

Abstract
Reinke oedema is a benign condition due to fluid collection within subepithelial space of the true vocal fold. This phenomenon is predisposed by chronic smoking, alcohol consumption and contribution of laryngopharyngeal reflux. Although benign, it may be life threatening when bilateral vocal folds are affected causing airway obstruction. In this report, awake tracheostomy was performed for a 65- year- old lady with stridor secondary to severe Reinke oedema. The importance of establishing a definitive airway is highlighted here in securing a difficult airway.
Supplementary Information
The online version contains supplementary material available at 10.1007/s12070-023-03714-4.
Keywords: Reinke, Tracheostomy, Stridor
Introduction
Reinke oedema is a benign condition of the vocal fold due to fluid collection in the superficial layer of lamina propria, also known as Reinke space [1]. It appears as diffuse or polypoidal oedema involving unilateral or bilateral vocal folds. In milder case, patients present with varying degrees of dysphonia. Dyspnea due to severe bilateral vocal cord oedema causing upper airway obstruction is a very rare presentation. To date, only one literature reported about Reinke oedema which required tracheostomy due to severe airway obstruction [2]. Here, a case of stridor secondary to severe Reinke oedema is presented and the experience in managing the patient is discussed.
Case Report
A 65- year- old lady with underlying hypertension and dyslipidemia, who is a chronic smoker with more than 30 packs years, presented to emergency department with sudden worsening of dyspnea and stridor for a week. She had hoarseness for the past 10 years that worsened gradually over the years.
On examination, she had biphasic stridor and appeared mildly tachypnoeic. A flexible nasopharyngolaryngoscope was done, showed polypoidal mass at the glottic level, obstructing her airway. An emergency tracheostomy under local anaesthesia was performed in order to secure her airway. Subsequently, direct laryngoscopy was carried out and showed bilateral oedematous vocal folds (Fig. 1A). The oedematous vocal folds epithelium was incised, and mucosal flap was raised. Excess mucosa was removed and fluid was aspirated followed by re- draping of the remained mucosa. The excised mucosa was sent for histopathological examination (HPE) which reported as mild to moderate squamous dysplasia with no malignancy seen (Fig. 2).
Fig. 1.

A Reinke oedema over right (triangle) and left (arrow) vocal folds during first operation after tracheostomy done. B Indirect laryngoscopic examination during follow up after decannulation
Fig. 2.
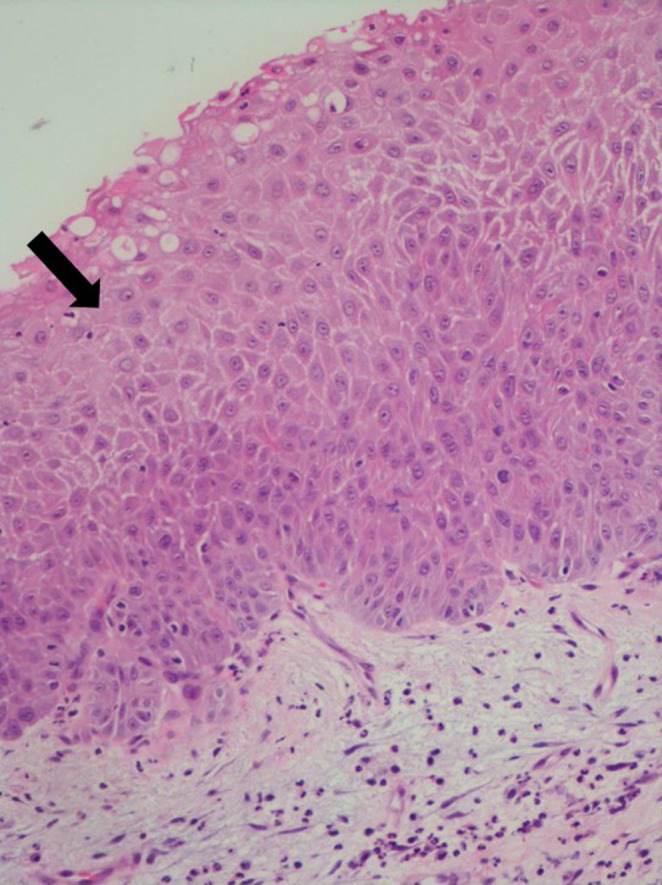
Mild to moderate dysplasia over lower one third to half of epithelial layer (arrow)
After the operation, she was advised for smoking cessation and sent home with tracheostomy tube. The patient was followed up monthly to examine her vocal folds and tracheostomy wound. After 6 months, her vocal folds appeared normal and she was successfully decannulated. She is now well on regular follow up with surveillance indirect laryngoscopic examination during each visit (Fig. 1B). She has a no hoarseness now and no breathiness on conversation.
Discussion
Reinke oedema, also called polypoid corditis, is a common benign condition of the true vocal folds as the result of oedema in the superficial layer of lamina propria3. It may be due to changes in the vessel permeability causing extravasation of fluid from capillary into Reinke space, or accumulation of blood because of poor lymphatic drainage with chronic inflammation [1, 3]. It usually involves bilateral vocal folds in an asymmetry fashion.
The clinical manifestations of Reinke oedema are dependent on its severity, ranging from dysphonia of varying degree to acute upper airway obstruction. Clinically, a few grading systems were proposed based on the morphology of vocal folds (Table 1) [4–6]. The present case had a grade 4 Reinke oedema based on the commonly used grading system that was introduced by Savic et al. [3]. Her oedema was very severe that no glottic airway can be visualized during flexible laryngoscopic examination. The patient was tachypnoeic with audible stridor, thus tracheostomy was performed under local anaesthesia to secure her airway. Awake fiberoptic intubation was deferred as the airway was not seen and it may worsen the airway due to laryngospasm or bleeding if the procedure failed.
Table 1.
Different grading system for Reinke’s oedema
| Author | Grade | Appearance |
|---|---|---|
| Savic et al. [4] |
1 2 3 4 |
Very early lesion that is not detectable during indirect laryngoscopy, only detectable using microscope and shows blunt amplitudes during stroboscopy Severe chronic oedema Large, transparent oedema Hyperemic, fluid- filled oedematous spaces |
| Tan et al. [5] |
1 2 3 4 |
Minimal polypoid degeneration of the vocal fold up to 25% of the glottic airway Expanded polypoid lesion occupying 25–50% of the glottic airway Expanded polypoid lesion, 50–75% of the glottic airway Obstructive lesion regardless of laterality, occupying beyond 75% of the glottic airway |
| Yonekawa et al. [6] |
I II III |
Involves anterior third of the vocal fold Involves anterior two third of the vocal fold Involves entire vocal fold |
Reinke oedema is strongly associated with chronic cigarette smoking. Other etiologies include vocal abuse and laryngopharyngeal reflux [7]. It is more common in female than male, frequently between age of 40 to 60 years old [1, 8]. There is no specific histological appearance for Reinke oedema. However, dysplasia can be seen occasionally with the incidence between 0 and 3% [3]. The patient in the present case had been a chronic smoker with 30 packs year, predispose the vocal folds to develop a premalignant change as reported in the HPE. The affected vocal folds eventually returned to normal after the surgery and cessation of cigarette smoking.
The management of Reinke oedema depends on its severity. In mild cases with only dysphonia, the treatment begins with elimination of the predisposing risk factors and voice therapy. Steroid injection is also one of the treatment options [9]. In more severe cases with airway obstruction, securing the airway is the priority that should be followed by surgery to excise the oedematous mucosa and remove the gelatinous fluid. The choice either intubation with a small endotracheal tube or tracheostomy under local anaesthesia would depends on the remaining visualized glottic airway and the availability of senior anaesthetist and ORL surgeon. As in this patient, tracheostomy under local anaesthesia was opted because the glottic airway was totally obscured by the oedematous and polypoidal mucosa. Manipulation of the airway during intubation may trigger laryngospasm or bleeding that would further compromise the airway. The goals of the endolaryngeal surgery is to reduce oedema and prevent stiff vocal folds due to scarring that would lead to undesirable life- long hoarseness [3]. The recommended surgery is by microflap techniques that include reduction of the gelatinous matrix, excision of the excess mucosa and redraping of the microflap, which was done for this patient.
Conclusion
Severe Reinke edema with total obstruction of the glottal airway is a life-threatening condition that requires emergency tracheostomy under local anaesthesia. A precision technique of endolaryngeal microsurgery after securing the airway should aimed at enlarging the glottal airway and preservation of voice following the healing process. Although it is known to be a benign lesion, concomitant premalignant lesion is not uncommon especially in a chronic smoker.
Electronic Supplementary Material
Below is the link to the electronic supplementary material.
Declarations
Conflict of Interest and Funding
None
Footnotes
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
References
- 1.Mohyuddin A, Sandhu G. Reinke’s Oedema presenting as Stridor: implications for otolaryngologists in difficult Airway. Int J Otol Head Neck Surg. 2017;6:11–15. [Google Scholar]
- 2.Honda K, Haji T, Satoh S, Tamura T, Motoyoshi K, Ozawa K, et al. Use of the Microdebrider for Reinke’s Edema compromising the Airway Compromise. Prac Oto Rhino Laryn. 2008;101:791–794. doi: 10.5631/jibirin.101.791. [DOI] [Google Scholar]
- 3.Tavaluc R, Tan-Geller M. Reinke’s Edema. Otolaryngol Clin North Am. 2019;52:627–635. doi: 10.1016/j.otc.2019.03.006. [DOI] [PubMed] [Google Scholar]
- 4.Savic D. Characteristiques morphologiques et histopathologiques de l’ oedema chronique des cordes vocales. J FR Otorhinolaryngol Audiophonol Chir Maxillofac. 1976;25:19–20. [PubMed] [Google Scholar]
- 5.Tan M, Bryson PC, Pitts C, Woo P, Benninger MS. Clinical grading of Reinke’s edema. Laryngoscope. 2017;127(10):2310–2313. doi: 10.1002/lary.26647. [DOI] [PubMed] [Google Scholar]
- 6.Yonekawa H. A clinical study of Reinke’s edema. Auris Nasus Larynx. 1998;15(1):57–78. doi: 10.1016/S0385-8146(88)80010-5. [DOI] [PubMed] [Google Scholar]
- 7.Yun SH, Park JC, Kim KW, Lim GC. Airway management in a patient with Reinke’s edema- A case report. Anesth Pain Med. 2015;10:317–320. doi: 10.17085/apm.2015.10.4.317. [DOI] [Google Scholar]
- 8.Singh SP, Sethi A, Sethi D, Mishra AK. Surgical Management of Reinke’s Edema: a retrospective analysis. J Dent Med Sci. 2018;17(5):56–59. [Google Scholar]
- 9.Tateya I, Omori K, Kojima H, Hirano S, Kaneko K, Ito J (2003 Apr) Steroid injection for Reinke’s edema using fiberoptic laryngeal surgery. Acta Otolaryngol 123(3):417–420 [DOI] [PubMed]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.