

Abstract
Background:
Serious car seat installation errors occur at high rates in infants and children. These errors significantly increase the risk of child injury in a motor vehicle crash, and few interventions have addressed the challenge longitudinally.
Methods:
This was a pilot randomized controlled feasibility trial of virtual car seat safety checks for caregivers of newborns recruited from an urban newborn nursery. The control [enhanced usual care (EUC)] group received an in-person car seat check as a newborn and virtual check at 9-months. The intervention group received two additional virtual checks at 3 and 6 months. Installation and infant positioning errors were documented and corrected by a child passenger safety technician (CPST). We measured feasibility and acceptability by tracking caregiver and CPST challenges, and caregiver retention. Group differences were tested for statistical significance using Chi-Square or Fisher’s Exact for categorical variables, and two sample T-tests for continuous variables.
Results:
33 caregivers were randomized to the EUC and 28 to the intervention group. Virtual checks were feasible, with variable participation levels at each quarter. WiFi and app challenges noted in 30%. There was satisfaction with the virtual car seat checks. At baseline, car seat installation and infant positioning errors occurred at equal frequency, and at 9 months the intervention group had a significantly lower mean proportion than the EUC group in all categories of errors. In summary, virtual seat checks are feasible and the optimal timing of repeat checks requires additional study. A larger study is needed to further evaluate the effect of longitudinal virtual checks on errors.
Keywords: child passenger safety, pediatric injury prevention, car seat misuse, feasibility trial
BACKGROUND
Motor vehicle crashes (MVC) are one of the leading causes of death and morbidity in children and young adults in the United States, and the third leading cause of injury-related deaths in children less than 1 year of age.1,2 Fatalities, hospitalizations, and Emergency Department visits for children in MVCs cost the United States over $11 billion in 2015.3,4 Proper use of the child safety seat (car seat, or CSS) reduces the risk of death by 71% in infants.5 While the rate of CSS use has increased across all age groups over the last few decades, rates of serious CSS installation and infant positioning errors as high as 91% have been reported in the newborn population.6 The reasons for CSS misuse are likely related to the complex design and function of the CSS, the lack of standardized hands-on instruction,6 and adjustments required over time as the child grows.
In addition to the high rates of serious errors in CSS installation and use overall, racial and geographic disparities have been identified surrounding proper CSS use. Nonwhite families have higher rates of misuse and non-use of CSSs than white families7 and death rates of metropolitan African American children are twice that of metropolitan white children. Death rates from an MVC are 10 times higher in rural African American and Hispanic children than in white children.8
One of the primary solutions used to correct the misuse of CSSs is interactive training from certified child passenger safety technicians (CPSTs), who provide families with education on the correct selection, installation, infant/child positioning, and use of their child’s car seat. CPSTs increase caregivers’ skills, knowledge, and confidence,9 and reduce errors in CSS use.10 There are only 33,000 CPSTs nationally for more than 40 million CSS-eligible children,11,12 with uneven geographic availability. In addition, a one-time interaction with a CPST does not lead to sustained correction of CSS errors, with 40% of families demonstrating serious CSS errors 4 months after training.13
To address geographic barriers, create convenience for families, and increase sustainability of the skills gained from each car seat check, one potential solution is regularly scheduled virtual car seat checks. Preliminary research suggests that virtual car seat checks can increase parental self-efficacy. Interacting with a remotely located CPST using visual and audio connections is better than a caregiver solely using a written instruction manual or phone conversation.14,15 While there are studies evaluating the feasibility of virtual car seat checks in isolation, there is no current research evaluating the use of regularly scheduled virtual car seat checks to address CSS selection, installation, and use longitudinally. This pilot randomized controlled feasibility trial tested the hypotheses that providing quarterly interactive virtual car seat checks using a remotely located CPST would be feasible and acceptable for infant caregivers, and would lead to reduction in observed errors from newborn discharge to the 9 month follow-up.
METHODS
We performed a pilot randomized controlled trial evaluating the feasibility and acceptability of quarterly virtual car seat checks in infant caregivers, and explored preliminary efficacy of the intervention. Study participants were recruited from an urban newborn nursery with a diverse patient population, approximately 40% Caucasian, 40% African American, and 50–60% covered with public insurance. Caregivers were approached for enrollment within 48 hours of their child’s birth, between 9am and 5pm on specific weekdays when the research assistant was available. They were excluded if the caregiver did not speak English or Spanish, if they did not have access to a smartphone or tablet, if they did not have regular access to a car, if the mother and infant were to be discharged separately, or if the infant was premature or had other special child passenger safety needs. After informed consent, all participants completed a survey to obtain demographic information and details regarding their previous experience with child safety seats. The research assistant used the randomization feature in REDCap to randomize into one of the two study groups, intervention or enhanced usual care (control). Randomization was stratified so that race and ethnicity were equally represented in each group. Caregivers were offered $10 for each virtual car seat check, and $25 on completion of the 9-month car seat check.
On discharge from the newborn nursery, caregivers in both the intervention and control groups received an in-person car seat check with a CPST at the hospital. After the initial car seat check, the intervention group received virtual car seat checks at 3 and 6 months of age, and both groups received virtual car seat checks at 9 months. Of note, the 9-month car seat check was initially planned to take place in-person but was changed to a virtual check because of the COVID-19 pandemic. At each in-person and virtual car seat check during the study, the parent was asked to install the car seat and position the infant into the CSS. The infant’s position was evaluated, including the use of harness webbing, buckles, retainer clip, and any other positioning devices. The seat installation was checked for location in the vehicle, angle of installation, and proper lower anchor or seatbelt installation. Errors were documented using a modified version of the standard Safe Kids Worldwide checklist, included as in the appendix. If a family was found to have an unsafe seat (e.g. expired or damaged), a new CSS was offered. All errors were noted and shown to the caregiver, and errors were corrected in real time under the supervision and instruction of the CPST. Statistical power was not the goal in this feasibility study, so sample size was set to be inclusive of a wide number of diverse participants.
The virtual car seat checks took place at the location of the caregiver’s choice with the infant present, and required access to Wi-Fi or a data plan for use with their smartphone or tablet. The instruction was provided by one of two CPSTs with experience conducting virtual car seat checks, using specialized real-time audio and video input through the Help Lightning application (Help Lightning, Inc., Birmingham, AL). Help Lightning is a free application that uses a patented technology to merge two real-time videos digitally.16 Using Help Lightning, the parent interacted virtually with the CPST in real-time, allowing for instruction, communication, and knowledge exchange similar to that provided with an in-person interaction.16 At each virtual car seat check the parent was asked if the CSS being used was new or different from the previous CSS evaluated. If so, they were asked to show the car seat label to confirm that the seat was not expired. The parent was asked to place the infant in the CSS first, then the installation and infant positioning were checked using the modified checklist described previously. The CPST then instructed the parent to perform maneuvers on camera to check tightness and positioning of each element of the installation on video, and feedback was provided when errors were noted.
We assessed the feasibility of scheduling and completing virtual car seat checks by keeping a detailed record of attempts to schedule appointments, and any technical or other challenges noted during the actual car seat check. Acceptability was measured by analyzing caregiver satisfaction through a debriefing survey (available in the appendix) sent electronically via text and e-mail to caregivers after the final car seat check. Study data were collected and managed using Research Electronic Data Capture (REDCap) hosted at the local hospital.17 REDCap is a secure, web-based software platform designed to support data capture for research studies.
Data collected during each car seat check included the number and type of CSS errors identified, time required for each car seat check, connectivity or communication issues during the car seat check, and parent satisfaction with the remote car seat check. Certain errors were characterized as serious based on previous literature.6,18–20 Errors that were closely correlated (such as whether the car seat moved more than an inch side to side, and whether it moved more than an inch front to back) were combined as a single error. Because of the differences in number of errors possible depending on installation type (11 possible serious errors with a LATCH installation and 12 in a seat belt installation), mean proportions of errors were calculated and compared across groups. Group differences were tested for statistical significance using Chi-Square or Fisher’s Exact for categorical variables, and two sample T-tests for continuous variables.
Patient and Public Involvement
Patients were involved in the first aim of this research, which is published separately.21 That aim was a qualitative aim in which parents of newborns were interviewed, and given the opportunity to share their thoughts on challenges with car seat installation and infant positioning, and provided input on the intervention described in this publication.
RESULTS
Of the 166 screened parent/infant dyads, 36 (22%) were ineligible, 66 (40%) declined participation, and 64 (39%) provided informed consent. Reasons for refusal were not systematically collected but were recorded in 21 (32%) when parents volunteered their reason for declining. The most frequently documented reason for refusals was lack of interest (42%), followed by an equal number who expressed they were feeling overwhelmed (14%), already knowledgeable in car seat installation (14%), plans to move from the area (14%), and inability to return for subsequent (initially planned) in-person car seat check (14%). Of the 64 parents who consented to participate, 3 were discharged and left before randomization, 33 were randomized to the control group, and 28 were randomized to the intervention group. Figure 1 is a CONSORT diagram showing participant enrollments.
Figure 1:
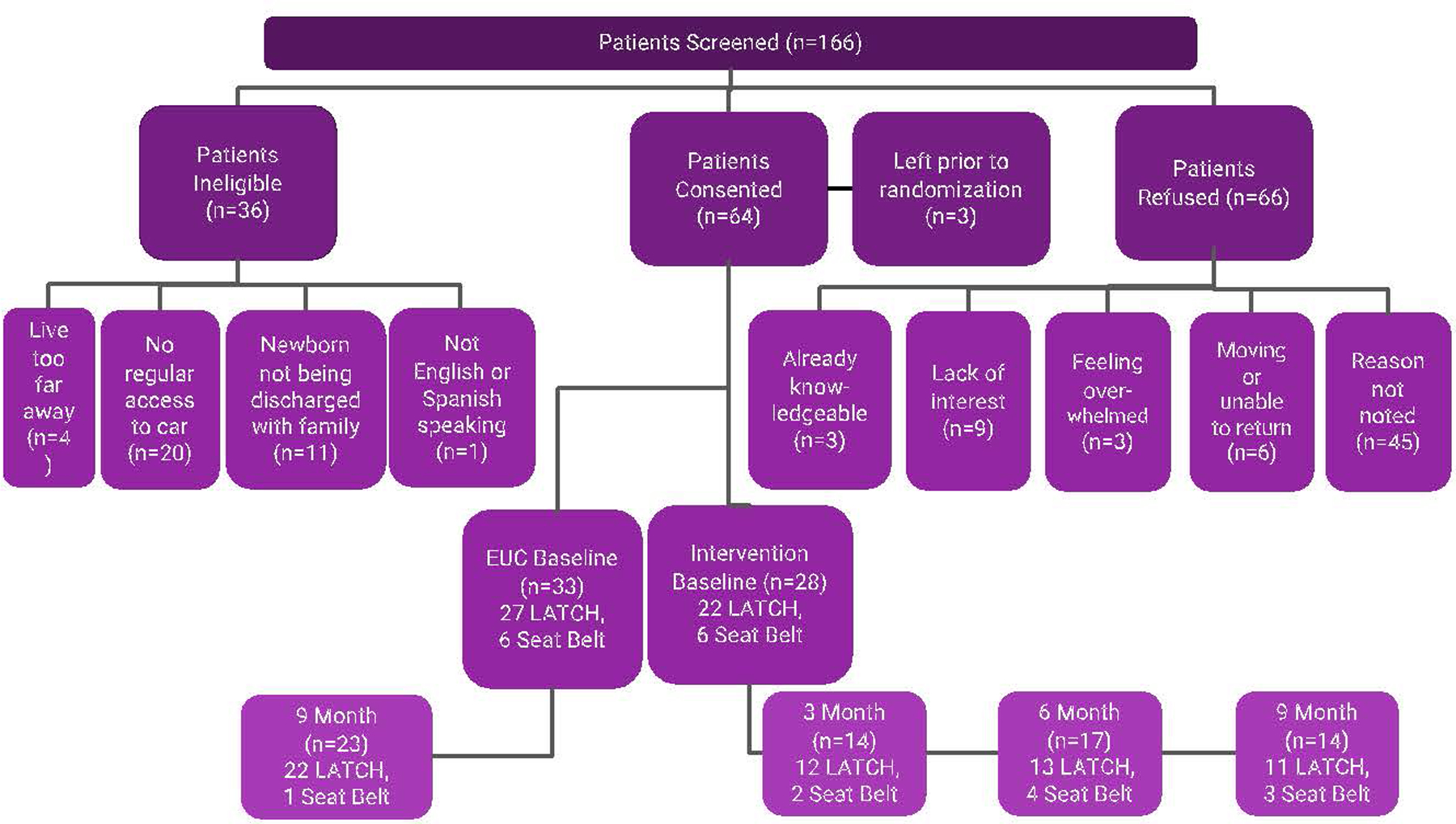
CONSORT Diagram
Demographics of the control and intervention groups are summarized in Table 1 below.
Table 1:
Demographics
| Demographic | EUC | Intervention | p-value |
|---|---|---|---|
| Total Number | 33 | 27 | |
| Median Number of Children | 2 | 2 | |
| Insurance type | N (%) | N (%) | 0.1796 |
| Public | 3 (9.1%) | 7 (25.9%) | |
| Private | 30 (90.9%) | 20 (74.1%) | |
| Caregiver Age | 0.3852 | ||
| 18–24 | 1 (3%) | 5 (18.5%) | |
| 25–29 | 5 (15.2%) | 2 (7.4%) | |
| 30–34 | 12 (36.4%) | 11 (40.7%) | |
| 35–39 | 10 (30.3%) | 5 (18.5%) | |
| 40+ | 5 (15.1%) | 4 (14.8%) | |
| Race | 0.5357 | ||
| Asian | 0 (0%) | 1 (3.7%) | |
| Black/African American | 13 (39.4%) | 10 (37%) | |
| White | 20 (60.6%) | 16 (59.3%) | |
| Education | 0.0928 | ||
| Graduate or Professional | 20 (60.6%) | 14 (51.9%) | |
| College or Associate | 11 (33.3%) | 6 (22.2%) | |
| High School or Below | 2 (6.1%) | 7 (25.9%) | |
| Annual income | 0.5156 | ||
| Not reported | 7 | 3 | |
| <$60,000 | 4 (15.4%) | 6 (25%) | |
| $60–150,000 | 6 (23.1%) | 7 (29.2%) | |
| >$150,000 | 16 (61.5%) | 11 (45.8%) | |
| Marital status | 0.1756 | ||
| Married/Partnered | 28 (84.8%) | 19 (70.4%) | |
| Never married/Single | 5 (15.2%) | 8 (29.6%) | |
| Confidence of car seat installation | 0.0781 | ||
| Very confident | 10 (30.3%) | 12 (44.4%) | |
| Somewhat confident | 22 (66.7%) | 11 (40.7%) | |
| Unsure (or not too confident) | 1 (3%) | 4 (14.8%) | |
| LATCH installation at baseline* | 27 (81.8%) | 22 (81.5%) | |
| Seatbelt installation at baseline* | 6 (18.2%) | 7 (25.9%) | |
| Infant carrier with base | 4 | 4 | |
| Infant carrier without base | 2 | 2 | |
| Other | 0 | 1 |
Numbers do not always add up to 100% because some caregivers asked for instruction on LATCH and seat belt installation.
There were no significant differences between the groups. There were only 9 participants who had less than a college education, and less than a quarter of participants who reported their annual income <$60,000. Both groups included very few caregivers who were not confident in their ability to install their car seat, with 1 (3%) in the EUC group and 4 (14.8%) in the intervention group. All car seats evaluated on discharge from the newborn nursery were infant carriers. Types of errors are summarized in Table 2, and baseline car seat installation and use errors are reported in Table 3. The rate and type of errors (serious errors, installation errors, and errors in infant positioning) all occurred at an equal frequency in both the control and intervention groups at baseline. There were no adverse events reported during the study.
Table 2:
Types of Errors
| Errors | |
|---|---|
| Installation | Incorrect for age, height, weight, or developmental level* |
| More than 1 inch of movement back and forth or side to side* | |
| Installed in front of air bag* | |
| Installed facing incorrect direction* | |
| Incorrect recline angle* | |
| Lower anchors/seat belt attached improperly* | |
| Lower anchor straps/seat belt not threaded through appropriate belt path* | |
| Car seat belt not locked* | |
| Lower anchor straps/seat belt twisted | |
| Incorrect carrying handle position | |
| Car seat too close to seat in front | |
| Harness straps threaded incorrectly behind seat | |
| Harness straps twisted | |
| LATCH and SB used at same time | |
| Been in crash | |
| Expired | |
| Harness traps torn, frayed or damaged | |
| Harness straps secured improperly | |
| Infant Positioning | Loose harness straps* |
| Chest clip not at armit level* | |
| Shoulder harness straps not at or below child’s shoulder height* (for rear facing) | |
| Child’s head not within the confines of the car seat (for rear facing) | |
| Crotch strap not tight/close to child’s body |
Serious Errors
Table 3:
Comparison of mean proportion of errors in control vs intervention group at baseline
| Control (n=33) | Intervention (n=27) | ||||
|---|---|---|---|---|---|
| Mean Proportion of Errors | Standard Deviation | Mean Proportion of Errors | Standard Deviation | p-value | |
| All Errors | 19% | ±8 | 20% | ±9 | 0.807 |
| Serious Errors (11 or 12 possible) | 25% | ±16 | 28% | ±17 | 0.477 |
| Installation | 21% | ±13 | 23% | ±15 | 0.549 |
| Errors (19 or 20 possible) | |||||
| Infant Positioning Errors (5 possible) | 40% | ±20 | 36% | ±22 | 0.514 |
Feasibility and Acceptability
There were 31 virtual seat checks completed over the course of study (n=14 at 3 months and n=17 at 6 months). 19 of 27 (70.4%) families enrolled in the intervention group doing virtual car seat checks at either or both the 3 and 6 month visits. 23 out of the 33 participants (69.6%) who enrolled in the control group and 14 out of 27 (51.9%) of the intervention group completed the 9-month car seat check. Participants were contacted by text message (median 1 attempt, range 1–5), telephone calls (median 2, range 1 to 7), and email (median 1, range 1 to 3). One of the challenges identified by caregivers, as well as CPST’s who participated in the study, was technical difficulties with Wi-Fi connectivity and/or the smartphone app used for the video call, identified in 30.9% of all virtual car seat checks.
At the final (9 month) visit, measures of confidence and acceptability were similar in the intervention and EUC groups. 12 out of 14 (85.7%) of the intervention group and 18 out of 21 (85.7%) of the EUC group had increased confidence in their car seat installation. When asked whether they would participate in a quarterly car seat program outside of the study, 46.2% of the intervention group answered yes (45% in the EUC group) and 38.5% answered maybe in the intervention group (40% in the EUC group).
Error Rates
At 9 months, intervention group participants had a reduced rate of all errors, serious errors, installation errors, and infant positioning errors as displayed in Table 4. All virtual car seat checks were completed by 11 out of 27 (40.7%) of the intervention group. Four participants had transitioned their child to a rear-facing convertible car seat before the 9-month virtual car seat check, including 3 from the control group and 1 from the intervention group. Of the caregivers who had their car seat checks completed at the subsequent time points, mean proportions of total and serious errors decreased substantially from baseline. In particular, the mean proportions of errors for the 11 participants that attended all four appointments (0, 3, 6, and 9 months) in comparison to the participants in the control group trended down, as displayed in Figure 2. The type and number of serious errors identified are displayed in Figure 3. While both groups showed a reduction in serious errors between the baseline car seat check in the newborn period and the final car seat check at 9 months, the intervention group showed a larger reduction in the number of serious errors.
Table 4:
Comparison of mean proportion of errors in control vs intervention group at 9 months
| Control Group (Mean Errors with SD) (n=23) | Intervention Group (Mean Errors with SD) (n=14) | p-value | |
|---|---|---|---|
| All Errors | 7% (±4 | 2% (±3) | <0.001 |
| Serious Errors (11 or 12 possible) | 10% (±8) | 2%6) | 0.003 |
| Installation Error Rate (19 or 20 possible) | 8% (±7) | 2% (±5 | 0.005 |
| Infant Positioning Error Rate (5 possible) | 15% (±17) | 3% (±7) | 0.018 |
Figure 2:
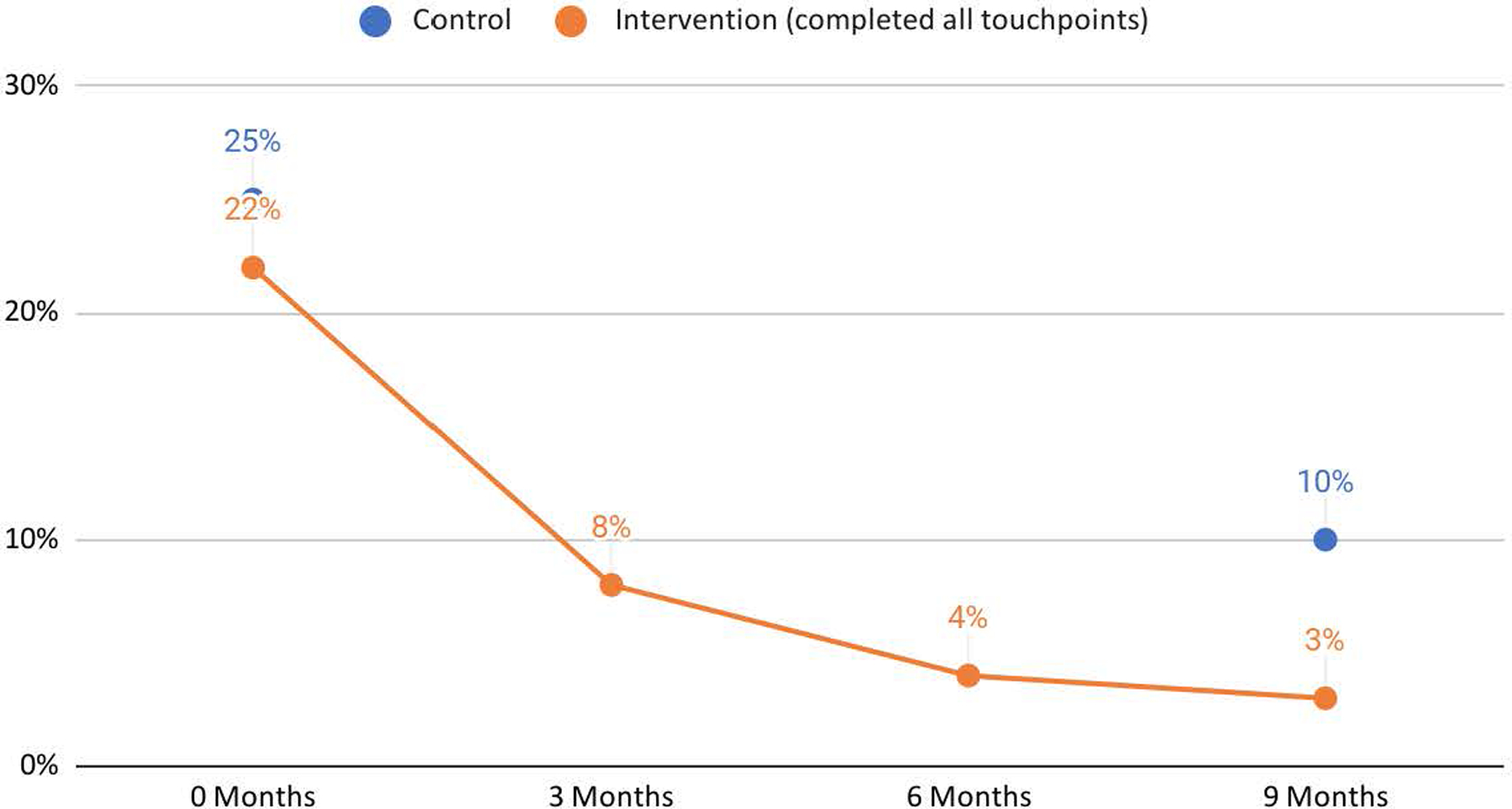
Mean proportion of Serious Errors in Control & Intervention Groups
Figure 3:
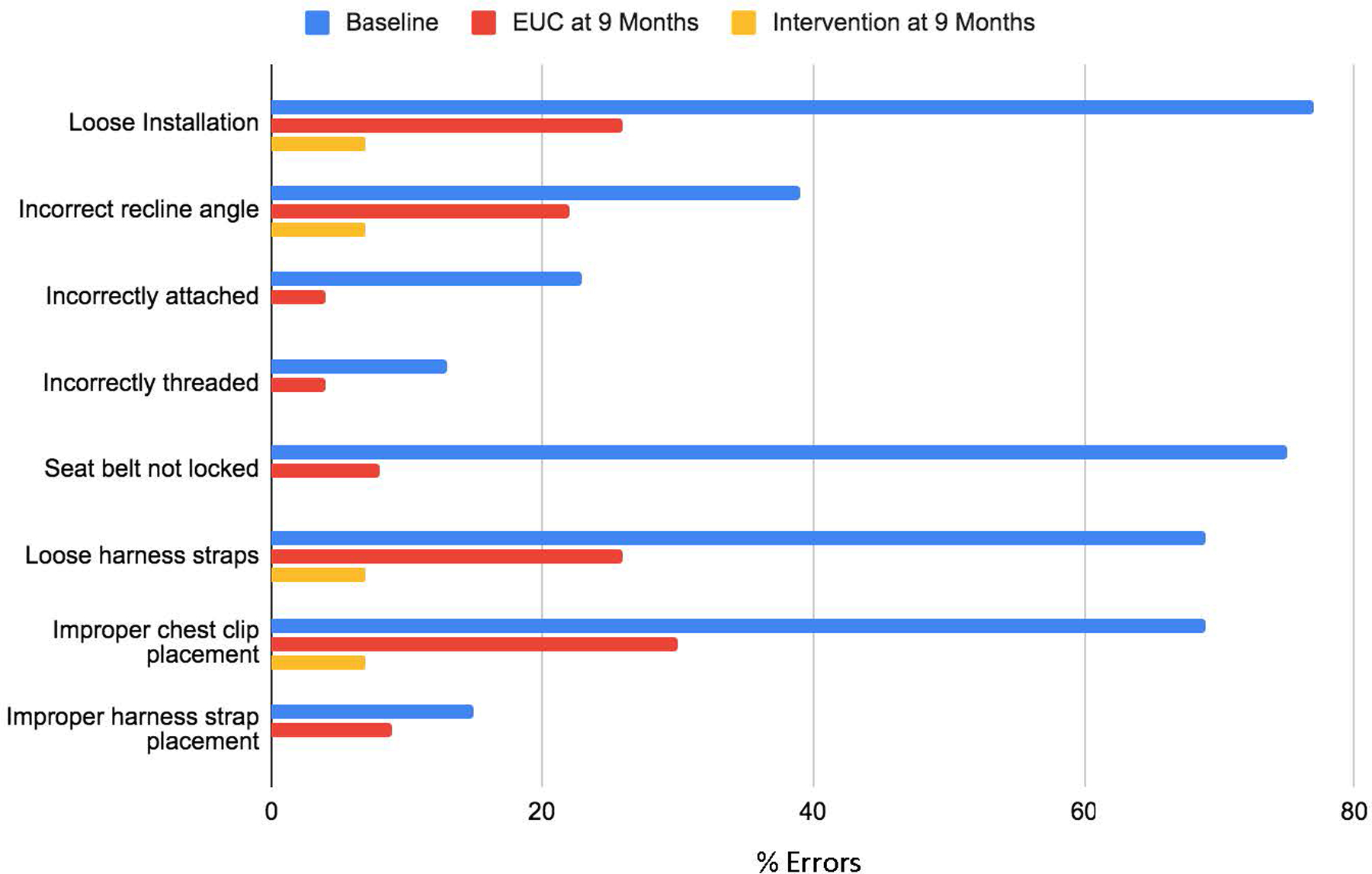
Mean Proportion of Errors at Baseline in Comparison to 9 Months
DISCUSSION
In this study, we found that providing virtual car seat checks using a remotely located CPST is feasible and acceptable, and more study is needed to determine the ideal interval and for longitudinal virtual car seat checks. leading to moderate to high acceptability ratings in the subset of infant caregivers who completed the study. Study participants from both the intervention and control group endorsed improved confidence in their use of car seats over the course of the study, which is similar to previous work on the use of one-time virtual car seat checks.22 Feasibility was demonstrated by the low median number of contact attempts required for scheduling and/or rescheduling, but the range included numbers as high as 7 for some caregivers. In future studies, this may be an opportunity to provide alternatives to scheduled quarterly virtual car seat checks (such as on-demand or same day car seat checks) which may be more convenient and feasible for some families. In addition, given that all car seat checks were completed virtually at the 9 month visit and measures of satisfaction and confidence were similar, future study will be required to better understand whether there is increased caregiver satisfaction with longitudinal scheduled virtual car seat checks.
The challenges in the use of technology needed to complete the virtual car seat checks, including the need for data usage and/or Wi-Fi, and the challenges of mastering the specialized app used to connect the CPST and parent during the study are further discussed in a previous publication.23 These challenges reveal that while virtual car seat checks are feasible in many populations, adaptations to the intervention will be required for populations with less access to high speed wireless internet or robust network data plans. Future studies should evaluate use of adjuncts to address some of these challenges, such as community locations which offer free Wi-Fi, tripods to assist with holding the phone during the installation, and additional lighting.
The high rates of serious errors in car seat installation and infant positioning seen in this study are similar to those identified in previous studies of newborns.6 We saw a decrease in the proportion of serious errors over time in the control group as well as the intervention group. These results support the idea that even a one-time car seat check is beneficial to families in reducing serious car seat installation and infant positioning errors, which has been seen in previous studies.11,24,25 While errors decreased in both groups, the intervention group had significantly fewer errors than the control group at the 9-month check, and this persisted when analyzing the mean proportion of serious errors, installation errors, and infant positioning errors.
Limitations
There were a large number of caregivers who were not eligible for the study due to lack of regular access to a car, which may have skewed the study population towards higher education and socioeconomic status. Future studies will need to include participants who have intermittent access to a car to further evaluate the efficacy of this type of intervention across groups of various socioeconomic, geographic, and racial backgrounds. There was significant attrition in both the intervention and control groups, with 51.9% and 69.6%, respectively, following up at the 9-month car seat check. This is similar to previous work on in-person car seat checks in the primary care setting, in which 50% of the control and 49.5% of the intervention group followed up at 4 months.11
However this project was completed during the COVID-19 pandemic, which may have affected attrition. Further work will seek to adapt the process for improved retention.
Conclusion
In conclusion, we found that virtual car seat checks are feasible and acceptable to parents of infants, and there is a strong preliminary correlation of reduced serious errors over time as a result of longitudinal scheduled virtual car seat checks. Further study is needed to refine and expand on the concept and timing of regularly scheduled virtual car seat checks to reach all families, with an additional focus on adaptation of this approach to address racial and geographic disparities in restraint misuse and mortality from motor vehicle crashes.
Supplementary Material
KEY MESSAGES.
What is already known on this topic:
Car seat installation errors in the newborn period occur in as many as 91% of installations observed.
What this study adds:
Virtual car seat checks are feasible in parents of infants in the first year of life, however more study is required to evaluate optimal timing of longitudinal car seat checks.
How this study might affect research, practice, or policy:
During the pandemic, many public health interventions have adopted virtual modalities. This study provides data which supports further investigation into the effectiveness of longitudinal virtual interventions for child passenger safety.
Acknowledgements
We would like to acknowledge the study team (T. Bobbe Thomas, Ryan Pearman, Alease Young, Julie Farmer, Leslie Brown), expertise of Dr. David Schwebel, and clinical staff at the newborn nursery for their work on this research, our funding source (Award Numbers UL1TR001876 and KL2TR001877 from the NIH NCATS), and the families who participated in the study.
Funding:
This publication was supported by Award Numbers UL1TR001876 and KL2TR001877 from the NIH National Center for Advancing Translational Sciences. These data have not been previously presented.
Footnotes
Competing Interests: There are no known competing interests for any of the authors.
Ethics Approval Statement: This study was approved by the Children’s National Hospital IRB Pro00010892.
ClinicalTrials.gov Identifier: NCT05252299
There are no known conflicts of interests for any of the authors.
Data Availability Statement:
Deidentified patient data and results are available upon request from the corresponding author at sadiqa.kendi@bmc.org..
REFERENCES
- 1.Data NonFatal | WISQARS | Injury Center | CDC [Internet] 2019. [cited 2019 Nov 16]. Available from: https://www.cdc.gov/injury/wisqars/nonfatal.html
- 2.leading_causes_of_death_by_age_group_unintentional_2018_1100w850h.jpg (1100×850) [Internet] [cited 2020 Nov 9]. Available from: https://www.cdc.gov/injury/images/lc-charts/leading_causes_of_death_by_age_group_unintentional_2018_1100w850h.jpg
- 3.WISQARS (Web-based Injury Statistics Query and Reporting System)|Injury Center|CDC [Internet] 2018. [cited 2018 Apr 12]. Available from: https://www.cdc.gov/injury/wisqars/index.html
- 4.Injury Data and Resources - Mortality Data [Internet] [cited 2018 Apr 12]. Available from: https://www.cdc.gov/nchs/injury/injury_mortality.htm
- 5.Durbin DR, Committee on Injury V. Technical Report—Child Passenger Safety. Pediatrics 2011. Mar 21;peds.2011–0215.
- 6.Hoffman BD, Gallardo AR, Carlson KF. Unsafe from the Start: Serious Misuse of Car Safety Seats at Newborn Discharge. J Pediatr 2016. Apr;171:48–54. [DOI] [PubMed] [Google Scholar]
- 7.Macy ML, Cunningham RM, Resnicow K, Freed GL. Disparities in Age-Appropriate Child Passenger Restraint Use Among Children Aged 1 to 12 Years. Pediatrics 2014. Feb 1;133(2):262–71. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Kendi S Child Passenger Safety in Rural and Urban Areas [Unpublished manuscript] 2021;
- 9.Safe Kids Worldwide. Impact of Safe Kids Buckle Up Inspections on Caregiver knowledge, Confidence, and Skill 2017. Aug. (Child Passenger Safety; ). [Google Scholar]
- 10.Duchossois GP, Nance ML, Wiebe DJ. Evaluation of child safety seat checkpoint events. Accid Anal Prev 2008. Nov 1;40(6):1908–12. [DOI] [PubMed] [Google Scholar]
- 11.Fifteen Years of CPS [Internet] [cited 2018 Apr 12]. Available from: http://www.saferidenews.com/srndnn/CPSTsProfessionals/HistoryofChildPassengerSafety/FifteenYearsofCPS/tabid/202/Default.aspx
- 12.Howden L, Meyer J. Age and Sex Composition: 2010 2011. May;(2010 Census Briefs; ):16. [Google Scholar]
- 13.Burstein D, Zonfrillo MR, Baird J, Mello MJ. Child Passenger Safety Technician Consultation in the Pediatric Primary Care Setting. Clin Pediatr (Phila) 2017. Sep;56(10):928–33. [DOI] [PubMed] [Google Scholar]
- 14.Schwebel DC, Tillman MA, Crew M, Muller M, Johnston A. Using interactive virtual presence to support accurate installation of child restraints: Efficacy and parental perceptions. J Safety Res 2017. Sep 1;62(Supplement C):235–43. [DOI] [PubMed] [Google Scholar]
- 15.Schwebel DC, Johnston A, Rouse J. Teaching infant car seat installation via interactive visual presence: An experimental trial. Traffic Inj Prev 2017. Feb 17;18(2):188–92. [DOI] [PubMed] [Google Scholar]
- 16.Be There Instantly | Help Lightning [Internet] [cited 2018 Apr 12]. Available from: https://helplightning.com/
- 17.Harris P, Taylor R, Minor B, Elliott V, Fernandez M, O’neal L, et al. The REDCap consortium: Building an international community of software partners. J Biomed Inform 2019. May 9; [DOI] [PMC free article] [PubMed]
- 18.Manary MA, Flannagan CAC, Reed MP, Orton NR, Klinich KD. Effects of child restraint misuse on dynamic performance. Traffic Injury Prevention Published online October 31, 2019. Accessed November 15, 2019. 10.1080/15389588.2019.1665177 [DOI] [PubMed]
- 19.Whyte T, Kent N, Bilston LE, Brown J. Comparative performance of rearward and forward-facing child restraint systems with common use errors: Effect on crash injury risk for a 1-year-old occupant. Traffic Injury Prevention 2022;23(2):91–96. doi: 10.1080/15389588.2021.2012168 [DOI] [PubMed] [Google Scholar]
- 20.Osborne H Child car seats: the common mistakes with shocking outcomes. The Guardian https://www.theguardian.com/money/2011/oct/15/child-car-seats-common-mistakes-shocking-outcomes. Published October 15, 2011. Accessed August 13, 2022.
- 21.Kendi S, Howard MB, Mohamed MA, Eaddy S, Chamberlain JM. So much nuance: A qualitative analysis of parental perspectives on child passenger safety. Traffic Inj Prev Published online March 4, 2021:1–6. doi: 10.1080/15389588.2021.1877276 [DOI] [PubMed]
- 22.Schwebel DC, Tillman MA, Crew M, Muller M, Johnston A. Using interactive virtual presence to support accurate installation of child restraints: Efficacy and parental perceptions. J Safety Res 2017. Sep 1;62(Supplement C):235–43. [DOI] [PubMed] [Google Scholar]
- 23.Kendi S, Taylor MF, Chamberlain J. Virtual car seat checks during a pandemic. Inj Prevco J Int Soc Child Adolesc Inj Prev 2020. Dec 3; [DOI] [PubMed]
- 24.Schwebel DC, Johnston A, Rouse J. Teaching infant car seat installation via interactive visual presence: An experimental trial. Traffic Inj Prev 2017. Feb 17;18(2):188–92. [DOI] [PubMed] [Google Scholar]
- 25.Quinlan KP, Holden J, Kresnow M. Providing car seat checks with well-child visits at an urban health center: a pilot study. Inj Prev 2007. Oct 1;13(5):352–4. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Data Availability Statement
Deidentified patient data and results are available upon request from the corresponding author at sadiqa.kendi@bmc.org..