

Abstract
Introduction: Foreign bodies in the paranasal sinuses are rare and can result from high velocity trauma. Here, we report a case of a 12 year old child, who sustained a penetrating injury to the left eye with a tree branch while playing. On CT scan, the wooden foreign body was found to extend into sphenoid sinus. Patient was posted for removal of foreign body in emergency OT under antibiotic coverage. The foreign body was mobilised from surrounding structures and was removed by giving strong traction. Primary closure of the wound was done and patient recovered with a stable post-op course. Discussion: Prompt and complete removal of wooden foreign body in the paranasal sinus is important due to their close proximity to vital structures. Their location and nature can be difficult to diagnose as they can have diverse appearances on imaging. Conclusion: Foreign bodies in close proximity to the sphenoid sinus should be removed by a multi-specialist team with good knowledge of head and neck anatomy in a tertiary care centre to avoid complications.
Keywords: Foreign body, Sphenoid sinus, Penetrating injury
Introduction
Foreign body in the paranasal sinuses is extremely rare. These foreign bodies are mainly traumatic in origin (maxillofacial) which occur directly as a result of external trauma to the respective sinuses or indirectly through orbital or palatal injuries. There can be visual morbidity and functional deficit when the route of these injuries is orbital. The location, size, shape and composition of the foreign body including the extent of damage caused by it, can be made out by CT scan only. If the foreign body is large, it’s removal is not easy by routine endoscopy. Rhinosurgical approaches also seem to be inadequate, keeping in view, the operative and post-operative morbidity as important structures like optic nerve, carotid artery, cribriform plate and orbit lie in close relation to these sinuses [1].
Case Report
A 12 year old female child, reported to the emergency room, following an accidental penetrating injury to the left eye with a tree branch while playing. The incident happened 2 hours before arriving at the hospital. She was referred from Ophthalmology OPD with the retained foreign body (Fig. 1).
Fig. 1.

Patient with penetrating foreign body of left eye
On examination, patient was found to be conscious, oriented with stable hemodynamic and respiratory state. Patient did not complain of any nasal obstruction, nasal bleeding or watery nasal discharge. Ophthalmological evaluation showed, left periorbital oedema with traumatic mydriasis, exposure keratitis and conjunctival prolapse of left eye. Vision was normal. No active bleeding was observed at the time of arrival to hospital.
Computed tomography scan was taken to evaluate the extent of penetration of the foreign body, which showed a radiolucent foreign body of width 10 mm in the left orbit, passing through the left medial canthus, extending medially along the medial wall of orbit in the extraconal compartment, causing fracture and displacement of lamina papyracea to the right and globe to the left. The tip of foreign body was found to extend into the sphenoid sinus via an opening in the roof of sinus with fracture of anterior wall and median septum with hemosinus. A clear interpretation of the location and trajectory of the foreign body was achieved with CT scan due to which we could avoid MRI scan in this case (Figs. 2, 3).
Fig. 2.
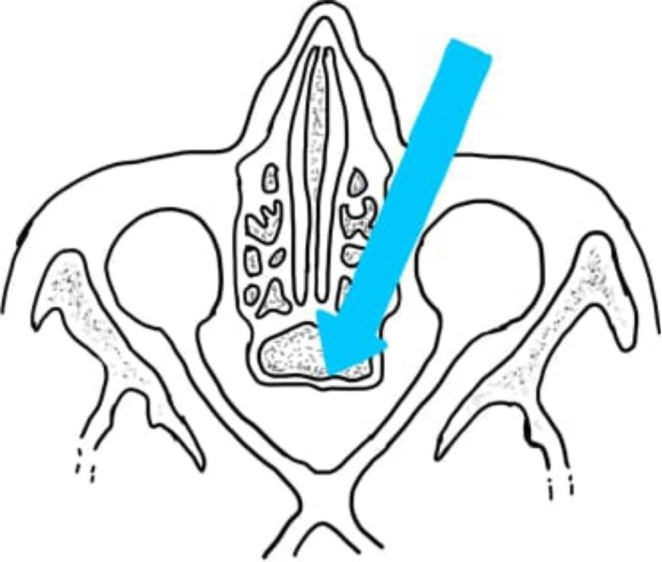
Pictorial representation of trajectory of the foreign body
Fig. 3.
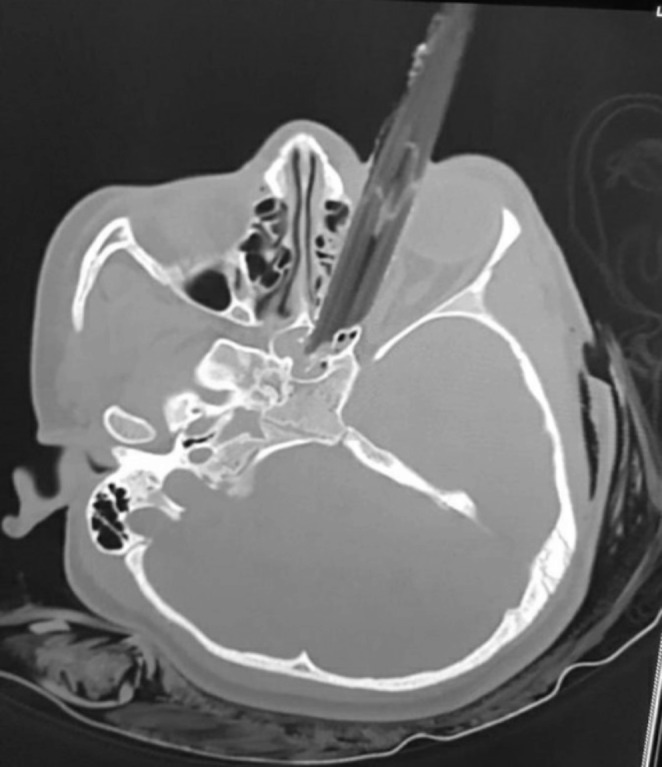
Pre-operative computed tomography image of penetrating foreign body
The patient was immediately hospitalised and high dose antibiotics, anti-tetanus prophylaxis and analgesics were started. Patient was posted for foreign body removal in emergency OT after reserving adequate blood. Our neurosurgery team was kept on standby after intimating them of the close proximity of the foreign body to vital structures. The foreign body was first mobilised from surrounding structures by gently dissecting the soft tissue around the foreign body through the external wound using artery forceps. Wound was explored in layers and adequate mobilisation of the foreign body was achieved. It was carefully removed by giving strong traction, ensuring that surrounding structures are not damaged. Wound was further explored for any residual splinters and debris. Tract was irrigated with betadine, hemostasis was achieved and primary closure was done. A diagnostic nasal endoscopy was also performed to ensure that there was no hemodynamic injury or CSF leak. Post-operatively, eye care in the form of antibiotic eye drops, carboxymethylcellulose eye drops, intravenous antibiotics, analgesics and steroids were given.
Endoscopic evaluation of nose was repeated on post-operative day 4, which did not reveal any active bleeding or CSF leak. Computed tomography scan done on fourth day, showed no residual foreign body. Periorbital oedema resolved and the patient was discharged after 15 days.
Patient was followed up for 6 months and was found to have no complications and normal vision in left eye (Figs. 4, 5).
Fig. 4.

Intact foreign body after removal
Fig. 5.

Post-operative picture on 7th day
Discussion
Foreign body in the ethmoid and sphenoid sinuses are mostly associated with orbital and maxillofacial trauma. The foreign body which is embedded in the orbit, sphenoid and ethmoid sinuses do not cause much symptoms except local irritation, pain on movement of eye and sometimes nasal discharge. CT scan is very useful to know the size, extent and relation of the foreign body to underlying vital structures. Intra-orbital wooden foreign body may also be misdiagnosed on CT as they may be mistaken for air or fat [2]. In such cases an MRI scan may be utilised [3]. MRI scan is also warranted in long term foreign bodies without any visible external components. It may also be of use, in checking for splinters of wood left behind after injuries. Chronic wooden foreign bodies may be difficult to diagnose through CT or MRI, due to the change in their density over time. Wooden foreign bodies if not diagnosed correctly and removed promptly may lead to complications due to their organic nature as they can serve as a good bacterial culture medium [4]. In case of a patient with laceration, foreign body can be removed through the wound site. If laceration has healed, then endoscopic approach will be useful [5]. If foreign body is left behind, it will lead to formation of a foreign body granuloma and there will be local symptoms like local irritation in the eye, lacrimation, epistaxis, nasal discharge and sometimes foreign body sensation at the particular site. Neglected foreign bodies of the orbit and paranasal sinuses may lie dormant for long periods of time and can present with complications later [6]. Therefore, removal of foreign bodies in the paranasal sinuses require a multimodality approach.
Conclusion
Most commonly, foreign body gets lodged in the maxilla (75%) and frontal sinuses(< 20%) compared to the ethmoid and sphenoid sinuses [7]. Foreign body reaches the sphenoid sinus either through the orbit or through the nasal cavity. Proximity of the sphenoid sinus to vital structures such as the internal carotid artery and optic nerve may render life threatening complications. Removal of such a foreign body requires good pre-operative planning and a multi-specialist team with good knowledge of anatomy and variations of sphenoid sinus in a tertiary care hospital [8, 9].
Funding
No external sources of funding received.
Declarations
Compliance with ethical standards
In concurrence with ethical standards.
Conflict of Interest
None.
Informed consent
Informed consent was obtained from the patient.
Ethical approval
This case report is conforming to the ethical standards of the institution and 1964 Helsinki declaration and it’s later amendments.
Footnotes
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
References
- 1.Sharma R, Minhas R, Mohindroo N. An unusual foreign body in the paranasal sinuses. Indian J Otolaryngol Head Neck Surg. 2008;60(1):88–90. doi: 10.1007/s12070-008-0028-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Roberts CF, Leehey PJ., 3rd Intraorbital wood foreign body mimicking air at CT. Radiology. 1992;185(2):507–508. doi: 10.1148/radiology.185.2.1410363. [DOI] [PubMed] [Google Scholar]
- 3.Takasaki K, Enatsu K, So E, Takahashi H. Fifty-four wooden toothpicks in the nasal cavity. Otolaryngol Head Neck Surg. 2005;132:669–670. doi: 10.1016/j.otohns.2004.09.073. [DOI] [PubMed] [Google Scholar]
- 4.Macrae JA. Diagnosis and management of a wooden intraorbital foreign body:Case report. Br J Ophthalmol. 1979;63:848–851. doi: 10.1136/bjo.63.12.848. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Kim SW, Cho KR A case of an tubular foreign body in the Paranasal Sinus after penetrating Orbital Injury.Journal of Medical Cases. 2014 Jan4;5(1):45–8
- 6.Sajad M, Kirmani MA, Patigaroo AR (2011 Jul) Neglected foreign body infratemporal fossa, a typical presentation:a case report. Indian J Otolaryngol Head Neck Surg 63(1):96–98 [DOI] [PMC free article] [PubMed]
- 7.Wadhwa V, Chitguppi C (2017) Retained orbito-sinal wooden foreign body as an unsuspected cause of epistaxis: a case report.Asian Journal of Ophthalmology. ; 15(2)
- 8.Padiyar BV, Vats A, Dhiman A, Rai AK. Impacted bullet in the sphenoid sinus: a Case Report. Dubai Med J. 2019;2(1):20–22. doi: 10.1159/000499038. [DOI] [Google Scholar]
- 9.Patro SK, Verma R, Panda NK Impacted Intra Sphenoid Foreign Body in an Adult: A Rare Event and a Lucky Survivor. Journal of Medicine. 2016 Oct 23;17(2):115-7