

Abstract
Background
There is some evidence that more social media use is related to poorer mental well-being and that social media use can become problematic when it starts to interfere with a person’s daily life and mental well-being. To address this issue and improve users’ mental well-being, social media use interventions (eg, abstinence from social media) have been developed and evaluated. However, there is limited understanding of the effectiveness of these interventions in improving mental well-being.
Objective
This systematic review aimed to synthesize the literature on the effectiveness of social media use interventions in improving mental well-being in adults.
Methods
A systematic search (January 1, 2004, to July 31, 2022) was completed across 3 databases in accordance with the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines. Experimental studies evaluating the impact of social media use interventions on mental well-being in adults were included. Outcomes related to mental well-being, such as depression, anxiety, stress, and loneliness, were included. A narrative synthesis without meta-analysis was completed to summarize the study characteristics and effectiveness by outcome and intervention type. The Effective Public Health Practice Project Quality Assessment Tool was used to measure the quality of the studies.
Results
Of the 2785 studies identified through the systematic search, 23 (0.83%) were included in the analysis. Many of the included studies (9/23, 39%) found improvements in mental well-being, some (7/23, 30%) found mixed effects, and others (7/23, 30%) found no effect on mental well-being. Therapy-based interventions that used techniques such as cognitive behavioral therapy were more effective than limiting use of social media or full abstinence from social media, with 83% (5/6) of these studies showing improvements in mental well-being compared with 20% (1/5) and 25% (3/12), respectively. Depression was the most frequently investigated and improved outcome with 70% (7/10) of the studies showing a significant improvement in depression after the intervention, whereas other outcomes showed more varied results. Quality was poor, with 96% (22/23) of the studies receiving a weak global score, mostly for issues related to selection bias because most of the studies (16/23, 70%) used a convenience sampling of university students.
Conclusions
This review provides some evidence that social media use interventions are effective in improving mental well-being, especially for depression and when using therapy-based interventions. Further experimental and longitudinal research is needed with representative samples to investigate who may benefit most from social media use interventions. This will help to develop guidance and recommendations for policy makers and clinicians on how best to manage problematic social media use.
Keywords: review, social media, mental well-being, mental health, addiction, intervention, mobile phone
Introduction
Background
Over the past decade, the rates of poor mental well-being have steadily increased in the United Kingdom, with steep increases seen for young adults [1,2]. As of 2022, in the United Kingdom, 1 in 4 individuals aged 17 to 19 years had reported a probable mental disorder, up from 1 in 10 in 2017 [3]. At the same time, social media use is on the rise, and it is estimated that 4.59 billion people globally used at least 1 form of social media in 2022 [4-6]. Social media generally refers to “internet-based tools that allow individuals and communities to gather and communicate; to share information, ideas, personal messages, images, and other content; and, in some cases, to collaborate with other users in real time” [7]. Social media has significantly changed how people communicate, form and maintain relationships, and perceive each other, and there is concern about how this affects mental health [8].
Evidence on the impact of social media on mental health is conflicting [9]. Some studies report benefits of social media use for mental health, including increased social support, strengthened bonds, and help seeking [10,11]. Other evidence has shown that high social media use has been linked with depression, anxiety, psychological problems, and distress, particularly for young people [12,13]. When social media use begins to interfere with everyday life, it can be considered problematic, with the most severe form arguably termed social media addiction [4,14]. Problematic social media use is described as a preoccupation with social media, resulting in distraction from primary tasks and the neglect of responsibilities in other aspects of life [15,16]. Reports suggest that 17.4% of social media users are affected by some form of problematic social media use, and it is most prevalent in adolescents and young adults [4,17]. Previous research has identified significant positive associations between problematic social media use and depression and anxiety [18]. However, the quality of studies linking social media use and mental well-being is limited by a reliance on unvalidated self-reported measures to assess social media use and by cross-sectional study designs in which causality cannot be inferred [9]. In addition, much of the research on the relationship between social media use and mental health has focused on adolescents, but there is growing evidence that social media use plays a role in adult mental health, particularly for young adults [18].
Social Media Use Interventions
Studies have explored the effectiveness of different types of social media use interventions to improve mental well-being, ranging from therapy-based approaches and taking complete breaks from social media to limiting social media use to a few hours a day [19-21]. Therapy-based approaches tend to use therapeutic techniques such as cognitive behavioral therapy (CBT) or group psychological counseling to prompt reflection on behaviors, thoughts, and feelings around social media and consideration of time management; for example, weekly group psychological counseling and CBT diaries have been used to help students manage their social media use by focusing on how they spend their time and how they can improve their relationships and communication skills offline [22]. These types of interventions are thought to bring about behavior change through facilitating self-control and reflection [23]. These therapeutic interventions can help individuals to regulate their social media use and reprioritize their social activity, which may improve well-being [24].
A recent systematic review that explored social media use interventions where participants had time-outs from smartphone use, or what is termed a digital detox, found mixed impacts of these interventions on mental well-being [25]. However, the review did not distinguish between abstinence from smartphone use more generally and specific abstinence from social media and did not explore effectiveness by the different types of social media interventions, such as limited use or full abstinence. Therefore, it is unclear what the effects of different types of interventions are on social media use and on mental well-being. It is also unclear from the literature what specific effects social media use interventions have on adults because much of the previous research in this area has focused on adolescents. Young adults are of particular interest because they have been identified as being vulnerable to problematic social media use in previous research [17,26]. A review specifically synthesizing the evidence on the effectiveness of social media use interventions on adults’ mental well-being will help to identify how best to support those with problematic social media use and poor mental well-being. Synthesizing these experimental studies will also help to understand the relationship between social media use and mental well-being. This systematic review aimed to (1) identify and describe evaluated social media use interventions, (2) report the effectiveness of these interventions on mental well-being outcomes, and (3) evaluate the quality of current research.
Methods
This review was completed in accordance with the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines [27], and the protocol is available via the Open Science Framework [28].
Search Strategy
The search was limited to studies published between January 1, 2004 (because the year 2004 marked the advent of widespread use of social media platforms), and July 31, 2022 [5]. The search strategy was developed by the research team with input from an experienced librarian. Three electronic databases were searched independently: MEDLINE, PsycINFO, and Web of Science. Papers at full-text screening were used for backward citation chaining, and the reference lists of similar previous reviews were checked for additional references. The search strategy for MEDLINE can be found in Multimedia Appendix 1.
Inclusion and Exclusion Criteria
The inclusion and exclusion criteria listed in Table 1 were applied.
Table 1.
Inclusion and exclusion criteria.
| Concepts | Inclusion criteria | Exclusion criteria |
| Population |
|
|
| Intervention |
|
|
| Comparator |
|
|
| Outcome |
|
|
| Study types |
|
|
| Publication types |
|
|
aCBT: cognitive behavioral therapy.
bN/A: not applicable.
cFOMO: fear of missing out.
Screening
We used the referencing manager software Rayyan to screen articles. Titles and abstracts were screened based on the inclusion and exclusion criteria, and 10.02% (279/2785) of the abstracts were screened by a second reviewer, with any conflicts resolved in discussion. The Cohen κ score was 0.56, with moderate agreement [33]. The full texts of the remaining articles were then screened, with 10% (4/42) screened by a second reviewer.
Data Extraction
Information on the authors, year, country of origin, aims, methods, types of interventions, main findings, and limitations of each study was extracted using a data extraction table in Excel (Microsoft Corp). The extraction of 26% (11/42) of the full-text articles was checked by a second reviewer to ensure accuracy and consistency.
Quality Assessment
The Effective Public Health Practice Project Quality Assessment Tool was used to assess quality because this is a validated tool designed to assess quality in public health topics [34]. All studies were given a global score (strong, moderate, or weak) based on 6 key topics: selection bias, study design, confounders, blinding, data collection method, and withdrawals or dropouts. Refer to Multimedia Appendix 2 for a breakdown of the scoring criteria for each key area and overall.
Analysis
A narrative synthesis without meta-analysis was completed owing to the heterogeneity of the outcomes and interventions. We summarized the studies, intervention characteristics, and effectiveness by outcome and type of intervention. We calculated the effect size (Cohen d) for all studies, where possible, to compare effectiveness across outcomes and intervention types.
Results
Search Results
The details of the search process and included studies are summarized in Figure 1.
Figure 1.
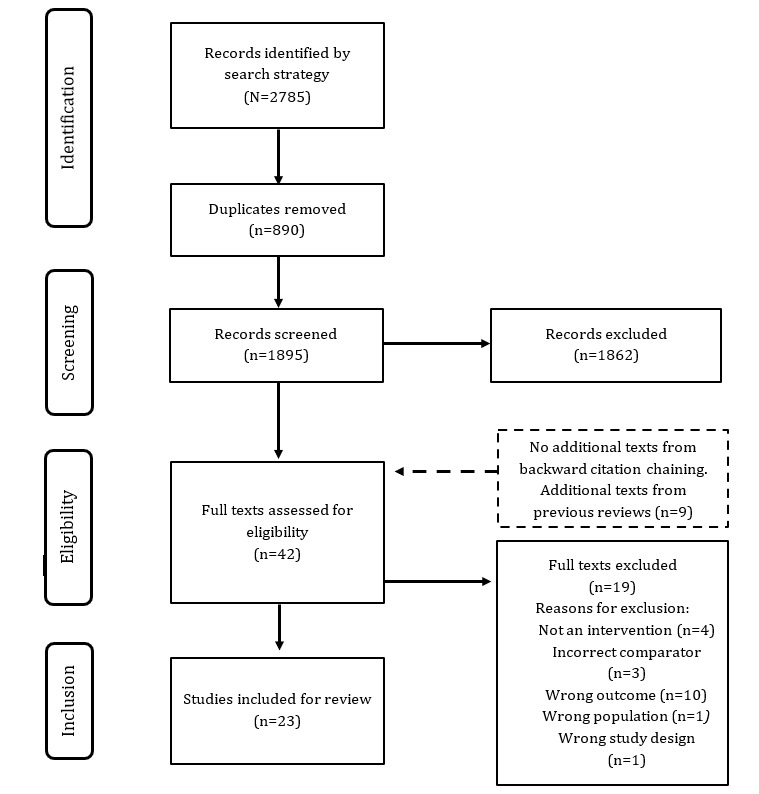
PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) flowchart of the systematic search results.
The search strategy yielded 2785 research papers, of which, after removing duplicates, 1895 (68.05%) were selected for title and abstract screening. Of these 1895 papers, we excluded 1862 (98.26%) based on the inclusion and exclusion criteria and added 9 texts based on the reference list of a previous review. Of these 42 papers eligible for full-text screening, 23 (55%) were included for final analysis.
Study Characteristics
Study characteristics are summarized in Table 2. All studies were published between 2016 and 2022, with the most common locations being the United States (6/23, 26%), the United Kingdom (5/23, 22%), and China (3/23, 13%). Most of the interventions targeted social media use on general social media sites (10/23, 44%) and Facebook (10/23, 44%), followed by those targeting Instagram (6/23, 26%), Twitter (3/23, 13%), Snapchat (3/23, 13%), TikTok (2/23, 9%), Pinterest (1/23, 4%), and Tumblr (1/23, 4%). Almost a third (7/23, 30%) of the studies targeted the use of multiple specific social media platforms. Randomized controlled trials were the most frequent study design (21/23, 91%). Only 2 (9%) of the 23 studies were pre- and postintervention studies, measuring mental well-being before and after an intervention with no control group [35,36]. There were 3 main types of interventions. Most of the studies (12/23, 52%) evaluated the impact of full abstinence from social media, with the abstinence period ranging from 1 day to 4 weeks. This was followed by therapy-based interventions such as counseling or CBT approaches (6/23, 26%) [22]. Many of the therapy-based types of interventions were self-guided (4/6, 67%) [37-40], with 2 (50%) of these 4 interventions using internet-based app–based platforms [38,39] and 2 (50%) of these 4 interventions using CBT-based diaries to reflect on social media use and time management [37,40]. Of the 6 therapy-based interventions, 1 (17%) used a mixture of in-person peer-based group psychological counseling and an internet-based social media group to share suggestions for alternative activities to social media use [22], 1 (17%) used entirely in-person sessions with training in basic mindfulness skills and values clarification based on acceptance and commitment therapy concepts [35], and 1 (17%) also encouraged limitation of social media use to only a few hours a day [37]. Roughly a quarter (5/23, 22%) of all included studies explored the effect of limiting social media use per day, with intervals ranging from 10- to 60-minute restrictions. More than a third (9/23, 39%) of the included interventions lasted 1 week, with the shortest lasting 1 day and the longest lasting 5 weeks [35].
Table 2.
Characteristics of studies and social media use interventions sorted by intervention type.
| Study, year; country | Study design | Intervention type | Social media intervention target | Intervention duration | Comparator | Sample size, n | Age (years), range (mean, SD) | |
| Interventions involving full abstinence from social media | ||||||||
|
|
Brown and Kuss [36], 2020; United Kingdom | Pre-post study | Full abstinence | Generala | 1 week | None | 61 | 20-49 (24.40, 4.95) |
|
|
Fioravanti et al [41], 2020; Italy | RCTb | Full abstinence | 1 week | Controlc | 80; IGd: 40, CGe: 40 | ≥18 (25.05, 4.17) | |
|
|
Hall et al [42], 2019; United States | RCT | Full abstinence | Facebook, Instagram, Snapchat, and Twitter | 4 groups: 1 week, 2 weeks, 3 weeks, and 4 weeks | Control | 130; IG 1 week: 28, IG 2 weeks: 17, IG 3 weeks: 24, and IG 4 weeks: 26; CG: 35 | 18-68 (26.80, 11.40) |
|
|
Hanley et al [43], 2019; Australia | RCT | Full abstinence | Facebook and Instagram | 1 week | Control | 78; IG: 40, CG: 38 | 18-48 (30.85, 7.12) |
|
|
Lambert et al [44], 2022; United Kingdom | RCT | Full abstinence | Facebook, Twitter, TikTok, and Instagram | 1 week | Control | 154; IG: 81, CG: 73 | ≥18 (28.90, 12.75) |
|
|
Mitev et al [45], 2021; United Kingdom and Bulgaria | RCT (crossover trialf) | Full abstinence | General | 3 days | Control | 232; IG: 116, CG: 116 | 18-71 (24.70, N/Rg) |
|
|
Mosquera et al [46], 2020; United States | RCT | Full abstinence | 1 week | Control | 167; IG: 77, CG: 90 | N/R; undergraduates | |
|
|
Przybylski et al [47], 2021; United Kingdom, United States, and Hong Kong | RCT (crossover trial) | Full abstinence | General | 1 day | Control | 297; IG: 297, CG: 297 | 18-56 (20.50, 2.86) |
|
|
Tromholt [48], 2016; Denmark | RCT | Full abstinence | 1 week | Control | 888; IG: 516, CG: 372 | N/R (34.00, 8.74) | |
|
|
Turel et al [49], 2018; United States | 2×2 RCT | Full abstinence | 1 week | Control | 555; IG: 413, CG: 142 | 19-54 (24.01, 4.14) | |
|
|
Vally and D’Souza [50], 2019; United Arab Emirates | RCT | Full abstinence | General | 1 week | Control | 78; IG: 39, CG: 39 | 18-27 (22.13, N/R) |
|
|
Vanman et al [51], 2018; Australia | RCT | Full abstinence | 5 days | Control | 138; IG: 60, CG: 78 | 18-40 (22.43, N/R) | |
| Therapy-based interventions | ||||||||
|
|
Chen et al [22], 2022; China | RCT | Group psychological counseling | General | 1 month | Control | 60; IG: 30, CG: 30 | N/R; undergraduates |
|
|
Hou et al [40], 2019; China | 2×2 RCT | Cognitive reconstruction, reminder cards, and diaries | General | 2 weeks | Control | 38; IG: 21, CG: 17 | N/R (19.71, 1.43) |
|
|
O’Connell [35], 2020; United Arab Emirates | Pre-post study | 1 hour per week mindfulness workshop | General | 5 weeks | None | 24; N/R | 18-25 (N/R) |
|
|
Esmaeili Rad and Ahmadi [38], 2018; Iran | RCT | Reality therapy mobile app+reflective questionnaires | General | 2 weeks | Control (only questionnaires) | 200; IG: 100, CG: 100 | 18-28 (N/R) |
|
|
Throuvala et al [39], 2020; United Kingdom | RCT | CBTh-based app | General | 10 days | Control | 143; IG: 72, CG: 71 | 18-32 (20.72, 3.12) |
|
|
Zhou et al [37], 2021; China | RCT | CBT-based part abstinence (4 of 7 weekdays)+daily reflective diaries | General | 2 weeks | Control (social media as usual+daily diaries) | 65; IG: 33, CG: 32 | N/R (28.80, 4.90) |
| Interventions involving limited social media use | ||||||||
|
|
Brailovskaia et al [52], 2020; Germany | RCT | Limited use (20 min/d) | 2 weeks | Control | 286; IG: 140; CG: 146 | 18-59 (25.39, 5.89) | |
|
|
Graham et al [53], 2021; New Zealand | RCT | Limited use (10 min/d) | Facebook, Instagram, and Snapchat | 1 week | Control | 184; IG: 92, CG: 92 | 18-61 (22.46, 6.83) |
|
|
Hunt et al [54], 2018; United States | RCT | Limited use (10 min/d) | Facebook, Instagram, and Snapchat | 3 weeks | Control | 143; N/R | N/R; undergraduates |
|
|
Hunt et al [55], 2021; United States | RCT | Limited use (30 min/d) | Facebook, Instagram, Twitter, and Snapchat | 3 weeks | (1) Control and (2) limited active group (30 min/d+1 action every 3 min, eg, posting and replying) | 88; N/R | N/R; undergraduates |
|
|
Thai et al [56], 2021; Canada | RCT | Limited use (60 min/d) | Instagram, Facebook, Twitter, Snapchat, TikTok, Pinterest, and Tumblr | 3 weeks | Control | 38; IG: 16, CG: 22 | 17-25 (N/R, 0.94) |
aTargeting any social media platform.
bRCT: randomized controlled trial.
cUsual social media use.
dIG: intervention group.
eCG: control group.
fAll participants receive all interventions, but the order in which they receive them (the sequence) is randomized.
gN/R: not reported.
hCBT: cognitive behavioral therapy.
Sample Characteristics
Sample sizes ranged from 24 to 888 individuals, with 44% (10/23) of the studies including a sample size of <100 people. Where provided, sample ages ranged from 17 to 71 years, and 61% (14/23) of the studies reported mean ages between 20 and 30 years. Of the 23 studies, 4 (17%) did not provide ages and categorized participants as undergraduates [22,46,54,55]. A little more than half (12/23, 52%) of the studies recruited participants via university sampling, 30% (7/23) used web advertisements, and 17% (4/23) combined these methods [39,42,51,53].
Quality Assessment
Nearly all studies (22/23, 96%) were given a weak global score, and no studies achieved a strong global score. Only the study by Throuvala et al [39] achieved a moderate score and this study showed a beneficial effect of the intervention on outcomes. Most of the studies were subject to selection bias, with 70% (16/23) being of moderate quality and 30% (7/23) being of weak quality on this criterion, because most of the studies (16/23, 70%) used convenience sampling from university populations. Most of the studies (21/23, 91%) did not report blinding of the researcher or participants. A little more than a third (8/23, 35%) of the studies were weak in study design because although they randomized participants, they did not report how they did this. The studies had relatively low withdrawals and dropouts, with a little more than half (12/23, 52%) reporting that ≥80% of the participants completed the studies. Less than half (9/23, 39%) of the studies fully accounted for confounding variables. A little more than half (12/23, 52%) demonstrated that the data collection tools used were reliable and valid. Scores for all sections are provided in Multimedia Appendix 3 alongside the effectiveness of the interventions.
Mental Well-Being Outcomes and Effectiveness
The details of study outcomes in relation to mental well-being are provided in Table 3. The main outcomes related to mental well-being reported in the studies were depression, life satisfaction, anxiety, fear of missing out (FOMO), mental well-being, positive affect, negative affect, loneliness, stress, self-esteem, and mindfulness. Depression was the most common outcome that was assessed (10/23, 44%), followed by life satisfaction (9/23, 39%), mental well-being (8/23, 35%), and anxiety (6/23, 26%). The least common outcomes that were assessed were self-esteem (3/23, 13%) and mindfulness (2/23, 9%). Most of the studies (18/23, 78%) investigated >1 mental well-being outcome. More than a third (9/23, 39%) of the studies demonstrated improvements in well-being–related outcomes. Almost one-third (7/23, 30%) of the studies found mixed effects across different well-being–related outcomes [35,41,46,49-51,54], and almost a third (7/23, 30%) found no effect [42,43,45,47,52,53,56].
Table 3.
Effectiveness of social media use interventions on mental well-being sorted by intervention type.
| Study, year | Outcomes | Measures | Comparison measurement | Postintervention-reported values (unless labeled) | Effect size (Cohen d) and interpretation | Main finding | Direction of effect | |
| Interventions involving full abstinence from social media | ||||||||
|
|
Brown and Kuss [36], 2020 |
|
|
Mean difference between before and after the intervention (SD) |
|
|
Significant improvements after the intervention | ↑g |
|
|
Fioravanti et al [41], 2020 |
|
|
Calculated mean difference between IGj and CGk for women and men |
|
|
Significantly improved life satisfaction and positive affect for women but not for men in the IG compared with those in the CG | ↕o |
|
|
Hall et al [42], 2019 |
|
|
Mean (SD) |
|
|
No significant difference for the IG compared with the CG across all measures | ↔q |
|
|
Hanley et al [43], 2019 |
|
|
Standardized coefficients from multiple regression |
|
|
No significant difference for the IG compared with the CG across all measures | ↔ |
|
|
Lambert et al [44], 2022 |
|
|
Mean (SD) |
|
|
Significant improvements for the IG compared with the CG across all measures | ↑ |
|
|
Mitev et al [45], 2021 | Mental well-being | Daily satisfaction question, self-esteem scale, and positive and negative affect scales were combined to create an overall composite score of participants’ well-being | F value and partial eta–squared value | F2,416=0.11; P=.89; ηp2=.001 | 0.06 (X) | No significant difference for the IG compared with the CG | ↔ |
|
|
Mosquera et al [46], 2020 |
|
|
Mean difference between before and after the intervention (SD) |
|
—t | Significant improvements for the IG compared with the CG for depression but not for life satisfaction | ↕ |
|
|
Przybylski et al [47], 2021 |
|
|
Mean (SD) |
|
|
No significant difference for the IG compared with the CG | ↔ |
|
|
Tromholt [48], 2016 |
|
|
Mean (SD) |
|
|
Significant improvements for the IG compared with the CG across all measures | ↑ |
|
|
Turel et al [49], 2018 |
|
|
Marginal means (95% CI) |
|
|
Significantly reduced absolute stress in the IG but not relative stress compared with the CG | ↕ |
|
|
Vally and D’Souza [50], 2019 |
|
|
Mean (SD) |
|
|
Significantly reduced life satisfaction and increased negative feelings and loneliness for the IG compared with the CG but no difference in positive affect or stress | ↕ |
|
|
Vanman et al [51], 2018 |
|
|
Mean difference between before and after the intervention (SD) |
|
0.54 (M) | The IG had significantly reduced life satisfaction compared with the CG but no other outcomes were significantly different | ↕ |
| Therapy-based interventions | ||||||||
|
|
Chen et al [22], 2022 |
|
|
Mean (SD) |
|
|
Significant improvements for the IG compared with the CG across all measures | ↑ |
|
|
Hou et al [40], 2019 |
|
|
Mean (SD) |
|
|
Significant improvements for the IG compared with the CG across all measures | ↑ |
|
|
O’Connell [35], 2020 |
|
|
Mean difference between before and after the intervention (N/Rac) |
|
|
Significant reduction in mindfulness after the intervention but no difference in FOMO, well-being, depression, or anxiety | ↕ |
|
|
Esmaeili Rad and Ahmadi [38], 2018 |
|
|
Mean rankae (N/R) |
|
|
Significant improvements within the IG across all measures | ↑ |
|
|
Throuvala et al [39], 2020 |
|
|
Mean (SD) |
|
|
Significant improvements for the IG compared with the CG across all measures | ↑ |
|
|
Zhou et al [37], 2021 | Life satisfaction | SWLS | Mean (SD) |
|
0.50 (M) | Significant improvements for the IG compared with the CG | ↑ |
| Interventions involving limited social media use | ||||||||
|
|
Brailovskaia et al [52], 2020 |
|
|
Mean difference (95% CI) between the groups |
|
|
No significant improvement in the IG compared with the CG across both measures | ↔ |
|
|
Graham et al [53], 2021 | Well-being | WEMWBS | Mean (SD) |
|
0.01 (X) | No significant improvement in the IG compared with the CG | ↔ |
|
|
Hunt et al [54], 2018 |
|
|
Mean |
|
— | Significant improvements in depression and loneliness for the IG compared with the CG; no significance for other outcomes | ↕ |
|
|
Hunt et al [55], 2021 | Depression | BDI | Mean (SD) |
|
— | Significant improvements for IG participants who were highly depressed compared with CG and AG participants | ↑ |
|
|
Thai et al [56], 2021 |
|
|
Mean (SD) |
|
|
No significant improvement in the IG compared with the CG across both measures | ↔ |
aFOMO: fear of missing out.
bFoMOs: Fear of Missing Out Scale.
cWEMWBS: Warwick-Edinburgh Mental Well-Being Scale.
dP<.001.
eM: medium.
fS: small.
gBeneficial effect.
hSWLS: Satisfaction With Life Scale.
iPANAS: Positive and Negative Affect Schedule.
jIG: intervention group.
kCG: control group.
lP<.05.
mL: Large.
nX: negligible.
oMixed effects.
pSF-36: 36-item Short Form Health Survey.
qNo effect.
rGAD-7: General Anxiety Disorder-7.
sOECD: Organisation for Economic Co-operation and Development.
tNot available (number in each group was not specified to calculate effect size).
uAverage mean and SD reported across the 3 countries because the relationship among variables was the same across the countries. Estimates based on unadjusted means because the adjusted means were not provided.
vCES-D: Center for Epidemiological Studies Depression Scale.
wPSS: Perceived Stress Scale.
xCES-D-20: Center for Epidemiological Studies Depression Scale, 20-item version.
yULS-8: University of California Los Angeles Loneliness Scale.
zGHQ-30: General Health Questionnaire-30.
aaMAAS: Mindful Attention Awareness Scale.
abPWB: Psychological Well-Being Scale.
acN/R: not reported.
adBDI: Beck Depression Inventory.
aeComparing the IG between before the intervention and after. The effect of the intervention between the IG and the CG was not reported and could not be calculated.
afDASS-21: Depression Anxiety Stress Scales 21.
agAG: active group (limited use of social media at 30 minutes per day plus 1 action every 3 minutes, eg, posting and replying).
An overview of the effectiveness of the interventions by outcome is shown in Figure 2. The most improved outcome was depression, with 70% (7/10) of the studies that measured this outcome showing a benefit of the intervention, with large or medium effect sizes being reported [22,38,44,46,48,54,55], whereas 30% (3/10) showed no effect of the intervention [35,52,56]. Anxiety was the next most improved outcome, with 50% (3/6) of the studies that assessed this outcome showing significant improvement in anxiety, with medium and large effect sizes being reported [38,39,44]; however, 50% (3/6) reported no effect on anxiety [35,54,56]. FOMO also improved in 50% (2/4) of the studies assessing this outcome, with medium and small effect sizes being reported [36,39], whereas 50% (2/4) found no effect on FOMO [35,54]. Brown and Kuss [36] also explored the effect on FOMO based on gender and identified no significant differences between men and women after the intervention. Mental well-being improved in 38% (3/8) of the studies assessing this outcome, with small, medium, and large effect sizes being reported [36,40,44], whereas 63% (5/8) found no significant improvements in mental well-being [35,42,45,53,54]. Self-esteem improved in 33% (1/3) of the studies assessing this outcome, with a medium effect size being reported [40], but 67% (2/3) found no effect of the intervention on self-esteem [47,54].
Figure 2.
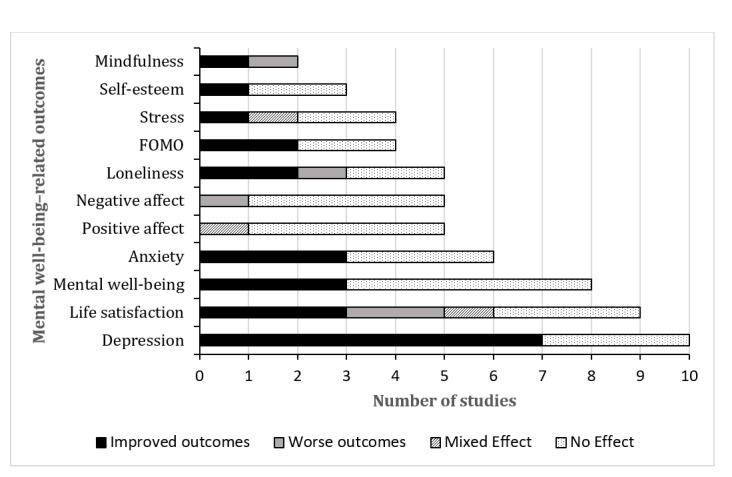
Summary of social media use intervention effects on mental well-being–related outcomes. FOMO: fear of missing out.
The other outcomes showed mixed and some negative results. Loneliness was reduced in 40% (2/5) of the studies that measured this outcome [22,54], whereas 40% (2/5) found no effect [42,51]; however, 1 (20%) of these 5 studies also found that the intervention increased loneliness, with a medium effect size being reported [50]. Mindfulness improved in 1 (50%) of the 2 studies that measured this outcome, with a large effect size being reported [39], but it was found to reduce in another study (1/2, 50%), with a small effect size being reported [35]. Life satisfaction improved in a third (3/9, 33%) of the studies that measured this outcome, with small, medium, and large effect sizes being reported [37,38,48], whereas another third (3/9, 33%) of the studies showed no effect [43,46,52], and 22% (2/9) found full abstinence to be harmful, reducing life satisfaction, with medium effect sizes being reported [50,51]. Of these 9 studies, 1 (11%) found mixed effects because a significant improvement in life satisfaction was found for women, with a large effect size being reported, but not for men [41]. For stress, 1 (25%) of the 4 studies that measured this outcome found reductions in stress, with a medium effect size being reported [39], but half (2/4, 50%) of the studies showed no effect of the intervention on stress [50,51], whereas 25% (1/4) showed mixed effects because absolute stress reduced but the relative stress score compared with the score at baseline did not [49]. For negative affect, 1 (20%) of the 5 studies that measured this outcome found that negative affect increased after the intervention, with a small effect size being reported [50], but the other studies (4/5, 80%) showed no effect [41,43,47,51]. Positive affect also did not change after the intervention in most of the studies (4/5, 80%) [43,47,50,51]; however, 20% (1/5) found mixed results because positive affect improved for women, with a small effect size being reported, but not for men [41].
Effectiveness by Intervention Type
Figure 3 shows an overview of the effectiveness of social media use interventions by intervention type. Therapy-based trials were the most effective because 83% (5/6) of the studies that assessed this intervention type found significant improvements in mental well-being outcomes [22,37-40], and only 17% (1/6) found mixed effects [35]. Full-abstinence interventions showed mixed effectiveness overall, with 42% (5/12) of them showing mixed effects [41,46,49-51], a third (4/12, 33%) showing no effect [42,43,45,47], and a quarter (3/12, 25%) showing a benefit of the intervention [36,44,48]. Social media use interventions that limited use also showed mixed effectiveness overall, with more than half (3/5, 60%) of the studies showing no effect [52,53,56] and 20% (1/5) showing an improvement [55] and mixed effects [54], respectively.
Figure 3.
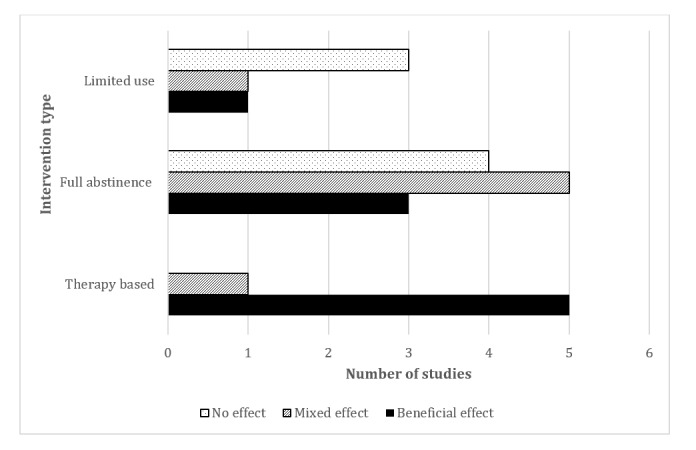
Summary of the effectiveness of the different types of social media use interventions on mental well-being–related outcomes.
Discussion
Principal Findings
This review provides some evidence for the improvement of mental well-being in adults after social media use interventions. Of the 23 studies included in our analysis, 9 (39%) demonstrated improvements in mental well-being–related outcomes, with most of them (8/9, 89%) showing medium to large effect sizes. Depression was the most improved outcome overall, with 70% (7/10) of the studies that assessed depression showing improvement. Therapy-based interventions were the most effective, with 83% (5/6) of the studies evaluating these interventions showing improvement. Most of the studies (22/23, 96%) were of low quality, with significant issues related to selection bias and blinding affecting their quality.
This review found that interventions that simply restrict social media use or impose full abstinence may not have as much benefit for mental well-being as therapy-based interventions. These interventions used established approaches such as counseling and CBT-based techniques to encourage mindfulness and reflection on how social media activity affects thoughts, emotions, and behavior. Therapy-based interventions may be more effective in causing behavior change in users than abstinence by enabling them to replace negative actions with structured goals and positive thinking and by providing motivation [58]. Therapy-based interventions may also help to reduce FOMO by encouraging individuals to reevaluate life priorities, focus on other activities, and reduce social comparison and envy [36,39].
We found limiting social media use to be the least effective method. One hypothesis is that users would still have been exposed to social media during the trial and may have intensified their use owing to an awareness of a time restriction. This would have offset any potential positive improvement. Adherence to limiting social media use or abstaining from social media use may also have been challenging for participants, and adherence is difficult to track and measure across devices used to access social media [37]. In 1 study, 19.4% (35/180) of the participants were excluded from analysis because they were unable to abstain from social media for >2 days, which may give an indication of compliance rates in these studies [42]. These findings overall suggest that health and care professionals, mental health charities, and public health bodies should encourage the use of therapy-based approaches to manage social media use rather than focusing on reducing time spent on social media. These interventions can also be relatively cost-effective because this review showed improvements in participants’ well-being after they used internet-based self-guided therapy-based interventions to manage problematic social media use. However, delivering therapy-based approaches to manage (problematic) social media use is currently limited owing to resource and time constraints in health and care systems.
This review found that 3 (13%) of the 23 studies showed a reduction in some mental well-being–related outcomes after the intervention, such as life satisfaction and loneliness [35,50,51]. The causes for these findings could be due to methodological reasons because the authors of 1 (33%) of these 3 studies proposed that their study participants were unaware at the time of recruitment that abstinence from social media may be required [50], which may have made participants less receptive to the intervention and eliminated the beneficial consequences of abstinence that may have arisen in other studies. Previous research also suggests that reducing or limiting social media use can reduce mental well-being by causing a loss of social connection and increasing loneliness [9]. Some individuals are reported to find social connections easier to maintain over the web, with social media enabling users to preserve their relationships [59,60]. Social media can also help to create and maintain social capital, fostering inclusion within web-based communities [61]; for instance, members of the lesbian, gay, bisexual, transgender, queer, and similar minority community report greater levels of social support over the web [62].
This review supports evidence from previous studies that show that the link between social media use and mental well-being is conflicting, with there being some benefits and some disadvantages of social media use related to mental well-being [9,25]. The variation in effectiveness across the studies could be due to individual differences [63]. Different people will have different responses to social media, and self-regulatory capabilities may be affected by factors such as gender, age, and personality traits [64]. Previous research has shown that those with neurotic or introverted tendencies have a higher risk of addiction to internet content [65]. Others may not be affected by social media use owing to elevated levels of digital resilience. Digital resilience is a person’s ability to cope with the negative consequences of being over the web, such as cyberbullying and misleading information [66,67]. Gender has been found to be a moderating factor in previous studies examining the relationship between social media use and mental well-being, with adolescent girls seeming to experience more negative effects from social media use than adolescent boys [4,68,69]. In this review, we found that 1 (4%) of the 23 studies showed that abstinence increased positive affect and life satisfaction for women but not for men, also suggesting that gender may affect the relationship between social media use and mental well-being [41]. Future research is needed to explore who may be most affected by problematic social media use to enable the development of more targeted interventions to improve mental well-being.
Limitations
There was a large degree of heterogeneity in the studies reviewed, with several different intervention types and outcome measures used. Therefore, it was not possible to conduct a meta-analysis to provide integrated results on the outcomes of the social media use interventions [70]. A further limitation to this review is that the search strategy may not have retrieved all relevant papers owing to the inclusion of English-language publications only. Our review also did not include unpublished studies; thus, it was not possible to estimate the degree of publication bias. This review also did not explore the impact of the type of social media use, such as passive use or active use, because this was out of the scope of the review, but this could affect mental well-being. Active use denotes direct messaging, posting, or responding to content, whereas passive use corresponds to scrolling and browsing profiles. Previous literature has suggested that passive use is associated with greater declines in subjective well-being [71,72], but a recent review found that this was not supported across 40 survey-based studies [73]. The review suggested that future studies should explore the characteristics of the content of social media as well as its senders and receivers to understand how different uses of social media affect mental well-being [73]. Understanding this relationship could help to develop more targeted problematic social media use interventions that move beyond simply aiming to reduce time spent on social media by targeting the reduction of specific negative activities or interactions.
A major limitation of the studies included in this review is that the majority (16/23, 70%) relied largely on convenience samples of those who were likely to be interested in reducing their social media use and improving their mental health. In addition, more than half (16/23, 70%) of the studies recruited university students. Therefore, these results must be interpreted with caution because they are not generalizable to all adults and are likely to be more relevant for young adults. Furthermore, none of the studies received a strong global score for quality using the Effective Public Health Practice Project Quality Assessment Tool. The sustainability of these interventions is also difficult to establish because most of the interventions (20/23, 87%) lasted <1 month, and the outcomes were assessed immediately after the interventions. Only 2 (9%) of the 23 studies included a longer-term measure. Brailovskaia et al [52] found consistency with their short-term recorded outcomes, with no significant difference in life satisfaction and depression between groups 3 months after the intervention. By contrast, Chen et al [22] found that the significant improvements in depression and loneliness for the intervention group continued to remain at 2 months.
Conclusions
There is some evidence that social media use interventions are effective in improving mental well-being in adults, especially for depression and when using therapy-based interventions. Current experimental research is of low quality, with issues of selection bias making it difficult to generalize the findings. Further experimental and longitudinal research is needed with representative samples to investigate who may benefit most from social media use interventions. Health and care professionals should be aware of the growing evidence that reducing social media use alone is unlikely to benefit mental well-being. Taking a more therapy-based approach and reflecting on how and why individuals are interacting with social media and managing these behaviors could help to improve mental well-being.
Acknowledgments
The authors would like to thank the librarians at University College London for helping them to refine the search strategy. RP holds a fellowship (MH013) funded by the Three National Institute for Health and Care Research (NIHR) Research Schools Mental Health Programme. This research is also supported by the NIHR Applied Research Collaboration North Thames. The views expressed are those of the authors and not necessarily those of the NIHR or the Department of Health and Social Care.
Abbreviations
- CBT
cognitive behavioral therapy
- FOMO
fear of missing out
- PRISMA
Preferred Reporting Items for Systematic Reviews and Meta-Analyses
Search strategy used for MEDLINE.
Quality assessment tool for quantitative studies scoring criteria.
Quality scores according to the Effective Public Health Practice Project Quality Assessment Tool and overall effectiveness of social media use interventions on outcomes.
Footnotes
Conflicts of Interest: None declared.
References
- 1.Mental Disorders. Health and Social care information centre. 2020. [2022-08-26]. https://tinyurl.com/5ezy99tc .
- 2.Mental health of children and young people in England 2021 - wave 2 follow up to the 2017 survey. Mental Health of Children and Young People Surveys. 2021. [2022-09-02]. https://digital.nhs.uk/data-and-information/publications/statistical/mental- health-of-children-and-young-people-in-england/2021-follow-up-to-the-2017-survey .
- 3.Mental health of children and young people in England 2022 - wave 3 follow up to the 2017 survey. National Health Service Digital. 2022. [2022-12-01]. https://digital.nhs.uk/data-and-information/publications/statistical/mental-health-of-children-and-young -people-in-england/2022-follow-up-to-the-2017-survey .
- 4.Henzel V, Håkansson A. Hooked on virtual social life. Problematic social media use and associations with mental distress and addictive disorders. PLoS One. 2021 Apr 8;16(4):e0248406. doi: 10.1371/journal.pone.0248406. https://dx.plos.org/10.1371/journal.pone.0248406 .PONE-D-20-07416 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Hall M. Facebook. Britannica. 2022. [2022-08-19]. https://www.britannica.com/topic/Facebook .
- 6.Number of social media users worldwide from 2018 to 2027 (in billions) Statista. 2022. [2022-11-04]. https://www.statista.com/statistics/278414/number-of-worldwide-social-network-users/
- 7.Ventola C. Social media and health care professionals: benefits, risks, and best practices. P T. 2014 Jul;39(7):491–520. https://europepmc.org/abstract/MED/25083128 . [PMC free article] [PubMed] [Google Scholar]
- 8.Brevers D, Turel O. Strategies for self-controlling social media use: classification and role in preventing social media addiction symptoms. J Behav Addict. 2019 Sep 01;8(3):554–63. doi: 10.1556/2006.8.2019.49. https://europepmc.org/abstract/MED/31545100 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Orben A. Teenagers, screens and social media: a narrative review of reviews and key studies. Soc Psychiatry Psychiatr Epidemiol. 2020 Apr;55(4):407–14. doi: 10.1007/s00127-019-01825-4.10.1007/s00127-019-01825-4 [DOI] [PubMed] [Google Scholar]
- 10.Lin S, Liu D, Niu G, Longobardi C. Active social network sites use and loneliness: the mediating role of social support and self-esteem. Curr Psychol. 2020 Feb 13;41(3):1279–86. doi: 10.1007/s12144-020-00658-8. [DOI] [Google Scholar]
- 11.Grieve R, Indian M, Witteveen K, Anne Tolan G, Marrington J. Face-to-face or Facebook: can social connectedness be derived online? Comput Human Behav. 2013 May;29(3):604–9. doi: 10.1016/j.chb.2012.11.017. https://www.sciencedirect.com/science/article/abs/pii/S0747563212003226 . [DOI] [Google Scholar]
- 12.Keles B, McCrae N, Grealish A. A systematic review: the influence of social media on depression, anxiety and psychological distress in adolescents. Int J Adolesc Youth. 2019 Mar 21;25(1):79–93. doi: 10.1080/02673843.2019.1590851. https://www.tandfonline.com/doi/full/10.1080/02673843.2019.1590851 . [DOI] [Google Scholar]
- 13.#StatusOfMind Social media and young people’s mental health and wellbeing. Royal Society for Public Health. [2023-07-02]. https://www.rsph.org.uk/our-work/campaigns/status-of-mind.html .
- 14.Cheng C, Lau YC, Chan L, Luk JW. Prevalence of social media addiction across 32 nations: meta-analysis with subgroup analysis of classification schemes and cultural values. Addict Behav. 2021 Jun;117:106845. doi: 10.1016/j.addbeh.2021.106845. https://linkinghub.elsevier.com/retrieve/pii/S0306-4603(21)00030-7 .S0306-4603(21)00030-7 [DOI] [PubMed] [Google Scholar]
- 15.Swar B, Hameed T. Fear of missing out, social media engagement, smartphone addiction and distraction: moderating role of self-help mobile apps-based interventions in the youth. Proceedings of the 10th International Joint Conference on Biomedical Engineering Systems and Technologies; BIOSTEC '17; February 21-23, 2017; Porto, Portugal. 2017. pp. 139–46. https://www.scitepress.org/Link.aspx?doi=10.5220/0006166501390146 . [DOI] [Google Scholar]
- 16.Uyaroğlu AK, Ergin E, Tosun AS, Erdem Ö. A cross-sectional study of social media addiction and social and emotional loneliness in university students in Turkey. Perspect Psychiatr Care. 2022 Oct;58(4):2263–71. doi: 10.1111/ppc.13056. [DOI] [PubMed] [Google Scholar]
- 17.Meng SQ, Cheng JL, Li YY, Yang XQ, Zheng JW, Chang XW, Shi Y, Chen Y, Lu L, Sun Y, Bao YP, Shi J. Global prevalence of digital addiction in general population: a systematic review and meta-analysis. Clin Psychol Rev. 2022 Mar;92:102128. doi: 10.1016/j.cpr.2022.102128.S0272-7358(22)00013-7 [DOI] [PubMed] [Google Scholar]
- 18.Hussain Z, Wegmann E, Yang H, Montag C. Social networks use disorder and associations with depression and anxiety symptoms: a systematic review of recent research in China. Front Psychol. 2020 Feb 21;11:211. doi: 10.3389/fpsyg.2020.00211. https://europepmc.org/abstract/MED/32153455 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Zhang X, Shi X, Xu S, Qiu J, Turel O, He Q. The effect of solution-focused group counseling intervention on college students' internet addiction: a pilot study. Int J Environ Res Public Health. 2020 Apr 07;17(7):2519. doi: 10.3390/ijerph17072519. https://www.mdpi.com/resolver?pii=ijerph17072519 .ijerph17072519 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Dogan H, Norman H, Alrobai A, Jiang N, Nordin N, Adnan A. A web-based intervention for social media addiction disorder management in higher education: quantitative survey study. J Med Internet Res. 2019 Oct 02;21(10):e14834. doi: 10.2196/14834. https://www.jmir.org/2019/10/e14834/ v21i10e14834 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Hiniker A, Hong SR, Kohno T, Kientz JA. MyTime: designing and evaluating an intervention for smartphone non-use. Proceedings of the 2016 CHI Conference on Human Factors in Computing Systems; CHI '16; May 7-12, 2016; San Jose, CA. 2016. pp. 4746–57. https://dl.acm.org/doi/10.1145/2858036.2858403 . [DOI] [Google Scholar]
- 22.Chen Y, Liu X, Chiu DT, Li Y, Mi B, Zhang Y, Ma L, Yan H. Problematic social media use and depressive outcomes among college students in China: observational and experimental findings. Int J Environ Res Public Health. 2022 Apr 19;19(9):4937. doi: 10.3390/ijerph19094937. https://www.mdpi.com/resolver?pii=ijerph19094937 .ijerph19094937 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Bandura A. Social cognitive theory of self-regulation. Organ Behav Hum Decis Process. 1991 Dec;50(2):248–87. doi: 10.1016/0749-5978(91)90022-L. https://www.sciencedirect.com/science/article/abs/pii/074959789190022L . [DOI] [Google Scholar]
- 24.Michie S, van Stralen MM, West R. The behaviour change wheel: a new method for characterising and designing behaviour change interventions. Implement Sci. 2011 Apr 23;6:42. doi: 10.1186/1748-5908-6-42. https://implementationscience.biomedcentral.com/articles/10.1186/1748-5908-6-42 .1748-5908-6-42 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Radtke T, Apel T, Schenkel K, Keller J, von Lindern E. Digital detox: an effective solution in the smartphone era? A systematic literature review. Mob Media Commun. 2021 May;10(2):190–215. doi: 10.1177/20501579211028647. https://journals.sagepub.com/doi/10.1177/20501579211028647 . [DOI] [Google Scholar]
- 26.Lu C, Zou L, Becker B, Griffiths MD, Yu Q, Chen ST, Demetrovics Z, Jiao C, Chi X, Chen A, Yeung A, Liu S, Zhang Y. Comparative effectiveness of mind-body exercise versus cognitive behavioral therapy for college students with problematic smartphone use: a randomized controlled trial. Int J Ment Health Promot. 2020;22(4):271–82. doi: 10.32604/ijmhp.2020.014419. https://www.techscience.com/IJMHP/v22n4/40887 . [DOI] [Google Scholar]
- 27.Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, Shamseer L, Tetzlaff JM, Akl EA, Brennan SE, Chou R, Glanville J, Grimshaw JM, Hróbjartsson A, Lalu MM, Li T, Loder EW, Mayo-Wilson E, McDonald S, McGuinness LA, Stewart LA, Thomas J, Tricco AC, Welch VA, Whiting P, Moher D. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021 Mar 29;372:n71. doi: 10.1136/bmj.n71. http://www.bmj.com/lookup/pmidlookup?view=long&pmid=33782057 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Plackett R. Protocol interventions for problematic social media use. Open Science Framework. 2022. [2022-12-08]. https://osf.io/ts8du .
- 29.Galderisi S, Heinz A, Kastrup M, Beezhold J, Sartorius N. Toward a new definition of mental health. World Psychiatry. 2015 Jun;14(2):231–3. doi: 10.1002/wps.20231. https://europepmc.org/abstract/MED/26043341 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Deniz M. Fear of missing out (FoMO) mediate relations between social self-efficacy and life satisfaction. Psicol Reflex Crit. 2021 Aug 23;34(1):28. doi: 10.1186/s41155-021-00193-w. https://europepmc.org/abstract/MED/34424439 .10.1186/s41155-021-00193-w [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Alutaybi A, Al-Thani D, McAlaney J, Ali R. Combating Fear of Missing Out (FoMO) on social media: the FoMO-R method. Int J Environ Res Public Health. 2020 Aug 23;17(17):6128. doi: 10.3390/ijerph17176128. https://www.mdpi.com/resolver?pii=ijerph17176128 .ijerph17176128 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Przybylski AK, Murayama K, DeHaan CR, Gladwell V. Motivational, emotional, and behavioral correlates of fear of missing out. Comput Human Behav. 2013 Jul;29(4):1841–8. doi: 10.1016/j.chb.2013.02.014. https://www.sciencedirect.com/science/article/abs/pii/S0747563213000800 . [DOI] [Google Scholar]
- 33.McHugh M. Interrater reliability: the kappa statistic. Biochem Med (Zagreb) 2012;22(3):276–82. https://europepmc.org/abstract/MED/23092060 . [PMC free article] [PubMed] [Google Scholar]
- 34.Thomas BH, Ciliska D, Dobbins M, Micucci S. A process for systematically reviewing the literature: providing the research evidence for public health nursing interventions. Worldviews Evid Based Nurs. 2004;1(3):176–84. doi: 10.1111/j.1524-475X.2004.04006.x.WVN04006 [DOI] [PubMed] [Google Scholar]
- 35.O’Connell C. How FOMO (Fear of Missing Out), the smartphone, and social media may be affecting university students in the Middle East. N Am J Psychol. 2020 Mar 01;22(1):83–102. doi: 10.31124/advance.14046824.v1. https://psycnet.apa.org/record/2020-12702-006 . [DOI] [Google Scholar]
- 36.Brown L, Kuss DJ. Fear of missing out, mental wellbeing, and social connectedness: a seven-day social media abstinence trial. Int J Environ Res Public Health. 2020 Jun 24;17(12):4566. doi: 10.3390/ijerph17124566. https://www.mdpi.com/resolver?pii=ijerph17124566 .ijerph17124566 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Zhou X, Rau PP, Yang CL, Zhou X. Cognitive behavioral therapy-based short-term abstinence intervention for problematic social media use: improved well-being and underlying mechanisms. Psychiatr Q. 2021 Jun;92(2):761–79. doi: 10.1007/s11126-020-09852-0.10.1007/s11126-020-09852-0 [DOI] [PubMed] [Google Scholar]
- 38.Esmaeili Rad M, Ahmadi F. A new method to measure and decrease the online social networking addiction. Asia Pac Psychiatry. 2018 Dec;10(4):e12330. doi: 10.1111/appy.12330. [DOI] [PubMed] [Google Scholar]
- 39.Throuvala MA, Griffiths MD, Rennoldson M, Kuss DJ. Mind over matter: testing the efficacy of an online randomized controlled trial to reduce distraction from smartphone use. Int J Environ Res Public Health. 2020 Jul 05;17(13):4842. doi: 10.3390/ijerph17134842.ijerph17134842 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Hou Y, Xiong D, Jiang T, Song L, Wang Q. Social media addiction: its impact, mediation, and intervention. Cyberpsychol. 2019 Feb 21;13(1):1–4. doi: 10.5817/cp2019-1-4. https://cyberpsychology.eu/article/view/11562 . [DOI] [Google Scholar]
- 41.Fioravanti G, Prostamo A, Casale S. Taking a short break from Instagram: the effects on subjective well-being. Cyberpsychol Behav Soc Netw. 2020 Feb;23(2):107–12. doi: 10.1089/cyber.2019.0400. [DOI] [PubMed] [Google Scholar]
- 42.Hall JA, Xing C, Ross EM, Johnson RM. Experimentally manipulating social media abstinence: results of a four-week diary study. Media Psychol. 2019 Nov 05;24(2):259–75. doi: 10.1080/15213269.2019.1688171. https://www.tandfonline.com/doi/abs/10.1080/15213269.2019.1688171?journalCode=hmep20 . [DOI] [Google Scholar]
- 43.Hanley SM, Watt SE, Coventry W. Taking a break: the effect of taking a vacation from Facebook and Instagram on subjective well-being. PLoS One. 2019 Jun 06;14(6):e0217743. doi: 10.1371/journal.pone.0217743. https://dx.plos.org/10.1371/journal.pone.0217743 .PONE-D-18-27980 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Lambert J, Barnstable G, Minter E, Cooper J, McEwan D. Taking a one-week break from social media improves well-being, depression, and anxiety: a randomized controlled trial. Cyberpsychol Behav Soc Netw. 2022 May;25(5):287–93. doi: 10.1089/cyber.2021.0324. [DOI] [PubMed] [Google Scholar]
- 45.Mitev K, Weinstein N, Karabeliova S, Nguyen T, Law W, Przybylski A. Social media use only helps, and does not harm, daily interactions and well-being. Technol Mind Behav. 2021 Jun 25;2(1):1–32. doi: 10.1037/tmb0000033. https://orca.cardiff.ac.uk/id/eprint/140263/3/a84b4400-9455-4258-baad-4aec648800eb.pdf . [DOI] [Google Scholar]
- 46.Mosquera R, Odunowo M, McNamara T, Guo X, Petrie R. The economic effects of Facebook. Exp Econ. 2019 Sep 26;23(2):575–602. doi: 10.1007/s10683-019-09625-y. https://link.springer.com/article/10.1007/s10683-019-09625-y . [DOI] [Google Scholar]
- 47.Przybylski AK, Nguyen TT, Law W, Weinstein N. Does taking a short break from social media have a positive effect on well-being? Evidence from three preregistered field experiments. J Technol Behav Sci. 2021 Feb 07;6(3):507–14. doi: 10.1007/s41347-020-00189-w. https://link.springer.com/article/10.1007/s41347-020-00189-w . [DOI] [Google Scholar]
- 48.Tromholt M. The Facebook experiment: quitting Facebook leads to higher levels of well-being. Cyberpsychol Behav Soc Netw. 2016 Nov;19(11):661–6. doi: 10.1089/cyber.2016.0259. [DOI] [PubMed] [Google Scholar]
- 49.Turel O, Cavagnaro DR, Meshi D. Short abstinence from online social networking sites reduces perceived stress, especially in excessive users. Psychiatry Res. 2018 Dec;270:947–53. doi: 10.1016/j.psychres.2018.11.017.S0165-1781(18)30607-3 [DOI] [PubMed] [Google Scholar]
- 50.Vally Z, D'Souza CG. Abstinence from social media use, subjective well-being, stress, and loneliness. Perspect Psychiatr Care. 2019 Oct;55(4):752–9. doi: 10.1111/ppc.12431. [DOI] [PubMed] [Google Scholar]
- 51.Vanman EJ, Baker R, Tobin SJ. The burden of online friends: the effects of giving up Facebook on stress and well-being. J Soc Psychol. 2018;158(4):496–507. doi: 10.1080/00224545.2018.1453467. [DOI] [PubMed] [Google Scholar]
- 52.Brailovskaia J, Ströse F, Schillack H, Margraf J. Less Facebook use – more well-being and a healthier lifestyle? An experimental intervention study. Comput Human Behav. 2020 Jul;108:106332. doi: 10.1016/j.chb.2020.106332. [DOI] [Google Scholar]
- 53.Graham S, Mason A, Riordan B, Winter T, Scarf D. Taking a break from social media improves wellbeing through sleep quality. Cyberpsychol Behav Soc Netw. 2021 Jun;24(6):421–5. doi: 10.1089/cyber.2020.0217. [DOI] [PubMed] [Google Scholar]
- 54.Hunt MG, Marx R, Lipson C, Young J. No more FOMO: limiting social media decreases loneliness and depression. J Soc Clin Psychol. 2018 Dec;37(10):751–68. doi: 10.1521/jscp.2018.37.10.751. [DOI] [Google Scholar]
- 55.Hunt M, All K, Burns B, Li K. Too much of a good thing: who we follow, what we do, and how much time we spend on social media affects well-being. J Soc Clin Psychol. 2021 Feb;40(1):46–68. doi: 10.1521/jscp.2021.40.1.46. https://guilfordjournals.com/doi/10.1521/jscp.2021.40.1.46 . [DOI] [Google Scholar]
- 56.Thai H, Davis CG, Stewart N, Gunnell KE, Goldfield GS. The effects of reducing social media use on body esteem among transitional-aged youth. J Soc Clin Psychol. 2021 Dec;40(6):481–507. doi: 10.1521/jscp.2021.40.6.481. [DOI] [Google Scholar]
- 57.Hughes ME, Waite LJ, Hawkley LC, Cacioppo JT. A short scale for measuring loneliness in large surveys: results from two population-based studies. Res Aging. 2004;26(6):655–72. doi: 10.1177/0164027504268574. https://europepmc.org/abstract/MED/18504506 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 58.Chand SP, Kuckel DP, Huecker MR. StatPearls Treasure Island. Treasure Island (FL): StatPearls Publishing; 2022. [2022-08-13]. Cognitive Behavior Therapy. https://www.ncbi.nlm.nih.gov/books/NBK470241/ [PubMed] [Google Scholar]
- 59.Harari GM, Gosling SD. Concerns about Facebook among users and abstainers: relationships with individual differences and Facebook use. Transl Issues Psychol Sci. 2016;2(3):261–74. doi: 10.1037/tps0000081. https://psycnet.apa.org/record/2016-47442-006 . [DOI] [Google Scholar]
- 60.Rideout V, Fox S. Digital health practices, social media use, and mental well-being among teens and young adults in the U.S. HopeLab. 2018. [2022-08-13]. https://hopelab.org/reports/pdf/a-national-survey-by-hopelab-and-well-being-trust-2018.pdf .
- 61.Srivastava K, Chaudhury S, Prakash J, Dhamija S. Social media and mental health challenges. Ind Psychiatry J. 2019 Jul;28(2):155–9. doi: 10.4103/ipj.ipj_154_20. https://europepmc.org/abstract/MED/33223706 .IPJ-28-155 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 62.Escobar-Viera CG, Whitfield DL, Wessel CB, Shensa A, Sidani JE, Brown AL, Chandler CJ, Hoffman BL, Marshal MP, Primack BA. For better or for worse? A systematic review of the evidence on social media use and depression among lesbian, gay, and bisexual minorities. JMIR Ment Health. 2018 Jul 23;5(3):e10496. doi: 10.2196/10496. https://mental.jmir.org/2018/3/e10496/ v5i3e10496 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 63.Du J, Kerkhof P, van Koningsbruggen GM. The reciprocal relationships between social media self-control failure, mindfulness and wellbeing: a longitudinal study. PLoS One. 2021 Aug 04;16(8):e0255648. doi: 10.1371/journal.pone.0255648. https://dx.plos.org/10.1371/journal.pone.0255648 .PONE-D-20-21281 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 64.Yao MZ, He J, Ko DM, Pang K. The influence of personality, parental behaviors, and self-esteem on Internet addiction: a study of Chinese college students. Cyberpsychol Behav Soc Netw. 2014 Feb;17(2):104–10. doi: 10.1089/cyber.2012.0710. https://europepmc.org/abstract/MED/24003966 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 65.Naslund JA, Bondre A, Torous J, Aschbrenner KA. Social media and mental health: benefits, risks, and opportunities for research and practice. J Technol Behav Sci. 2020 Sep;5(3):245–57. doi: 10.1007/s41347-020-00134-x. https://europepmc.org/abstract/MED/33415185 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 66.Sharma MK, Anand N, Roopesh BN, Sunil S. Digital resilience mediates healthy use of technology. Med Leg J. 2022 Dec;90(4):195–9. doi: 10.1177/00258172211018337. [DOI] [PubMed] [Google Scholar]
- 67.Orben A, Przybylski AK. The association between adolescent well-being and digital technology use. Nat Hum Behav. 2019 Feb;3(2):173–82. doi: 10.1038/s41562-018-0506-1.10.1038/s41562-018-0506-1 [DOI] [PubMed] [Google Scholar]
- 68.Çimke S, Cerit E. Social media addiction, cyberbullying and cyber victimization of university students. Arch Psychiatr Nurs. 2021 Oct;35(5):499–503. doi: 10.1016/j.apnu.2021.07.004.S0883-9417(21)00113-8 [DOI] [PubMed] [Google Scholar]
- 69.Ioannidis JP, Patsopoulos NA, Rothstein HR. Reasons or excuses for avoiding meta-analysis in forest plots. BMJ. 2008 Jun 21;336(7658):1413–5. doi: 10.1136/bmj.a117. https://europepmc.org/abstract/MED/18566080 .336/7658/1413 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 70.Escobar-Viera CG, Shensa A, Bowman ND, Sidani JE, Knight J, James AE, Primack BA. Passive and active social media use and depressive symptoms among United States adults. Cyberpsychol Behav Soc Netw. 2018 Jul;21(7):437–43. doi: 10.1089/cyber.2017.0668. [DOI] [PubMed] [Google Scholar]
- 71.Winstone L, Mars B, Haworth C, Heron J, Kidger J. Adolescent social media user types and their mental health and well-being: results from a longitudinal survey of 13-14-year-olds in the United Kingdom. JCPP Adv. 2022 Mar 10;2(2):e12071. doi: 10.1002/jcv2.12071.JCV212071 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 72.Verduyn P, Ybarra O, Résibois M, Jonides J, Kross E. Do social network sites enhance or undermine subjective well-being? A critical review. Soc Issues Policy Rev. 2017 Jan 13;11(1):274–302. doi: 10.1111/sipr.12033. https://spssi.onlinelibrary.wiley.com/doi/abs/10.1111/sipr.12033 . [DOI] [Google Scholar]
- 73.Valkenburg PM, van Driel II, Beyens I. The associations of active and passive social media use with well-being: A critical scoping review. New Media Soc. 2021 Dec 31;24(2):530–49. doi: 10.1177/14614448211065425. https://journals.sagepub.com/doi/10.1177/14614448211065425 . [DOI] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Search strategy used for MEDLINE.
Quality assessment tool for quantitative studies scoring criteria.
Quality scores according to the Effective Public Health Practice Project Quality Assessment Tool and overall effectiveness of social media use interventions on outcomes.