

Abstract
Associations between depressive symptoms and relationship distress are well-established, but little is known about these linkages among Black couples, or about the role of sociocultural factors in these processes. In this study, we applied a dyadic analytic approach, Actor Partner Interdependence Modeling (APIM), to address two goals: to assess the prospective, bidirectional associations between depressive symptoms and marital satisfaction over a one-year period in a racially homogenous sample of 168 heterosexual Black couples, and to explore whether these associations were moderated by husbands’ and wives’ experiences of racial discrimination and/or the centrality of race in their personal identities. Findings revealed that depressive symptoms predicted relative declines in marital satisfaction reported by both self and partner for both husbands and wives. Moderation analyses indicated that, when wives reported greater racial centrality, their depressive symptoms predicted relative declines in husbands’ marital satisfaction. In contrast, when wives reported lower racial centrality, their depressive symptoms were not associated with husbands’ satisfaction. Together, the findings highlight the interdependence between spouses’ mental health and relationship satisfaction and the role of sociocultural factors in these linkages.
Keywords: African-American, couples, romantic relationships, discrimination, racial identity
Recognizing the unique stressors Black Americans face and their distinct cultural resources, scholars have called for research dedicated to the continued improvement of health and relationship quality in Black families and investigation of cultural factors that enhance such functioning (McNeil Smith & Landor, 2018). Doing so requires examining links between individual psychological functioning and romantic relationship adjustment in Black couples. Although prior research has established associations between depression and relationship quality in the general population (Kouros, Papp, & Cummings, 2008; Whisman, 2001), little is known about these linkages among Black couples. Further, sociocultural factors, such as racial discrimination and racial identity, have implications for the links between mental health and marital quality (Bryant et al., 2010). With some important exceptions (Lincoln & Chae, 2010; McNeil, Fincham, & Beach, 2014; Murry, Brown, Brody, Cutrona & Simons, 2001), however, these moderating processes have received little attention. Accordingly, this study aimed to advance understanding of the well-being of Black couples by using longitudinal, dyadic analyses to examine the prospective associations between depressive symptoms and martial satisfaction in a racially homogenous sample of heterosexual, Black romantic couples and explore the extent to which these associations were moderated by each partner’s experiences of discrimination and racial centrality.
Depression and Couple Functioning
Consistent with interpersonal theories of depression (Coyne, 1976; Hammen, 2006), depressive symptoms have been linked to poorer intimate relationship quality (Davila, Karney, Hall, & Bradbury, 2003; Kouros et al., 2008). From these perspectives, individuals prone to depression or depressive symptoms become engaged in a feedback loop in which negative cognitive appraisals and interpersonal vulnerabilities create stressful interactions between romantic partners, subsequently increasing relationship distress. These stressful interactions can, in turn, exacerbate depressive symptoms for both partners. In this way, depressive symptoms erode relationship satisfaction, and relationship dissatisfaction increases depressive symptoms. Indeed, an epidemiological study of married older White, British couples found bidirectional, longitudinal, within-person linkages between depressive symptoms and perceived marital discord for both wives and husbands (Whisman & Uebelacker, 2009). Romantic partners’ depressive symptoms and marital satisfaction are also linked: depressive symptoms in one spouse are associated with lower marital satisfaction in the other (MacKenzie et al., 2014; Whisman & Uebelacker, 2009), and one spouse’s marital satisfaction is negatively associated with depressive symptoms in the other (Beach, Katz, Kim, & Brody, 2003).
Prior studies have examined the psychological benefits of marriage for Black Americans (Taylor, Chae, Chatters, Lincoln, & Brown, 2012). However, we know less about how marital satisfaction is related to mental health in this population. The depressive symptoms-relationship quality link may be especially relevant for Black couples. First, although depression is less prevalent among Black as compared to White Americans, depression in Black Americans is usually longer-lasting and more severe (Walton & Payne, 2016) and may serve as a chronic stressor for Black couples. Second, compared to other racial groups, Black Americans report lower marital satisfaction and experience higher rates of divorce (Bulanda & Brown, 2007). Thus, understanding the relations between depressive symptoms and marital satisfaction in this population has important public health implications. The few studies that have included substantial numbers of Black couples suggest that the links between depressive symptoms and relationship qualities are not necessarily the same as those reported in the broader literature, which has focused on predominantly White samples. For example, Fagan (2009) found that African American and Hispanic fathers, but not White fathers, experienced decreases in depressive symptoms over a 2-year period when they initially perceived higher levels of spousal support. Studies of the dyadic, cross-sectional associations between psychological distress and relationship quality have also yielded inconsistent results. A study of cohabitating couples revealed a link between one partner’s depressive symptoms and the other’s report of relationship quality for White couples, but this association was nonsignificant for Black couples (MacKenzie et al., 2014). However, actor and partner effects from psychological distress to negative couple interactions emerged in a sample of married and cohabitating Black couples (Sutton, Simons, Simons, & Cutrona, 2017). Reliance on racially comparative and cross-sectional designs limits the ability to discern the directionality of effects in the links between mental health and relationship quality among Black couples. To address these limitations and extend prior work, we used dyadic longitudinal data to examine the prospective associations between depressive symptoms and relationship satisfaction among Black couples.
The Moderating Roles of Discrimination and Racial Centrality
We also investigated potential sociocultural moderators of the longitudinal links between husbands’ and wives’ depressive symptoms and their ratings of marital satisfaction. We focused first on racial discrimination as it is a common stressful experience of Black Americans. One national survey found that almost 50% of Black respondents reported at least one major experience of discrimination, and 71% reported everyday discrimination occurring “sometimes” or “often” (Kessler, Mickelson, & Williams, 1999). Discrimination has been linked to psychological distress (Brown et al., 2000) as well as poorer intimate relationship quality (Trail, Goff, Bradbury, & Karney, 2012). Conceptually, the Mundane Extreme Environmental Stress (MEES; Carroll, 1998; Peters & Massey, 1983) theory suggests that Black families are faced with chronic and ubiquitous encounters with racism and discrimination that create stressful environments, which can deplete individuals’ cognitive and emotional resources over time, resulting in lowered capacity to manage family stressors (e.g. spousal behaviors and conflicts) and amplifying the negative implications of family stressors (Lincoln & Chae, 2010; Murry et al., 2001). We expand the MEES theory by applying it in a family systems framework to examine its operation within a relational context, considering if the impact of discrimination can amplify effects of stressors for individuals and their partners (Minuchin, 1985). Because discrimination experiences are shared within families, the consequences of racism may spread through the couple system, as spouses attempt to cope collectively with discrimination-related stress (Shorter-Gooden 2004; St. Jean & Feagin, 1998). Thus, from the perspective of MEES theory, more frequent experiences of discrimination should amplify the effect of stressors on the couple system by strengthening negative associations between depressive symptoms and relationship satisfaction within and between spouses.
We also tested partners’ racial identity as a potential moderator of depressive symptoms-satisfaction linkages. Research and theory suggest links between racial identity and individual mental health (Settles, Navarrete, Pagano, Abdou, & Sidanius, 2010). Racial identity also may reduce negative effects of sociocultural stressors on marital quality (Bryant et al., 2010). We know little about the effects of racial identity on romantic relationships, though some work has examined racial attitudes. For instance, both negative and mixed stereotypes about African Americans were negatively related to African American husbands’ concurrent reports of marital trust and dyadic adjustment; but their positive stereotypes were positively related to their concurrent marital trust among those with relatively higher socioeconomic status and lower religious well-being (Kelly & Floyd, 2006). MEES theory posits that dimensions of racial identity, such as racial centrality, or the extent to which individuals define their identity in terms of their race (Sellers, Smith, Shelton, Rowley, & Chavous, 1998), can promote belonging and acceptance that may mitigate effects of sociocultural stressors on Black families (Carroll, 1998). Consistent with a family systems perspective, we examined whether the benefits of racial centrality extended to links between spouses’ depressive symptoms and marital satisfaction given that racial centrality may serve as a psychological resource in the face of stress for both partners. Thus, from this perspective, under conditions of higher racial centrality, the links between depressive symptoms and marital satisfaction would be attenuated within and between spouses.
Current Study
In sum, our goals were to assess the links between depressive symptoms and marital satisfaction using longitudinal, dyadic data to capture the experiences of both husbands and wives over time and to explore whether experiences of racial discrimination and racial centrality moderate these associations. To address these goals, we applied the Actor-Partner Interdependence Model (APIM; Kenny, Kashy, & Cook, 2006), which permits the simultaneous examination of both within-spouse (actor) and between-spouse (partner) effects on depressive symptoms and marital satisfaction. Based on theory and prior studies, for both husbands and wives, we expected: negative, bidirectional longitudinal links between one’s depressive symptoms and marital satisfaction over time, i.e., cross-construct actor effects (Hypothesis 1); and negative, bidirectional longitudinal links between actors’ depressive symptoms and their partners’ marital satisfaction and vice versa, i.e., cross-construct partner effects (Hypothesis 2). In testing these hypotheses, we also assessed whether actor and partner effects were moderated by gender. In addition, we tested whether discrimination and racial centrality served as risk and protective factors, respectively, such that negative associations between depressive symptoms and marital satisfaction would be stronger at higher levels of discrimination (Hypothesis 3) and weaker at higher levels of racial centrality (Hypothesis 4). Given limited literature, however, we did not make a priori hypotheses concerning moderation for specific actor and partner paths.
Method
Participants
Data were from a longitudinal study of family relationships among African American families collected from 2002-2004 (McHale et al., 2006). Families identifying as African American/Black, including cohabitating mother and father figures, and at least two adolescent-age children were recruited from locations in the mid-Atlantic region of the United States. Half were contacted by local African American recruiters via churches and community events and the other half via a mailing list purchased from a marketing firm.
At Time 1 (T1) of the parent study, 202 families participated. From this sample, parents not in a romantic relationship (e.g. mother-grandfather pairs, n = 7), families in which one parent identified as other than African American/Black (n = 14), couples divorced at T1 (n = 7), and couples who had cohabited for fewer than three years (n = 6) were omitted to increase the sample’s homogeneity. The study sample thus included 168 co-residential Black couples, 10 of whom divorced or withdrew in the year between T1 and T2. Men and women averaged 43.57 (SD = 7.21) and 40.75 (SD = 5.66) years of age at T1. Almost 96% of the sample was married; the remaining 7 couples were cohabitating. Given that most couples were married, partners are referred to as “husbands” and “wives” henceforth. At T1, couples had been living together for 14.16 years (SD = 6.88) on average. The median annual family income was $83,850.
Procedure
Data were collected during annual, 2-3 hour in-home visits conducted by teams of two interviewers, almost all of whom were Black. Interviews began with informed consent procedures and families received a $200 honorarium at each wave. Study protocols and procedures were approved by the University’s Institutional Review Board, and all participants provided written informed consent prior to being assessed.
Measures
Depressive symptoms were assessed at T1 and T2 using a 12-item version of the Center for Epidemiological Studies Depression scale (CES-D; Radloff, 1977). Participants rated how frequently they experienced each symptom in the previous week (e.g. “feeling blue”) using a 4-point Likert-type scale ranging from 1 (rarely or none of the time) to 4 (most or all of the time). Higher summed scores reflected greater depressive symptom severity. Cronbach’s alphas ranged from .75 to .80 across time points and gender.
Marital satisfaction was measured at T1 and T2 using an 8-item version of the Domains of Marriage Scale (Huston, McHale, & Crouter, 1986). Spouses rated their satisfaction using a 9-point Likert-type scale ranging from 1 (extremely dissatisfied) to 9 (extremely satisfied), e.g., “How satisfied are you with how well the two of you talk over important and unimportant issues?” Higher summed scores reflected greater satisfaction. Alphas ranged from .89 to .92 across time points and gender.
Discrimination was assessed at T1 with 11 items from the Experience with Discrimination Scale (Murry et al., 2001). Participants rated the frequency of discrimination experiences using a 4-point scale ranging from 1 (never) to 4 (several times), e.g., “How often have you been treated unfairly because you are African American instead of White?” Higher summed scores reflected more experiences of discrimination. Alphas were .90 for both partners.
Racial centrality was assessed at T1 using eight items from the Centrality Subscale of the Multidimensional Inventory of Black Identity (Sellers et al., 1998). Participants rated their agreement from 1 (strongly agree) to 4 (strongly disagree), e.g., “In general, being Black is an important part of my self-image.” Items were averaged, with higher scores reflecting greater racial centrality. Cronbach’s alpha was .71 for husbands and .73 for wives.
Data Analysis
First, descriptive statistics were calculated and effect sizes were interpreted consistent with Cohen’s (1988) recommendations (small = .10, medium = .30, large = .50). Then, to investigate the prospective associations between depressive symptoms and marital satisfaction within a dyadic context, we estimated an autoregressive cross-lagged model within the Actor-Partner Interdependence Modeling framework (APIM; Kenny et al., 2006) using Structural Equation Modeling in Mplus version 7.4 (Muthén & Muthén, 1998-2012). To test cross-construct actor and partner effects, controlling for autoregressive effects of each construct, husbands’ and wives’ T1 depressive symptoms and marital satisfaction scores were entered as simultaneous predictors and their T2 depressive symptoms and marital satisfaction scores entered as simultaneous outcomes in the same model. Given the documented within-construct partner effects for depression and marital satisfaction (Whisman & Uebelacker, 2009), these effects (e.g., the path from one partner’s depressive symptoms to the other’s) were included. All predictors were free to covary at T1, and all residuals were free to correlate at T2. Robust maximum likelihood (MLR) was used for estimation to account for missing data and non-normality of some study variables.
Missingness ranged from 0% to 16%, with husbands’ T2 depressive symptoms and marital satisfaction the highest. Husbands with missing data on depressive symptoms or marital satisfaction at T2 did not differ significantly on their T1 scores from those who completed these measures at both time points (ps > .25). Little’s MCAR (Missing Completely at Random) test suggested that the data were not missing completely at random (χ2 (91) = 115.54, p = .042). We explored all key variables, but only gender was related to missingness (χ2 (1) = 11.07, p = .001). Because gender is included in the model, we treated the data as missing at random, thereby meeting the assumptions of Full Information Maximum Likelihood approaches like MLR. The Time 1 scores of the 10 couples who divorced or withdrew from the study did not differ significantly from those of participants who contributed data at both time points with respect to total depressive symptoms, marital satisfaction, discrimination, or racial centrality (ps > .098); thus, their Time 1 scores were retained to contribute to the estimation of the covariances among predictors.
Given prior findings that partner age, length of relationship, income, and child ages are associated with relationship quality and mental health (Clavél et al., 2017), they were initially included as covariates. However, because none predicted the outcome variables and the pattern of results was the same with or without the covariates, they were removed in the final model.
Consistent with recommendations by Hu and Bentler (1999), good model fit was interpreted in terms of a non-significant chi-square test, Root Mean Square Error of Approximation (RMSEA) less than or equal to .06, Standardized Root Mean Square Residual (SRMR) less than or equal to .08, and a Comparative Fit Index (CFI) greater than or equal to .95. Gender differences in the estimated paths were examined using chi-square difference tests (corrected for the use of MLR) to compare models in which paths between husbands and wives were constrained to be equivalent versus freely estimated. When model fit did not significantly degrade when paths were constrained to be the same, the more parsimonious model was retained.
To explore the moderating effects of discrimination and racial centrality on the links between depressive symptoms and marital satisfaction within and across partners, four moderation models were estimated: For each moderator, we tested its effects on both depressive symptoms and marital satisfaction outcomes in separate models. Thus, each model included the main effects of the predictors (depressive symptoms predicting marital satisfaction or marital satisfaction predicting depressive symptoms), the main effects of the moderators (i.e., discrimination or racial centrality), and the interaction terms between the predictor and moderator, along with the autoregressive effects of the outcome variable. For each moderation model, four 2-way interactions were created between actors’ and partners’ predictor and moderator scores. All variables were centered before creating the interaction terms and the covariance of each interaction with its components was constrained to zero to improve model convergence (constraints did not change the size or direction of effects). T1 predictors and interactions were allowed to covary, and T2 residuals were allowed to correlate.
To examine the moderating effect of experiences of discrimination on the linkages between depressive symptoms and marital satisfaction, the main effects for actors’ and partners’ depressive symptoms and experiences of discrimination, as well as the four 2-way interactions between actors’ and partners’ depressive symptoms and experiences of discrimination (i.e., husbands’ depressive symptoms by husbands’ discrimination, husbands’ depressive symptoms by wives’ discrimination, wives’ depressive symptoms by wives’ discrimination, and wives’ depressive symptoms by husbands’ discrimination), were included to predict actors’ and partners’ marital satisfaction at T2 after controlling for the actor and partner effects of marital satisfaction at T1 (Moderation Model 1). The remaining moderation models were constructed in a similar manner and included the main effects and interactions between: T1 marital satisfaction by discrimination predicting T2 depressive symptoms (Moderation Model 2); T1 depressive symptoms by racial centrality predicting T2 marital satisfaction (Moderation Model 3); and T1 marital satisfaction by racial centrality predicting T2 depressive symptoms (Moderation Model 4). Significant interactions were probed at low (one standard deviation below the mean) and high (one standard deviation above the mean) levels of the moderator.
Results
Table 1 presents the means, standard deviations, and bivariate correlations between the study variables. Consistent with the non-clinical nature of the sample, depressive symptoms were relatively low, and marital satisfaction was high. Both husbands’ and wives’ depressive symptoms and marital satisfaction were significantly correlated, with moderate to large effect sizes. Paired t-tests indicated that husbands reported higher marital satisfaction (t(159) = 4.04, p < .001) than wives at T1 and more depressive symptoms at both T1 and T2 (t(160) = 3.48, p = .001; t(141) = 2.23, p = .027). Cross-time and cross-partner correlations between actors’ depressive symptoms and marital satisfaction and partners’ depressive symptoms and marital satisfaction were generally significant and small to moderate in size. Correlations between husbands’ and wives’ discrimination scores were not significant, and husbands reported more discrimination than wives (t(159) = 2.65, p = .009). Correlations between spouses’ racial centrality scores was significant but small, and the difference between husbands’ and wives’ racial centrality, however, was nonsignificant (t(161) = 1.44, p = .153). Wives’ but not husbands’ racial centrality and discrimination were significantly associated.
Table 1.
Means, Standard Deviations, and Correlations between Husbands’ and Wives’ Depressive Symptoms, Marital Satisfaction, Experiences of Discrimination, and Racial Centrality
| Variables | Husbands |
Wives |
||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Time 1 |
Time 2 |
Time 1 |
Time 2 |
|||||||||
| DS | MS | ED | RC | DS | MS | DS | MS | ED | RC | DS | MS | |
|
|
|
|||||||||||
| Husbands | ||||||||||||
| Time 1 | ||||||||||||
| DS | -- | |||||||||||
| MS | −.24 * | -- | ||||||||||
| ED | .21 * | −.13 | -- | |||||||||
| RC | −.09 | .12 | .13 | |||||||||
| Time 2 | -- | |||||||||||
| DS | .60 * | −.20 * | −.14 | .11 | -- | |||||||
| MS | −.36 * | .67 * | −.04 | −.13 | −.31 * | -- | ||||||
| Wives | ||||||||||||
| Time 1 | ||||||||||||
| DS | .13 | −.18 * | −.01 | −.01 | .14 | −.33 * | -- | |||||
| MS | −.13 | .37 * | .08 | .00 | −.16 | .41 * | .19 * | -- | ||||
| ED | .15 | −.09 | .10 | .03 | .02 | −.12 | .07 | −.03 | -- | |||
| RC | −.04 | .12 | .00 | .18 * | .02 | −.03 | .03 | −.01 | .20 * | -- | ||
| Time 2 | ||||||||||||
| DS | .05 | −.04 | −.02 | .02 | .02 | −.16 | .49 * | −.11 | .08 | −.01 | -- | |
| MS | −.16 * | .23 * | .12 | .06 | −.21 * | .38 * | −.24 * | .60* | −.03 | .04 | −.35 * | -- |
|
| ||||||||||||
| M | 19.64 | 58.51 | 20.68 | 2.76 | 19.48 | 57.38 | 17.87 | 53.91 | 19.01 | 2.68 | 18.12 | 55.20 |
| SD | 5.38 | 11.01 | 6.93 | .56 | 5.79 | 12.01 | 4.40 | 12.92 | 6.30 | .57 | 4.83 | 12.24 |
Note. N = 168 couples.
p < .05.
M = Mean, SD = Standard Deviation, DS = Depressive Symptoms, MS = Marital Satisfaction, ED = Experiences of Discrimination, and RC = Racial Centrality.
Prospective Associations Between Depressive Symptoms and Marital Satisfaction
Unstandardized estimates, p-values, and 95% confidence intervals (CIs) for the model focused on depressive symptoms and marital satisfaction as simultaneous outcomes are presented in Table 2. The final model (Figure 1) provided excellent fit to the data, (χ2(7) = 3.91, p = .790; RMESA = .00; SRMR = .04; CFI = 1.00). All paths were constrained to be equivalent across husbands and wives, except for the paths between spouses’ marital satisfaction from T1 to T2, which were estimated separately as described below.
Table 2.
Unstandardized Coefficients, Standard Errors, p Values, and 95% Confidence Intervals for Actor and Partner Effects Linking Depressive Symptoms and Marital Satisfaction at Time 1 and Time 2
| Husbands | Wives | |||||||
|---|---|---|---|---|---|---|---|---|
| Effect | B | SE | p-value | 95% CI | B | SE | p-value | 95% CI |
| DS (T2) | ||||||||
| Actor DS (T1) | .569 | .065 | .000 | [.442, .696] | .569 | .065 | .000 | [.442, .696] |
| Partner DS (T1) | −.022 | .058 | .701 | [−.138, .094] | −.022 | .059 | .701 | [−.138, .094] |
| Actor MS (T1) | −.032 | .023 | .161 | [−.077, .013] | −.032 | .023 | .161 | [−.077, .013] |
| Partner MS (T1) | .001 | .019 | .957 | [−.036, .038] | .001 | .019 | .957 | [−.036, .038] |
| MS (T2) | ||||||||
| Actor DS (T1) | −.385 | .098 | .000 | [−.577, −.193] | −.385 | .098 | .000 | [−.577, −.193] |
| Partner DS (T1) | −.344 | .125 | .006 | [−.589, −.099] | −.344 | .125 | .006 | [−.589, −.099] |
| Actor MS (T1) | .573 | .049 | .000 | [.477, .669] | .573 | .049 | .000 | [.477, .669] |
| Partner MS (T1) | .206 | .059 | .000 | [.090, .322] | −.041 | .075 | .580 | [−.188, .106] |
Note. B = Unstandardized Coefficient, SE = Standard Error, CI = Confidence Interval, DS = Depressive Symptoms, MS = Marital Satisfaction, T1 = Time 1, T2 = Time 2.
Figure 1.
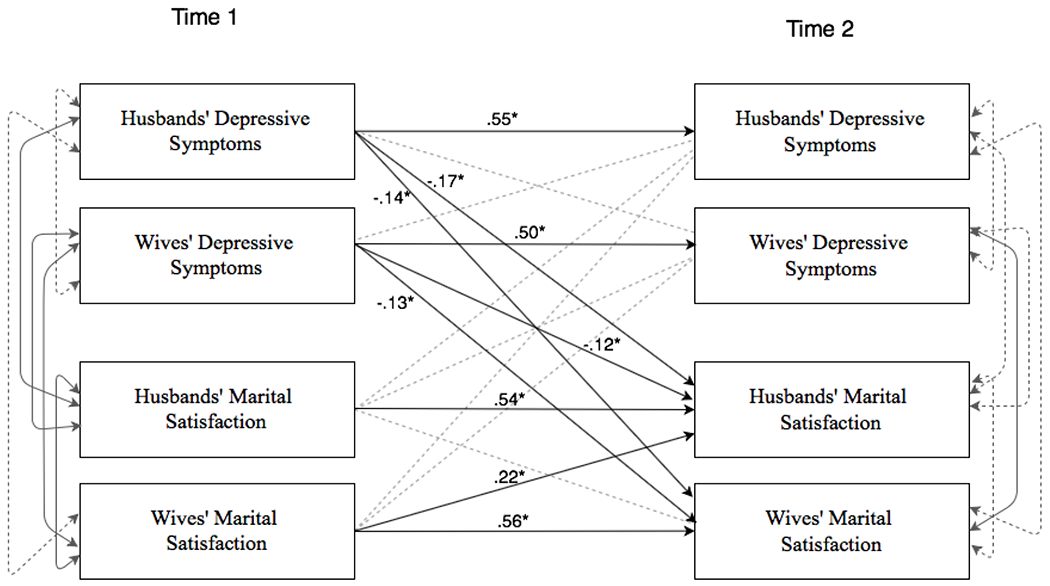
The prospective associations between depressive symptoms and marital satisfaction in an Actor-Partner Interdependence Modeling framework. Standardized coefficients are provided for significant paths. Dashed lines represent non-significant paths.
* p < .05
In partial support of our first hypothesis, for both husbands and wives, there was a significant negative association between actors’ T1 depressive symptoms and actors’ T2 marital satisfaction (cross-construct actor effect). T1 marital satisfaction did not predict T2 depressive symptoms, however. Partial support for our second hypothesis was evidenced by a negative link between actors’ T1 depressive symptoms and partners’ T2 marital satisfaction (cross-construct partner effect) for both husbands and wives. This relation was similarly not bidirectional, as actors’ T1 marital satisfaction did not predict partners’ T2 depressive symptoms.
Although not central to the primary study, exploration of within-construct partner effects indicated that wives’ T1 marital satisfaction positively predicted husbands’ T2 marital satisfaction but husbands’ satisfaction did not significantly predict that of wives. A significant chi-square difference test (χ2 (1) = 7.10, p = .008) confirmed a gender difference in this effect. Exploration of the depressive symptoms within-construct partner effect indicated that actors’ T1 depressive symptoms did not predict partners’ T2 depressive symptoms.
Moderation by Discrimination and Racial Centrality
All four moderation models yielded significant interaction effects. Tables 3 and 4 present the unstandardized coefficients, p values, and CIs for Moderation Models 1 and 2 examining the moderating effect of discrimination on the links between T1 depressive symptoms and T2 marital satisfaction (χ2(8) = 8.07, p = .427, RMESA = .01; SRMR = .05; CFI = 1.00) and between T1 marital satisfaction and T2 depressive symptoms (χ2(8) = 3.29, p = .915, RMESA = .00; SRMR = .03; CFI = 1.00), respectively. Three significant interactions emerged. First, the husbands’ depressive symptoms by husbands’ discrimination interaction predicted wives’ marital satisfaction (β = −.12, p = .045). Post hoc probing (Figure 2a) indicated that, when husbands experienced more discrimination (1 SD above the mean), their depressive symptoms negatively predicted wives’ satisfaction (b = −.42, p = .005), whereas at low levels of husbands’ discrimination (1 SD below the mean), this association was not significant (b = .09, p = .689). Second, the wives’ marital satisfaction by husbands’ discrimination interaction predicted husbands’ depressive symptoms (β = −.16, p = .035). Post hoc probing (Figure 2b) indicated that, when husbands experienced more discrimination, wives’ satisfaction negatively predicted husbands’ depressive symptoms (b = −.10, p = .041), whereas this association was not significant when husbands experienced low levels of discrimination (b = .03, p = .339). Third, the husbands’ marital satisfaction by wives’ discrimination interaction predicted wives’ depressive symptoms (β = .21, p = .020). Post hoc probing (Figure 2c) revealed that, when wives experienced more discrimination, husbands’ satisfaction positively predicted wives’ depressive symptoms (b = 0.09, p = .049), although this association was not significant when wives experienced low levels of discrimination (b = −.07, p = .085).
Table 3.
Unstandardized Coefficients, Standard Errors, p Values, and 95% Confidence Intervals for Moderation of the Links between Time 1 Depressive Symptoms and Time 2 Marital Satisfaction by Time 1 Experiences of Discrimination
| Husbands’ Marital Satisfaction (T2) | Wives’ Marital Satisfaction (T2) | |||||||
|---|---|---|---|---|---|---|---|---|
| T1 Variables | B | SE | p-value | 95% CI | B | SE | p-value | 95% CI |
| Actor DS | −.391 | .136 | .004 | [−.658, −.124] | −.335 | .151 | .027 | [−.631, −.039] |
| Partner DS | −.465 | .201 | .020 | [−.859, −.071] | −.163 | .144 | .257 | [−.445, .119] |
| Actor ED | −.012 | .100 | .905 | [−.208, .184] | .022 | .115 | .848 | [−.203, .247] |
| Partner ED | −.094 | .098 | .336 | [−.286, .098] | .218 | .108 | .044 | [.006, .430] |
| Actor DS x Actor ED | .013 | .018 | .470 | [−.022, .048] | −.034 | .028 | .222 | [−.089, .021] |
| Actor DS x Partner ED | −.001 | .025 | .984 | [−.050, .048] | −.017 | .025 | .496 | [−.066, .032] |
| Partner DS x Actor ED | −.045 | .032 | .156 | [−.108, .018] | .004 | .023 | .857 | [−.041, .049] |
| Partner DS x Partner ED | −.050 | .028 | .072 | [−.105, .005] | −.037 | .018 | .047 | [−.072, −.002] |
| Actor MS | .641 | .070 | .000 | [.504, .778] | .535 | .078 | .000 | [.382, .688] |
| Partner MS | .165 | .066 | .012 | [.036, .294] | .016 | .087 | .854 | [−.155, .187] |
Note. B = Unstandardized Coefficient, SE = Standard Error, CI = Confidence Interval, DS = Depressive Symptoms, MS = Marital Satisfaction, T1 = Time 1, T2 = Time 2, and ED = Experiences of Discrimination.
Table 4.
Unstandardized Coefficients, Standard Errors, p Values, and 95% Confidence Intervals for Moderation of the Links between Time 1 Marital Satisfaction and Time 2 Depressive Symptoms by Time 1 Experiences of Discrimination
| Husbands’ Depressive Symptoms (T2) | Wives’ Depressive Symptoms (T2) | |||||||
|---|---|---|---|---|---|---|---|---|
| T1 Variables | B | SE | p-value | 95% CI | B | SE | p-value | 95% CI |
| Actor MS | −.011 | .038 | .767 | [−.085, .063] | −.020 | .027 | .442 | [−.073, .033] |
| Partner MS | −.033 | .027 | .223 | [−.086, .020] | .012 | .029 | .681 | [−.045, .069] |
| Actor ED | .010 | .060 | .871 | [−.108, .128] | .063 | .066 | .333 | [−.066, .192] |
| Partner ED | −.105 | .071 | .140 | [−.244, .034] | −.005 | .052 | .921 | [−.107, .097] |
| Actor MS x Actor ED | .003 | .007 | .704 | [−.011, .017] | −.005 | .005 | .265 | [−.015, .005] |
| Actor MS x Partner ED | .003 | .006 | .631 | [−.009, .015] | .001 | .005 | .771 | [−.009, .011] |
| Partner MS x Actor ED | −.010 | .005 | .039 | [−.020, .00] | .012 | .005 | .010 | [.002, .022] |
| Partner MS x Partner ED | .005 | .005 | .336 | [−.005, .015] | .002 | .004 | .592 | [−.006, .010] |
| Actor DS | .629 | .079 | .000 | [.474, .784] | .506 | .107 | .000 | [.296, .716] |
| Partner DS | .044 | .088 | .618 | [−.128, .216] | −.042 | .073 | .561 | [−.185, .101] |
Note. B = Unstandardized Coefficient, SE = Standard Error, CI = Confidence Interval, DS = Depressive Symptoms, MS = Marital Satisfaction, T1 = Time 1, T2 = Time 2, and ED = Experiences of Discrimination.
Figure 2.
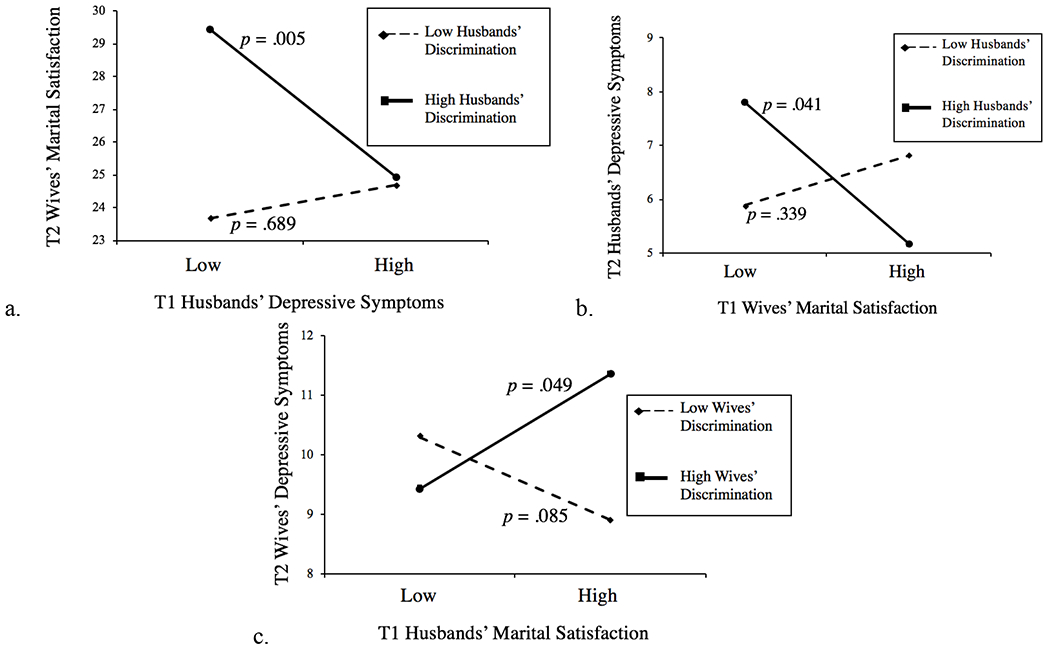
The top left panel (a) depicts the prospective association between husbands’ depressive symptoms and wives’ marital satisfaction at high versus low levels of husbands’ experiences of discrimination. The top right panel (b) depicts the prospective association between wives’ marital satisfaction and husbands’ depressive symptoms at high versus low levels of husbands’ experiences of discrimination. The bottom panel (c) depicts the prospective association between husbands’ marital satisfaction and wives’ depressive symptoms at high versus low levels of wives’ experiences of discrimination. T1 = Time 1, T2 = Time 2.
Tables 5 and 6 present the unstandardized coefficients, p values, and CIs for Moderation Models 3 and 4 examining the moderating effect of racial centrality on the links between T1 depressive symptoms and T2 marital satisfaction (χ2(8) = 8.67, p = .371, RMESA = .02; SRMR = .05; CFI = 1.00) and between T1 marital satisfaction and T2 depressive symptoms (χ2(8) = 8.96, p = .346, RMESA = .03; SRMR = .05; CFI = .99), respectively. Two significant interactions emerged. First, the wives’ depressive symptoms by wives’ racial centrality interaction predicted husbands’ marital satisfaction (β = −.23, p = .003). Post hoc probing (Figure 3a) indicated that, at high levels of wives’ racial centrality, wives’ depressive symptoms negatively predicted husbands’ satisfaction (b = −.92, p < .001), whereas this association was not significant at low levels of wives’ racial centrality (b = .28, p = .166). Second, the husbands’ marital satisfaction by husbands’ racial centrality interaction predicted husbands’ depressive symptoms (β = −.12, p = .044). Post hoc probing (Figure 3b) indicated that husbands’ marital satisfaction negatively predicted their own depressive symptoms at high levels of husbands’ racial centrality (b = −.08, p = .169) but positively predicted their depressive symptoms at low levels of racial centrality (b = .06, p = .175). Neither slope was significantly different from zero, however, meaning that we can only conclude that these differed as a function of husbands’ racial centrality.
Table 5.
Unstandardized Coefficients, Standard Errors, p Values, and 95% Confidence Intervals for Moderation of the Links between Time 1 Depressive Symptoms and Time 2 Marital Satisfaction by Time 1 Racial Centrality
| Husbands’ Marital Satisfaction (T2) | Wives’ Marital Satisfaction (T2) | |||||||
|---|---|---|---|---|---|---|---|---|
| T1 Variables | B | SE | p-value | 95% CI | B | SE | p-value | 95% CI |
| Actor DS | −.408 | .131 | .002 | [−.665, −.151] | −.342 | .183 | .061 | [−.701, .011] |
| Partner DS | −.319 | .158 | .043 | [−.629, −.009] | −.135 | .129 | .297 | [−.388, .118] |
| Actor RC | −2.050 | 1.359 | .132 | [−4.714, .614] | .578 | 1.476 | .695 | [−2.315, 3.471] |
| Partner RC | −1.628 | 1.088 | .135 | [−3.760, .504] | .646 | 1.348 | .623 | [−1.996, 3.288] |
| Actor DS x Actor RC | −.136 | .217 | .529 | [−.561, .289] | .215 | .331 | .516 | [−.434, .864] |
| Actor DS x Partner RC | .339 | .242 | .161 | [−.135, .813] | .279 | .408 | .493 | [−.521, 1.079] |
| Partner DS x Actor RC | .268 | .408 | .512 | [−.532, 1.068] | −.434 | .246 | .077 | [−.916, .048] |
| Partner DS x Partner RC | −1.043 | .242 | .000 | [−1.517, −.569] | −.467 | .335 | .163 | [−1.124, .190] |
| Actor MS | .629 | .065 | .000 | [.502, .756] | .549 | .083 | .000 | [.386, .712] |
| Partner MS | .150 | .063 | .016 | [.027, .273] | −.003 | .081 | .974 | [−.162, .156] |
Note. B = Unstandardized Coefficient, SE = Standard Error, CI = Confidence Interval, DS = Depressive Symptoms, MS = Marital Satisfaction, T1 = Time 1, T2 = Time 2, and RC = Racial Centrality.
Table 6.
Unstandardized Coefficients, Standard Errors, p Values, and 95% Confidence Intervals for Moderation of the Links between Time 1 Marital Satisfaction and Time 2 Depressive Symptoms by Time 1 Racial Centrality
| Husbands’ Depressive Symptoms (T2) | Wives’ Depressive Symptoms (T2) | |||||||
|---|---|---|---|---|---|---|---|---|
| T1 Variable | B | SE | p-value | 95% CI | B | SE | p-value | 95% CI |
| Actor MS | −.008 | .037 | .824 | [−.081, .065] | −.013 | .028 | .642 | [−.068, .042] |
| Partner MS | −.028 | .028 | .320 | [−.083, .027] | .025 | .030 | .397 | [−.034, .084] |
| Actor RC | −.814 | .997 | .414 | [−2.768, 1.140] | −.271 | .728 | .710 | [−1.698, 1.156] |
| Partner RC | .646 | .587 | .271 | [−.505, 1.797] | .302 | .602 | .616 | [−.878, 1.482] |
| Actor MS x Actor RC | −.119 | .057 | .037 | [−.231, −.007] | .015 | .059 | .803 | [−.101, .131] |
| Actor MS x Partner RC | .080 | .050 | .111 | [−.018, .178] | −.047 | .055 | .393 | [−.155, .061] |
| Partner MS x Actor RC | −.018 | .059 | .768 | [−.134, .098] | .037 | .046 | .422 | [−.053, .127] |
| Partner MS x Partner RC | .019 | .061 | .756 | [−.101, .139] | .018 | .046 | .692 | [−.072, .108] |
| Actor DS | .589 | .082 | .000 | [.428, .750] | .559 | .110 | .000 | [.343, .775] |
| Partner DS | .047 | .087 | .589 | [−.124, .218] | .001 | .071 | .994 | [−.138, .140] |
Note. B = Unstandardized Coefficient, SE = Standard Error, CI = Confidence Interval, DS = Depressive Symptoms, MS = Marital Satisfaction, T1 = Time 1, T2 = Time 2, and RC = Racial Centrality.
Figure 3.
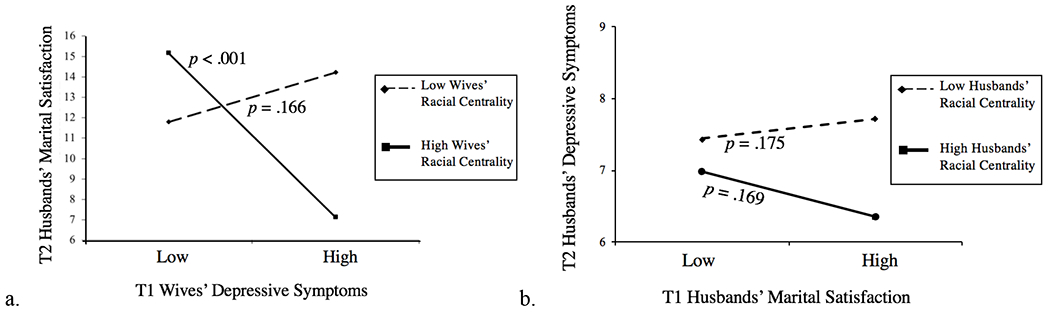
The left panel (a) depicts the prospective association between wives’ depressive symptoms and husbands’ marital satisfaction at high versus low levels of wives’ racial centrality. The right panel (b) depicts the prospective association between husbands’ marital satisfaction and husbands’ depressive symptoms at high versus low levels of husbands’ racial centrality. T1 = Time 1; T2 = Time 2.
Given that multiple tests of interactions were conducted (i.e., four models with four interactions in each model), we applied the Benjamini-Hochberg false discovery rate as a conservative test of the interactions (Benjamini & Hochberg, 1995). The moderating effect of wives’ racial centrality on the association between wives’ depressive symptoms and husbands’ marital satisfaction remained significant. However, the other interactions were not statistically significant using this more conservative test.
Discussion
This study was designed to assess the longitudinal associations between depressive symptoms and marital satisfaction among Black couples and to test potential moderating effects of experiences of discrimination and racial centrality in these linkages. As such, this investigation directly answers the call for research on the health and well-being of Black families (McNeil Smith et al., 2018), taking the novel steps of assessing associations between mental health and relationship quality among Black couples and examining them within a dyadic, longitudinal, and culturally specific context. Our findings revealed that, after accounting for stability in marital satisfaction, spouses’ depressive symptoms predicted their own and their spouses’ marital satisfaction one year later. Further, wives’ depressive symptoms predicted relative declines in husbands’ martial satisfaction when wives reported high racial centrality. Together, these findings add to the literature documenting links between mental health and intimate relationship quality among Black couples and underscore the importance of taking into account the sociocultural context in which couples are embedded.
In contrast to prior work demonstrating bidirectional, within-person associations between depressive symptoms and relationship satisfaction (Davila et al., 2003), we did not find significant main effects of marital satisfaction on depressive symptoms for either husbands or wives. However, depressive symptoms predicted lower marital satisfaction for self and partner, a pattern consistent with theory and empirical research. This pattern suggests that negative appraisals and stressful social experiences of depressed individuals can lead to negative perceptions of relationship quality and decreases in marital satisfaction for both self and partner (Hammen, 2006; Whisman & Beach, 2015). Future research should directly assess social interaction patterns and negative appraisals to clarify whether these theorized mechanisms mediate the links between depressive symptoms and marital satisfaction among Black couples.
Although not the focus of the current investigation, we also found evidence of gender differences in the partner effects of marital satisfaction. Consistent with prior research suggesting that wives may serve as “emotional barometers” in heterosexual relationships given their relatively greater attunement to relationship functioning (Floyd & Markman, 1983), wives’ marital satisfaction was a stronger predictor of husbands’ satisfaction than the reverse. In contrast to marital satisfaction linkages, we found no partner effects linking spouses’ depressive symptoms. This pattern differs from findings on emotional contagion in predominately White samples (Whisman & Uebelacker, 2009) but is consistent with research suggesting that Black couples exhibit less interdependence in mental health, possibly due to retentions of West African cultural traditions to organize families around blood relatives rather than marital unions (O’Neal, Wickrama & Bryant, 2014). This tradition may result in strong allegiances with extended family members but weaken couple linkages in mental health. Future research should examine how extended family and kinship networks combine with couple relationship processes in Black couples’ mental health.
Our examination of racial centrality also contributed to the literature on mental health and intimate relationships among Black couples, supporting the growing body of research on the importance of racial identity for romantic relationships. By documenting the role of wives’ racial identity in husbands’ relationship satisfaction, our findings added to prior research that found links between husbands’ racial attitudes and their own marital reports (Kelly & Floyd, 2006). Although we originally conceptualized racial centrality as a protective factor for relationships (LaTaillade, 2006), results indicated that wives’ depressive symptoms negatively predicted husbands’ marital satisfaction when wives’ racial centrality was high. It may be that individuals with a stronger sense of Black identity are more inclined to provide for their spouses’ “physical, intellectual, emotional, and social stimulation” (Bell et al., 1990; p. 171). Indeed, husbands’ marital satisfaction was highest when wives reported fewer depressive symptoms and high racial centrality. Wives high in racial centrality but with more depressive symptoms, however, may disengage from this “stimulation” process, thereby decreasing husbands’ satisfaction. Wives low in centrality may seldom provide this kind of stimulation that increases relational interdependence, so their depressive symptoms may not impact husbands’ satisfaction. Future work is needed to determine if racial centrality increases interdependence in couple relationships in other samples.
Moderation Effects for Future Study
We observed four other significant interactions that were not robust to the multiple testing correction but were consistent with theory and prior research. Although inconclusive, these patterns may suggest avenues for future research. First, results suggested that husbands’ discrimination experiences may moderate the longitudinal links between their depressive symptoms and wives’ marital satisfaction and between wives’ satisfaction and husbands’ depressive symptoms. That is, when husbands experienced more discrimination, their depressive symptoms predicted lower marital satisfaction for wives, but wives’ marital satisfaction predicted fewer depressive symptoms for husbands. The latter effect is consistent with findings that negative effects of discrimination on Black men’s mental health were attenuated in the presence of high spousal support (McNeil, Fincham, & Beach, 2014). When wives are satisfied, they may escalate their support to protect their husbands from the negative consequences of discrimination. Given their orientations to close relationships, however, women may be more susceptible than men to their spouses’ distress: The combination of husbands’ discrimination experiences and depressive symptoms may result in wives’ lower levels of marital satisfaction.
Wives’ discrimination experiences may also moderate the link between their husbands’ marital satisfaction and their own depressive symptoms. When wives reported more discrimination, husbands’ marital satisfaction predicted relative increases in wives’ depressive symptoms. Although this pattern differs from the effects of husbands’ discrimination, it is consistent with findings that high spousal support does not attenuate the negative effects of discrimination for Black women (McNeil et al., 2014). When wives experience discrimination, they may focus on their romantic relationships, investing additional energy that results in husbands’ being more satisfied in their marriages but at the expense of wives’ mental health. In general, less is known about the impact of discrimination on Black women’s, as compared with Black men’s, mental health; thus, these findings are notable in documenting these gendered patterns. Together, these trends highlight the potentially deleterious effect of the “Black Superwoman” schema (Woods-Giscombé, 2010) and the cultural pressure felt by some Black women to protect Black men from the effects of racial trauma (Cowdery et al., 2009), effects that may be amplified by women’s gendered orientations to invest emotion, attention, and care in their romantic relationships, particularly in response to threat (Taylor et al., 2000). Future research should examine how discrimination intersects with gender dynamics among Black couples to affect both the mental health and relationship functioning of romantic partners.
A final possible moderation pattern was that the longitudinal link between husbands’ marital satisfaction and depressive symptoms was negative at high levels of levels of husbands’ racial centrality but was positive at low levels of racial centrality. This is consistent with theory and research on racial centrality as a protective factor but contrasts with our findings for the effects of wives’ racial centrality. Future research should examine potentially different functions of actors’ versus partner’s racial identity and whether these processes are gendered to clarify the conditions under which racial centrality serves as a protective or risk factor for Black couples.
Importantly, although these four patterns were congruent with psychological theories and some empirical literature, they should be viewed with caution given that they did not survive the multiple testing correction. These patterns provide direction for future research to determine whether these effects hold with larger samples with more statistical power.
Implications and Limitations
Our findings have practical significance. First, we found that Black couples’ mental health and relationship quality are linked both within and across partners and that these associations are influenced by the sociocultural context of discrimination experiences and racial centrality. As such, our results are congruent with the rationale for empirically supported relationship education programs such as Protecting Strong African American Families (Barton, Beach, Bryant, Lavner, & Brody, 2018) that serve as accessible, low-stigma methods for improving mental health and enhancing relationship quality among Black couples. Given that stigma for mental health treatment and mistrust of service providers still pose barriers to help-seeking among many Black Americans who experience psychological distress, culturally-informed relationship interventions may circumvent barriers typically associated with treatment to improve relationship quality while providing indirect benefit to mental health (Barton et al., 2018). Second, practitioners working with Black couples should assess spouses’ discrimination experiences and racial identity, in addition to couple satisfaction and mental health symptoms, as these factors may impact both spouses and the couple relationship (LaTaillade, 2006).
This investigation contributes to the scientific literature by virtue of its several strengths, including its dyadic, longitudinal design and formal examination of sociocultural factors relevant for influence Black couples. Limitations of the study, however, suggest directions for future research. First, this investigation focused on heterosexual couples from a relatively advantaged community sample with respect to income and education who were drawn from a single geographic region of the U.S. Future studies should include same-sex couples as well as samples that are more diverse with respect to demographic characteristics; clinical samples are essential to determine the extent to which our results are generalizable. Second, we relied exclusively on self-report measures. We took a conservative approach, minimizing shared method variance by including all autoregressive paths and including reports from two relationship partners, but future work should collect clinical interview measures of depression and/or observational measures of relationship quality. Third, although this was the first study to apply MEES theory within a family systems framework by assessing the moderating effect of discrimination and racial centrality on the associations between depressive symptoms and marital satisfaction for both spouses, we did not advance a priori hypotheses concerning specific moderating effects of gender. Further, although our study represented an advance over prior research, it may have been underpowered to detect moderated partner effects after accounting for multiple testing. As noted, these moderation results should be considered exploratory and highlight the vital need for additional research and focused data collection on marriage and mental health of Black couples.
In conclusion, this study addressed an important public health need—to improve understanding of the reciprocal influences of mental health and relationship satisfaction in Black couples. Our findings provided insights into these linkages by investigating them in the context of each partner’s experiences of discrimination and racial centrality, two sociocultural factors of significance to Black Americans. Future research that identifies the mechanisms by which mental health is associated with couple functioning will add nuance to the understanding of the relational context of mental health among Black couples and open up additional avenues for interventions designed to support the psychological and relational well-being of Black families.
Acknowledgments
This study was conducted in partial fulfillment of the requirements for the master of science degree at the Pennsylvania State University for August I. C. Jenkins and was supported by grant R01 HD32336 from the National Institute of Child Health and Human Development to Susan M. McHale and Ann C. Crouter, the Bunton Waller Fellowship to August I. C. Jenkins, the Karl R. and Diane Wendle Fink Early Career Professorship for the Study of Families to Steffany J. Fredman, grants KL2 TR002015 and UL1 TR002014 from the National Center for Advancing Translational Science to support Steffany J. Fredman’s time, and grant UL1 TR002014 to support Timothy R. Brick’s time. The content is solely the responsibility of the authors and does not necessarily represent the official views of the NIH. Results of this study were presented at the 2018 conference for the National Council of Family Relations, San Diego, CA. We thank Gregory Fosco for feedback on the manuscript, Peter Molenaar for guidance with data analysis, and Christiana Awosan for assistance with interpretation of the findings.
Contributor Information
August I. C. Jenkins, Department of Human Development and Family Studies, The Pennsylvania State University
Steffany J. Fredman, Department of Human Development and Family Studies, The Pennsylvania State University
Yunying Le, Department of Human Development and Family Studies, The Pennsylvania State University.
Xiaoran Sun, Department of Human Development and Family Studies, The Pennsylvania State University.
Timothy R. Brick, Department of Human Development and Family Studies, The Pennsylvania State University
Susan M. McHale, Department of Human Development and Family Studies, The Pennsylvania State University
Olivenne D. Skinner, Merrill Palmer Skillman Institute, Wayne State University
References
- Barton AW, Beach SRH, Bryant CM, Lavner JA, & Brody GH (2018). Stress spillover, African Americans’ couple and health outcomes, and the stress-buffering effect of family-centered prevention. Journal of Family Psychology, 32, 186–196. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Beach SRH, Katz J, Kim S, & Brody GH (2003). Prospective effects of marital satisfaction on depressive symptoms in established marriages: A dyadic model. Journal of Social and Personal Relationships, 20, 355–371. [Google Scholar]
- Bell YR, Bouie CL, & Baldwin JA (1990). Afrocentric cultural consciousness and African-American male-female relationships. Journal of Black Studies, 21, 162–189. [Google Scholar]
- Benjamini Y, & Hochberg Y (1995). Controlling the false discovery rate: A practical and powerful approach to multiple testing. Journal of the Royal Statistical Society, 57, 289–300. [Google Scholar]
- Brown TN, Williams DR, Jackson JS, Neighbors HW, Torres M, Sherrill SL, & Brown KT (2000) “Being black and feeling blue”: The mental health consequences of racial discrimination. Race and Society, 2, 117–131. [Google Scholar]
- Bryant CM, Wickrama KAS, Bolland J, Bryant BM, Cutrona CE, & Stanik CE (2010). Race matters, even in marriage: Identifying factors linked to marital outcomes for African Americans. Journal of Family Theory & Review, 2, 157–174. [Google Scholar]
- Bulanda JR, & Brown SL (2007). Race-ethnic differences in marital quality and divorce. Social Science Research, 36, 945–967. [Google Scholar]
- Carroll G (1998). Mundane extreme environmental stress and African American families: A case for recognizing different realities. Journal of Comparative Family Studies, 29, 271–284. [Google Scholar]
- Clavél FD, Cutrona CE, & Russell DW (2017). United and divided by stress: How stressors differentially influence social support in African American couples over time. Personality and Social Psychology Bulletin, 43, 1050–1064. [DOI] [PubMed] [Google Scholar]
- Cohen J (1988). Statistical power analysis for the behavioral sciences. (2nd ed.). Hillsdale, NJ: Erlbaum. [Google Scholar]
- Cowdery RS, Scarborough N, Knudson-Martin C, Seshadri G, Lewis ME, & Mahoney AR (2009). Gendered power in cultural contexts: Part II. Middle class African American heterosexual couples with young children. Family Process, 48, 25–39. [DOI] [PubMed] [Google Scholar]
- Coyne JC (1976). Depression and the response of others. Journal of Abnormal Psychology, 85, 186–193. [DOI] [PubMed] [Google Scholar]
- Davila J, Karney BR, Hall TW, & Bradbury TN (2003). Depressive symptoms and marital satisfaction: Within-subject associations and the moderating effects of gender and neuroticism. Journal of Family Psychology, 17, 557–570. [DOI] [PubMed] [Google Scholar]
- Fagan J (2009). Relationship quality and changes in depressive symptoms among urban, married African Americans, Hispanics, and Whites. Family Relations, 58, 259–274. [Google Scholar]
- Floyd FJ, & Markman HJ (1983). Observational biases in spousal observations: Toward a cognitive behavioral model of marriage. Journal of Consulting and Clinical Psychology, 51, 450–457. [DOI] [PubMed] [Google Scholar]
- Hammen C (2006). Stress generation in depression: Reflections on origins, research, and future directions. Journal of Clinical Psychology, 62, 1065–1082. [DOI] [PubMed] [Google Scholar]
- Hu L, & Bentler PM (1999). Cutoff criteria for fit indexes in covariance structure analysis: Conventional criteria versus new alternatives. Structural Equation Modeling, 6, 1–55. [Google Scholar]
- Huston TL, McHale SM, & Crouter AC (1986). When the honeymoon’s over: Changes in the marriage relationship over the first year. In Gilmour R & Duck S (Eds.), The emerging field of personal relationships (pp. 109–132). Hillsdale, NJ: Erlbaum. [Google Scholar]
- Kelly S, & Floyd FJ (2006). Impact of racial perspectives and contextual variables on marital trust and adjustment for African American couples. Journal of Family Psychology, 20, 79–87. [DOI] [PubMed] [Google Scholar]
- Kenny DA, Kashy DA, & Cook WL (2006). The analysis of dyadic data. New York: Guilford. [Google Scholar]
- Kessler RC, Mickelson KD, & Williams DR (1999). The prevalence, distribution, and mental health correlates of perceived discrimination in the United States. Journal of Health and Social Behavior, 40, 208–230. [PubMed] [Google Scholar]
- Kouros CD, Papp LM, & Cummings EM (2008). Interrelations and moderators of longitudinal links between marital satisfaction and depressive symptoms among couples in established relationships. Journal of Family Psychology, 22, 667–677. [DOI] [PubMed] [Google Scholar]
- LaTaillade JJ (2006). Considerations for treatment of African American couple relationships. Journal of Cognitive Psychotherapy, 20, 341–358. [Google Scholar]
- Lincoln KD, & Chae DH (2010). Stress, marital satisfaction, and psychological distress among African Americans. Journal of Family Issues, 31, 1081–1105. [Google Scholar]
- MacKenzie J, Smith TW, Uchino B, White PH, Light KC, & Grewen KM (2014). Depressive symptoms, anger/hostility, and relationship quality in young couples. Journal of Social and Clinical Psychology, 33, 380–396. [Google Scholar]
- McHale SM, Crouter AC, Kim JY, Burton LM, Davis KD, Dotterer AM, & Swanson DP (2006). Mothers’ and fathers’ racial socialization in African American families: Implications for youth. Child Development, 77, 1387–1402. [DOI] [PubMed] [Google Scholar]
- McNeil SN, Fincham FD, & Beach SR (2014). Does spousal support moderate the association between perceived racial discrimination and depressive symptoms among African American couples? Family Process, 53, 109–119. [DOI] [PubMed] [Google Scholar]
- McNeil Smith S & Landor A (2018). Toward a better understanding of African American families: Development of the sociocultural family stress model. Journal of Family Theory & Review, 10, 434–450. [Google Scholar]
- Minuchin P (1985). Families and individual development: Provocations from the field of family therapy. Child Development, 56, 289–302. [PubMed] [Google Scholar]
- Murry VM, Brown PA, Brody GH, Cutrona CE, & Simons RL (2001). Racial discrimination as a moderator of the links among stress, maternal psychological functioning, and family relationships. Journal of Marriage and Family, 63, 915–926. [Google Scholar]
- Muthén LK, & Muthén BO (1998-2012). Mplus User’s Guide. Seventh Edition. Los Angeles, CA: Muthén & Muthén. [Google Scholar]
- O’Neal CW, Wickrama KAS, & Bryant CM (2014). Control over work, positive self, and health among African American husbands and wives. Journal of Family Issues, 35, 384–410. [Google Scholar]
- Peters MF, & Massey G (1983). Mundane extreme environmental stress in family stress theories: The case of Black families in White America. Marriage & Family Review, 6, 193–218. [Google Scholar]
- Radloff LS (1977). The CES-D scale: A self-report depression scale for research in the general population. Applied Psychological Measurement, 1, 385–401. [Google Scholar]
- Sellers RM, Smith MA, Shelton JN, Rowley SA, & Chavous TM (1998). Multidimensional model of racial identity: A reconceptualization of African American racial identity. Personality and Social Psychology Review, 2, 18–39. [DOI] [PubMed] [Google Scholar]
- Settles IH, Navarrete CD, Pagano SJ, Abdou CM, & Sidanius J (2010). Racial identity and depression among African American women. Cultural Diversity and Ethnic Minority Psychology, 16, 248–255. [DOI] [PubMed] [Google Scholar]
- Shorter-Gooden K (2004). Multiple resistance strategies: How African American women cope with racism and sexism. Journal of Black Psychology, 30, 406–425. [Google Scholar]
- Jean Y & Feagin JR (1998). The family costs of white racism: The case of African American families. Journal of Comparative Family Studies, 29, 297–312. [Google Scholar]
- Sutton TE, Simons LG, Simons RL, & Cutrona C (2017). Psychological distress, couple interactions, and parenting: A dyadic analysis of African American couples. Journal of Marriage and Family, 79, 850–864. [Google Scholar]
- Taylor RJ, Chae DH, Chatters LM, Lincoln KD, & Brown E (2012). DSM-IV 12-month and lifetime major depressive disorder and romantic relationships among African Americans. Journal of Affective Disorders, 142, 339–342. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Taylor SE, Klein LC, Lewis BP, Gruenewald TL, Gurung RAR, & Updegraff JA (2000). Biobehavioral responses to stress in females: Tend-and-befriend, not fight-or-flight. Psychological Review, 107, 411–429. [DOI] [PubMed] [Google Scholar]
- Trail TE, Goff PA, Bradbury TN, & Karney BR (2012). The costs of racism for marriage: How racial discrimination hurts, and ethnic identity protects, newlywed marriages among Latinos. Personality and Social Psychology Bulletin, 38, 454–465. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Walton QL, & Payne JS (2016). Missing the mark: Cultural expressions of depressive symptoms among African-American women and men. Social Work in Mental Health, 14, 637–657. [Google Scholar]
- Whisman MA (2001). The association between depression and marital dissatisfaction. In Beach SRH (Eds.), Marital and family processes in depression: A scientific foundation for clinical practice (pp. 3–24). Washington, DC: American Psychological Association. [Google Scholar]
- Whisman MA, & Beach SRH (2015). Couple therapy and depression. In Gurman AS, Lebow JL & Synder DK (Eds.), Clinical handbook of couple therapy (pp. 585–605). New York: Guilford. [Google Scholar]
- Whisman MA, & Uebelacker LA (2009). Prospective associations between marital discord and depressive symptoms in middle-aged and older adults. Psychology and Aging, 24, 184–189. [DOI] [PubMed] [Google Scholar]
- Woods-Giscombé CL (2010). Superwoman schema: African American women’s views on stress, strength, and health. Qualitative Health Research, 20, 668–683. [DOI] [PMC free article] [PubMed] [Google Scholar]