rate, and implantation rate | Live birth rate and OHSS rate |
| Ali | 2020 | Number of MII oocytes | Number of mature oocytes, total number of oocytes, implantation rate, chemical /clinical pregnancy rate, live birth rate, and miscarriage rate | OHSS rate |
| Haas | 2020 | Number of mature oocytes | Number of mature oocytes, total number of oocytes, clinical pregnancy rate, implantation rate, live birth rate, and OHSS rate | Miscarriage rate and OHSS rate |
| Maged | 2021 | Number of oocytes retrieved | Number of mature oocytes, total number of oocytes, biochemical pregnancy rate, clinical pregnancy rate, and implantation rate | Miscarriage rate, live birth rate, and OHSS rate |
| Zhou | 2022 | Number of retrieved oocytes | Number of mature oocytes, total number of oocytes, clinical pregnancy rate, implantation rate, live birth rate, miscarriage rate, and OHSS rate | Nil |
Abbreviation: MII metaphase II, OHSS ovarian hyperstimulation syndrome
Number of retrieved oocytes
All 10 studies reported the number of retrieved oocytes.
The forest plot included the data of nine studies after omitting the data from the study by Haas et al. (2020) because the study indicated the means without standard deviations. The results suggested that the dual trigger significantly increased the number of oocytes retrieved (MD = 1.05 [0.43, 1.68], P = 0.0009, I2 = 48%, moderate evidence) (Figs. 2A, and 6). A subgroup analysis, including the two studies done on patients with poor ovarian response or advanced age, showed that dual trigger was associated with significantly increased number of retrieved oocytes in this patient group (MD = 0.62 [0.18, 1.06], P = 0.006, I2 = 0) (Fig. 8A).
Fig. 6.

GRADE pro
Fig. 8.

Subgroup analysis: meta-analysis for the following outcomes in patients with poor ovarian response or advanced age. A Number of oocytes retrieved; B Number of mature oocytes retrieved; C Biochemical pregnancy; D Clinical pregnancy; E Implantation rate; F Clinical pregnancy rate after fresh ET
Number of mature oocytes retrieved
Data regarding the number of mature oocytes (MII oocytes) retrieved were available in eight studies. The results indicated that dual triggering significantly increased the number of mature oocytes retrieved (MD = 0.82 [0. 84, 1.16], P < 0.000001, I2 = 11%, high evidence) (Fig. 2B). A subgroup analysis, including the two studies done on patients with poor ovarian response or advanced age, showed that dual trigger significantly increased the number of retrieved oocytes in this patient group (MD = 0.73 [0.38, 1.08], P < 0.001, I2 = 0%) (Fig. 8B).
Biochemical pregnancy rate per cycle
Five studies reported the biochemical pregnancy rate per cycle. The data regarding the outcomes of fresh and frozen–thawed ET in the study by Zhou et al. (2022) was pooled together to calculate the biochemical pregnancy rate. The analysis revealed that dual triggering did significantly increase the biochemical pregnancy rate (OR = 1.39 [1.03, 1.87], P = 0.03, I2 = 0%, moderate evidence) in ART treatment (Fig. 2C). A subgroup analysis, including the two studies done on patients with poor ovarian response or advanced age, suggested that dual trigger significantly increased the biochemical pregnancy rate in this patient group (OR = 1.84 [1.14, 2.96], P < 0.01, I2 = 0%) (Fig. 8C).
Clinical pregnancy rate
The clinical pregnancy rate per cycle was reported in nine studies. The data regarding pregnancy outcomes in fresh and frozen–thawed ET in the study by Zhou et al. (2022) were pooled together to calculate the clinical pregnancy rate. The dual trigger was associated with a significantly higher clinical pregnancy rate (OR = 1.46 [1.07, 1.98], P = 0.02, I2 = 45%, low evidence) (Fig. 2D). A subgroup analysis, including the two studies done on patients with poor ovarian response or advanced age, revealed that dual trigger was associated with a nonsignificant increase in the biochemical pregnancy rate in this patient group (OR = 1.77 [0.72, 4.32], P = 0.21, I2 = 0%) (Fig. 8D).
Implantation rate per cycle
The implantation rate was reported in six studies, which included data regarding the number of gestational sacs and the total number of transferred embryos. We excluded studies that only provided the percentage [8, 21, 22]. A nonsignificantly higher implantation rate was noted with the dual trigger than with the hCG trigger (OR = 1.35 [0.93, 1.95], P = 0.11, I2 = 54%, moderate evidence) (Fig. 2E). A subgroup analysis, including the two studies done on patients with poor ovarian response or advanced age, showed that there was no statistically significant difference between the dual trigger and hCG trigger in terms of implantation rate in this patient group (OR = 1.08 [0.67, 1.73], P = 0.75, I2 = 0%) (Fig. 8E).
Miscarriage rate per cycle
Five studies reported the miscarriage rate per cycle. The forest plot indicated that the dual trigger treatment was associated with a nonsignificantly decreased miscarriage rate per cycle compared with the hCG trigger (OR = 0.66 [0.33, 1.33], P = 0.25, I2 = 24%, moderate evidence) (Fig. 2F).
Live birth rate per cycle (primary outcome)
The live birth rate per cycle was reported in four studies. The data regarding live birth rates in fresh and frozen–thawed ET in the study by Zhou et al. (2022) were pooled together to calculate the live birth rate. The results suggested that the dual trigger was associated with a significantly higher live birth rate per cycle than the hCG trigger (OR = 1.61 [1.16, 2.25], P = 0.005, I2 = 21%, moderate evidence) (Fig. 2G).
OHSS rate per cycle
Only four studies reported OHSS rate per cycle [3, 18, 19, 23]. One study reported two OHSS cases in the dual trigger group and two in the hCG group [19], and there were no participants with OHSS in the other included studies. Meta-analysis showed that dual trigger was not associated with an increased OHSS rate (Fig. 7).
Fig. 7.

OHSS rate
Subgroup analysis
Clinical pregnancy rate after fresh ET
The clinical pregnancy rate per cycle after fresh ET was reported in eight studies.
Among these studies, Decleer et al. (2014), Ali et al. (2020), Haas et al. (2020), and Zhou et al. (2022) reported the clinical pregnancy rate per fresh ET, and all patients in the studies by Schachter et al. (2008), Kim et al. (2014), Eftekhar et al. (2017), and Maged et al. (2021) received fresh ET. The results suggested that dual triggering was associated with a significantly higher clinical pregnancy rate after fresh ET (OR = 1.37 [1.05, 1.79], P = 0.02, I2 = 44%, moderate evidence) (Fig. 3A). We further conducted meta-analysis on the subgroup of patients with poor ovarian response or advanced age, and it revealed that dual triggering significantly increased the clinical pregnancy rate after fresh ET in this special group of patients (OR = 2.84 [1.31, 6.12], P = 0.08, I2 = 0%) (Fig. 8F).
Subgroup analysis
Clinical pregnancy rate after frozen–thawed ET
In three studies, the clinical pregnancy rate after frozen–thawed ET was reported separately from the overall pregnancy rate, regardless of the ET method.
The data indicated that dual triggering was not associated with an increased pregnancy rate in this patient group (OR = 1.15 [0.64, 2.08], P = 0.73, I2 = 0%, moderate evidence) (Fig. 3B).
Discussion
The present meta-analysis revealed that dual triggering was associated with a significantly higher number of retrieved oocytes, number of mature oocytes, pregnancy rate, and live birth rate than the traditional hCG trigger. Moreover, subgroup analysis revealed that the beneficial effect of the dual trigger was significant in patients receiving fresh ET, but not in those receiving frozen–thawed ET. This finding suggests that dual triggering achieves a higher pregnancy rate not only by increasing the number and quality of oocytes but also by increasing endometrial receptivity for embryos in fresh transfer cycles.
Accumulating evidence indicates that dual triggering combines the advantages of the GnRHa and hCG. Several mechanisms have been proposed to explain the beneficial effect of the dual trigger, including the induction of the LH and FSH surge by the dual trigger treatment, mimicking the physiologic condition during spontaneous ovulation, and the direct action of the GnRHa on its receptors.
The GnRHa induces the FSH and LH surge from the pituitary gland. The LH surge has a synergistic effect with the hCG trigger on LH receptors [23]. FSH facilitates nuclear maturation and cumulus expansion by maintaining open gap junctions between the oocyte and cumulus cells. It also promotes the formation of LH receptors on luteinising granulosa cells [23]. In addition to its action mechanism involving the induction of the gonadotropin surge from the pituitary gland, GnRHa regulates ovulation through direct action on ovarian granulosa cells [7]. GnRHa also has beneficial effects on endometrial receptivity and preimplantation embryonic development [17, 25].
Nevertheless, the superiority of the dual trigger over the conventional hCG trigger remains controversial. A 2021 systematic review and meta-analysis including 10 RCTs and 16 observational studies revealed that dual triggering significantly improves clinical pregnancy rates, but no difference was observed in the number of retrieved oocytes and the number of mature oocytes [11]. However, another 2021 meta-analysis by Hu et al., including eight randomized trials, concluded that dual triggering significantly increased the number of oocytes retrieved, the number of mature oocytes retrieved, and clinical pregnancy compared with the hCG trigger [14]. Hu et al. also analyzed the impact of dual triggering on the implantation rate in four trials [17–19, 23]. They reported that after excluding the data from one study with low quality and significant heterogeneity, the meta-analysis revealed a significantly increased implantation rate with the dual trigger [18]. Our study drew a similar conclusion; that is, the dual trigger caused a significant increase in the number of oocytes retrieved, the number of mature oocytes retrieved, and the clinical pregnancy rate. Furthermore, in the subgroup analysis of poor responders or advanced-age patients, dual-trigger demonstrates superiority over hCG trigger in terms of the number of retrieved oocytes, mature oocytes, and the biochemical pregnancy rate. Another subgroup analysis indicated that dual trigger was associated with an increased clinical pregnancy rate after fresh ET but not after frozen–thawed ET. This finding may be because dual triggering probably increases the pregnancy rate by increasing endometrial receptivity, which does not benefit IVF with frozen–thawed ET.
The pooled data indicated that dual triggering was associated with a significantly increased live birth rate, which is consistent with the finding of a previous systematic review and meta-analysis [14]. However, that study included only three studies with this outcome, and the sample size was limited to 426 patients. We additionally included the trial by Zhou et al. [3], which increased the sample size to 673 patients. Nevertheless, more studies are warranted to analyze this important infertility treatment outcome.
The miscarriage rate in this meta-analysis did not increase. This result confirmed previous studies, which concluded that the concomitant administration of hCG compensates for the luteolytic effects of the GnRHa, providing extended luteal support [3, 26], and improves pregnancy rates [7].
The strength of our study is that only randomized trials were included in this meta-analysis.
This study has some limitations. First, incomplete reporting of methods in the included study protocols increases the risk of bias. More well-designed RCTs with larger sample sizes are warranted to obtain stronger evidence. Second, the heterogeneity of the participants and the study design also limited the certainty of our results. For instance, three of the included trials used a low dose of hCG (compared with the control group) in the dual trigger group [3, 20, 21], whereas the remaining seven trials used a regular dose of hCG (same as that in the control group) in the dual trigger group. Although no consensus has been reached regarding the optimal hCG dosing for dual triggering, Shapiro et al. examined the infertility treatment outcome and the risk of OHSS in high responders and concluded that 1000–2500 IU of hCG administered concomitantly with the GnRHa aids in oocyte maturation and provides more sustained support for the corpus luteum while not increasing the OHSS risk [27]. The doses of HCG used in the dual trigger group in all the trials included in our meta-analysis were higher than this minimum dose, thereby achieving beneficial results. However, only four studies reported the number of participants with OHSS, and some of our included studies specifically excluded patients with PCOS and those at risk for OHSS. As a result, even though our study demonstrated that dual trigger is not associated with an increase in OHSS rate, future research should focus on identifying the minimal dose of hCG that should be added to the GnRH trigger to optimise fresh cycle outcomes without increasing OHSS rates.
Conclusion
Our systematic review and meta-analysis revealed that the dual trigger was associated with a significantly higher number of retrieved oocytes, number of mature oocytes, clinical pregnancy rate, and LBR in IVF cycles than the hCG-only trigger. The beneficial effect of fresh ET cycles compared with frozen–thawed ET might be associated with increased endometrial receptivity. The result of our study suggests that a dual trigger followed by fresh ET can achieve a satisfactory clinical pregnancy rate and LBR. Delaying ET due to the concern of endometrial receptivity might not be needed.
The protocol of the meta-analysis was registered in the International Prospective Register of Systematic Reviews (PROSPERO, https://www.crd.york.ac.uk/PROSPERO/) on 2022/04/14, with the registration number of PROSPERO CRD42023417155.
Acknowledgements
This manuscript was edited by Wallace Academic Editing.
Authors’ contributions
THL and YLL designed and executed the study. LHH and YHL reviewed the literature, extracted the data and assessed the included studies' quality. LHH analyzed the data and wrote the manuscript. YYH and HJC took part in critical discussions. All authors scrutinised and revised the manuscript.
Funding
There was no financial or non-financial support for this study.
Data availability
All data analyzed in this study are included in this present manuscript.
Declarations
Conflict of interests
The authors declare no competing interest.
Footnotes
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
References
- 1.Griffin D, Benadiva C, Kummer N, Budinetz T, Nulsen J, Engmann L. Dual trigger of oocyte maturation with gonadotropin-releasing hormone agonist and low-dose human chorionic gonadotropin to optimize live birth rates in high responders. Fertil Steril. 2012;97(6):1316–1320. doi: 10.1016/j.fertnstert.2012.03.015. [DOI] [PubMed] [Google Scholar]
- 2.Maged AM, Ragab MA, Shohayeb A, Saber W, Ekladious S, Hussein EA, El-Mazny A, Hany A. Comparative study between single versus dual trigger for poor responders in GnRH-antagonist ICSI cycles: a randomized controlled study. Int J Gynaecol Obstet. 2021;152(3):395–400. doi: 10.1002/ijgo.13405. [DOI] [PubMed] [Google Scholar]
- 3.Zhou C, Yang X, Wang Y, Xi J, Pan H, Wang M, Zhou Y, Xiao Y. Ovulation triggering with hCG alone, GnRH agonist alone or in combination? A randomized controlled trial in advanced-age women undergoing IVF/ICSI cycles. Reproduction. 2022;37(8):1795–1805. doi: 10.1093/humrep/deac114. [DOI] [PubMed] [Google Scholar]
- 4.Russell DL, Robker RL. Molecular mechanisms of ovulation: co-ordination through the cumulus complex. Hum Reprod Update. 2007;13(3):289–312. doi: 10.1093/humupd/dml062. [DOI] [PubMed] [Google Scholar]
- 5.Alyasin A, Mehdinejadiani S, Ghasemi M. GnRH agonist trigger versus hCG trigger in GnRH antagonist in IVF/ICSI cycles: a review article. Int J Reprod Biomed. 2016;14(9):557–566. [PMC free article] [PubMed] [Google Scholar]
- 6.Abed WM, Selman MO. Outcome of GnRH Antagonist ICSI Cycles Triggered by GnRH Agonist Plus Recombinant hCG Versus Triggered With Recombinant hCG Alone in Fresh Autologous ICSI Cycle. Biochem Cell Arch. 2021;21(1):393–398. [Google Scholar]
- 7.Griffin D, Feinn R, Engmann L, Nulsen J, Budinetz T, Benadiva C. Dual trigger with gonadotropin-releasing hormone agonist and standard dose human chorionic gonadotropin to improve oocyte maturity rates. Fertil Steril. 2014;102(2):405–409. doi: 10.1016/j.fertnstert.2014.04.028. [DOI] [PubMed] [Google Scholar]
- 8.Eftekhar M, Mojtahedi MF, Miraj S, Omid M. Final follicular maturation by administration of GnRH agonist plus HCG versus HCG in normal responders in ART cycles: An RCT. Int J Reprod BioMed. 2017;15(7):429–434. [PMC free article] [PubMed] [Google Scholar]
- 9.Shapiro BS, Daneshmand ST, Garner FC, Aguirre M, Hudson C. Comparison of “triggers” using leuprolide acetate alone or in combination with low-dose human chorionic gonadotropin. Fertil Steril. 2011;95(8):2715–2717. doi: 10.1016/j.fertnstert.2011.03.109. [DOI] [PubMed] [Google Scholar]
- 10.Sloth A, Kjolhede M, Sarmon KG, Knudsen UB. Effect of dual trigger on reproductive outcome in low responders: a systematic PRISMA review and meta-analysis. Gynecol Endocrinol. 2022;38(3):213–221. doi: 10.1080/09513590.2021.2000962. [DOI] [PubMed] [Google Scholar]
- 11.Gayete-Lafuente S, Moreno-Sepulveda JA, Espinos JJ, Miguel CA. Dual trigger impact on reproductive outcomes of gnrh antagonist cycles for ivf a systematic review and meta-analysis. Fertil Steril. 2021;116(3, Supplement):e242–e243. doi: 10.1016/j.fertnstert.2021.07.653. [DOI] [Google Scholar]
- 12.Zhang Y, Guo X, Guo L, Chang HM, Shu J, Leung PCK. Outcomes comparison of IVF/ICSI among different trigger methods for final oocyte maturation: a systematic review and meta-analysis. Faseb J. 2021;35(7):e21696. doi: 10.1096/fj.202100406R. [DOI] [PubMed] [Google Scholar]
- 13.Gonzalez VG, Triana AM, Garcia IS, Nieto SO, Urrutia MC, Garcia IC, Gastanaga-Holguera T. Dual trigger vs. Conventional trigger outcomes in In Vitro Fertilization. Systematic review and meta-analysis. JBRA Assist Reprod. 2023;27(1):112–119. doi: 10.5935/1518-0557.20220035. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Hu KL, Wang S, Ye X, Zhang D, Hunt S. GnRH agonist and hCG (dual trigger) versus hCG trigger for follicular maturation: a systematic review and meta-analysis of randomized trials. Reprod Biol Endocrinol. 2021;19(1):78. doi: 10.1186/s12958-021-00766-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Ding N, Liu X, Jian Q, Liang Z, Wang F. Dual trigger of final oocyte maturation with a combination of GnRH agonist and hCG versus a hCG alone trigger in GnRH antagonist cycle for in vitro fertilization: a systematic review and meta-analysis. Eur J Obstet Gynecol Reprod Biol. 2017;218:92–98. doi: 10.1016/j.ejogrb.2017.09.004. [DOI] [PubMed] [Google Scholar]
- 16.Zegers-Hochschild F, Adamson GD, Dyer S, Racowsky C, de Mouzon J, Sokol R, Rienzi L, Sunde A, Schmidt L, Cooke ID, Simpson JL, van der Poel S. The international glossary on infertility and fertility care, 2017. Hum Reprod. 2017;32(9):1786–1801. doi: 10.1093/humrep/dex234. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Schachter M, Friedler S, Ron-El R, Zimmerman AL, Strassburger D, Bern O, Raziel A. Can pregnancy rate be improved in gonadotropin-releasing hormone (GnRH) antagonist cycles by administering GnRH agonist before oocyte retrieval? A prospective, randomized study. Fertil Steril. 2008;90(4):1087–1093. doi: 10.1016/j.fertnstert.2007.07.1316. [DOI] [PubMed] [Google Scholar]
- 18.Decleer W, Osmanagaoglu K, Seynhave B, Kolibianakis S, Tarlatzis B, Devroey P. Comparison of hCG triggering versus hCG in combination with a GnRH agonist: a prospective randomized controlled trial. Facts Views Vis Obgyn. 2014;6(4):203–209. [PMC free article] [PubMed] [Google Scholar]
- 19.Kim CH, Ahn JW, You RM, Kim SH, Chae HD, Kang BM. Combined administration of gonadotropin-releasing hormone agonist with human chorionic gonadotropin for final oocyte maturation in GnRH antagonist cycles for in vitro fertilization. J Reprod Med. 2014;59(1–2):63–68. [PubMed] [Google Scholar]
- 20.Mahajan N, Sharma S, Arora PR, Gupta S, Rani K, Naidu P. Evaluation of dual trigger with gonadotropin-releasing hormone agonist and human chorionic gonadotropin in improving oocyte maturity rates: a prospective randomized study. J Hum Reprod Sci. 2016;9(2):101–106. doi: 10.4103/0974-1208.183506. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Alleyassin A, Ghasemi M, Aghahosseini M, Safdarian L, Sarvi F, Almasi-Hashiani A, Hosseinimousa S, Najafian A, Esmailzadeh A. Final oocyte maturation with a dual trigger compared to human chorionic gonadotropin trigger in antagonist co-treated cycles: a randomized clinical trial. Middle East Fertil Soc J. 2018;23(3):199–204. doi: 10.1016/j.mefs.2018.01.001. [DOI] [Google Scholar]
- 22.Ali SS, Elsenosy E, Sayed GH, Farghaly TA, Youssef AA, Badran E, Abbas AM, Abdelaleem AA. Dual trigger using recombinant HCG and gonadotropin-releasing hormone agonist improve oocyte maturity and embryo grading for normal responders in GnRH antagonist cycles: randomized controlled trial. J Gynecol Obstet Hum Reprod. 2020;49(5):101728. doi: 10.1016/j.jogoh.2020.101728. [DOI] [PubMed] [Google Scholar]
- 23.Haas J, Bassil R, Samara N, Zilberberg E, Mehta C, Orvieto R, Casper RF. GnRH agonist and hCG (dual trigger) versus hCG trigger for final follicular maturation: a double-blinded, randomized controlled study. Hum Reprod. 2020;35(7):1648–1654. doi: 10.1093/humrep/deaa107. [DOI] [PubMed] [Google Scholar]
- 24.Haas J, Zilberberg E, Nahum R, Mor Sason A, Hourvitz A, Gat I, Orvieto R. Does double trigger (GnRH-agonist + hCG) improve outcome in poor responders undergoing IVF-ET cycle? A pilot study. Gynecol Endocrinol. 2019;35(7):628–630. doi: 10.1080/09513590.2019.1576621. [DOI] [PubMed] [Google Scholar]
- 25.Orvieto R, Meltzer S, Rabinson J, Zohav E, Anteby EY, Nahum R. GnRH agonist versus GnRH antagonist in ovarian stimulation: the role of endometrial receptivity. Fertil Steril. 2008;90(4):1294–1296. doi: 10.1016/j.fertnstert.2007.10.022. [DOI] [PubMed] [Google Scholar]
- 26.Beckers NGM, Macklon NS, Eijkemans MJ, Ludwig M, Felberbaum RE, Diedrich K, Bustion S, Loumaye E, Fauser BCJM. Nonsupplemented Luteal Phase Characteristics after the Administration of Recombinant Human Chorionic Gonadotropin, Recombinant Luteinizing Hormone, or Gonadotropin-Releasing Hormone (GnRH) Agonist to Induce Final Oocyte Maturation in in Vitro Fertilization Patients after Ovarian Stimulation with Recombinant Follicle-Stimulating Hormone and GnRH Antagonist Cotreatment. J Clin Endocrinol Metab. 2003;88(9):4186–4192. doi: 10.1210/jc.2002-021953. [DOI] [PubMed] [Google Scholar]
- 27.Shapiro BS, Daneshmand ST, Garner FC, Aguirre M, Thomas S. Gonadotropin-releasing hormone agonist combined with a reduced dose of human chorionic gonadotropin for final oocyte maturation in fresh autologous cycles of in vitro fertilization. Fertil Steril. 2008;90(1):231–233. doi: 10.1016/j.fertnstert.2007.06.030. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
All data analyzed in this study are included in this present manuscript.