

Abstract
Social support after sexual assault is important for recovery, but violence and recovery may also challenge relationships. We examined functional and structural social support changes following sexual assault and their association with mental health. College women (N=544) with and without a sexual assault history completed a cross-sectional survey assessing current and past egocentric social networks. Functional support (perceived global support, assault disclosure, perceived helpfulness of responses) and structural support (network density, size, retention) were examined. Multilevel models revealed that, relative to non-survivors, survivors reported smaller, less dense past networks, but similarly sized current networks. Survivors retained less of their networks than non-survivors, and network members who provided unhelpful responses to disclosure were less likely to be retained. Structural equation modeling revealed that, among survivors, perceived unhelpful responses to disclosure and a greater loss of network members were associated with worse mental health. Findings suggest that survivors may experience a restructuring of social networks following sexual assault, especially when network members respond in unhelpful ways to disclosure. Although survivors appeared to build new relationships, this restructuring was associated with more mental health problems. It is possible that interventions to improve post-assault social network retention may facilitate recovery.
Keywords: trauma, rape, social support, social network analysis, recovery
Sexual assault is a pervasive problem among college women. Prevalence estimates indicate that upwards of 20–25% of college women experience sexual assault victimization (Fedina et al., 2018). Numerous studies have linked sexual assault to increased risk for mental health problems, including posttraumatic stress disorder (PTSD), depression, and anxiety (see Dworkin et al., 2017). Clarifying how post-assault experiences contribute to mental health outcomes is vital to informing interventions aimed at promoting recovery.
Social Support and Mental Health
Recovery from sexual assault is fundamentally embedded in survivors’ social contexts, which can be a source of protection or risk for mental health (Dworkin & Weaver, 2021; Joseph et al., 1997; Williams & Joseph, 1999). Perceived global functional support, or the perception that social support is available, is consistently associated with less trauma-related psychopathology in cross-sectional and longitudinal studies of trauma exposure (Guay et al., 2006; Wang et al., 2021), including sexual assault (Littleton, 2010; Ullman, 1999). Meta-analyses indicate that greater perceived global support (i.e., not necessarily linked to the trauma) is one of the strongest correlates of less severe PTSD (Brewin et al., 2000; Ozer et al., 2003), suggesting the importance of social support for survivors’ recovery.
Within this social context, over two thirds of sexual assault survivors disclose their assault to others (66–79.5%; Hequembourg et al., 2021; Ruggiero et al., 2004; Ullman et al., 2007). The assault-specific functional support that survivors receive in response to these disclosures can also have important implications for recovery (Ullman, 2010). Recent meta-analyses suggest that, although positive responses received from others are not consistently protective, a clear relation exists between receiving negative responses and worse mental health in sexual assault survivors (Dworkin et al., 2019; Zalta et al., 2021). Because survivors do not always perceive positive responses to be helpful and negative responses to be unhelpful (Dworkin et al., 2018), it is important to examine perceived assault-specific support in relation to psychopathology. Indeed, perceptions of these responses are associated with psychopathology, such that positive perceptions of assault-specific support (e.g., perceiving responses to be more helpful) are associated with better mental health, and negative perceptions of assault-specific support (e.g., perceiving responses to be less helpful) are associated with worse mental health (Dworkin et al., 2019). Both perceived and received functional assault-specific support represent potentially modifiable risk factors that may be amenable to intervention (e.g., Edwards et al., 2022).
Most research on sexual assault survivors’ social contexts and mental health outcomes has examined the aforementioned functional aspects of social support. However, there are also structural aspects of social support, which can be examined within a social network approach. Measuring an individual’s social network facilitates understanding of the social context (e.g., size and interconnectedness of support groups) in which the aforementioned functional aspects of social support occur. Assessing social networks allows for consideration of a wide range of structural social support constructs, such as the number of close friends one has, and the degree to which a person belongs to a close-knit friend group (Holt-Lunstad et al., 2017). Structural support has received less attention in sexual assault research (for exceptions, see Dworkin et al., 2016; Um et al., 2021), though it has been linked to mental health outcomes in other trauma survivors (see Zalta et al., 2021). For example, after a natural disaster, adults who felt close to fewer people reported more depressive symptoms (Bryant et al., 2017). Similarly, having a smaller social network was associated with PTSD in refugees (Lee & Yuom, 2011), women experiencing domestic violence (Levendosky et al., 2004), and mixed trauma samples (Olson et al., 2021). Adults with a trauma history were also more likely to have PTSD when their social network had fewer types of relationships (e.g., friends, neighbors; Platt et al., 2014). In the one known study connecting structural aspects of the social network to sexual assault outcomes, Um et al. (2021) found that female Korean refugees who experienced pre-migration sexual violence were less likely to identify family members in their social network, and this lack of kin ties was associated with greater suicidal ideation. Taken together, this small but growing literature suggests a connection between smaller networks and more severe post-trauma mental health problems.
Another risk factor for mental health problems is being a part of a social network that is not interconnected (i.e., low network density). Navigating between disconnected network members may require more resources (e.g., spending time with each person separately) and involve being an intermediary of potential conflicts. Indeed, adolescent girls whose social networks involved fewer interconnected friends were more likely to report suicidal ideation (Bearman & Moody, 2004). After trauma, having close relationships with individuals who are not themselves interconnected has also been associated with risk for PTSD (Bryant et al., 2017; for exception, see Lee & Yuom, 2011). This lack of cohesion and connectedness amongst network members may make it less likely that others will collectively notice early signs of mental health struggles and provide support. In this way, the structure of the social network in which survivors recover may have important implications for mental health outcomes.
Trauma and Changes in Social Support
Trauma recovery processes are not only affected by social contexts, but may also lead to changes in survivors’ social contexts over time (Kaniasty & Norris, 1993; Wagner et al., 2016). According to the conservation of resources theory (Hobfoll & Lilly, 1993), social support is one of many resources that may be lost as part of experiencing and recovering from stressful life events. Cross-sectional research has established that a history of trauma, including sexual trauma, is associated with lower levels of perceived global functional support (e.g., Bruwer et al., 2008; Burrage et al., 2021; Kao et al., 2014). Regarding structural support, cross-sectional research has also revealed smaller social networks among individuals with a history of partner violence (Coohey, 2007; Katerndahl et al., 2013; Levendosky et al., 2004). Social network characteristics beyond size have rarely been examined in relation to trauma, but the few studies that exist have revealed inconsistent findings. Social network diversity (i.e., variability in the social roles represented in one’s network) has been associated with sexual violence (Um et al., 2021), but not general trauma history (Olson et al., 2021). Further, Katerndahl et al. (2013) found no differences in social network density between women in violent relationships and a comparison group.
Fewer studies have directly assessed both pre- and post-trauma social support. In a notable exception, participants in a longitudinal study occurring at the time of Hurricane Katrina evidenced significant reductions in perceived global support from pre- to post-hurricane (Chan et al., 2015; Lowe et al., 2010), suggesting trauma may lead to reductions in global functional social support. Changes in structural support have also been observed following specific forms of violence. A recent study involving retrospective interviews revealed that women’s social network size increased upon leaving an abusive partner and entering a shelter, and decreased after leaving the shelter, but as network size increased, the interconnectedness of the network decreased (Nolet et al., 2021). In a longitudinal study, maltreated adolescents had smaller networks in each of three yearly assessments than comparisons (Negriff et al., 2015). These studies highlight the potential effect of interpersonal violence on social network structures, but it remains unclear if findings would generalize to sexual assault survivors.
Sexual assault may have specific implications for functional and structural social support changes. For instance, when a sexual assault survivor discloses to a network member, that person may rally resources, increasing perceived and received assault-specific functional support.
Alternatively, disclosure could be met with negative responses that threaten a previously close relationship. For instance, network members may distance themselves from survivors if they do not know how to help, or survivors may distance themselves from network members whom they perceive to have betrayed their trust following a disclosure. In addition, because sexual assaults are commonly perpetrated by individuals known to the survivor (Smith et al., 2017), the perpetrator may also be known to other network members and the assault experience may threaten the cohesion of the network as a whole.
Indeed, changes in social relationships have been documented following disclosure of sexual assault. In a qualitative study of college students who had experienced a sexual assault (DeLoveh & Cattaneo, 2017), nearly all survivors discussed concerns about the impact of the assault on their perceptions of global functional support, including difficulty trusting friends whom they had expected would keep them safe the night of the assault. In another retrospective qualitative study of sexual assault survivors, the effect of assault-specific functional support on relationships was highlighted. Following disclosure, 51% of relationships grew worse or stayed poor when the other person responded in ways that survivors deemed harmful, and 90% of relationships grew closer or stayed close when the other person responded in ways that survivors deemed helpful (Ahrens & Aldana, 2012). Although structural support changes are indicated by these qualitative findings, additional work is needed to quantify how assault-specific functional support may relate to structural support changes.
Trauma-Related Changes in Social Support and Mental Health
Changes in social support may be relevant to understanding post-assault mental health. The conservation of resources theory suggests that trauma-related losses in social support may be detrimental to mental health due to the efforts needed to re-establish lost resources (Hobfoll & Lilly, 1993). This theory posits that individuals seek to avoid resource loss and gain new resources following stressful life events. Although there have been few direct tests of this theory in relation to trauma exposure, one longitudinal study that was occurring at the time of the Virginia Tech shootings assessed students’ perceptions of resource loss and gains (including global perceived functional support) since the shooting (Littleton et al., 2009). Resource loss 2 and 6 months after the shooting was associated with worse mental health at 6 months, suggesting post-trauma resource loss can have a serious impact.
Current Study
A small but growing body of research suggests that experiencing sexual assault may lead to changes in functional and structural social support, which could have implications for mental health outcomes. However, prior research is limited in several respects. First, examinations of trauma and social networks have largely depended on single timepoints (for exception, see Negriff et al., 2015), limiting understanding about trauma-related changes in structural support. Second, little research has used social network analysis to characterize structural support following trauma, potentially because such research is difficult to conduct on sensitive topics (Dworkin & Allen, 2017). Social network analysis could illuminate novel characteristics of structural support (e.g., size, interconnectedness) that may be important to understanding the broader social contexts in which global and assault-specific functional support are available. Third, there has been insufficient research examining structural support in relation to sexual assault specifically.
To address these gaps, we examined functional and structural support across two retrospectively assessed time periods in a sample of college women with and without a history of sexual assault. The retrospective design was indicated given the nascent state of this literature and difficulty prospectively capturing pre-assault social functioning. We aimed to evaluate (1) differences in structural support changes by sexual assault history, and among sexual assault survivors specifically, (2) the connection between perceived assault-specific functional support (i.e., helpfulness of responses to assault disclosure) and structural support changes, and (3) how perceived global functional support (i.e., overall perceptions of support availability), perceived assault-specific functional support, and changes in structural support were associated with mental health outcomes. First, we hypothesized that, relative to women without a sexual assault history, sexual assault survivors would report a greater reduction in overall network size and interconnection (i.e., density), while also retaining fewer individual network members over time. Second, focusing only on sexual assault survivors, we hypothesized that disclosure to a specific network member would increase the likelihood that this person would be retained in the current network. However, we expected that responses to disclosure perceived to be unhelpful from a given network member would decrease the likelihood of this person remaining in the network. Finally, we hypothesized that more positive perceptions of global functional support would be associated with fewer mental health problems, and that after controlling for disclosure, perceiving an unhelpful response from any network member or multiple network members would be associated with worse mental health. We also hypothesized unique effects of structural support on mental health, such that losing more members from the network, adding fewer network members, and having a greater loss in network density, would each be associated with more mental health problems.
Method
Participants and Procedures
Following Institutional Review Board approval, undergraduates aged 18 years and older were recruited to participate via a university subject pool. Participants received course credit for completing a 50-minute online survey on sexual assault, social support, help-seeking experiences, and mental health. A total of 1,111 students responded to at least some survey questions. The analytic sample was selected based on responses to sexual assault, social network, and gender questions. As detailed below, sexual assault screener questions were followed by an item assessing whether participants had endorsed any of the previous experiences. This follow-up item served as both an attention check and a prompt for branching. Participants were excluded if they did not answer any of the screener questions (n = 3), the follow-up question (n = 37), or had inconsistent responses between the two, signaling a lack of attention or understanding (n = 24). Social networks were retrospectively assessed for two 6-month time periods: (1) currently and (2) at a specified period in the past – either prior to the sexual assault, or for those without a sexual assault, a randomly assigned time of 1 to 4 years ago. To facilitate interpretation and comparability of these networks, participants were excluded if their “most meaningful” sexual assault took place within the past 6 months (n = 109) or 5 or more years ago (i.e., 60+ months; n = 10), or if they did not respond to the timing questions (n = 5). Because only 4.5% of the 375 men in the remaining sample reported experiencing a sexual assault and there were few remaining participants who did not identify as either men or women (2 participants identified as “other” and 1 participant did not indicate their gender), we limited analyses to women. We also excluded one participant who provided nonsensical text-based responses to the network survey.
The final analytic sample was 544 women, including 120 who experienced a sexual assault between 6 and 59 months ago. Participants were, on average, 19.36 years old (SD = 1.22, Range = 18–23) and 91.5% identified as heterosexual. The sample was 46.4% White, 28.7% Asian or Asian American, 9.4% Hispanic or Latinx, 7.2% Black or African American, 6.6% multi-racial, and 1.7% another race/ethnicity. Regarding year in college, 36.4% were in their first year, 30.5% second year, 20.0% third year, 11.9% fourth year, and 1.1% fifth year or later. Most participants lived on campus in dormitories (45.6%) or other on-campus housing (31.1%).
Measures
Sexual Assault
The Sexual Experiences Survey – Short Form Victimization (SES-SFV; Koss et al., 2007) was used to assess nonconsensual sexual experiences. The measure includes seven behaviorally specific question stems regarding the nature of the sexual contact involved (e.g., sexual contact, attempted or completed oral/anal/vaginal penetration) and five tactics used by the perpetrator (e.g., verbal coercion, incapacitation, actual or threatened force). Participants reported how many times (0 = 0 times to 3 = 3+ times) they had experienced any of the behaviors and tactics for two time periods: (1) between the age of 14 and 12 months prior to taking the survey and (2) in the past 12 months. Participants were then asked to indicate which assault was “most meaningful” if they endorsed multiple assaults, the date that the most meaningful assault occurred, and whether that assault happened more than 6 months ago. Follow-up questions were asked to characterize the most meaningful assault, including the relationship with and gender of the perpetrator, whether the survivor was intoxicated (“drunk or high”) at the time of the experience, whether participants were “physically injured (e.g., cut, bruised, sore),” and whether a weapon was involved. The SES has shown concurrent validity (Davis et al., 2014) as well as adequate test-retest reliability and good predictive validity (Johnson et al., 2017). A response of 1 or more times to any nonconsensual sexual experience since the age of 14 was coded as a history of sexual assault.
Structural Support
A single name generator prompt from the General Social Survey (Burt, 1984) was used. The prompt for the current network was: “Looking back over the last 6 months, who are the people with whom you discussed matters important to you?” (Burt, 1984; Marin & Hampton, 2007). Participants defined their network size by identifying up to 10 people (“alters”) with whom they discussed important matters. For each alter, we assessed gender, relationship type (response options: spouse, romantic partner, date, coworker, relative, friend, acquaintance, other), and frequency of communication (response options: at least once a day, at least once a week, at least once a month, at least once a year). Network density was assessed when participants were presented with a network member-by-member matrix and asked to report the interconnection (“ties”) between the alters (“mark the boxes corresponding to the pairs of people who discussed important matters with each other”). Given the focus on “pairs,” we assumed that all ties were reciprocated (i.e., if alter A talked to alter B, we assumed alter B also talked to alter A). Network density was computed as the proportion of alter-alter ties reported out of all possible ties.
The past network was generated using a similar approach to the current network, except that it asked participants to characterize their network at a time in the past. Participants were assigned to different periods of time based on whether they experienced sexual assault. Survivors were asked about their social network during the 6-month period prior to their “most meaningful” sexual assault. Those without a sexual assault history were randomly assigned via Qualtrics to a 6-month period either 1, 2, 3, or 4 years ago. These participants were given a set of questions to aid in remembering what was happening around that timeframe (e.g., “Think about a time 3 years ago—approximately [month and year]. At that time, where were you living?”). Participants were then presented a matrix of their past and current network members and were asked to indicate which members represented the same individuals. This was used to calculate network retention, defined as the percent of people in both past and current networks.
Functional Support
Perceived Global Support.
The Multidimensional Scale of Perceived Social Support (MSPSS; Zimet et al., 1988) was used to assess perceived global support for all participants (i.e., not necessarily linked to the assault). The MSPSS is a 12-item scale measuring three different types of support, with four items each assessing the support of family, friends, and a significant other on a 7-point Likert scale (1 = very strongly disagree to 7 = very strongly agree). The MSPSS has shown good internal reliability (α = .88) and test-retest reliability (α = .85; Zimet et al., 1988). In the current study, an overall mean score was computed (α = .95).
Disclosure and Perceived Assault-Specific Support.
Through a single item developed by the authors, survivors were asked to indicate which of the following was true for each alter identified on either past or current networks: (a) I told this person, and they were helpful to me, (b) I told this person, and they were NOT helpful to me, (c) I did not tell this person, but they found out from someone else, and (d) this person does not know about my sexual experience. From this response, variables were created to represent whether the survivor disclosed the assault to each alter (responses a and b were recoded as 1; responses c and d were recoded as 0), and if disclosed, whether the alter was unhelpful (response b was recoded as 1; responses a, c, and d were recoded as 0).
Mental Health Problems
Posttraumatic Stress.
The PTSD Checklist for DSM-IV (Weathers et al., 1993) was used to assess symptoms in relation to a “stressful experience.” The PCL is a 17-item survey that assesses DSM-IV symptoms of PTSD. Participants were asked to indicate how much each symptom bothered them within the past 4 months on a 5-point Likert scale from 0 = not at all to 4 = extremely. The PCL has strong internal consistency (α = .92–.98) and test-retest reliability (α = .96; Blanchard et al., 1996; Weathers et al., 1993). In the current study, sum and means were computed as specified for analyses below (α = .94).
Depression.
The anhedonic depression subscale of the short version of the Mood and Anxiety Symptom Questionnaire (MASQ; Clark & Watson, 1991) measured depressive symptoms. Participants rated their experience of eight symptoms during the last week on a 5-point Likert scale from 1 = very slightly or not at all to 5 = extremely. In past research, the anhedonic depression subscale has shown strong internal consistency (α = .94–.96; Bredemeir et al., 2010; Wardenaar et al., 2010), acceptable convergent validity, and good construct validity (Wardenaar et al., 2010). In the current study, mean scores were computed (α = .89).
Anxiety.
Within the short version of the MASQ (Clark & Watson, 1991), the anxious arousal subscale measured anxiety symptoms. Participants reported their experience of 17 symptoms during the last week on a 5-point Likert scale from 1 = very slightly or not at all to 5 = extremely. The anxious arousal subscale has previously shown strong internal consistency (α = .92; Wardenaar et al., 2010). In the current study, mean scores were computed (α = .91).
Data Analysis
Analyses were conducted in R version 4.0.3 (R Core Team, 2020). As a measure of structural support, social network characteristics were computed using the egor package (Krenz et al., 2021). Descriptive analyses were conducted to characterize the sample, including bivariate associations (Pearson correlations) and differences by sexual assault history (t-tests). We then examined (1) differences in structural support changes by sexual assault history, and among sexual assault survivors specifically, (2) the connection between received functional support and structural support changes, and (3) how perceived global functional support, perceived assault-specific functional support, and changes in structural support were associated with mental health outcomes.
First, regressions were conducted to evaluate predictors of network characteristics over time. Because network density and size were both measured at two timepoints, measures were nested within participants and multilevel models were estimated with a random intercept using the R package, glmmTMB (Brooks et al., 2017). Current age and years between the network were included as Level 2 (i.e., between-participant) covariates. The main and interactive effects of sexual assault (Level 2) and time (Level 1, within-participant; current vs. past network) were of primary interest. Because network retention requires consideration of both timepoints to create a single number (i.e., proportion of alters retained from the past network into the current network), a single-level regression model was used to evaluate sexual assault as a predictor, after controlling for current age and years between networks. Distributions for each outcome and appropriate modeling strategies were considered, as detailed below.
Second, among sexual assault survivors, perceived assault-specific functional support was examined as a predictor of structural support changes. Specifically, the likelihood of each individual alter in the past (pre-assault) network being retained to the current network was examined as a function of disclosure experiences with each alter. Because alters were nested within survivors, a multilevel model with random intercept was estimated using the R package, glmmTMB (Brooks et al., 2017), and a binomial distribution. Current age and years between the network were included as Level 2 (i.e., between-participant) covariates. Level 1 (within-participant, alter-specific) predictors were whether the survivor disclosed the assault to each alter (0 = no, 1 = yes), and if so, whether the alter was unhelpful (0 = no, 1 = yes).
Third, perceived global functional support, perceived assault-specific functional support, and structural support were examined as predictors of mental health problems among sexual assault survivors. Because posttraumatic stress, anhedonic depression, and anxious arousal were expected to be strongly correlated, a latent variable was created to represent mental health problems. Because all other measures were on a 1–5 scale, a mean score of posttraumatic stress (possible range 1–5) was also computed for these analyses to facilitate model estimation. Age, years between networks (i.e., years since assault for survivors), and social support variables were then regressed on the latent variable for mental health problems. Perceived assault-specific functional support across both past and current networks was examined via the following dummy variables: (1) whether the assault was disclosed to any alters, (2) unhelpful response from any alters, and (3) unhelpful response from more than one alter. Post-assault changes in structural support were operationalized as (1) network density increase (amongst those with multiple alters per network), (2) number of alters lost (i.e., individuals not retained in the new network), and (3) number of alters added (i.e., individual alters in the current network not reported in the past network). This model was estimated in the R package, lavaan (Rosseel, 2012), using maximum likelihood estimation and Huber-White standard errors robust to non-normality. Covariances between exogenous variables were estimated to retain all 120 survivors in the latent variable model regardless of item-level missing data. The latent variable was identified using the effects-coding method (Little et al., 2006), such that no single factor loading was constrained, but the average of the loadings was constrained to one. Model fit was evaluated via the comparative fit index (CFI), root mean square error of approximation (RMSEA), and standardized root mean square residual (SRMR). Acceptable fit would be reflected by CFI > .95, RMSEA < .06, and SRMR < .08 (Hu & Bentler, 1999).
Results
Descriptive Statistics
The sample consisted of survivors, who experienced a recent sexual assault between 6 and 59 months ago (n = 120; 22.1%), and non-survivors, who had not experienced a sexual assault since age 14 (n = 424; 77.9%). Survivors’ most meaningful sexual assault experience was most commonly perpetrated by a man (98.3%) and the perpetrator was either a romantic partner (25.8%), acquaintance (20.8%), friend (20.0%), or date (16.7%), with the remaining reporting the perpetrator was a stranger (13.3%), relative (1.7%), or another relationship (1.7%). Half reported they were either intoxicated (48.3%) or unsure if they were intoxicated (3.3%) at the time of the assault. In addition, 15.8% were physically injured and 1.7% reported a weapon was present during the incident.
Participants reported between 1 and the maximum possible of 10 alters (i.e., people to whom they spoke about important matters) in their past networks (Mdn = 5) and in their current networks (Mdn = 6). Over two-thirds of alters were women (past: 69.8%, current: 71.4%). Most alters were friends (past: 59.9%, current: 58.7%), relatives (past: 29.7%, current: 30.0%), or an intimate partner (i.e., spouse, romantic partner, or date: past: 7.5%, current: 7.8%). Participants communicated with most alters at least daily (past: 67.1%, current: 48.9%) or weekly (past: 25.2%, current: 38.1%).
Descriptive statistics (see Table 1) indicated that current perceived global functional support was associated with larger past and current networks (rs ≥ .14, ps < .001), but also disclosing to fewer network members (rs ≤ −.19, ps ≤ .041). Network density of past and current networks was strongly correlated (r = .46, p < .001) as was the size of past and current networks (r = .70, p < .001). Network retention was higher among individuals with denser past and current networks (rs ≥ .17, ps < .001) and lower for those with smaller past and current networks (rs ≤ −.13, ps ≤ .005). Mental health variables including posttraumatic stress, anxious arousal, and anhedonic depression were all strongly correlated (rs ≥ .53, ps < .001). At the bivariate level, each mental health variable was associated with lower perceived global functional support (rs ≤ −.19, ps < .001), more unhelpful alters (i.e., lower perceived assault-specific functional support) in past and current networks (rs ≥ .21, ps ≤ .026), and lower current network density (rs ≤ −.09, ps ≤ .035).
Table 1.
Descriptive Statistics and Correlations
| Variable | M (SD) | Correlations | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | 12 | 13 | 14 | ||
| 1. Age | 19.36 (1.22) | ||||||||||||||
| 2. Years between networks | 2.05 (1.21) | .02 | |||||||||||||
| 3. Perceived global functional support | 5.75 (1.19) | −.03 | .06 | ||||||||||||
| 4. Alters disclosed to in past network+ | 2.11 (2.00) | .00 | .00 | −.20* | |||||||||||
| 5. Alters disclosed to in current network+ | 2.25 (2.16) | .00 | .08 | −.19* | .80*** | ||||||||||
| 6. Alters with perceived unhelpful responses in past network+ | 0.40 (0.82) | .25** | .06 | −.10 | .42*** | .38*** | |||||||||
| 7. Alters with perceived unhelpful responses in current network+ | 0.33 (0.80) | .32*** | .03 | −.02 | .29** | .38*** | .79*** | ||||||||
| 8. Past network density | 0.32 (0.28) | −.11* | .12** | .04 | .06 | −.01 | −.02 | −.05 | |||||||
| 9. Current network density | 0.25 (0.21) | −.05 | .03 | .01 | .12 | .04 | .00 | .02 | .46*** | ||||||
| 10. Past network size | 5.25 (2.74) | −.09* | .03 | .14*** | .56*** | .38*** | .32*** | .17 | −.12** | −.09* | |||||
| 11. Current network size | 6.37 (2.58) | −.09* | .05 | .16*** | .28** | .33*** | .11 | .11 | −.07 | −.09* | .70*** | ||||
| 12. Network retention | 0.69 (0.28) | .05 | −.23*** | −.07 | −.17 | −.04 | −.19 | −.04 | .17*** | .18*** | −.30*** | −.13** | |||
| 13. Posttraumatic stress (sum) | 30.22 (13.83) | .04 | −.01 | −.21*** | .24* | .12 | .43*** | .27** | −.11* | −.13** | .05 | .05 | −.04 | ||
| 14. Anhedonic depression | 2.23 (0.90) | .04 | .05 | −.21*** | .10 | .07 | .34*** | .31*** | −.01 | −.10* | −.03 | .00 | .02 | .59*** | |
| 15. Anxious arousal | 1.52 (0.60) | .00 | −.03 | −.19*** | .17 | .14 | .32*** | .21* | −.01 | −.09* | .07 | .09* | .03 | .60*** | .53*** |
Note. Total N = 544.
Sexual assault disclosures to alters and unhelpful responses from alters were only assessed in the 120 sexual assault survivors.
p < .05.
p < .01.
p < .001.
Differences in perceived global functional support, structural support, and mental health problems were also considered by sexual assault history (see Table 2). Perceived assault-specific support was only relevant to survivors and therefore differences were not assessed by sexual assault history. Results revealed that current perceived global support did not differ by sexual assault history. However, regarding structural support, survivors reported lower past and current network density as well as smaller past networks than those without a sexual assault history. Relative to those without a sexual assault history, survivors reported more severe posttraumatic stress, but there were no differences in depression or anxiety.
Table 2.
Social Support and Mental Health Differences by Sexual Assault History
| Variable | History of Sexual Assault | Test of difference | |
|---|---|---|---|
| No (n = 424) | Yes (n = 120) | ||
| M (SD) | M (SD) | p | |
| Perceived global functional support | 5.79 (1.18) | 5.61 (1.26) | .180 |
| Past network density | 0.34 (0.27) | 0.24 (0.29) | .001** |
| Current network density | 0.26 (0.22) | 0.21 (0.16) | .008** |
| Past network size | 5.50 (2.72) | 4.37 (2.65) | < .001*** |
| Current network size | 6.35 (2.56) | 6.45 (2.63) | .717 |
| Network retention | 0.68 (0.27) | 0.72 (0.29) | .121 |
| Posttraumatic stress (sum) | 29.54 (13.34) | 32.69 (15.32) | .047* |
| Anhedonic depression | 2.21 (0.86) | 2.30 (1.02) | .376 |
| Anxious arousal | 1.50 (0.59) | 1.60 (0.64) | .162 |
Note. Disclosure and perceived assault-specific functional support (i.e., perceptions of unhelpful responding) were only assessed among survivors and therefore are not included here. p values correspond to t-tests.
p < .05.
p < .01.
p < .001.
Most survivors (81.0%) disclosed their assault to at least one alter in their past or current network, disclosing to 3.05 unique alters on average (SD = 2.93). The proportion of alters told in past networks (M = 52.6%, SD = 38.7%) was greater than current networks (M = 37.2%, SD = 32.4%), p < .001. The proportion of survivors who encountered a response perceived to be unhelpful from at least one person was 26.3% for past networks and 19.8% in current networks, with the average number of unhelpful alters being 0.40 (SD = 0.82) and 0.33 (SD = 0.80) in past and current networks, respectively. A paired t-test revealed the proportion of alters who were perceived to be unhelpful in past networks (M = 9.4%, SD = 18.4%) was not significantly different than in current networks (M = 6.3%, SD = 15.4%), p = .054. However, the total number of unhelpful individuals was low. When considering unique alters across networks, 70.7% of survivors reported no unhelpful alters, 14.7% reported one, 12.1% reported two, and 2.6% reported three or more unhelpful alters.
Changes in Structural Support by Sexual Assault History
Network Density
Density (i.e., network interconnectedness) could range between 0 and 1. Density was zero (i.e., reflecting no connections between alters) in past networks for 17.8% of participants and zero in current networks for 11.0% of participants. Density was one (i.e., indicating the presence of connections between all alters) in past networks for 8.0% of participants and in current networks for 2.6% of participants. Thus, following Fang and Ma’s (2013) unconstrained three-part model for proportions with non-ignorable zeroes and ones, density was modeled using three multilevel sub-models: (a) a logistic regression predicting whether the density was 0, (b) a logistic regression model predicting whether the density was 1 for values above 0, and (c) a beta regression model with a logit link predicting density values between 0 and 1.
Model results (see Table 3) revealed that the likelihood of a zero-density network was lower for current than past networks, with this difference being greater for survivors than non-survivors. The likelihood of a density of one was lower for current than past networks, with no difference by sexual assault history. This suggests that reporting of more nuanced network connections (a density other than zero or one) was more likely for current than past networks. Within these nuanced networks, density amount was lower among survivors than those without a sexual assault history, and although density decreased between past and current networks, this change did not differ as a function of sexual assault history.
Table 3.
Prediction of Structural Social Support Variables Over Time by Sexual Assault History
| Network Density | Network Size | Network Retention | ||||
|---|---|---|---|---|---|---|
| Density of Zero | Density of One | Density Amount | Number of Alters | All Alters Retained | Proportion Retained | |
| Predictor | OR (95% CI) | OR (95% CI) | OR (95% CI) | IRR (95% CI) | OR (95% CI) | OR (95% CI) |
| Current age | 1.36 (0.81 – 2.30) | 0.96 (0.28 – 3.27) | 0.99 (0.93 – 1.04) | 0.97* (0.94 – 1.00) | 1.11 (0.94 – 1.30) | 1.01 (0.94 – 1.08) |
| Years between networks | 0.86 (0.49 – 1.53) | 1.34 (0.40 – 4.45) | 0.98 (0.93 – 1.04) | 1.01 (0.98 – 1.04) | 0.81* (0.68 – 0.97) | 0.83*** (0.77 – 0.89) |
| Sexual assault (vs. none) | 4.20 (0.92 – 19.11) | 2.20 (0.06 – 78.58) | 0.70** (0.56 – 0.88) | 0.80*** (0.70 – 0.90) | 1.43 (0.88 – 2.31) | 0.79* (0.62 – 0.99) |
| Time (past network = 0, current network =1) | 0.27** (0.11 – 0.70) | <0.01*** (<0.01 – <0.01) | 0.74*** (0.67 – 0.81) | 1.16*** (1.09 – 1.23) | -- | -- |
| Sexual assault × Time | 0.01*** (<0.01 – 0.05) | 0.02 (<0.01 – 88.84) | 1.15 (0.91 – 1.45) | 1.31*** (1.15 – 1.50) | -- | -- |
| Model Details | ||||||
| N | 522 | 486 | 472 | 525 | 467 | 317 |
| R2 | 0.022 | 0.036 | 0.079 | 0.129 | 0.027 | 0.073 |
Note. OR = odds ratio, CI = confidence interval, IRR = incidence rate ratio,
p < .05.
p < .01.
p < .001.
Network Size
Network size (i.e., the number of alters identified) in past and current networks could range from 1 to 10, and therefore had a zero-truncated count distribution. A truncated negative binomial distribution was tested, but the dispersion parameter was so small that it resulted in problems with model convergence. Thus, a truncated Poisson distribution was used.
Model results (see Table 3) revealed a significant main effect of age, such that for each year older, the network size was 3% smaller. When controlling for age and years between networks, there was a significant interaction between sexual assault history and time in predicting network size. Sexual assault survivors had 20% fewer alters in past networks than non-survivors but evidenced a greater increase over time. Compared to a 16% increase in network size from past to current networks among those without a sexual assault history, sexual assault survivors had a 52% increase. Model-predicted number of alters at each timepoint after controlling for age and time between networks is shown in Figure 1.
Figure 1.
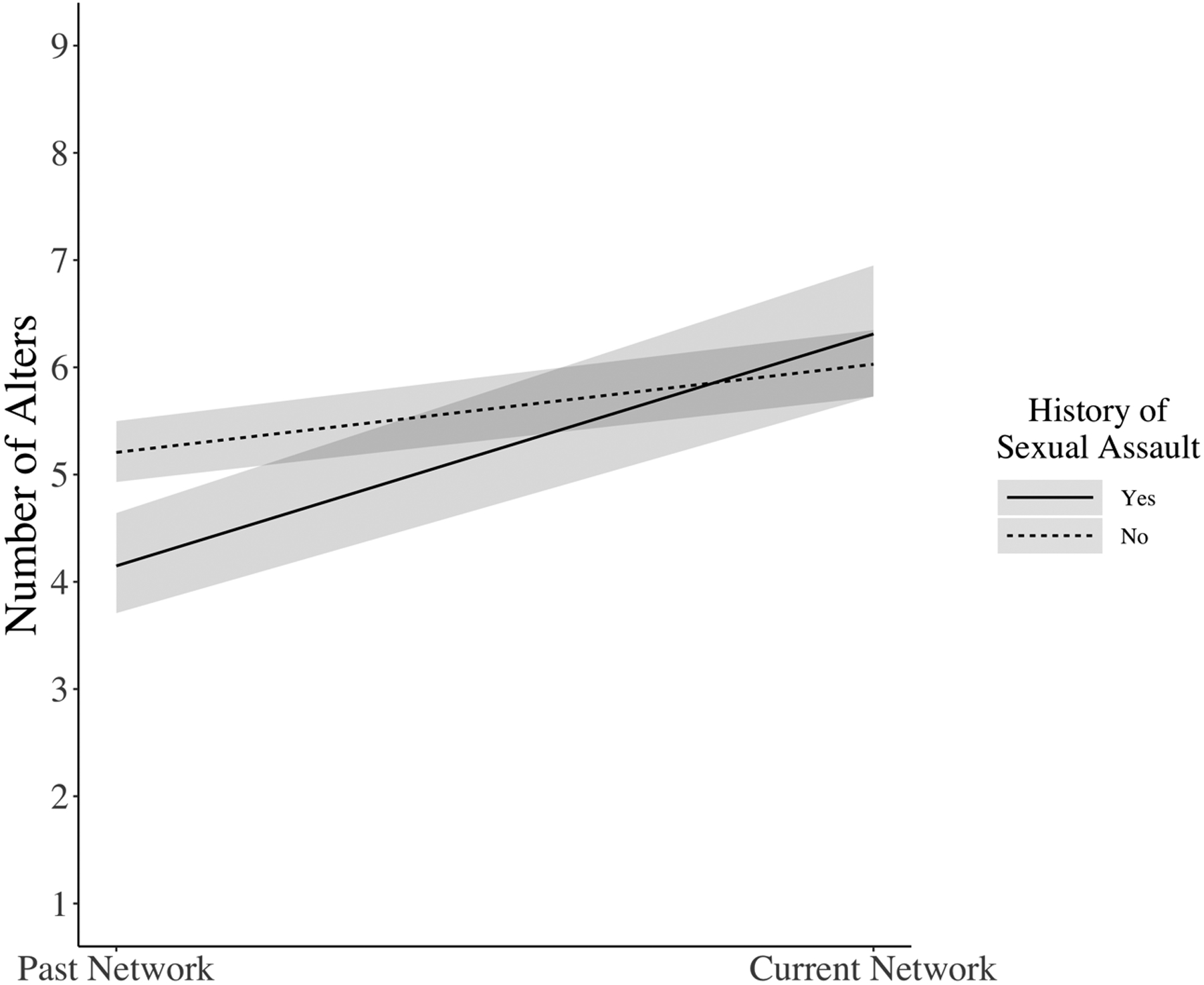
Model-Predicted Network Size by Sexual Assault History
Note. Shaded regions represent 95% confidence intervals.
Network Retention
The proportion of alters retained from past networks was above 0% for all participants and 100% for 32.0% of participants. Thus, the percent of alters retained was modeled with two sub-models: (a) a logistic regression predicting whether all alters were retained from the past network, and (b) a beta regression model with a logit link (via betareg in R; Cribari-Neto & Zeileis, 2010) predicting proportion of alters retained amongst those who did not retain 100%.
Model results (see Table 3) revealed significant main effects for years between networks, such that the likelihood of all alters being retained and the proportion retained were both lower with more years between the networks assessed. After controlling for age and years between networks, there was no association between sexual assault and likelihood of all alters being retained. However, among participants who retained less than 100% of alters in their social network, survivors retained a significantly lower proportion of alters than non-survivors.
Perceived Assault-Specific Functional Support and Changes in Structural Support
Within survivors, multilevel modeling was used to examine perceived assault-specific functional support as a predictor of individual network members being retained (see Table 4). As indicated by the intraclass correlation coefficient, 32% of the variability in whether alters were retained was due to differences between participants; the remaining 68% of variability was due to differences in alters. After controlling for age and time since assault (i.e., years between networks), simply telling the alter about the assault was not associated with network retention, but perceiving an unhelpful response from the alter was associated with a lower probability that the alter was retained in the current network.
Table 4.
Prediction of Changes in Structural Social Support Among Sexual Assault Survivors
| Alter from Past Network Retained to Current Network | |||
|---|---|---|---|
| Predictor | OR | 95% CI | p |
| Current age | 1.33 | 1.01 – 1.76 | .044* |
| Years between networks | 0.59 | 0.44 – 0.80 | .001** |
| Disclosed sexual assault to alter | 1.33 | 0.78 – 2.27 | .296 |
| Perceived unhelpful response from alter | 0.39 | 0.16 – 0.93 | .034* |
Note. Of 120 survivors, six were excluded from this model due to incomplete data on perceived assault-specific functional support and one was excluded due to missing data on age. Thus, n = 113 participants for this model, who reported on n = 491 alters in total. ICC = .32. R2 = .087. OR = odds ratio, CI = confidence interval, ICC = intraclass correlation,
p < .05.
p < .01.
Prediction of Mental Health Problems in Survivors
A latent construct of mental health problems (as indicated by posttraumatic stress, depression, and anxiety) was regressed on variables representing perceived global functional support, perceived assault-specific functional support, and changes in structural support (see Table 5). Model fit was acceptable, CFI = 0.976; RMSEA = 0.058, 90% CI: 0.000 – 0.107; SRMR = 0.031. Perceived global functional support was not uniquely associated with mental health problems (B = −0.11, SE = 0.06, p = .069). Regarding perceived assault-specific functional support, disclosing the assault to at least one alter was not associated with mental health problems (B = −0.11, SE = 0.15, p = .463), but perceiving unhelpful responses from any alter was associated with more mental health problems (B = 0.42, SE = 0.19, p = .029); perceiving unhelpful responses from two or more alters was not associated with mental health problems above and beyond the other predictors (B = 0.18, SE = 0.27, p = .498). Regarding structural support changes, losing more individuals from the past network was associated with more severe current mental health problems (B = 0.13, SE = 0.04, p = .002). However, other aspects of structural support changes, including adding new alters to the network (B = −0.03, SE = 0.03, p = .298) and changes in density, were not uniquely associated with mental health problems (B = 0.00, SE = 0.21, p = .999). As indicated by R2, the predictors collectively accounted for 33.1% of the variability in mental health problems.
Table 5.
Prediction of Mental Health Problems among Sexual Assault Survivors (n = 120)
| B | SE | p | |
|---|---|---|---|
| Mental Health Factor Loadings | |||
| Posttraumatic stress (mean) | 1.11 | 0.08 | < .001*** |
| Anhedonic depression | 1.13 | 0.08 | < .001*** |
| Anxious arousal | 0.75 | 0.07 | < .001*** |
| Predictors of Mental Health | |||
| Age | 0.03 | 0.05 | .543 |
| Years between networks | 0.01 | 0.07 | .917 |
| Perceived global functional social support | −0.11 | 0.06 | .069 |
| Perceived assault-specific functional social support: | |||
| Disclosed assault to any alters | −0.11 | 0.15 | .463 |
| Perceived unhelpful response from any alters | 0.42 | 0.19 | .029* |
| Perceived unhelpful response from multiple alters | 0.18 | 0.27 | .498 |
| Structural social support: | |||
| Density change | 0.00 | 0.21 | .999 |
| Alters lost from network | 0.13 | 0.04 | .002** |
| Alters added to network | −0.03 | 0.03 | .298 |
Note. Unstandardized estimates are shown for all factor loadings and regression slopes. A mean score for posttraumatic stress was employed to facilitate model estimation. SE = standard error. Model n = 120.
p < .05.
p < .01.
p < .001.
Discussion
Building on prior research revealing the importance of social context for trauma recovery (e.g., Bryant, 2016), we investigated three domains of social support in connection with sexual assault recovery: perceived global availability of functional support, perceptions of functional support received in response to disclosure of the assault, and structural support in the form of social network characteristics. The current study represents the first known investigation of social network changes following sexual assault. Extending qualitative research (Ahrens & Aldana, 2012), this study also quantified the association between disclosure and disruption of relationships following sexual assault. In addition, we investigated which domains of social support were uniquely associated with current mental health problems among sexual assault survivors. Findings are discussed below in the context of the cross-sectional design involving retrospective assessment of past and current social networks.
Changes in Structural Support
To date, few studies have reported on structural support among those who have experienced sexual assault (Dworkin et al., 2016; Um et al., 2021). The current study adds to this small but growing literature by investigating the structural characteristics of women’s social networks and whether changes in network density, size, and retention were associated with the experience of sexual assault. Across the sample, women reported having around five or six individuals to whom they spoke about important matters in their past and current networks, many of whom were female friends or relatives. Overall, findings revealed differences in structural support following sexual assault, but not in the anticipated directions. We hypothesized that, relative to those without a sexual assault history, survivors’ networks would become less dense and smaller over time, and we presumed that the two groups would have similar social networks prior to the assault. Contrary to these expectations, social networks were less dense and smaller among sexual assault survivors prior to the assault relative to non-survivors’ networks at a similar time in the past. The fact that survivors retrospectively reported sparse social networks prior to the assault may indicate that individuals who are not well-integrated into interconnected social networks may be at greater risk for sexual assault (Perez-Trujillo et al., 2019). Qualitative work examining college women’s sexual assault risk in social contexts points to the importance of friends in mitigating risk (Blayney et al., 2021). As discussed in focus groups, friends share a sense of trust and responsibility for each other’s safety. To reduce risk, friends use a variety of protective strategies with each other, including keeping tabs on friends and using signals to convey potential danger (Blayney et al., 2021). Being less integrated in a social network may mean that the added protection offered by friends is less available, thus making women more vulnerable targets in social contexts.
An alternative possibility is that social networks may be more sparsely recalled when assessed in connection to a sexual assault, which would align with findings that current networks were similarly sized in survivors and non-survivors. Given the retrospective reporting of structural support, having survivors focus on the sexual assault may have evoked negative memories and led survivors to recall smaller, sparser, or less supportive social networks than recall of the same time period without the assault as a referent point. Trauma exposure can also impair autobiographical memory (Barry et al., 2018). Thus, findings should be replicated with non-trauma referent periods for past social networks, or in prospective studies.
Despite differences in past networks, survivors appeared to build up their social networks after the assault, resulting in similar density and size of current networks to those of non-survivors. Interestingly, compared to women without a sexual assault history, survivors had 20% fewer alters in the past network but retrospectively reported a 52% increase in network size over time. Thus, in contrast to expectations and prior research suggesting challenges during trauma recovery can degrade social relationships over time, we found that survivors in the current study appeared to experience growth in social support after assault, which may reflect resilience. That is, survivors may have made active choices about their social relationships (e.g., which friends to reach out to, which friends to cut ties with) in ways that best supported their recovery. Future prospective research is needed to examine this possibility and investigate factors such as optimism and gratitude (Kumar et al., 2021) that may promote resilient coping among survivors.
Finally, we examined network retention over time. After controlling for age and years between networks, there was no association between sexual assault and likelihood of all alters being retained. Although 32% of participants reported that all alters were exactly the same between networks, social networks often change quickly in young adulthood (Wrzus et al., 2013). Thus, we focus our interpretation on results for participants who reported some variability in the composition of their social networks. Amongst women reporting some changes, experiencing a sexual assault was associated with losing specific individuals from their social network. That is, although the overall number of social network members increased after the assault, survivors experienced more restructuring of their networks, whereby they stopped discussing important matters with the people with whom they had done so prior to the assault, and they identified new people to discuss important matters with to replace and further grow the network. In contrast to one longitudinal study, which found that maltreated and comparison adolescents’ social network size changed similarly across 3 years (Negriff et al., 2015), current findings suggest that the stigmatized interpersonal trauma of sexual assault may have specific effects that disrupt young adults’ relationships. Given that most perpetrators are known by survivors prior to an assault (Smith et al., 2017), survivors might have been motivated to leave their existing social networks following sexual assault to avoid the perpetrator as well as to develop new and more supportive relationships within the changing social network. It is also possible that survivors expected their friends to be a source of protection (Blayney et al., 2021), and after the assault, had difficulty trusting pre-existing friends (DeLoveh & Catteneo, 2017), although more research is needed to examine these possibilities.
Perceived Assault-Specific Functional Support and Structural Support
To further understand why survivors may encounter a restructuring of their social network after a sexual assault, we examined perceived assault-specific support as a predictor of network retention. Although we expected that disclosing the assault to a particular network member would reflect or solidify a strong relationship that would persist over time, no such association was found between disclosure and network retention. Similar to prior work focused on outcomes of disclosure (Dworkin et al., 2019), perceptions of a person’s responses to the disclosure, rather than simply the act of telling that person about the assault, were predictive of the likelihood of retaining that person in a network. That is, if the survivor retrospectively reported discussing important matters with a person prior to the assault and told them about the assault after it happened, but that person responded to the disclosure in a manner the survivor perceived as unhelpful, the survivor was less likely to report recently discussing important matters with this person. More research is needed to clarify whether receiving responses generally considered to be negative (e.g., victim blame) is related to loss of relationships, or whether the survivor needs to perceive negative responses as unhelpful for this to occur. There is qualitative evidence that survivors who are able to reframe negative responses in a positive light are able to maintain relationships with the disclosure recipients that offered these responses (Ahrens & Aldana, 2012). It is also unclear whether perceiving an unhelpful response to disclosure signals that a network member will distance themselves from the survivor, or if the survivor distances themselves from individuals perceived to be unhelpful. Nonetheless, the current quantitative findings add to prior qualitative work (Ahrens & Aldana, 2012) in documenting associations between social changes and unhelpful responses to disclosure, suggesting the need to train peers in supportive responding (Edwards et al., 2022).
Functional and Structural Support Predicting Mental Health
Functional support has been consistently identified as a correlate of post-trauma mental health (Brewin et al., 2000; Dworkin et al., 2019; Ozer et al., 2003), and the conservation of resources theory suggests that loss of social resources following trauma can be detrimental to mental health (Hobfoll & Lilly, 1993). We thus evaluated perceived global functional support, perceived assault-specific functional support, and changes in structural support as predictors of current mental health problems. Although perceived global functional support was related to observed mental health severity scores within the full sample, among sexual assault survivors, there was no association between perceived global support and the latent construct of mental health problems. This is inconsistent with past work supporting an association between perceptions of functional support and mental health in sexual assault survivors (Littleton, 2010), and may reflect that the mental health symptoms assessed in the current study were not specific to the assault. Current findings suggest that assessment of survivors’ core social network might be particularly valuable, as perceived assault-specific functional support from social network members and structural support changes in one’s network were more strongly associated with current mental health than general perceived global support assessed without regard to one’s social network.
Regarding perceived assault-specific functional support, there was no association between disclosure and mental health of survivors, but perceiving an unhelpful response from at least one person was associated with worse current mental health. This finding adds to past work on associations between mental health and perceptions of responses to disclosure (Dworkin et al., 2019). Whereas responses to disclosure and perceptions of responses are typically measured broadly across all responses received from any disclosure recipient, current findings add specificity and nuance to this work. Specifically, our findings reveal that a response to disclosure that is perceived to be unhelpful from even one person in a survivor’s network was associated with mental health problems. Surprisingly, perceiving that more than one person responded to disclosures in an unhelpful manner was not associated with additional mental health problems among survivors. It is possible that perceiving an initial unhelpful response to disclosure from one person contributes to distress because it violates the survivors’ expectations of support (Dworkin et al., 2019); this initial experience may then change survivors’ expectations as they proceed with additional disclosures, such that further unhelpfully-perceived responses no longer violate expectations and therefore do not add to survivors’ distress. Although further research and replication is needed, findings hint at the potential importance of arming survivors with realistic expectations of potential responses to disclosures.
Beyond functional support, some structural support changes were linked to survivors’ mental health. Specifically, survivors who lost more individuals from their past social network reported more severe mental health problems. Taken together, findings suggest that unhelpful responses to sexual assault disclosures may be associated with challenges in recovery. In particular, when the response is so detrimental it disrupts the relationship and leads to the removal of the person from the social network, this reshuffling of the social network might be associated with worsened mental health problems. This is consistent with the premise of conservation of resources theory, which posits that the loss of social resources can be detrimental to mental health (Hobfoll & Lilly, 1993). Consistent with this theory’s prediction that survivors work to gain new resources following stressful life events, survivors may be resilient in rebuilding their social network. However, adding new people to the network was not protective against mental health problems. It is possible that mental health outcomes may depend on the support provided by each new alter. The addition of new people might also be more associated with post-traumatic growth, rather than reduction in mental health problems per se; these possibilities should be tested in future research. Also contrary to expectations, changes in network density were not uniquely associated with mental health outcomes, suggesting that other aspects of social support—unhelpful responses to disclosure and losing relationships—might have been more important predictors of survivors’ mental health.
Limitations and Future Directions
Although this study built on prior research by examining sexual assault survivors’ social networks changes in size, density, and retention, this study also has limitations. First, there were limits to our measures. To minimize participant burden, disclosure and perceived helpfulness of responses to disclosure for each alter were assessed with a single, combined item that was developed for this study. A more nuanced measure of perceived assault-specific support (e.g., that permitted participants to characterize responses from a given person as both helpful and unhelpful) might have revealed different patterns of relationships. We also did not measure received assault-specific support, and more work is needed to understand the social network implications of behaviorally-defined positive and negative responses to disclosures. Our measurement of PTSD symptoms was also limited in that these symptoms were not assessed in reference to sexual assault or a particular index trauma. Thus, the PCL may reflect general distress in this study rather than PTSD per se, although this limitation is somewhat mitigated by our conceptualization of PTSD symptoms as an indicator of overall mental health problems. Additionally, the study only assessed current (not past) mental health. Thus, changes in mental health between time periods remain unclear and mental health problems may have preceded change in social networks. That is, although we hypothesized that sexual assault-related changes in networks may contribute to mental health outcomes, consistent with the social causation model (Wagner et al., 2016), the social selection model also suggests sexual assault-related PTSD symptoms may deteriorate social networks over time (Kaniasty & Norris, 1993; Wagner et al., 2016). This possibility was not assessed. Similarly, we did not assess changes in perceived functional support, and therefore cannot determine if changes in perceived support might contribute to mental health outcomes.
Second, there are limitations to the conclusions that can be reached based on our research design and sample. Although a retrospective design was indicated given the early stage of social network research in relation to sexual assault, our retrospective assessment of prior networks may have been impacted by recall bias, and prospective research is needed to understand temporal associations. Further, because we did not gather information from participants’ friends, directed social networks evaluating whether relationships were reciprocated could not be examined, nor could associations with friends’ mental health. Additionally, because few men and nonbinary survivors were in the current sample, analyses were limited to women. More research with larger samples should examine gender differences in social network changes following sexual assault. Different patterns of change based on gender of the support provider and relationship type also warrant further investigation. Finally, past research suggests differences by symptom type (e.g., depression vs. PTSD) in associations between functional and structural support on partner violence survivors’ mental health (Levendosky et al., 2004) and symptom differences in “emotional contagion” effects after a natural disaster (Ben-Ezra, 2017; Bryant et al., 2017), but these possibilities were not tested in this study. Thus, we encourage longitudinal research exploring symptom-specific emotional contagion effects after sexual assault, including how the emotional experiences of survivors and supporters interact.
Practice Implications
Although more research is needed, the initial connection between structural support changes (especially relationship losses) and mental health suggests the potential utility of social network interventions to support survivors’ recovery. Social network interventions have been indicated in survivors of partner violence (Goodman & Smyth, 2011) and could be extended to intervention efforts for sexual assault survivors. Such interventions could teach survivors ways to maximize support and to build coping skills that might buffer against unhelpful responses to disclosure. Current findings also highlight the potential utility of interventions designed to teach those in survivors’ social networks how to respond to sexual assault disclosures in ways that provide maximum support (Edwards et al., 2022). Pending future work that clarifies the sequence of negative responses to disclosure, perceptions of those responses, relationship loss, and mental health problems, interventions designed to repair important relationships disrupted by a negative disclosure encounter may be indicated to avoid structural social support changes that could exacerbate survivors’ distress. Given the importance of perceptions of social support on post-assault mental health in the current study, empirically supported cognitive therapies (e.g., Resick et al., 2017) may be applied to help survivors navigate social relationships disrupted by a sexual assault.
Conclusion
This study adds to emerging research on trauma-related social network changes to highlight considerations for sexual assault survivors. Among college women who retrospectively reported on their social networks in the past and currently, sexual assault was associated with more restructuring of social networks, as indicated by changing the people with whom they were willing to discuss important matters. When a survivor disclosed their assault to a previously trusted individual and were met with a response perceived to be unhelpful, it appears that the survivor was less likely to continue discussing important matters with that individual. This relationship loss was associated with worse mental health problems for survivors, even when accounting for the unhelpful response. The current approach demonstrates the utility of examining connections between functional and structural support and paves the way for additional research examining how social network structures shape the contexts and interactions in which survivors’ recovery takes place and how those structures change as a result. Thus, findings suggest the need for more research on relationship changes following sexual assault, the implications of shifting social networks on trauma recovery, and the potential utility of social network intervention for survivors.
Acknowledgments
Manuscript preparation was funded by grants from the National Institute of Alcohol Abuse and Alcoholism: K08AA028546 (PI: Jaffe), K99AA028777 (PI: Blayney), and R00AA026317 (PI: Dworkin). The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institute on Alcohol Abuse and Alcoholism.
References
- Ahrens CE, & Aldana E (2012). The ties that bind: Understanding the impact of sexual assault disclosure on survivors’ relationships with friends, family, and partners. Journal of Trauma & Dissociation, 13(2), 226–243. 10.1080/15299732.2012.642738 [DOI] [PubMed] [Google Scholar]
- Barry TJ, Lenaert B, Hermans D, Raes F, & Griffith JW (2018). Meta-analysis of the association between autobiographical memory specificity and exposure to trauma. Journal of Traumatic Stress, 31(1), 35–46. 10.1002/jts.22263 [DOI] [PubMed] [Google Scholar]
- Bearman PS & Moody J (2004). Suicide and friendships among American adolescents. American Journal of Public Health, 94(1), 89–95. 10.2105/ajph.94.1.89 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ben-Ezra M (2017). No man is an island: Another worthwhile approach to the study of mental disorders using social network analysis. American Journal of Psychiatry, 174(3), 202–204. 10.1176/appi.ajp.2016.16121378 [DOI] [PubMed] [Google Scholar]
- Blanchard EB, Jones-Alexander J, Buckley TC, & Forneris CA (1996). Psychometric properties of the PTSD Checklist (PCL). Behavioral Research & Therapy, 34(8), 669–673. 10.1016/0005-7967(96)00033-2 [DOI] [PubMed] [Google Scholar]
- Blayney JA, Jenzer T, Read JP, Livingston J, Testa M, & Carroll Q (2021). A qualitative study on friends and the social context of sexual victimization: Implications for campus-based interventions. Violence Against Women, 27(11), 2092–2110. 10.1177/1077801220954277 [DOI] [PubMed] [Google Scholar]
- Bredemeier K, Spielberg JM, Silton RL, Berenbaum H, Heller W, & Miller GA (2010). Screening for depressive disorders using the Mood and Anxiety Symptoms Questionnaire Anhedonic Depression Scale: A receiver-operating characteristic analysis. Psychological Assessment, 22(3), 702–710. 10.1037/a0019915 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Brewin CR, Andrews B, & Valentine JD (2000). Meta-analysis of risk factors for posttraumatic stress disorder in trauma-exposed adults. Journal of Consulting and Clinical Psychology, 68(5), 748–766. 10.1037/0022-006X.68.5.748 [DOI] [PubMed] [Google Scholar]
- Brooks ME, Kristensen K, van Benthem KJ, Magnusson A, Berg CW, Nielsen A, Skaug HJ, Machler M, & Bolker BM (2017). glmmTMB balances speed and flexibility among packages for zero-inflated generalized linear mixed modeling. The R Journal, 9(2), 378–400. 10.32614/RJ-2017-066 [DOI] [Google Scholar]
- Bruwer B, Emsley R, Kidd M, Lochner C, & Seedat S (2008). Psychometric properties of the Multidimensional Scale of Perceived Social Support in youth. Comprehensive Psychiatry, 49(2), 195–201. 10.1016/j.comppsych.2007.09.002 [DOI] [PubMed] [Google Scholar]
- Bryant RA (2016). Social attachments and traumatic stress. European Journal of Psychotraumatology, 7(1), 29065. 10.3402/ejpt.v7.29065 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bryant RA, Gallagher CH, Gibbs L, Pattison P, MacDougall C, Harms L, Block K, Baker E, Sinnott V, Ireton G, Richardson J, Forbes D, & Lusher D (2017). Mental health and social networks after disaster. The American Journal of Psychiatry, 17(3), 277–285. 10.1176/appi.ajp.2016.15111403 [DOI] [PubMed] [Google Scholar]
- Burrage RL, Gagnon M, & Graham-Bermann SA (2021). Trauma history and social support among American Indian/Alaska Native and non-native survivors of intimate partner violence. Journal of Interpersonal Violence, 36(5–6), NP3326–NP3345. 10.1177/0886260518772103 [DOI] [PubMed] [Google Scholar]
- Burt RS (1984). Network items and the General Social Survey. Social Networks, 6, 293–339. 10.1016/0378-8733(84)90007-8 [DOI] [Google Scholar]
- Chan CS, Lowe SR, Weber E, & Rhodes JE (2015). The contribution of pre- and postdisaster social support to short- and long-term mental health after Hurricanes Katrina: A longitudinal study of low-income survivors. Social Science & Medicine, 138, 38–43. 10.1016/j.socscimed.2015.05.037 [DOI] [PubMed] [Google Scholar]
- Clark LA, & Watson D (1991). Tripartite model of anxiety and depression: Psychometric evidence and taxonomic implications. Journal of Abnormal Psychology, 100(3), 316–336. 10.1037/0021-843X.100.3.316 [DOI] [PubMed] [Google Scholar]
- Coohey C (2007). The relationship between mothers’ social networks and severe domestic violence: A test of the social isolation hypothesis. Violence and Victims, 22(4), 503–512. 10.1891/088667007781554008 [DOI] [PubMed] [Google Scholar]
- Cribari-Neto F & Zeileis A (2010). Beta regression in R. Journal of Statistical Software, 34(2), 1–24. 10.18637/jss.v034.i02 [DOI] [Google Scholar]
- Davis KC, Gilmore AK, Stappenbeck CA, Balsan MJ, George WH, & Norris J (2014). How to score the Sexual Experiences Survey? A comparison of nine methods. Psychology of Violence, 4(4), 445–461. 10.1037/a0037494 [DOI] [PMC free article] [PubMed] [Google Scholar]
- DeLoveh HL, & Cattaneo LB (2017). Deciding where to turn: A qualitative investigation of college students’ helpseeking decisions after sexual assault. American Journal of Community Psychology, 59(1–2), 65–79. 10.1002/ajcp.12125 [DOI] [PubMed] [Google Scholar]
- Dworkin ER, & Allen NE (2017). For the good of the group? Balancing individual and collective risks and benefits in community psychology research. American Journal of Community Psychology, 60(3–4), 391–397. 10.1002/ajcp.12184 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Dworkin ER, Brill CD, & Ullman SE (2019). Social reactions to disclosure of interpersonal violence and psychopathology: A systematic review and meta-analysis. Clinical Psychology Review, 72, 101750. 10.1016/j.cpr.2019.101750 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Dworkin ER, Menon SV, Bystrynski J, & Allen NE (2017). Sexual assault victimization and psychopathology: A review and meta-analysis. Clinical Psychology Review, 56, 65–81. 10.1016/j.cpr.2017.06.002 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Dworkin ER, Newton E, & Allen NE (2018). Seeing roses in the thorn bush: Sexual assault survivors’ perceptions of social reactions. Psychology of Violence, 8(1), 100–109. 10.1037/vio0000082 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Dworkin ER, Pittenger SL, & Allen NE (2016). Disclosing sexual assault within social networks: A mixed‐method investigation. American Journal of Community Psychology, 57(1–2), 216–228. 10.1002/ajcp.12033 [DOI] [PubMed] [Google Scholar]
- Dworkin ER, & Weaver TL (2021). The impact of sociocultural contexts on mental health following sexual violence: A conceptual model. Psychology of Violence, 11(5), 476–487. 10.1037/vio0000350 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Edwards KM, Waterman EA, Ullman SE, Rodriguez LM, Dardis CM, & Dworkin ER (2022). A pilot evaluation of an intervention to improve social reactions to sexual and partner violence disclosures. Journal of Interpersonal Violence, 37(5–6), 2510–2534. 10.1177/0886260520934437 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Fang K, & Ma S (2013). Three-part model for fractional response variables with application to Chinese household health insurance coverage. Journal of Applied Statistics, 40(5), 925–940. 10.1080/02664763.2012.758246 [DOI] [Google Scholar]
- Fedina L, Holmes JL, & Backes BL (2018). Campus sexual assault: A systematic review of prevalence research from 2000 to 2015. Trauma, Violence, & Abuse, 19(1), 76–93. 10.1177/1524838016631129 [DOI] [PubMed] [Google Scholar]
- Goodman LA, & Smyth KF (2011). A call for a social network-oriented approach to services for survivors of intimate partner violence. Psychology of Violence, 1(2), 79–92. 10.1037/a0022977 [DOI] [Google Scholar]
- Guay S, Billette V, & Marchand A (2006). Exploring the links between posttraumatic stress disorder and social support: Processes and potential research avenues. Journal of Traumatic Stress, 19(3), 327–338. 10.1002/jts.20124 [DOI] [PubMed] [Google Scholar]
- Hequembourg AL, Blayney JA, Livingston JA, Bostwick W, & Auerbach S (2021). A mixed methods investigation of sexual victimisation and coping among sexual minority compared to heterosexual women. Psychology & Sexuality, 12(1–2), 17–36. 10.1080/19419899.2019.1678193 [DOI] [Google Scholar]
- Hobfoll SE, & Lilly RS (1993). Resource conservation as a strategy for community psychology. Journal of Community Psychology, 21(2), 128–148. [DOI] [Google Scholar]
- Holt-Lunstad J, Robles TF, & Sbarra DA (2017). Advancing social connection as a public health priority in the United States. American Psychologist, 72(6), 517–530. 10.1037/amp0000103 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hu LT, & Bentler PM (1999). Cutoff criteria for fit indexes in covariance structure analysis: Conventional criteria versus new alternatives. Structural Equation Modeling: A Multidisciplinary Journal, 6(1), 1–55. 10.1080/10705519909540118 [DOI] [Google Scholar]
- Johnson S, Murphy MJ, & Gidycz CA (2017). Reliability and validity of the sexual experiences surveys – short forms victimization and perpetration. Violence and Victims, 32(1), 78–92. 10.1891/0886-6708.VV-D-15-00110 [DOI] [PubMed] [Google Scholar]
- Joseph S, Williams R, & Yule W (1997). Understanding posttraumatic stress: A psychosocial perspective on PTSD and treatment. Wiley. [Google Scholar]
- Kaniasty K, & Norris FH (1993). A test of the social support deterioration model in the context of natural disaster. Journal of Personality and Social Psychology, 64(3), 395–408. 10.1037/0022-3514.64.3.395 [DOI] [PubMed] [Google Scholar]
- Kao JC, Chuong A, Reddy MK, Gobin RL, Zlotnick C, & Johnson JE (2014). Associations between past trauma, current social support, and loneliness in incarcerated populations. Health & Justice, 2, 7. 10.1186/2194-7899-2-7 [DOI] [Google Scholar]
- Katerndahl D, Burge S, Ferrer R, Becho J, & Wood R (2013). Differences in social network structure and support among women in violent relationships. Journal of Interpersonal Violence, 28(9), 1948–1964. 10.1177/0886260512469103 [DOI] [PubMed] [Google Scholar]
- Koss MP, Abbey A, Campbell R, Cook S; Norris J, Testa C, Ullman S, West C, & White J (2007). Revising the SES: A collaborative process to improve assessment of sexual aggression and victimization. Psychology of Women Quarterly, 31(4), 357–370. 10.1111/j.1471-6402.2007.00385.x [DOI] [Google Scholar]
- Krenz T, Krivitsky PN, Vacca R, Bojanowski M, & Herz A (2021). egor: Import and analyse ego-centered network data. R package version 1.21.6. https://CRAN.R-project.org/package=egor
- Kumar SA, Jaffe AE, Brock RL, & DiLillo D (2022). Resilience to suicidal ideation among college sexual assault survivors: The protective role of optimism and gratitude in the context of posttraumatic stress. Psychological Trauma: Theory, Research, Practice, and Policy, 14(S1), S91–S100. 10.1037/tra0001141 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lee B, & Youm Y (2011). Social network effects on post-traumatic stress disorder (PTSD) in female North Korean immigrants. Journal of Preventive Medicine and Public Health, 44(5), 191–200. 10.3961/jpmph.2011.44.5.191 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Levendosky AA, Bogat GA, Theran SA, Trotter JS, Eye AV, & Davidson WS (2004). The social networks of women experiencing domestic violence. American Journal of Community Psychology, 34(1–2), 95–109. 10.1023/B:AJCP.0000040149.58847.10 [DOI] [PubMed] [Google Scholar]
- Little TD, Slegers DW, & Card NA (2006). A non-arbitrary method of identifying and scaling latent variables in SEM and MACS models. Structural Equation Modeling, 13(1), 59–72. 10.1207/s15328007sem1301_3 [DOI] [Google Scholar]
- Littleton HL (2010). The impact of social support and negative disclosure reactions on sexual assault victims: A cross-sectional and longitudinal investigation. Journal of Trauma & Dissociation, 11(2), 210–227. 10.1080/15299730903502946 [DOI] [PubMed] [Google Scholar]
- Littleton HL, Axsom D, & Grills-Taquechel AE (2009). Adjustment following the mass shooting at Virginia Tech: The roles of resource loss and gain. Psychological Trauma: Theory, Research, Practice, and Policy, 1(3), 206–209. 10.1037/a0017468 [DOI] [Google Scholar]
- Lowe SR, Chan CS, & Rhodes JE (2010). Pre-hurricane perceived social support protects against psychological distress: A longitudinal analysis of low-income mothers. Journal of Consulting and Clinical Psychology, 78(4), 551–560. 10.1037/a0018317 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Marin A & Hampton KN (2007). Simplifying the personal network name generator. Field Methods, 19(2), 163–193. 10.1177/1525822X06298588 [DOI] [Google Scholar]
- Negriff S, James A, & Trickett PK (2015). Characteristics of the social support networks of maltreated youth: Exploring the effects of maltreatment experience and foster placement. Social Development, 24(3), 483–500. 10.1111/sode.12102 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Nolet A-M, Morselli C, & Cousineau M-M (2021). The social network of victims of domestic violence: A network-based intervention model to improve relational autonomy. Violence Against Women, 27(10), 1630–1654. 10.1177/1077801220947169 [DOI] [PubMed] [Google Scholar]
- Olson EA, Pizzagalli DA, & Rosso IM (2021). Social anhedonia is associated with low social network diversity in trauma‐exposed adults. Journal of Traumatic Stress, 34(1), 241–247. 10.1002/jts.22577 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ozer EJ, Best SR, Lipsey TL, & Weiss DS (2003). Predictors of posttraumatic stress disorder and symptoms in adults: A meta-analysis. Psychological Bulletin, 129(1), 52–71. 10.1037/0033-2909.129.1.52 [DOI] [PubMed] [Google Scholar]
- Perez-Trujillo M, Jaramillo-Sierra AL, & Quintane E (2019). Connectedness as a protective factor of sexual victimization among university students. Victims & Offenders, 14(7), 895–919. 10.1080/15564886.2019.1655121 [DOI] [Google Scholar]
- Plat J., Keye KM., & Koene KC. (2014). Size of the social network versus quality of social support: Which is more protective against PTSD? Social Psychiatry and Psychiatric Epidemiology, 49(8), 1279–1286. 10.1007/s00127-013-0798-4 [DOI] [PMC free article] [PubMed] [Google Scholar]
- R Core Team (2020). R: A language and environment for statistical computing. R Foundation for Statistical Computing [Computer software]. https://www.R-project.org/ [Google Scholar]
- Resick PA, Monson CM, & Chard KM (2017). Cognitive processing therapy for PTSD: A comprehensive manual. Guilford Publications. [Google Scholar]
- Rosseel Y (2012). lavaan: An R package for structural equation modeling. Journal of Statistical Software, 48(2), 1–36. http://www.jstatsoft.org/v48/i02/ [Google Scholar]
- Ruggiero KJ, Smith DW, Hanson RF, Resnick H, Saunders BE, Kilpatrick DG, & Best CL (2004). Is disclosure of childhood rape associated with mental health outcome? Results from the National Women’s Study. Child Maltreatment, 9(1), 62–77. 10.1177/1077559503260309 [DOI] [PubMed] [Google Scholar]
- Smith SG, Chen J, Basile KC, Gilbert LK, Merrick MT, Patel N, Walling M, & Jain A (2017). The National Intimate Partner and Sexual Violence Survey (NISVS): 2010–2012 state report. National Center for Injury Prevention and Control, Centers for Disease Control and Prevention. [Google Scholar]
- Ullman SE (1999). Social support and recovery from sexual assault: A review. Aggression and Violent Behavior: A Review Journal, 4, 343–358. 10.1016/S1359-1789(98)00006-8 [DOI] [Google Scholar]
- Ullman SE (2010). Why, how often, and to whom do women disclose, and what factors influence whether disclosure is healing? In Ullman SE, Talking about sexual assault: Society’s response to survivors (pp. 41–57). American Psychological Association. [Google Scholar]
- Ullman SE, Townsend SM, Filipas HH, & Starzynski LL (2007). Structural models of the relations of assault severity, social support, avoidance coping, self-blame, and PTSD among sexual assault survivors. Psychology of Women Quarterly, 31(1), 23–37. 10.1111/j.1471-6402.2007.00328.x [DOI] [Google Scholar]
- Um MY, Lee JO, Kim HJ, Rice E, & Palinkas LA (2021). Testing the pathway from pre-migration sexual violence to suicide-related risk among North Korean refugee women living in South Korea: Do social networks matter? Social Psychiatry and Psychiatric Epidemiology, 56(3), 485–495. 10.1007/s00127-020-01977-8 [DOI] [PubMed] [Google Scholar]
- Wagner AC, Monson CM, & Hart TL (2016). Understanding social factors in the context of trauma: Implications for measurement and intervention. Journal of Aggression, Maltreatment & Trauma, 25(8), 831–853. 10.1080/10926771.2016.1152341 [DOI] [Google Scholar]
- Wang Y, Chung MC, Wang N, Yu X, & Kenardy J (2021). Social support and posttraumatic stress disorder: A meta-analysis of longitudinal studies. Clinical Psychology Review, 85, 101998. 10.1016/j.cpr.2021.101998 [DOI] [PubMed] [Google Scholar]
- Wardenaar KJ, van Veen T, Giltay EJ, de Beurs E, Penninx BW, & Zitman FG (2010). Development and validation of a 30-item short adaptation of the Mood and Anxiety Symptoms Questionnaire (MASQ). Psychiatry Research, 179(1), 101–106. 10.1016/j.psychres.2009.03.005 [DOI] [PubMed] [Google Scholar]
- Weathers F, Litz B, Herman D, Huska J, & Keane T (October 1993). The PTSD Checklist (PCL): Reliability, validity, and diagnostic utility. Paper presented at the Annual Convention of the International Society for Traumatic Stress Studies, San Antonio, TX. [Google Scholar]
- Williams R, & Joseph S (1999). Conclusions: An integrative psychosocial model of PTSD. In Yule W (Ed.), Post-traumatic stress disorders: Concepts and therapy (pp. 297–314). Wiley. [Google Scholar]
- Wrzus C, Hänel M, Wagner J, & Neyer FJ (2013). Social network changes and life events across the life span: A meta-analysis. Psychological Bulletin, 139(1), 53–80. 10.1037/a0028601 [DOI] [PubMed] [Google Scholar]
- Zalta AK, Tirone V, Orlowska D, Blais RK, Lofgreen A, Klassen B, Held P, Stevens NR, Adkins E, & Dent AL (2021). Examining moderators of the relationship between social support and self-reported PTSD symptoms: A meta-analysis. Psychological Bulletin, 147(1), 33–54. 10.1037/bul0000316 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Zimet GD, Dahlem NW, Zimet SG & Farley GK (1988). The Multidimensional Scale of Perceived Social Support. Journal of Personality Assessment, 52(1), 30–41. 10.1207/s15327752jpa5201_2 [DOI] [PubMed] [Google Scholar]