

Abstract
Aim: Chronic kidney disease (CKD) is becoming a great concern, especially in developing countries and SNHL among patients with CKD is considerably higher than general population. So, current study aims evaluation and assessment of degree of hearing loss in chronic kidney disease patients using pure tone audiogram and correlation of hearing loss with its contributing factors. Materials and methods:70 patients with CKD were included in this prospective observational cross sectional study performed in tertiary care hospital. A detailed history; general physical, otological examination, blood investigation was done.CKD staging was done using KDIGO guidelines and hearing assessment using pure tone audiometry. Hearing loss association with CKD and contributing factors were studied. Result: Out of 70 participants, SNHL was seen in twenty one participants. Hearing loss was present in 3 out of 22 participants of CKD-3; 6 out of 12 participants of CKD-4 and 12 out of 15 participants of stage CKD-5. A statistically significant association of hearing loss was found with CKD stage, albuminuria, hemodialysis, hypertension and other factors. Discussion: Since hearing impairment may well have a negative impact on the social function of an affected individual, the use of pure tone audiogram to monitor CKD patients should be considered as a routine procedure. Patients with CKD would benefit from early detection of hearing loss which will allow for early rehabilitative measures to be taken.
Keywords: Chronic Kidney Disease, Sensorineural Hearing Loss, Pure Tone Audiogram
Introduction
The commonest form of hearing disorder in developing countries is loss of hearing sensitivity [1]. Hearing loss in adults not only leads to social isolation but also poor quality of life [2].
Chronic kidney disease (CKD) is becoming a great concern, especially in developing countries where most patients present in the late stages of the disease [3]. Hearing loss, tinnitus, and vertigo are the most common otologic symptoms in patients with CKD. There are ultrastructural, immunological and pathophysiological similarities between the nephron of kidney and stria vascularis of cochlea [4].
SNHL(sensorineural hearing loss) among patients with CKD is considerably higher than general population and varies from mild hearing disturbance found in 77% cases to moderately severe hearing loss in 46% of the tested patients [3]. Presence of hearing loss and estimation of type and degree constitute one of the most common method used to investigate the effects of renal disease on the auditory system.
So current study was designed to evaluate and assess the degree of hearing loss in chronic kidney disease patients using pure tone audiogram and correlation of hearing loss with its contributing factors.
Materials and Methods
The prospective observational cross sectional study was performed in a tertiary care hospital, included 70 chronic kidney disease patients with no history of diabetes, noise exposure, renal transplantation and ear- related complaints prior to the development of disease. Patients having congenital hearing loss, middle ear disorder, a family history of hearing loss, age below 15 years and above 60 years were excluded.
A written fully explained consent stating the voluntary participation of subjects in the study was undertaken before the enrolment of the study subject. After taking the detailed history(personal, family ,disease), patients were subjected to general physical examination, otoscopic examination of ear was done to see the status of tympanic membrane and hearing test by tuning fork test (256 Hz, 512 and 1024 Hz).
The blood and urine investigations were performed alongwith the ultrasonography of abdomen/KUB of each patient. In this study, eGFR (mL/min/1.73m2) for the cases were calculated using the Chronic Kidney Disease Epidemiology Collaboration (CKD-EPI) Eq. 5 as follows [5]:
eGFRcr = 141 x min(Scr/κ, 1)α x max(Scr/κ, 1)-1.209 × 0.9938Age x 1.018 [if Female
where:
Scr = standardized serum creatinine in mg/dL.
κ = 0.7 (females) or 0.9 (males).
α = -0.329 (female) or -0.411 (male).
min(Scr/κ, 1) is the minimum of Scr/κ or 1.0.
max(Scr/κ, 1) is the maximum of Scr/κ or 1.0.
Age (years).
The eGFR obtained was classified into five stages of CKD : ≥90, 60–89, 30–59, 15–29, and < 15 mL/min/1.73m2, according to the different stages of CKD defined by the Kidney Disease: Improving Global Outcomes (KDIGO) guideline [6].
The cases underwent general physical examination followed by examination of ear, nose and throat to rule out any structural deformity or existing pathology; audiometric assessment using pure tone audiometry (PTA) was done using a Pure Tone Audiometer model AUL 12,096 audiometer of Labat company in a sound proof room, to identify hearing threshold levels in patients to determine the degree of hearing loss.
Data analysis was done using licensed SPSS software version 21.0 (Chicago, Illinois). Independent t-test and ANOVA test were used to compare the continuous variable and chi-square test was used for categorical variables. A p-value < 0.05 was considered as statistically significant.
Results
Mean age of study participants was 35.6 ± 11.4 years. Maximum (19 patients) were in age of 21–30 years age group followed by 18 in age group of 31–40 years. Amongst them 46 (65.7%) were male and 24 (34.3%) were female participants.
CKD
Out of the 70 participants, maximum 22 participant were having CKD-3 stage,21 patients were in CKD-2 stage, 12 patients had CKD-4 and 15 patients had CKD-5 stage.(Table 1) Mean duration of CKD disease amongst the study participants was 1.1 ± 0.5 years.
Table 1.
Distribution of participants according to CKD stage
| Stage | Frequency | Percent (%) |
|---|---|---|
| CKD-2 | 21 | 30.0 |
| CKD-3 | 22 | 31.4 |
| CKD-4 | 12 | 17.1 |
| CKD-5 | 15 | 21.4 |
| Total | 70 | 100.0 |
Hearing Loss
In our study, average right ear AC and BC was 29.9 ± 12.9 dB and 21.4 ± 10.9 dB respectively. Average left ear AC and BC was 28.6 ± 11.7 dB and 21.3 ± 10.7 dB respectively. Hearing loss was seen in twenty one (30%) participants which was of sensorineural type. Out of which 2 had bilateral and rest had unilateral SNHL. Amongst the 21 cases, 14 had mild followed by 5 having moderate and 2 patients showed severe degree of hearing loss.
Association of CKD and Hearing Loss
Participants in CKD-2 stage did not show any type of hearing loss. Hearing loss was present in 3 out of 22 participants (13.63%) of CKD-3; 6 out of 12 participants (50%) of CKD-4 and 12 out of 15 participants (80%) of stage CKD-5 stage.
In our study, a statistically significant association of hearing loss was found with CKD stage. Hearing loss increase rate was directly proportional to the CKD stage.(Table 2).
Table 2.
Association of hearing loss with CKD Stage
| CKD stage | No Hearing loss | Hearing loss | p-value | ||
|---|---|---|---|---|---|
| Count | % | Count | % | ||
| CKD-2 | 21 | 42.9% | 0 | 0.0% | |
| CKD-3 | 19 | 38.8% | 3 | 14.3% | |
| CKD-4 | 6 | 12.2% | 6 | 28.6% | |
| CKD-5 | 3 | 6.1% | 12 | 57.1% | |
| Total | 49 | 100.0% | 21 | 100.0% | 0.0001 |
Factors Affecting CKD and Hearing Loss
Lab Investigations :
Serum urea and creatinine level were elevated, Haemoglobin was found to be low and RBS (random blood sugar) was within normal range in most participants. The association of these levels with hearing loss was found to be significant.(Table 3).
Table 3.
Comparision of various laboratory parameter with hearing loss
| Laboratory parameter | Hearing loss | ||||
|---|---|---|---|---|---|
| No | Yes | p- value |
|||
| Mean | SD | Mean | SD | ||
| Sr Urea (mg/dl) | 111.3955 | 48.35447 | 202.3810 | 71.89470 | 0.0001 |
|
Sr Creatinine (mg/dl) |
5.5747 | 3.03670 | 9.7048 | 2.33118 | 0.0001 |
| RBS (mg/dl) | 97.7857 | 13.68231 | 101.1429 | 14.45090 | 0.358 |
| Serum Electrolyte (mMol/dl) | |||||
| Na + | 136.00 | 5.489 | 135.52 | 3.983 | 0.721 |
| K+ | 4.4855 | 0.69800 | 4.6129 | 0.94582 | 0.533 |
| Cl - | 102.71 | 4.916 | 103.57 | 4.935 | 0.507 |
| Complete Blood Count | |||||
| Hb | 8.85 | 2.307 | 7.69 | 1.789 | 0.047 |
| TLC | 8593.67 | 3261.774 | 8495.71 | 3991.571 | 0.915 |
| TPC | 6818.2071 | 2088.6 | 2859.1162 | 1887.79 | 0.425 |
Anaemia and Hypertension:
Out of the 70 participants, anaemia was present in 46 (65.7%) and hypertension was present in 56 (80%) participants. 95.2% of the cases having hearing loss also had hypertension which was significant. Mean Hb among all study participants was 8.48 ± 2.21 gm/dl and mean Hb among 21 patients of HL was 7.79 ± 1.78 gm/dl.(Fig. 1).
Fig. 1.
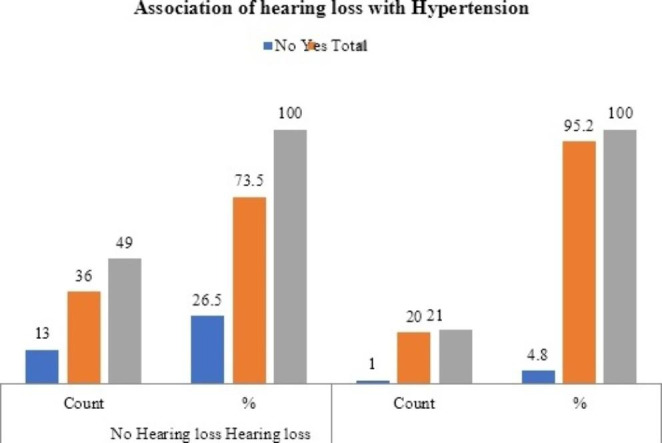
Bar diagram showing association of hearing loss with hypertension
Kidney Size :
The mean right and left side kidney size was 3242.2 ± 783.8 mm2 and 3349.4 ± 715.9 mm2 respectively. Amongst 21 patients having hearing loss mean kidney size of right and left kidney was 2543.33 ± 666.38 mm2 and 2644.76 ± 563.792 mm2 which was significantly reduced as compared with CKD patients without hearing loss .(Fig. 2).
Fig. 2.
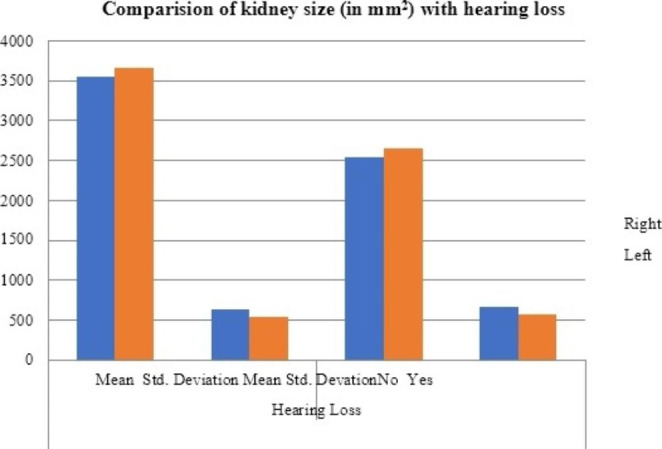
Bar diagram showing comparision of kidney size with hearing loss
Albuminuria and Hemodialysis:
In our study, maximum 27 had 2 + followed by 16 had 3 + albuminuria. Almost all patients (98.57%) had albuminuria in urine routine microscopy except one patient. Amongst the 21 cases having hearing loss all had 2 + and above albuminuria making it a significant factor.
43 cases out of 70 and 85.7% of the cases having hearing loss had undergone hemodialysis for the management of CKD. So the association of hypertension and hearing loss was also found to be significant.(Fig. 3).
Fig. 3.

Bar diagram depicting association of hearing loss with haemodialysis
Discussion
Chronic kidney disease (CKD) is considered a serious public health issue due to its increased prevalence among adults. Many research have shown a relation between the ear and the kidney in terms of physiology and ultrastructure [4].
Hearing loss are mostly acquired but preventable, hence exploration of risk factors is of great significance. Various complications associated with CKD result in poor quality of life, and hearing loss is one of them [7].
So early detection and management of CKD will not only save the kidneys the patients but will also improve quality of life by preventing the complications, hearing loss being one of them.
In the present study mean age of study participants was 35.6 ± 11.4 years. Amongst them 46 (65.7%) were male and 24 (34.3%) were female participants. A similar male preponderance was seen in study done by Mukhtar S et al. [8] (58% males) and Reddy EK et al. [9] (71.5% males).
CKD and Hearing Loss:
In our study, out of the 70 participants, maximum 22 participant were having CKD-3 stage, 21 patients were in CKD-2 stage, 12 patients had CKD-4 and 15 patients had CKD-5 stage. Mean duration of CKD disease amongst the study participants was 1.1 ± 0.5 years.
Average right ear AC and BC was 29.9 ± 12.9 dB and 21.4 ± 10.9 dB; and average left ear AC and BC was 28.6 ± 11.7 dB and 21.3 ± 10.7 dB respectively. Hearing loss was seen in twenty one (30%) participants which was of sensorineural type. Amongst the 21 cases, 14 had mild followed by 5 having moderate and 2 patients showed severe degree of hearing loss.
Bazzi C and colleagues [10] (1995) revealed that incidence of SNHL among patients with CRF was considerably higher than general population. It varied from mild HL found in 77% cases to moderately severe HL in 46% and most of the HL was in high frequencies.
Peyvandi A et al. [11] (2013) studied seventy (37 male, 33 female) CRF patients out of which 23 patients (46%) had hearing loss which was Sensory–neural hearing loss mostly involving higher frequencies. Mean PTA result in this group of patients was 21.46 (7.5–45.63) dB.
In 2016, Rezwanur Rahman and colleagues [12] studied 55 CKD patients and a control group of 50 people and found that, prevalence of SNHL in CKD patients was 54% and in control subjects was 16%. In CKD patients, 10% had mild loss of hearing impairment, 30% had moderate loss, severe loss was present in 40% patients and 20% had profound loss. Although control group was not taken in our study, but prevelance of SNHL was high in ours too.
Pushpa K.C. et al. [13] (2021) concluded that the proportion of SNHL in CRF patients was found to be 40% (46 out of 115 patients). Out of this, 13% had slight, 13% mild, 8.7% moderate, 3.5% moderately severe, 0.9% severe and 0.9% profound degree of HL. At high frequencies, 66.9% had SNHL which shows that most of the patients had high frequency hearing loss. SNHL was bilateral and symmetrical in majority of the cases (44 out of 46 patients). Even in our study almost all cases had SNHL.
Similar study was done by Mukhtar S et al. [8] (2020), in which majority of the patients had stage 5 renal disease, followed by stage 4 and stage 3 chronic renal disease. Stage III CKD was present in 9, stage IV in 13 and Stage V in 28 patients. 12 patients (24%) out of 50 participants had SNHL. PTA threshold was below or equal to 35 dB in 4 patients, equal to 45 dB in 3 patients and 45–60 dB in 5 patients .
Fufore MB et al. [14] (2020) revealed that hearing loss was present in 69 (57.5%) ears out of 120 ears in the patient group, whereas in the control group, the hearing loss was present in 25 (20.8%) ears. Of the 69 ears with hearing loss among the patients, majority (67, 97.1%) had SNHL and 2 (2.9%) had mixed hearing loss. Of the 25 ears with hearing loss among the controls, 24 (96.0%) had SNHL and only 1 (4.0%) had mixed hearing loss. However this study was case control study compare to our prospective observational study.
Association
In our study, a statistically significant association of hearing loss was found with CKD stage, albuminuria, hemodialysis and hypertension. All 21 patients who had hearing loss also had some degree of albuminuria and 20 patients (95.2%) out of above 21 patients were known case of hypertension. Out of 21 patients who had hearing loss, 18 patients (85.7%) were on hemodialysis treatment for their disease management.
A statistically significant high serum urea and serum creatinine was found among the patients with hearing loss in the present study. As most patients were under haemodialysis, the urea and creatinine values may not be reflective of the severity or stage of the disease.
The study also revealed that low Hb and reduced kidney size was found among the patients with hearing loss which was statistically significant as discussed in results.
Pushpa K.C. et al. [13] revealed significant positive association between HL and cycles of HD but no significant association found between hearing loss and primary hypertension. It was found that as the duration of CRF increased, the occurrence of SNHL also increased.
In a study by Seo et al. [15] (2015) among various risk factors of CKD which can be associated with hearing loss, it was found that each increase of serum creatinine level or blood pressure level was significantly associated with an increase in hearing threshold (p value was significant and was < 0.01).
Conclusion
Hearing is the main key to communication with society and environment. Hearing loss disables a person in every aspect of life. SNHL in CKD can be prevented if detected in early stage. In our study 30% of the CKD patients were found to have hearing loss. The use of audiological tests (non invasive) to monitor CKD patients should be considered as a routine procedure.
CKD stage, albuminuria, hemodialysis and hypertension were significantly associated factors with hearing loss in this study. Knowledge of associated factors in a disease not only fastens the management but can also be kept as a measure in routine check-ups and its prevention.
Funding
None.
Declarations
Conflict of Interest
Authors declare that we have no potential conflict of interests.
Compliance with Ethical Standards
Yes.
Footnotes
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
References
- 1.World Health Organization, deafness and hearing loss- fact sheet – April,2021 available at https://www.who.int/news-room/fact-sheets/detail/deafness-and-hearing-loss
- 2.Mick P, Kawachi I, Lin FR. The association between hearing loss and social isolation in older adults. Otolaryngol Head Neck Surg. 2014;150:378–384. doi: 10.1177/0194599813518021. [DOI] [PubMed] [Google Scholar]
- 3.Okoye OA, Oviasu E, Ojogwu L. Prevalence of chronic kidney disease and its risk factors amongst adults in a rural population in Edo state, Nigeria. J US Chi Med Sci. 2011;8:471–481. [Google Scholar]
- 4.Arnold W. Inner ear and renal diseases. Ann Oto Rhino Lary. 1984;112(Suppl):119–124. doi: 10.1177/00034894840930S420. [DOI] [PubMed] [Google Scholar]
- 5.Levey AS, Stevens LA, Schmid CH, Zhang YL, Castro AF, Feldman HI, et al. A new equation to estimate glomerular filtration rate. Ann Intern Med. 2009;150:604–612. doi: 10.7326/0003-4819-150-9-200905050-00006. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Kidney Disease Improving global outcomes (KDIGO) CKD Work Group. KDIGO 2012 clinical practice guideline for the evaluation and management of chronic kidney disease. Kidney Int Suppl. 2013;3:1–150. [Google Scholar]
- 7.Nordvik Ø, Laugen Heggdal PO, Bra¨nnstro¨m J, Vassbotn F, Aarstad AK, Aarstad HJ. Generic quality of life in persons with hearing loss: a systematic literature review. BMC Ear Nose Throat Disord. 2018;18:1. doi: 10.1186/s12901-018-0051-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Mukhtar S, Thomas J, Ghate G, Khan R. Evaluation of hearing in patients of chronic renal failure. Int J Otorhinolaryngol Head Neck Surg. 2020;6:1069–1073. doi: 10.18203/issn.2454-5929.ijohns20202060. [DOI] [Google Scholar]
- 9.Reddy EK, Prakash SDR, Ramakrishna MG. Proportion of hearing loss in chronic renal failure: our experience. Indian J Otol. 2016;22(1):4–9. doi: 10.4103/0971-7749.176503. [DOI] [Google Scholar]
- 10.Bazzi C, Venturini C, Arrigo GD, Amico G. Hearing loss in short and long term haemodialyzed patients. Nephrol Dial Transpl. 1995;10:1865–1868. [PubMed] [Google Scholar]
- 11.Peyvandi A, Roozbahany NA. Hearing loss in chronic renal failure patient undergoing hemodialysis. Indian J Otolaryngol Head Neck Surg. 2013;65:537–540. doi: 10.1007/s12070-011-0454-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Rezwanur Rahman N, Akhtar A, Khanam, Alam MR. ―Prevalence and patterns of hearing loss among chronic kidney disease of various stages in bangladeshi patients.‖. Am J Med Sci Med. 2016;4(3):53–58. [Google Scholar]
- 13.Pushpa KC, Jayaprabha S, Chippi Mohan N, Gracious C, Satheesh S. Sensorineural hearing loss in chronic renal failure patients in a tertiary care centre. Int J Health Clin Res. 2021;4(9):261–267. [Google Scholar]
- 14.Fufore MB, Kirfi AM, Salisu AD, Samdi TM, Abubakar AB, Onakoya PA. Stage of chronic kidney disease and cochlear function: a cross-sectional survey. Niger Postgrad Med J. 2020;27:122–126. doi: 10.4103/npmj.npmj_148_19. [DOI] [PubMed] [Google Scholar]
- 15.Seo YJ, Ko SB, Ha TH, Gong TH, Bong JP, Park DJ, Park SY (2015 Sep) Association of hearing impairment with chronic kidney disease: a cross-sectional study of the korean general population. BMC Nephrol 16:16:154 [DOI] [PMC free article] [PubMed]