

Abstract
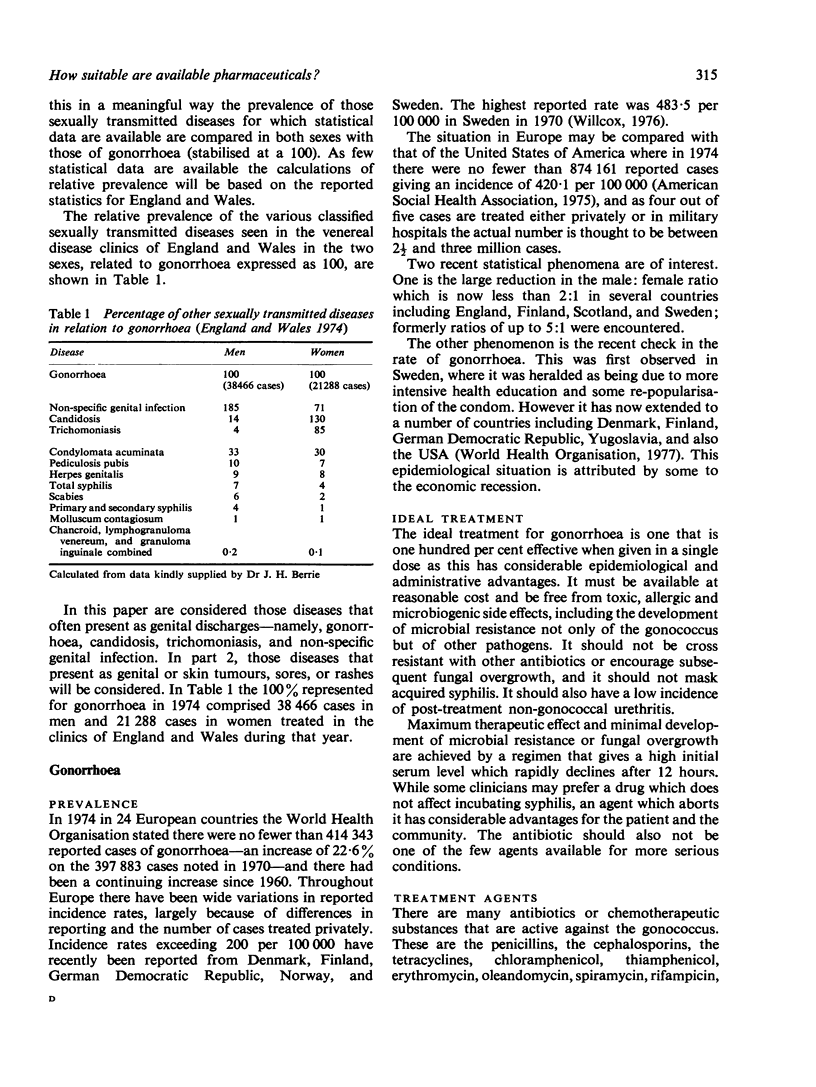
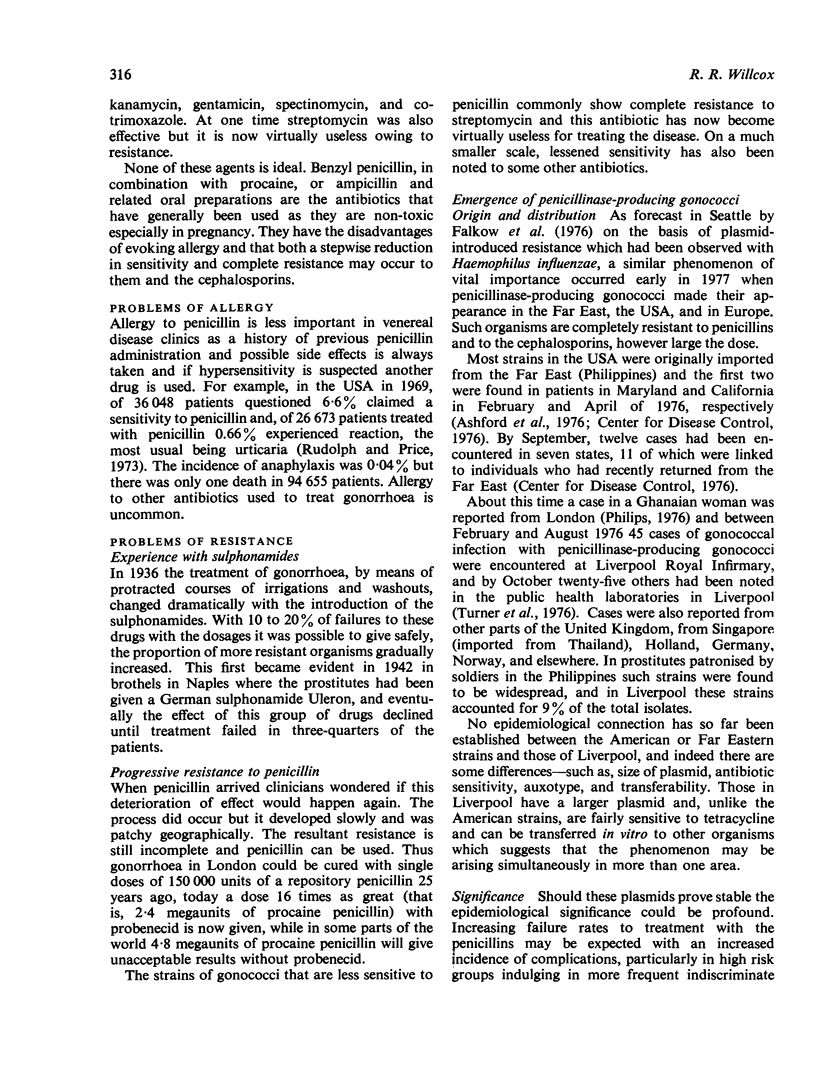
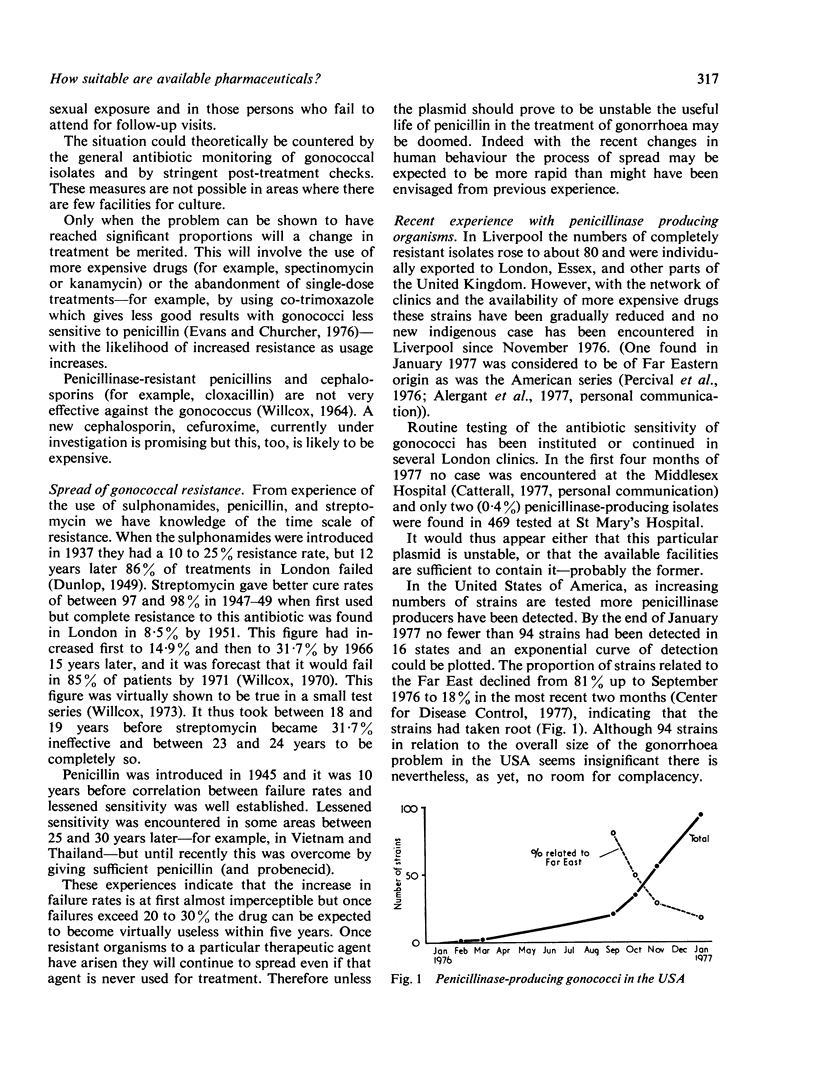
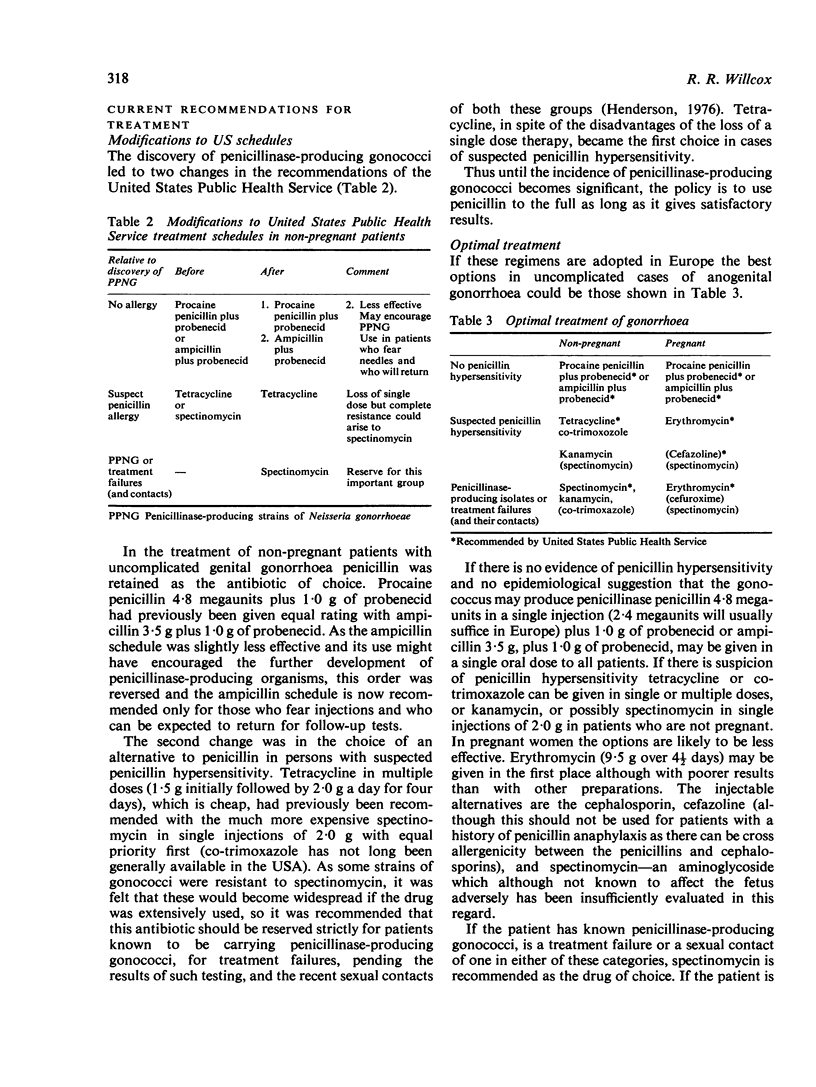
The relative prevalence of sexually transmitted diseases and the agents available for the treatment of these diseases commonly presenting as genital discharges—namely, gonorrhoea, candidosis, trichomoniasis, and non-specific genital infection—are reviewed. The many agents that are active against gonorrhoea are listed, but none is ideal. Penicillin, in spite of its allergic side effects, has remained the drug of choice for 25 years because it is cheap, easily obtained, lacks toxicity even in pregnancy, and is effective. Its use is now threatened by the emergence of some strains that are able to produce penicillinase. At present the policy is to obtain the best results from penicillin while these are acceptable, but the clinician in some countries is badly served by the availability of procaine penicillin in aqueous suspension. There is a need for an effective penicillin or cephalosporin that is penicillinase resistant and cheap. Cefuroxime offers considerable hope but it is likely to be expensive in the immediate future.
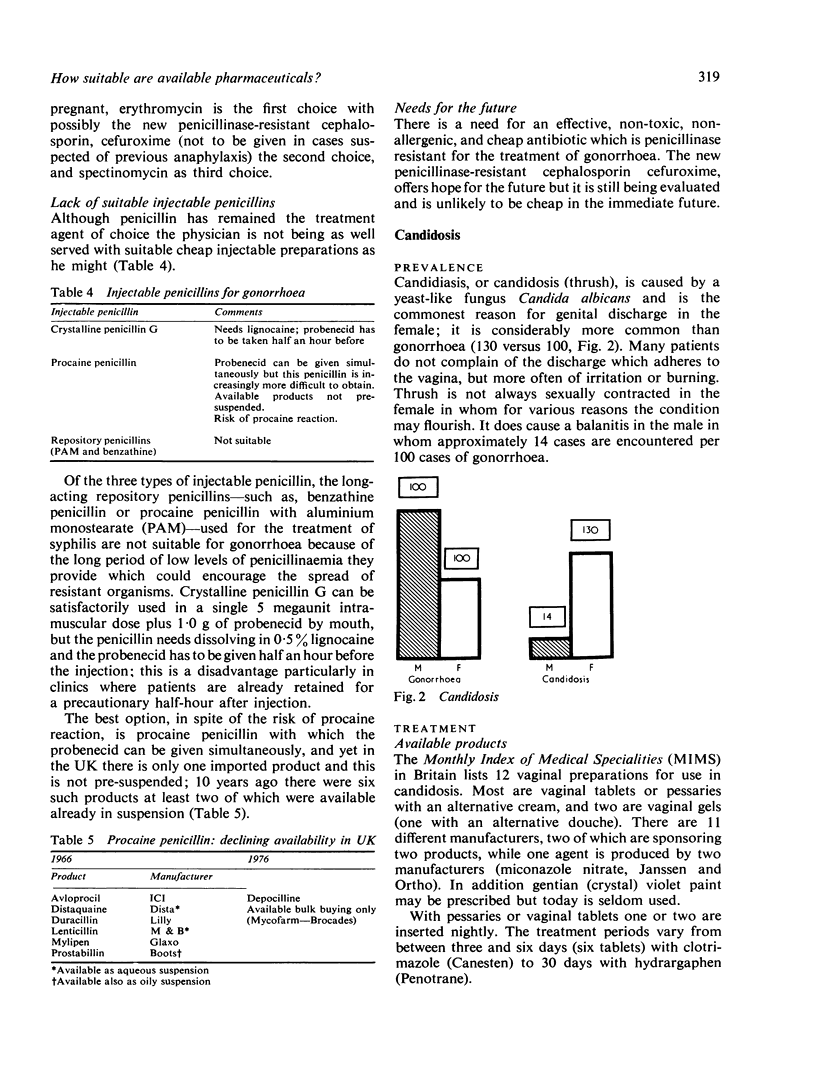
There are many preparations for the local treatment of candidosis. The confidence expressed by the manufacturers in recommending a three-day treatment is, it is hoped, based on a superior product. Nevertheless there is a need for a safe systemically absorbed fungicide which could be used orally, or some substance that could render the vagina an inhospitable environment for the organism.
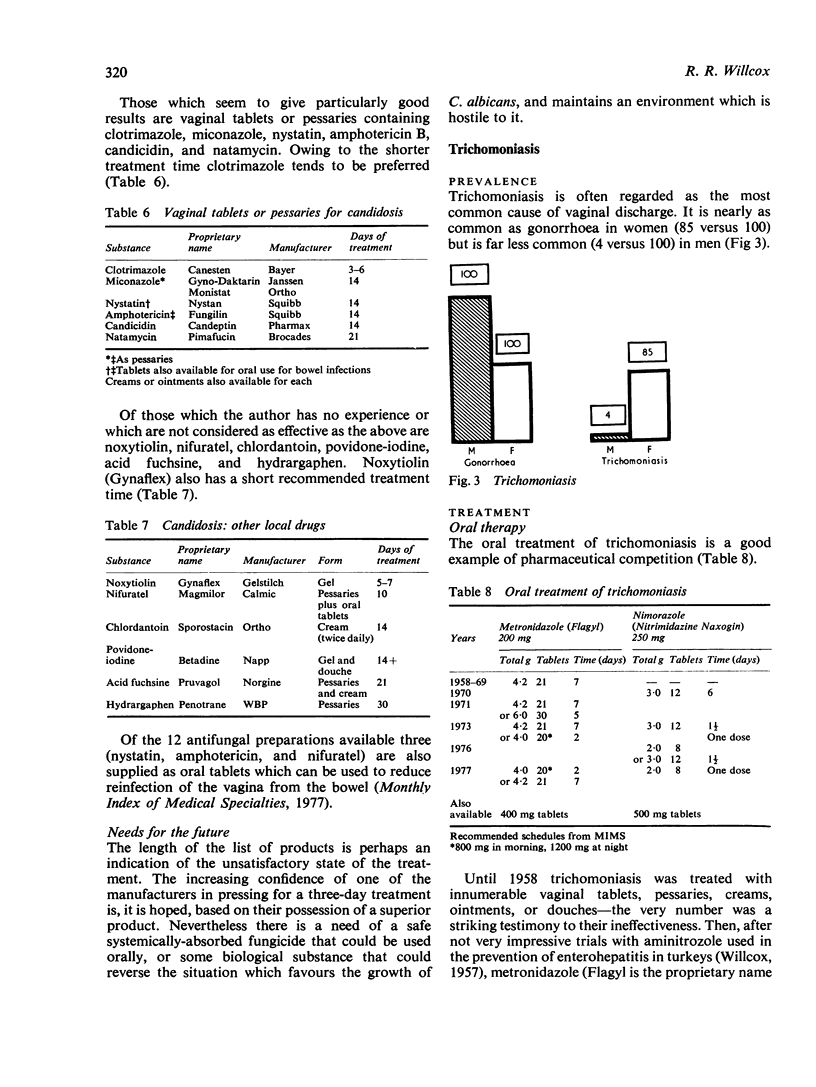
In the treatment of trichomoniasis the pharmaceutical industry in providing substances more than 90% effective in a single dose has done all that can be expected. Any further advances lie in the field of human behaviour rather than pharmaceutical research.
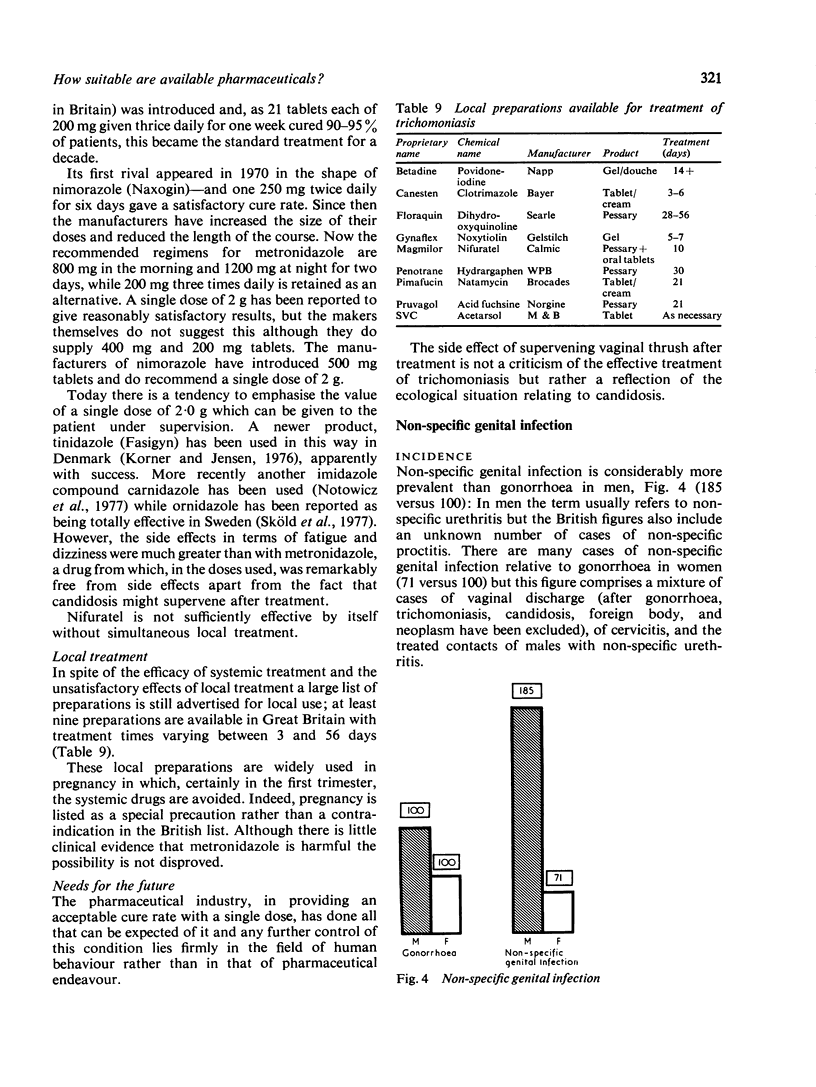
In the treatment of non-specific genital infection the needs are more of research than of therapy. More knowledge is required of the cause of the condition and the relative role of contending pathogens, and of the results of treatment of patients and contacts in which Chlamydia or other suspect pathogens have been isolated.
Full text
PDF

Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Ashford W. A., Golash R. G., Hemming V. G. Penicillinase-producing Neisseria gonorrhoeae. Lancet. 1976 Sep 25;2(7987):657–658. doi: 10.1016/s0140-6736(76)92467-3. [DOI] [PubMed] [Google Scholar]
- Evans A. J., Churcher G. M. Penicillinase-producing gonococci. Lancet. 1976 Oct 16;2(7990):864–864. doi: 10.1016/s0140-6736(76)91266-6. [DOI] [PubMed] [Google Scholar]
- Korner B., Jensen H. K. Sensitivity of Trichomonas vaginalis to metronidazole, tinidazole, and nifuratel in vitro. Br J Vener Dis. 1976 Dec;52(6):404–408. doi: 10.1136/sti.52.6.404. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Notowicz A., Stolz E., de Koning G. A. First experiences with single-dose treatment of vaginal trichomoniasis with carnidazole (R 25831). Br J Vener Dis. 1977 Apr;53(2):129–131. doi: 10.1136/sti.53.2.129. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Penicillinase-producing Neisseria gonorrhoeae. Lancet. 1976 Oct 9;2(7989):793–793. [PubMed] [Google Scholar]
- Rein M. F., Chapel T. A. Trichomoniasis, candidiasis, and the minor venereal diseases. Clin Obstet Gynecol. 1975 Mar;18(1):73–88. doi: 10.1097/00003081-197503000-00008. [DOI] [PubMed] [Google Scholar]
- Rudolph A. H., Price E. V. Penicillin reactions among patients in venereal disease clinics. A national survey. JAMA. 1973 Jan 29;223(5):499–501. [PubMed] [Google Scholar]
- Sköld M., Gnarpe H., Hillström L. Ornidazole: a new antiprotozoal compound for treatment of Trichomonas vaginalis infection. Br J Vener Dis. 1977 Feb;53(1):44–48. doi: 10.1136/sti.53.1.44. [DOI] [PMC free article] [PubMed] [Google Scholar]
- WILLCOX R. R. Treatment of vaginal trichomoniasis with 2-acetylamino-5-nitrothiazole (aminitrozole) given orally. Br J Vener Dis. 1957 Jun;33(2):115–117. doi: 10.1136/sti.33.2.115. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Willcox R. R. 'Triple tetracycline' in the treatment of non-gonococcal urethritis in males. Br J Vener Dis. 1972 Apr;48(2):137–140. doi: 10.1136/sti.48.2.137. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Willcox R. R. A survey of problems in the antibiotic treatment of gonorrhoea. With special reference to South-East Asia. Br J Vener Dis. 1970 Jun;46(3):217–242. doi: 10.1136/sti.46.3.217. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Willcox R. R., Sparrow R. W., Fazluddin C. M. Minocycline in the treatment of non-gonococcal urethritis. Br J Vener Dis. 1975 Jun;51(3):206–209. doi: 10.1136/sti.51.3.206. [DOI] [PMC free article] [PubMed] [Google Scholar]