

Abstract
Autoimmune hepatitis (AIH) is a non-contagious, chronic, inflammatory autoimmune disease in which one’s own immune system attacks healthy, normal hepatic cells. The exact cause of AIH is unknown; however, the combination of genetic, environmental (eg, drugs and natural infection) and immunological factors may lead to AIH. AIH may also be potentiated with the use of vaccines: this case reports one such event following immunisation, along with 1 year of follow-up. A female patient in her late 20s presented to the hospital with yellowish discolouration of eyes, urine and stools. Her medical history revealed that she had been vaccinated with the first dose of a COVID-19 vaccine 10 days earlier. She had a history of asymptomatic COVID-19 infection 3 months ago and a history of chronic analgesic consumption for migraine. She was diagnosed as having AIH through extensive clinical and laboratory workup. This case may be an immediate enhancement of a hidden autoimmune disorder triggered by the vaccination. This adverse event following immunisation has an adequate temporal relationship with her COVID-19 vaccine. The causality can be categorised as ‘indeterminate’ and may be considered as a potential signal following COVID-19 vaccination.
Keywords: Immunization; ALLERGY AND IMMUNOLOGY; DRUG-RELATED SIDE EFFECTS AND ADVERSE REACTIONS; COVID-19; PHARMACY SERVICE, HOSPITAL; Safety
Background
Today we have adequate experience with the COVID-19 vaccines, which were initially approved under Emergency Use Listing. As well as traditional live or inactivated vaccines, today new platforms such as RNA and DNA therapeutics are familiar in the field of vaccine development.1 The concept of viral vectors in vaccinology has its root in 1972, when Jackson et al first created recombinant DNA from the SV40 virus through genetic engineering.2 Today, viral vectors represent a promising novel platform in the development of vaccines against pathogens, ranging from Ebola to tuberculosis.3
Viral vector-based vaccines are one step ahead of conventional vaccines in their ease of design, rapid development, low production cost, high efficiency, high specificity in delivering genes to target cells and increased response of cellular immunity.4–6 However, certain safety concerns have also been reported from previous animal studies, including gene toxicity, variation in genetic stability, viral tropism and gene integration.4 7 The emergence of new onset autoimmune disorders following COVID-19 immunisation is a recently observed adverse event.8
On 27 April 2021, the WHO designated vaccine-induced immune thrombotic thrombocytopenia (VITT) as a plausible adverse event of COVID-19 vaccines. One in a million people had developed VITT after immunisation with ChAdOx1 nCoV-19 (AstraZeneca vaccine).9 Subsequently, numerous isolated cases of autoimmune hepatitis (AIH) following immunisation with the AstraZeneca vaccine have been reported globally.10–12 According to the WHO Programme for International Drug Monitoring (PIDM) database; 9130 cases of hepatobiliary disorders were reported following COVID-19 vaccination, of which 507 (5.6%) cases were AIH.13
Women are affected by AIH more frequently than men, and cases are predominantly in young women.11 AIH is a chronic inflammatory condition of the liver which can be triggered by many environmental, genetic and immunological factors.10 Proposed environmental triggering factors of AIH include infection, drugs and toxins. AIH may also be potentiated by the use of vaccines.14 Here, we discuss a case of AIH following COVID-19 vaccination along with 1 year of follow-up details of the event.
Case presentation
A woman in her late 20s presented to hospital with significant yellowish discolouration of her eyes, which had been there for 2 days (figures 1 and 2). She had also noticed dark yellow coloured urine and very pale yellow stools. She described having taken the first dose of AstraZeneca vaccine 10 days ago. She gave a history of experiencing fever, chills and persistent tiredness from the day after vaccination. Her fever and chills resolved in 2 days but her fatigue continued.
Figure 1.

Yellowish discolouration of eyes 8 days after vaccination.
Figure 2.

Yellowish discolouration of eyes 10 days after vaccination.
Medical history
The patient has had irritable bowel syndrome for 6 years, for which she is not currently on any medication. She reported a history of persistent cluster-type headaches since childhood, and a family history of headache. She reported an aggravation of her headache since 1 year ago and receives analgesics (paracetamol 300 mg+propyphenazone 150 mg+caffeine 50 mg) one time per day since last year. Apart from family history (second-degree relatives) of cancer, there were no other identifiable risk factors. She also had a history of asymptomatic COVID-19 infection, detected by the presence of IgG antibodies (anti-SARS-CoV-2 IgG—positive (110 AU/mL)), on a routine lab investigation. All other lab investigations, including liver function tests, were found to be normal during the routine investigation. She had no reactions to drugs and vaccines received in the past. Her first- and second-degree relatives who had received the same vaccine (both doses) had no reaction to it.
Investigations
Investigations were done on the day of diagnosing jaundice. Ultrasonography of the patient's abdomen showed periportal cuffing which was correlated with elevated liver enzymes (aspartate aminotransferase (AST) 1855 U/L; alanine aminotransferase (ALT) 1790 U/L; total bilirubin 4.91 mg/dL; direct bilirubin 3.85 mg/dL; total protein 8.4 g/dL). Her reports of hepatitis A, B, C and E infection were found negative and anti-nuclear antibody (ANA) titre (1:100) was found positive. A positive ANA report was the initial clue for suspecting autoimmune disorder in this patient. Subsequently, the immunofluorescence assay confirmed the presence of autoantibodies such as nuclear centromere AC-3 (Centromere protein B 1:1000) and cytoplasmic reticular and mitochondrial AC-21 (1:320). Elevated IgG (>27 000 g/L) and IgM (240.5 g/L) were also detected.
She underwent a percutaneous liver biopsy 23 days after her first clinical presentation. The liver histology report showed ‘chronic hepatitis with moderate activity with bridging fibrosis (compatible with autoimmune hepatitis with the possibility of super-imposed drug toxicity)’. It also detected stage III fibrosis according to Ishak’s modified Histologic Activity Index (HAI) scoring system (scored 7/18).
Treatment
Drug therapy pre-biopsy
The patient was prescribed ursodeoxycholic acid (300 mg two times per day) and pantoprazole (40 mg two times per day). In the second week, she was prescribed S-adenosyl-L-methionine (400 mg two times per day), N-acetylcysteine (600 mg two times per day) and vitamin K4 10 mg (one time per day for 3 days). In the third week, she was given prednisolone 40 mg one time per day.
Drug therapy post-biopsy
The patient was prescribed prednisolone one time per day for 2 months (40 mg for 10 days, 30 mg for 10 days, 20 mg for 10 days, 10 mg for 10 days, 5 mg for 10 days and 5 mg alternative days for a week). She was also prescribed cholecalciferol (60 000 IU one time per week for 6 weeks), esomeprazole (40 mg for 2 months), calcium carbonate+vitamin D3 (500 mg/250 IU one time per day) and azathioprine (75 mg one time per day). She was also prescribed one multivitamin capsule per day.
Outcome and follow-up
Response to therapy
The patient responded very well to drug therapy with significant improvement in liver function tests (AST and ALT, figure 3), bilirubin (total and direct, figure 4) and prothrombin time test/international normalized ratio (PT/INR, figure 5). The patient has been followed up for 1 year, she is symptomatically better and the latest PT/INR is 1.53 liver Function test. All other lab investigation results are within normal limits. She strictly follows her diet plan and follows non-pharmacological interventions for her persistent headache. She was not recommended to take any further doses of COVID-19 vaccines.
Figure 3.
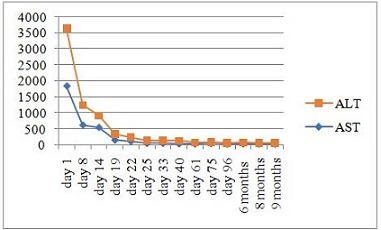
Improvement of aspartate aminotransferase (AST) and alanine aminotransferase (ALT) for 9 months post-vaccination.
Figure 4.

Improvement of total (TB) and direct bilirubin (DB) for 9 months post-vaccination.
Figure 5.
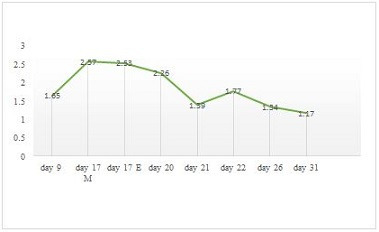
Improvement of prothrombin time test/international normalized ratio (PT/INR) during treatment.
Unintended response to drug therapy/adverse drug reactions
In the first week post-biopsy, the patient started to present with papules over the forehead and scalp. It gradually spread all over her body and was diagnosed as steroid-induced acneiform eruptions and acanthosis nigricans. She was prescribed adapalene (0.1% w/w)+clindamycin (1% w/w) gel and clobetasol (0.05% w/w)+salicylic acid (3% w/w) ointment for local application for a period of 3 weeks to manage her dermatological condition. Although the patient's condition improved after the use of the drugs, her dermatological problems subsided only after stopping steroid therapy. She had altered blood sugar levels and insomnia during the therapy period.
Discussion
There are case reports of suspected AIH following COVID-19 vaccination.11 Since AIH doesn’t have a single pathognomonic test, diagnosis mainly depends on several indicative clinical, serological, biochemical and histological findings.15 ‘Simplified diagnostic criteria for autoimmune hepatitis’ is used as the tool to help healthcare professionals to distinguish AIH from other conditions.16 This patient’s ‘simplified diagnostic criteria for AIH’ score was six, which equates to a ‘probable’ chance of AIH.
Correlation of parameters such as the presence of autoantibodies and the biopsy report of ‘chronic hepatitis with moderate activity with bridging fibrosis, Ishak’s modified HAI 7/18, fibrosis 3’ confirmed the diagnosis of AIH. Specifically, the patient’s condition can be categorised as type I AIH because of the solo appearance of ANA.17 Significantly, 70% of type I AIH incidence has been observed in females, with a peak incidence among those aged 16–30 years.18 Here, the patient’s age group and sex match.
The histopathological result of liver biopsy also raises the possibility of superimposed drug toxicity along with AIH. Thus, a situation arises with a new question of the role of drugs in AIH. Several drugs such as minocycline,19 nitrofurantoin,20 melatonin,21 diclofenac,22 statins23 and ornidazole24 have been implicated in the aetiology of drug-induced AIH (DIAIH). None of these drugs had been administered to this patient. However the chronic use of analgesics (paracetamol 300 mg+propyphenazone 150 mg+caffeine 50 mg) could produce liver injury.25 Therefore, the possibility of superimposed drug toxicity, which was pointed out in this patient’s biopsy, cannot be ruled out.
The patient had a history of asymptomatic COVID-19 infection, which was only known after the detection of IgG antibodies from the serum. This raises the question of whether viral infection can trigger AIH. Many cases have being reported with the incidence of autoimmune disorders following COVID-19 infection.26 Although the exact mechanism is unknown, theories such as molecular mimicry between viral and human proteins,26 immunologic intolerance and a sudden rise of cytokine storm27 are under discussion. Here, the patient’s history of COVID-19 infection could also be a contributing factor. However, patient’s normal liver function tests during the detection of COVID-19 antibodies would suggest otherwise.
Post-immunisation induced autoimmune reactivity is considered a very rare event.11 AIH can be hidden as asymptomatic for many years, and can develop into stage IV chronic liver disorder.14 Additionally, many similar events after COVID-19 vaccination suggest a significant threat worthy of further investigation. Even though this patient had multiple potential triggering factors in her history, immunisation was the recent event she has been exposed to just before clinical presentation. Also, the very low latency period taken by the vaccine to precipitate such autoimmune events is remarkably different from other triggering factors.
Many postulated theories exist in the current knowledge of vaccine-associated autoimmune disorders. Vaccines can induce immune dysregulation or can stimulate an aggressive innate immunity. Once this happens, there is a break in self-tolerance, especially in genetically predisposed individuals. This causes stimulation of multiple mechanisms, leading to cross-reactivity between vaccine-induced antibodies and the host antigens.28
Although many autoimmune disorders after immunisation by certain vaccines have been described previously,29 the trend of AIH after COVID-19 vaccination is alarming. Here, the dose taken by the patient was from a non-replicating adenovirus vector vaccine (AstraZeneza). It was isolated from chimpanzee adenovirus isolate Y25 (causes common cold in chimpanzees) which has much lower seroprevalence in humans.4 However, previous animal studies have come across certain safety concerns regarding these vector-based vaccine technology.3 One of these study highlights how Ad5 (human adenovirus serotype 5) vectors have a strong tropism for liver parenchyma cells, which can directly raise the risk of heptotoxicity.7
Autoimmune syndrome induced by adjuvants (ASIA) is a term coined by Shoenfeld and Agmon-Levin in 2011,30 which denotes how adjuvants or other vaccine ingredients may act as triggering factors in autoimmune disorders. The literature provides a detailed account of immunisation-associated triggering agents such as adjuvant (aluminium), stabilisers (gelatin), preservatives (thiomersal) and residual yeast proteins from cell cultures (fibronectin).31 The vaccine involved in the present case (AstraZeneca) contains ingredients such as L-histidine, L-histidine hydrochloride monohydrate, magnesium chloride hexahydrate, polysorbate 80, ethanol, sucrose, sodium chloride, disodium edetate dihydrate (EDTA) and water for injection.32 Most vaccine-associated autoimmune disorders can lead to the probability of ASIA;30 however, differentiating the diagnoses from one another is a herculean task. Therefore, this case may serve as an indication to conduct more detailed differential study into vector-based COVID-19 vaccines.
The low latency period taken to develop such a serious disorder is food for thought. There are similar cases reported with COVID-19 vaccine-induced AIH occurring within 4–10 days post-immunisation.10–12 As we excluded other possible triggering agents from the patient’s medical history, we considered the possibility of AIH triggered by COVID-19 vaccination. Causality assessment of this adverse event following immunisation falls under the category of ‘indeterminate’: the temporal relationship is consistent, but there is insufficient definitive evidence for the vaccine causing the event. This event could be a new vaccine-linked event and can be considered as a potential signal.
Patient's perspective.
The statements explained in this case report were true and based on my knowledge. I am a healthcare professional and I could read and understand this case report. I was so much shocked with my health condition and it was very hard to cope. Now, 1 year after being diagnosed with autoimmune hepatitis, I am still on my regular medication (azathioprine 75 mg one time per day). The adequate dietary and lifestyle modifications and regular checkups (every 6 months) help me to manage and control my health condition effectively.
Learning points.
In short, the patient’s presentation is a condition of intolerance of self-antigens, stimulated by an external environmental trigger (such as a vaccine or its components) resulting in the precipitation of a hidden disorder. It should be specifically noted that the core reason for autoimmune hepatitis (AIH) would be any of the genetic alterations in human leukocyte antigen (HLA) genes which are commonly associated with autoimmune disorders. Thus, cases of AIH following vaccination cannot be simply taken as coincidental. This event could be a severe adverse event with an indeterminate causal association with COVID-19 vaccination, possibly triggered by the antigen or adjuvants present in the vaccine.
Footnotes
Correction notice: This article has been updated since it was first published. The author affiliations have been corrected.
Collaborators: not applicable.
Contributors: MM: contributed to the original article and writing. SBJ: contributed the resources. JS: critically reviewed the case report and is guarantor. MDR: reviewed and served as scientific advisor.
Funding: The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests: None declared.
Provenance and peer review: Not commissioned; internally peer reviewed.
Ethics statements
Patient consent for publication
Consent obtained directly from patient(s)
Ethics approval
This study involves human participants and was approved by the ethical committee, overseeing the study site is Institutional Ethics Committee of JSS Medical College Mysuru. The ethical approval number: JSSMC/IEC/240921/01NCT/2021-22. Participants gave informed consent to participate in the study before taking part.
References
- 1. Rosa SS, Prazeres DMF, Azevedo AM, et al. mRNA vaccines manufacturing: challenges and bottlenecks. Vaccine 2021;39:2190–200. 10.1016/j.vaccine.2021.03.038 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2. Jackson DA, Symons RH, Berg P. Biochemical method for inserting new genetic information into DNA of simian virus 40: circular SV40 DNA molecules containing lambda phage genes and the galactose operon of Escherichia coli. Proc Natl Acad Sci U S A 1972;69:2904–9. 10.1073/pnas.69.10.2904 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3. Chen RT, Carbery B, Mac L, et al. The Brighton collaboration viral vector vaccines safety Working Group (V3SWG). Vaccine 2015;33:73–5. 10.1016/j.vaccine.2014.09.035 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4. Chavda VP, Bezbaruah R, Athalye M, et al. Replicating viral vector-based vaccines for COVID-19: potential avenue in vaccination arena. Viruses 2022;14:1–21. 10.3390/v14040759 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5. Crommelin DJA, Volkin DB, Hoogendoorn KH, et al. The science is there: key considerations for stabilizing viral vector-based Covid-19 vaccines. J Pharm Sci 2021;110:1–15. 10.1016/j.xphs.2020.11.015 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6. Custers J, Kim D, Leyssen M. Vaccines based on replication incompetent Ad26 viral vectors:Standardized template with key considerations for a risk/benefit assessment. Viruses 2022;14:2–21. 10.1016/j.vaccine.2020.09.018 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7. Ura T, Okuda K, Shimada M. Developments in viral vector-based vaccines. Vaccines 2014;2:624–41. 10.3390/vaccines2030624 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8. Chen Y, Xu Z, Wang P, et al. New-onset autoimmune phenomena post-COVID-19 vaccination. Immunology 2022;165:386–401. 10.1111/imm.13443 [DOI] [PubMed] [Google Scholar]
- 9. Aleem A, Nadeem AJ. Coronavirus (COVID-19) vaccine-induced immune thrombotic thrombocytopenia (VITT). StatPearls Publishing, 2022: 1–19. [PubMed] [Google Scholar]
- 10. Garrido I, Lopes S, Simões MS, et al. Autoimmune hepatitis after COVID-19 vaccine - more than a coincidence. J Autoimmun 2021;125:102741. 10.1016/j.jaut.2021.102741 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11. Rela M, Jothimani D, Vij M, et al. Auto-immune hepatitis following COVID vaccination. J Autoimmun 2021;123:102688. 10.1016/j.jaut.2021.102688 [DOI] [PubMed] [Google Scholar]
- 12. Bandera JM, Albújar AH, Salguero AI. Acute hepatitis with autoimmune features after COVID-19 vaccine: coincidence or vaccine-induced phenomenon? Gastroenterology Rep 2022:1–4. 10.1093/gastro/goac014 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13. Vigiaccess . Uppsala monitoring centre, 2015. World health organisation. Available: http://www.vigiaccess.org [Accessed 18 Jun 2022].
- 14. Manns MP, Czaja AJ, Gorham JD, et al. Diagnosis and management of autoimmune hepatitis. Hepatology 2010;51:2193–213. 10.1002/hep.23584 [DOI] [PubMed] [Google Scholar]
- 15. Ducazu O, Degroote H, Geerts A, et al. Diagnostic and prognostic scoring systems for autoimmune hepatitis: a review. Acta Gastroenterol Belg 2021;84:487–95. 10.51821/84.3.014 [DOI] [PubMed] [Google Scholar]
- 16. Hennes EM, Zeniya M, Czaja AJ, et al. Simplified criteria for the diagnosis of autoimmune hepatitis. Hepatology 2008;48:169–76. 10.1002/hep.22322 [DOI] [PubMed] [Google Scholar]
- 17. Ishak K, Baptista A, Bianchi L, et al. Histological grading and staging of chronic hepatitis. J Hepatol 1995;22:696–9. 10.1016/0168-8278(95)80226-6 [DOI] [PubMed] [Google Scholar]
- 18. Sucher E, Sucher R, Gradistanac T, et al. Autoimmune hepatitis—immunologically triggered liver Pathogenesis—diagnostic and therapeutic strategies. J Immunol Res 2019;2019:1–19. 10.1155/2019/9437043 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19. Björnsson E, Talwalkar J, Treeprasertsuk S, et al. Drug-induced autoimmune hepatitis: clinical characteristics and prognosis. Hepatology 2010;51:2040–8. 10.1002/hep.23588 [DOI] [PubMed] [Google Scholar]
- 20. Czaja AJ. Transitioning from idiopathic to Explainable autoimmune hepatitis. Dig Dis Sci 2015;60:2881–900. 10.1007/s10620-015-3708-7 [DOI] [PubMed] [Google Scholar]
- 21. Hong YG, Riegler JL. Is melatonin associated with the development of autoimmune hepatitis? J Clin Gastroenterol 1997;25:376–8. 10.1097/00004836-199707000-00020 [DOI] [PubMed] [Google Scholar]
- 22. Scully LJ, Clarke D, Barr RJ. Diclofenac induced hepatitis. 3 cases with features of autoimmune chronic active hepatitis. Dig Dis Sci 1993;38:744–51. 10.1007/BF01316809 [DOI] [PubMed] [Google Scholar]
- 23. Alla V, Abraham J, Siddiqui J, et al. Autoimmune hepatitis triggered by statins. J Clin Gastroenterol 2006;40:757–61. 10.1097/00004836-200609000-00018 [DOI] [PubMed] [Google Scholar]
- 24. Koşar Y, Saşmaz N, Oguz P, et al. Ornidazole-induced autoimmune hepatitis. Eur J Gastroenterol Hepatol 2001;13:737–9. 10.1097/00042737-200106000-00022 [DOI] [PubMed] [Google Scholar]
- 25. Rotundo L, Pyrsopoulos N. Liver injury induced by paracetamol and challenges associated with intentional and unintentional use. World J Hepatol 2020;12:125–36. 10.4254/wjh.v12.i4.125 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26. Liu Y, Sawalha AH, Lu Q. COVID-19 and autoimmune diseases. Curr Opin Rheumatol 2021;33:155–62. 10.1097/BOR.0000000000000776 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27. Cañas CA. The triggering of post-COVID-19 autoimmunity phenomena could be associated with both transient immunosuppression and an inappropriate form of immune reconstitution in susceptible individuals. Med Hypotheses 2020;145:110345–9. 10.1016/j.mehy.2020.110345 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28. Segal Y, Shoenfeld Y. Vaccine-induced autoimmunity: the role of molecular mimicry and immune crossreaction. Cell Mol Immunol 2018;15:586–94. 10.1038/cmi.2017.151 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29. Perumalswami P, Peng L, Odin JA. Vaccination as a triggering event for autoimmune hepatitis. Semin Liver Dis 2009;29:331–4. 10.1055/s-0029-1233537 [DOI] [PubMed] [Google Scholar]
- 30. Shoenfeld Y, Agmon-Levin N. 'ASIA' - autoimmune/inflammatory syndrome induced by adjuvants. J Autoimmun 2011;36:4–8. 10.1016/j.jaut.2010.07.003 [DOI] [PubMed] [Google Scholar]
- 31. Shoenfeld Y, Aron-Maor A. Vaccination and autoimmunity-'vaccinosis': a dangerous liaison? J Autoimmun 2000;14:1. 10.1006/jaut.1999.0346 [DOI] [PubMed] [Google Scholar]
- 32. COVISHIELD fact sheet for vaccine recipient Approved for restricted use in emergency situation of chAdOx 1 nCoV- 19 corona virus vaccine (recombinant).SII. Available: https://cdsco.gov.in/opencms/export/sites/CDSCO_WEB/en/Factsheetof-ChAdSerum.pdf [Accessed 22 Jun 2022].